
Abstract
Objective:
To describe the frequency and trends of use of antipsychotics in Canadian children and adolescents from 2005 to 2009.
Methods:
We performed analyses on the IMS Brogan databases on drug recommendation (prescribed drug) frequency, reasons for recommendations (therapeutic indication), and duration of use of antipsychotics, psychostimulants, and selective serotonin reuptake inhibitors (SSRIs) for Canadian children between 2005 and 2009. Changes in the number of and reasons for drug recommendations over the 5-year period are highlighted by using descriptive statistics.
Results:
Antipsychotic drug recommendations by all specialists for children increased by 114% from 2005 to 2009. In contrast, psychostimulant and SSRI drug recommendations increased by 36% and 44%, respectively. The majority of antipsychotic drug recommendations were for second-generation antipsychotics (SGAs). Attention-deficit/hyperactivity disorder (ADHD) was the most common therapeutic indication associated with an SGA recommendation. Antipsychotic drug recommendations for children with ADHD more than tripled between 2005 and 2009. The average duration of antipsychotic use in children varied by drug and age group. For risperidone, median duration of use was 90 days in children aged 1–6, 180 days in children aged 7–12, and 200 days in children aged 13–18.
Conclusion:
The use of antipsychotics in Canadian children greatly increased from 2005 to 2009. Comparison of antipsychotic data with psychostimulant and SSRI data shows that there has been a disproportionate increase in antipsychotic use over this interval, despite the lack of approval for pediatric use by Health Canada. Postmarketing surveillance activities of antipsychotic use in children appear appropriate.
Introduction
The SGAs have been used “off-label” in Canadian youth for a number of mental health disorders, including aggression in attention-deficit/hyperactivity disorder (ADHD), Oppositional Defiant Disorder, and Conduct Disorder; irritability related to autism spectrum disorders; tic disorders, mood disorders, and psychosis. Randomized controlled trials (RCTs) have demonstrated efficacy of SGAs in these conditions (Kumra et al. 1996; Sallee et al. 2000; DelBello et al. 2002; Findling et al. 2008; Haas et al. 2009; Kryzhanovskaya et al. 2009; Marcus et al. 2009). At present, none of the SGAs has received official indications by Health Canada for the treatment of children. A survey of Canadian clinicians found that 94% of child psychiatrists and 89% of developmental pediatricians prescribed SGAs to children. Most survey respondents indicated that they prescribed SGAs for numerous diagnoses and symptoms (Doey et al. 2007).
The use of SGAs in children and adolescents has dramatically increased in the United States and United Kingdom over the past decade. Patel examined trends in prescribing antipsychotics within the Texas Medicaid Program from 1996 to 2000 (Patel et al. 2002). They assessed the number of children with at least one Medicaid prescription claim for an antipsychotic per 1,000 enrollees over a 5-year period. Over this period, there was a 160% increase in prescriptions for antipsychotics. The SGA use increased by 494%. Olfson et al. (2006) also examined trends in outpatient treatment of children with antipsychotic drugs from the U.S. National Ambulatory Medical Care Survey. They found that from 2000 to 2002, the most common diagnoses associated with a mental health care visit with the prescription of an antipsychotic were disruptive behavior disorders (37.8%), mood disorders (31.8%), pervasive developmental disorders or mental retardation (17.3%), and psychotic disorders (14.2%). Rani et al. (2008) investigated the epidemiology of antipsychotic prescribing to children in general practice in the United Kingdom. They found that the overall prevalence of use of all antipsychotics doubled from 1992 to 2005, with a 60-fold increase in SGA prescriptions.
To date, there is no available information on the national use of SGAs in youth in Canada. Existing studies from the United States (Patel et al. 2002; Olfson et al. 2006) do not describe longitudinal use of these medications, do not provide details on which SGAs are prescribed, or do not distinguish the specialty of prescribing physicians. Our objective is to describe the frequency of use, and trends in use, of antipsychotics for children and adolescents in Canada, including the specialty of the prescribing physician, the reason for drug recommendations, and the duration of use. To place this information in a larger overall context, we will compare trends in antipsychotic medication prescribing in children with prescriptions for psychostimulants and selective serotonin reuptake inhibitors (SSRIs) in children over the 2005 to 2009 time interval. We hypothesized that the use of antipsychotics in Canadian youth increased from 2005 to 2009, and that the increase would be disproportionately greater than the rate of increase in psychostimulant and SSRI use.
Methods
IMS Brogan (IMS) is a proprietary source of pharmacoepidemiologic data that can be used to describe the pharmacoepidemiology of antipsychotics in Canadian children. Administrative data cannot be used for this purpose, because, in most Canadian provinces, administrative records for prescription data are only collected in special population groups, for example, those covered by publicly funded drug plans, and the extent of coverage differs across provinces. Several national surveys have collected information on medication use (e.g., the National Population Health Survey) (Catlin and Will 1992), National Longitudinal Study of Children and Youth (Statistics Canada 2009), but no surveys having an adequate sample size have targeted the relevant age group.
IMS is a world leading provider of market intelligence to the pharmaceutical and health care industries. Their data products are used by academics, pharmaceutical companies, drug plan administrators, and government. At the time data is requested (in our case, January of 2010), information on the medications of interest for the last 5 completed years (2005–2009) is available for analysis. We performed analyses based on the IMS databases (Carleton et al. 2005). We studied data from the Canadian Disease and Therapeutic Index (CDTI), a national physician panel study. Participating physicians comprise a representative sample both geographically and by specialty, with weighting adjustments made to estimate national drug recommendations by year. Each physician participating in the panel completes a record of all patient visits during a 2-day period. The nature of each visit, including the age and gender of the patient, drug recommendation (prescribed drug), and the therapeutic indication (reason for making the recommendation) are recorded. Analyses of the CDTI database allow us to characterize the frequency with which physicians recommend medications for children as well as the reasons for these recommendations. The data are recorded as recommendations, rather than prescriptions, as the rate of prescription purchases are not recorded in this database. We derived estimates of the pattern of antipsychotic (risperidone, olanzapine, quetiapine, aripiprazole, clozapine, ziprasidone, and paliperidone), psychostimulant (methylphenidate and dextroamphetamine), and SSRI (fluoxetine, sertraline, fluvoxamine, citalopram, paroxetine, and escitalopram) use during the preceding 5 years up to 2009. Risperidone, olanzapine, quetiapine, and clozapine have been available in Canada from before 2005, but ziprasidone and paliperidone were released in Canada in 2008, and aripiprazole, in 2010. We also analyzed the specific therapeutic indication for drug recommendations. Mood disorder included both bipolar disorder and major depressive disorder, and psychotic disorder included schizophrenia, schizoaffective disorder, and psychosis not otherwise specified.
We also utilized the IMS Longitudinal database. This database links prescriptions together over time, creating a longitudinal, individual level record. We used the Longitudinal database to estimate the average duration of the use of antipsychotics, psychostimulants, and SSRIs in children between 2005 and 2009. IMS’ anonymized longitudinal prescription information provides weekly refreshed data from a representative sampling of more than 4,000 retail pharmacies representing all regions and all payers (public, private, and uninsured). This database captures in excess of 62% of all prescription activity in Canada. The longitudinal database tracks over 20 million anonymized patients whose prescription data can be longitudinally followed within a pharmacy. Patient age is submitted as an element on the prescription records. The longitudinal data are sourced from geographically dispersed retail pharmacy panels, which provide IMS with 100% of their prescription transactions. In 2006, 17.3% of the 16,318,881 patients in the longitudinal database were less than 19 years of age. IMS Brogan estimates that there is a 5%–15% loss of patients over a 5-year cohort.
Census data were obtained from Statistics Canada to obtain the total population of inhabitants of Canada under 19 years of age by year from 2005 to 2009 and by province. Census data were obtained to assess whether changes occurred in the size of the population of children and adolescents in Canada from 2005 to 2009, which could account for increased use of medications.
Results
Using the CDTI database, antipsychotic drug recommendations for youth by physicians (all specialties) in Canada have increased by 114% from 2005 to 2009, from 308,490 drug recommendations in 2005 to 661,300 in 2009 (Fig. 1). The majority of drug recommendations were for SGAs, which accounted for 95% of the recommendations in 2009. Recommendations for SGAs rose from 285,070 in 2005 to 631,980 in 2009. Risperidone was the most commonly recommended drug, followed by quetiapine (Fig. 2; data not shown for ziprasidone, aripiprazole, and paliperidone due to overall low numbers). Recommendations for risperidone and quetiapine increased on a yearly basis. Recommendations for olanzapine and clozapine remained stable. In comparison, drug recommendations for psychostimulants in children rose by 36% from 2005 to 2009, from 1,253,890 drug recommendations in 2005 to 1,702,820 in 2009; and drug recommendations for SSRIs increased by 44%, from 360,200 prescriptions in 2005 to 518,230 in 2009. Methylphenidate was the most commonly recommended drug of the psychostimulants. Fluoxetine was the most commonly recommended SSRI, followed by citalopram. The relative proportion of drug recommendations yearly by class for SGAs, FGAs, psychostimulants, and SSRIs is shown in Table 1. This revealed that SGA recommendations increased ∼7% relative to the other medication classes.

Yearly antipsychotic drug recommendations, for children in Canada, 2005–2009. Source: IMS Brogan, A Unit of IMS–Canadian Disease & Therapeutic Index.
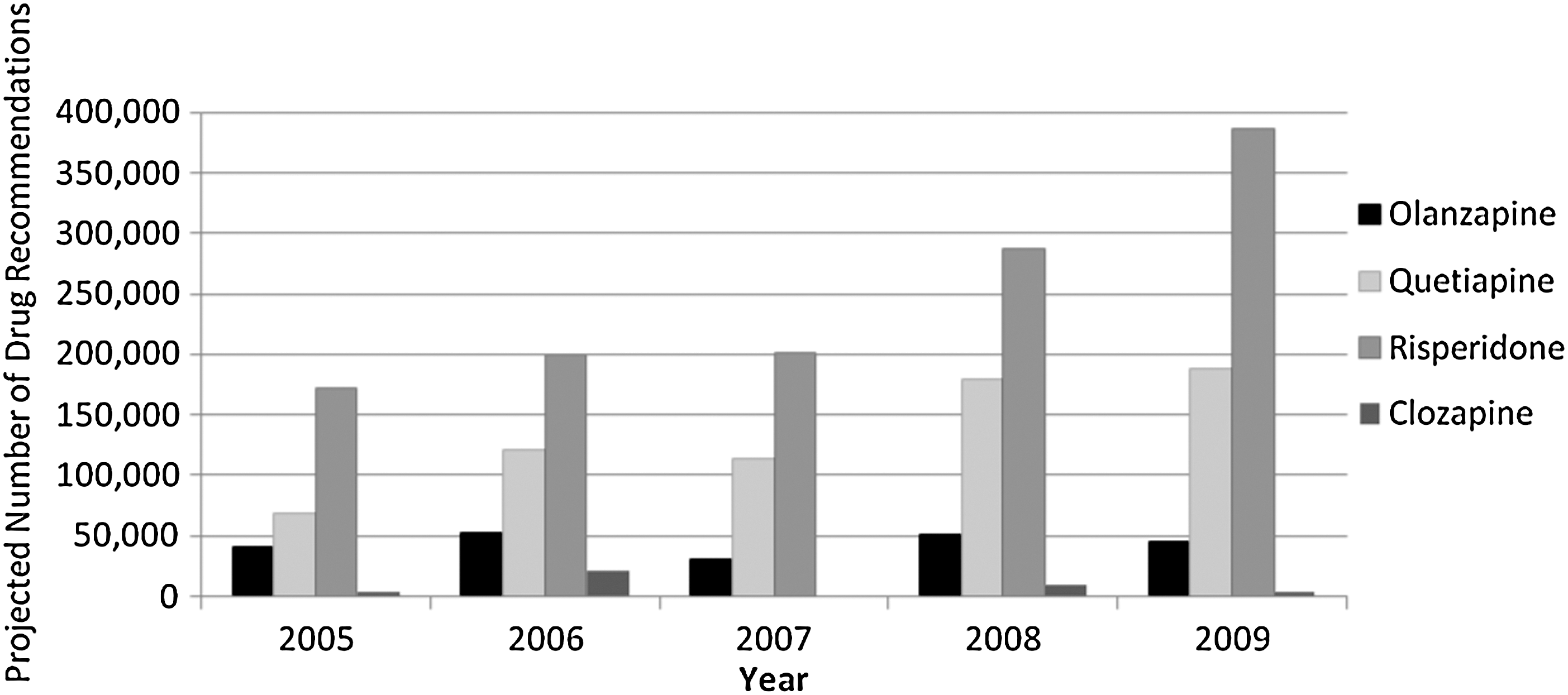
Yearly second-generation antipsychotic recommendations by medication for children in Canada, 2005–2009. Source: IMS Brogan, A Unit of IMS–Canadian Disease & Therapeutic Index.
FGAs=first-generation antipsychotics; SGAs=second-generation antipsychotics; SSRIs=selective serotonin reuptake inhibitors.
The most common reasons an SGA was recommended for a child or adolescent (therapeutic indication) from 2005 to 2009 was for ADHD (17%), mood disorder (16%), conduct disorder (14%), and psychotic disorder (13%) (Fig. 3). The number of antipsychotic recommendations for ADHD more than tripled over this 5-year period, from 38,140 drug recommendations in 2005, to 134,200 in 2009. In comparison to the other four top reasons for antipsychotic recommendations, ADHD showed a steady increase from 2005 to 2009, whereas there was more random yearly fluctuation for the other disorders (see Fig. 4). The most common reasons an FGA was recommended for a child from 2005 to 2009 was for a tic disorder (30%), followed by a psychotic disorder (28%). The most common reason that a psychostimulant was recommended for a child from 2005 to 2009 was for ADHD (91%). Mood disorder (50%) and anxiety disorders (25%) were the most common reasons for drug recommendations for SSRIs. Increases in drug recommendations for children occurred each year despite population data from Statistics Canada which show that the number of children (persons aged 0–19) in Canada actually slightly decreased each year, from 7,874,686 children in 2005, to 7,863,731 children in 2009. The number of antipsychotic drug recommendations per one hundred children in Canada rose from 3.6 in 2005 to 8.2 in 2009.
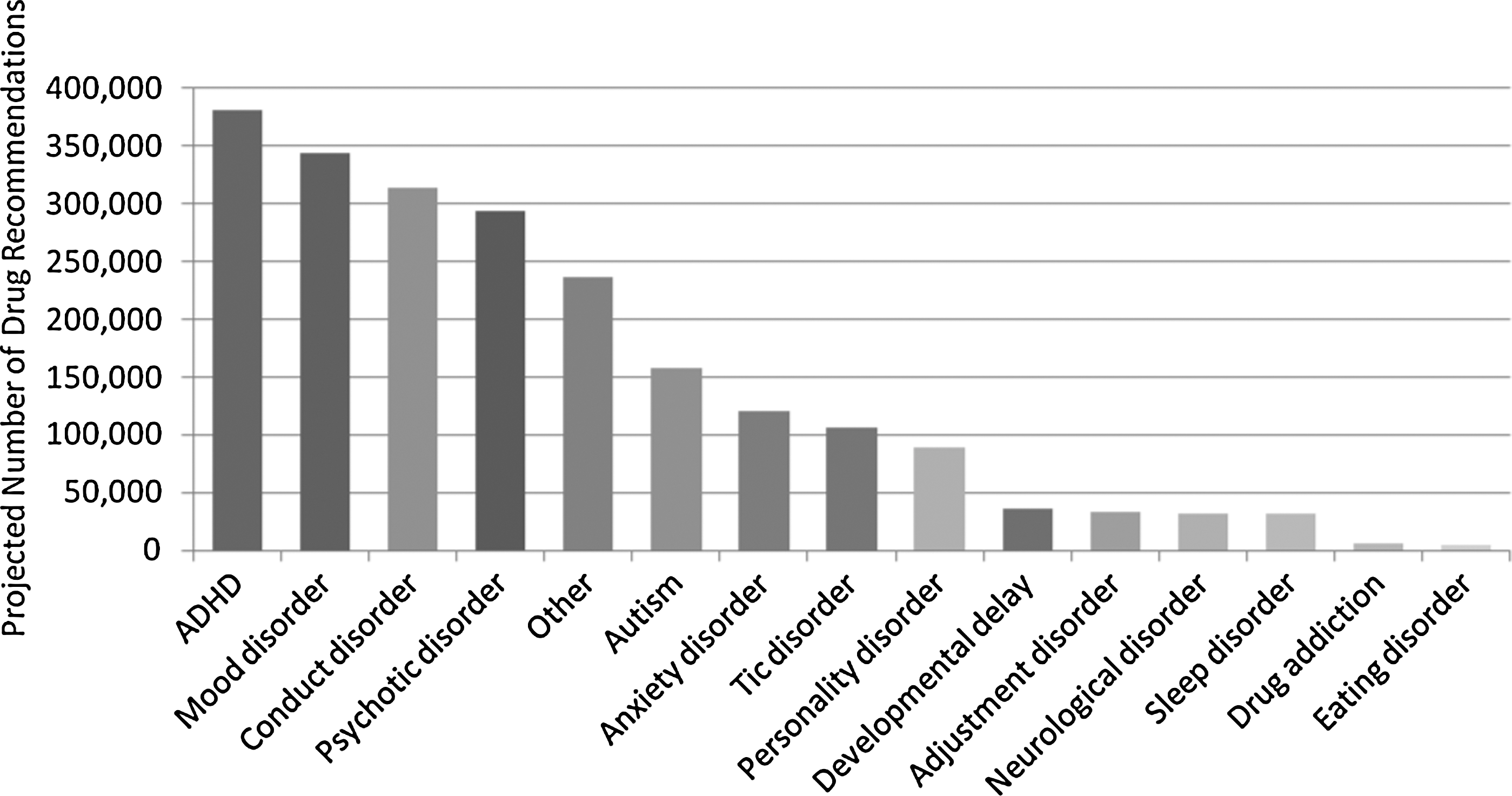
Second-generation antipsychotic drug recommendations by therapeutic indication for children in Canada, 2005–2009. Source: IMS Brogan, A Unit of IMS–Canadian Disease & Therapeutic Index.

Yearly second-generation antipsychotic drug recommendations by diagnosis for children in Canada, 2005–2009. Source: IMS Brogan, A Unit of IMS–Canadian Disease & Therapeutic Index.
Drug recommendations for antipsychotics for youth were made mainly by psychiatrists. Nationally, 62% of recommendations for antipsychotics were made by a psychiatrist, followed by pediatricians and family physicians/general practitioners (GP) each at 17%, and other specialties at 3%. For psychostimulants, pediatricians made the majority of drug recommendations (44%), followed by family physicians (37%), psychiatrists (17%), and other specialties (3%). Psychiatrists made the majority of SSRI recommendations in children (52%). This was followed by family physicians/GP (37%), pediatricians (10%), and other specialties (1%).
The average duration of antipsychotic use by children and adolescents in Canada over the 5-year period of 2005 to 2009 varied by drug type and age group. Nationally for risperidone, median duration of use was 90 days in children aged 1–6, 180 days in children aged 7–12, and 200 days in children aged 13–18. Length of prescriptions for each drug by age group are described in Table 2. In comparison to psychostimulants and SSRIs, the average duration of treatment with the most commonly prescribed antipsychotic, risperidone, was comparable to the average duration of methylphenidate use by age group, and considerably longer than the average duration of use of fluoxetine.
Source: IMS Brogan, A Unit of IMS–LRx Longitudinal Database.
Discussion
Drug recommendations for antipsychotics for Canadian children and adolescents dramatically increased from 2005 to 2009, despite the fact that Health Canada has not approved any of the SGAs for use in children, and the absence of population growth. The Canadian situation closely resembles the United States, though the FDA has approved the use of risperidone and aripiprazole for the treatment of schizophrenia in adolescents, acute manic or mixed episodes in children aged 10–17 with bipolar disorder, and in children aged 5–16 with irritability associated with autistic disorder. The increase in use in Canada may be due to emerging evidence over the past decade from RCTs, especially with regard to the treatment of ADHD. Of the SGAs, risperidone has the greatest number of pediatric trials. According to our Canadian data, the number of drug recommendations for children for risperidone are greater than for all the other SGAs combined. This suggests that Canadian clinicians are following the literature with regard to which medications have been most studied in children with mental health disorders.
Comparison of the data on antipsychotic prescribing for children with that of psychostimulants and SSRIs shows there has been a disproportionate increase in antipsychotic use over this time interval. Psychostimulant and SSRI use in children use has also increased, but the amount of growth was moderate. The relative proportion of drug recommendations for SGAs rose approximately by 7% between 2005 and 2009. Although this is not as impressive as the 114% increase in drug recommendations for SGAs over this time period, this is mainly due to the fact that psychostimulant medication recommendations, which account for the majority of drug recommendations for children, also rose by 36% over this time period.
SSRI prescriptions in Canadian children increased despite the Health Canada warning in 2004 regarding the use of all SSRI medications in children and adolescents, prompted by reports of suicidality in pediatric patients treated with antidepressant drugs (Hammad et al. 2006). This supports the findings of Valluri et al. (2010), who found that children with major depression disorder did not experience a decrease in antidepressant treatment between 2003 and 2006. An important difference in prescribing patterns for these three types of medications is the diversity of indications in which the antipsychotics are being recommended for, in comparison to psychostimulants, which are almost exclusively used for ADHD and SSRIs, which are mainly used for mood and anxiety disorders.
Although the growing use of antipsychotic medications has arisen from progress in the psychopharmacology of pediatric mental health disorders, there is concern for the evidence for metabolic side effects in children taking these medications. Correll studied the association of SGAs with body composition and metabolic parameters in children in a prospective cohort study (Correll et al. 2009). After a median of 10.8 weeks of therapy (interquartile range 10.5–11.2 weeks), weight increased by 8.5 kg with olanzapine, 6.1 kg with quetiapine, 5.3 kg with risperidone, and 4.4 kg with aripiprazole, in comparison to a minimal weight change of 0.2 kg in an untreated comparison group. Changes in cholesterol were also seen over this period; baseline to endpoint changes reached statistical significance for olanzapine and quetiapine for total cholesterol, triglycerides, and non-high-density lipoprotein cholesterol. In the risperidone group, triglyceride levels were significantly increased. These metabolic side effects, which have also been demonstrated in controlled clinical trials of the SGAs in children, are important given the frequency of use of these medications and rising rates of childhood obesity over the past decade.
Between 2005 and 2009, recommendations for antipsychotics for children with ADHD more than tripled. Three RCTs on the use of risperidone in children with ADHD and/or disruptive behavioral disorders have been published (Aman et al. 2002; Snyder et al. 2002; Armenteros et al. 2007). Armenteros et al. (2007) evaluated the effects of risperidone augmentation for treatment resistant aggression in children with ADHD. Children already on treatment with a psychostimulant were randomized to placebo or risperidone for 4 weeks. The study found a significant reduction in aggressive behaviors (decrease of at least 30% on the Children's Aggression Scale-Parent total score) from baseline to endpoint when compared with placebo treatment. However, no other differences were found for the individual subscales of the instrument or for the Teacher total score or any of its subscales. Snyder et al. (2002) and Aman et al. (2002) performed nearly identical RCTs and found that risperidone was efficacious in treating aggression in children with disruptive behavior disorders, with and without co-morbid ADHD. These studies, however, included a large number of children with subnormal IQ, a notable difference from the Armenteros study.
The Texas Children's Medication Algorithm Project for Pharmacotherapy of ADHD (Pliszka et al. 2006) includes an algorithm and recommendations for the treatment of ADHD co-morbid with aggression. The consensus panel recommends that treating physicians assess the effectiveness of stimulants in reducing aggressive behaviors. If aggressive outbursts remain problematic despite attenuation of ADHD symptoms, then a behavioral intervention targeting the aggressive behavior is recommended. If the behavioral treatment produces inadequate improvement, or the aggressive behavior is so extreme that it poses a danger, then an SGA is recommended to be added to the stimulant. The use of SGAs for aggressive behavior in children with ADHD is reasonable; it is unclear from our current data whether clinicians are pursuing the recommended intermediate steps before the initiation of SGAs.
The fact that school age children are remaining on risperidone for several months further underscores the need for close monitoring of adverse effects related to their use. Since the longitudinal database captures in excess of 62% of all prescription activity in Canada, we feel that the data presented are a good representation of Canadian youth receiving these medications. The majority of RCTs are of short duration, with treatment periods of 6–12 weeks. Three RCTs of 6 months duration in children with autism and disruptive behavioral disorders have demonstrated significant weight gain and a higher risk of extrapyramidal side effects in children treated long term (Luby et al. 2006; Nagaraj et al. 2006; Reyes et al. 2006).
Our study used data from IMS. Although this is a valuable source of pharmacoepidemiologic information, there are some limitations. Data from the CDTI are based on a national sampling strategy that comprises a representative sample both geographically and by specialty; it is possible for sampling errors to over or under estimate national drug recommendations. The longitudinal database is limited to prescribed medications in Canada that are dispensed in a retail pharmacy. No hospital-based administered medications are included in the longitudinal database. In the case where patients spread their prescriptions across multiple outlets, some prescription activity may not be included.
Conclusion
In conclusion, national pharmacoepidemiologic data show that the use of antipsychotics in Canadian children and adolescents greatly increased from 2005 to 2009, and that once prescribed, these medications are used for several months. Despite the availability of clinical trial data supporting the efficacy of these medications for pediatric mental health disorders, Health Canada has not approved the use of these drugs in children. Given the increasing frequency of use of these medications in Canadian children, and the known side effects, high standards of care are required. Postmarketing surveillance activities of antipsychotic use in children appear appropriate. Further research on the prevention of side effects of these drugs will help improve the standard of care of pediatric mental health disorders.
Clinical Significance
There has been a disproportionate increase in the use of antipsychotic medications in Canadian children in comparison to psychostimulants and SSRIs. Antipsychotic medications are being prescribed for a wide variety of pediatric mental health conditions, and once prescribed, they are taken for long periods. From 2005 to 2009, the use of antipsychotic medications in children with a primary diagnosis of ADHD has increased more than three fold. Given the long-term use of antipsychotic medications, diversity of conditions for which they are being used, and increasing overall use, postmarket surveillance activities aiming at prevention of adverse effects appear appropriate.
Footnotes
Disclosures
Tamara Pringsheim, Darren Lam, and Scott Patten have nothing to disclose.