
Abstract
The purpose of this study was to investigate whether a long-acting methylphenidate formulation (MPH-ret) is as effective as two doses of immediate-release methylphenidate (MPH-IR) in reducing attention-deficit/hyperactivity disorder (ADHD) symptoms including inattention, impulsivity, and hyperactivity during the course of the day. Two groups of children (n=18 each) with ADHD aged between 8 and 12 years completed a continuous performance test in combination with a motion-tracking system four times a day within 8 hours. Inattention (standard deviation of reaction time), impulsivity (commission error rate), and hyperactivity (path length of the headband) were simultaneously measured. We included a control group (n=20) to rule out circadian fluctuations of attentional performance and motor activity. We observed a postlunch dip in attentional performance and an increasing trend of motor activity throughout the day whereas impulsivity remained stable in controls. The MPH-ret and MPH-IR groups had comparable treatment effects on measures of hyperactivity and inattention and normalized participant performance to control levels. In contrast, MPH-IR seems to have an advantage over MPH-ret in impulsivity treatments. Thus, our data suggest that it is crucial to assess the different domains of ADHD symptoms precisely over the course of a day to determine the optimal titration and stimulant formulation for a person with ADHD.
Introduction
Due to the fact that MPH-LA products are taken once per day, child compliance may increase for a number of reasons: Children who feel stigmatized by the public administration of a pill may refuse MPH-LA less often; there will be fewer problems with schools refusing to administer medication; there will be less parental unwillingness to use the medication if the school is unaware; and there will be less medication diversion in school (Swanson 2003). Thus, patients with ADHD who use MPH-LA are more likely to remain on their medication than those prescribed MPH-IR and have significantly fewer emergency room and general practitioner visits over 1 year (Kemner and Lage 2006). Hence, the standard practice in North America is now to use longer duration medications as the first line of treatment (CADDRA-Guidelines-Steering-Committe 2006). In clinical settings, however, patients often complain about the reduced efficacy of MPH-LA compared to MPH-IR, especially during the first hours after drug intake. This criticism is particularly important for the first hours at school. Therefore, some children get an additional prescription of MPH-IR for mornings to assist ADHD control at the beginning of the day or in the evening to prevent an unsettling loss of action (Banaschewski et al. 2008).
Teicher et al. (2006) used a combined system of motion tracking and continuous performance test (CPT) to examine the effects of different 12-hour MPH titration paradigms. The authors used d-MPH to simulate an escalating dose schedule wherein a low dose (0.2 mg/kg bodyweight) was given in the morning followed by small hourly doses (0.1 mg/kg). This paradigm was compared with a pulsatile-delivery paradigm in which a 0.4 mg/kg dose was first applied, followed by 0.4 mg/kg 4 hours later, and 0.2 mg/kg 8 hours later. In addition to the expected divergences in plasma levels, the authors detected differences in the motion-tracking system (MTS) and the CPT. For most children, the pulsatile delivery schedule optimally reduced ADHD symptoms. Thus, these results are in line with the above-mentioned clinical findings and suggest that a moderately large dose in the morning significantly reduces inattention and hyperactivity within 1 hour.
Teicher et al. (2006) showed that objective measures might be more sensitive than most of the studies that applied only behavioral rating scales to measure the efficacy of different MPH formulations across the day. For example, most studies that use behavioral scales did not find any differences between MPH-LA and MPH-IR regimes (Buitelaar and Medori 2009). Thus, the more subtle changes in attention or hyperactivity may go unnoticed when assessing parental or teacher ratings of ADHD symptoms. Moreover, more detailed analyses are possible if objective variables like computerized and highly standardized measures are used (Konrad et al. 2005).
Neuropsychological measures commonly assess attention (Egeland et al. 2009), impulsivity (i.e., inhibition; Nigg 2005), or hyperactivity (Teicher et al. 1996); these neuropsychological tools may be a valuable addition for measuring the efficacy of MPH medication (Konrad et al. 2004; Günther et al. 2005b, 2006, 2010). Moreover, subjective measures (e.g., rating scales) may significantly differ from these objective measures. We previously demonstrated that behavior ratings of inattentive symptoms are more related to objective measures of hyperactivity than to those of inattention. Thus, symptom scales suffer from problems of bias and subjectivity.
The purpose of this study was to determine whether a specific MPH-LA formulation is as effective as MPH-IR at reducing ADHD symptoms on objective measures of inattention, impulsivity and hyperactivity over the course of the day. Therefore, two groups of children with ADHD completed a CPT test with a MTS (“QbTest”; Bergfalk 2003) four times a day within 8 hours. The use of actigraphy and CPT together has been shown to have high discriminative validity in distinguishing children with ADHD from controls and has good test-retest reliability (Reichenbach et al. 1992; Teicher et al. 1996; Brocki et al. 2010). Further, CPT commission error rate can be used to assess impulsivity (Baker et al. 1995; Newcorn et al. 2001). Thus, this combination makes it possible to assess the three main symptoms of ADHD within one task in a short and economic way several times a day. We also included a control group to rule out circadian fluctuations and to adequately control fluctuations in inattention, impulsivity, and hyperactivity in typically developing children (Nakajima et al. 1998; Kraemer et al. 2000; Janvier and Testu 2007).
Methods
Participants and selection procedure
Thirty-six 8- to 12-year-olds with the combined subtype of ADHD (18 in each medication group) and 20 healthy 8- to 12-year-olds participated in this study. All children with ADHD met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) criteria (American Psychiatric Association 2000) and were recruited from our inpatient and outpatient departments of child and adolescent psychiatry. All new referrals suspected of having ADHD underwent an extensive psychiatric examination conducted by an experienced child and adolescent psychiatrist. We based DSM-IV-TR classification (ADHD diagnosis and co-morbidity) on a German semi-structured interview (K-DIPS; Unnewehr et al. 1995) of the parents and the child, the child's developmental history, playroom observation, and a pediatric examination. Exclusion criteria were: IQ below 80 (Wechsler Intelligence Scale for Children, 3rd edition; Tewes et al. 1999); potentially confounding diagnoses such as psychosis, mania, major depression, substance abuse, pervasive developmental or receptive language disorders; or taking any kind of additional medication. The three groups were not different with respect to age (F(2;55)=0.80; p=0.4454), IQ, (F(2;55)=0.04; p=0.961), and sex (χ 2 (2)=2.21; p=0.332). The ADHD groups did not differ with respect to symptom severity (parental rating; subscale for attention problems from the Child Behavior Check List [CBCL]; t(34)=0.45; p=0.653) or co-morbidity patterns. We obtained informed parental consent for all participants. The Medical Ethical Committee of the University Hospital of Aachen approved this study. In addition, all children gave their assent to participate. Table 1 summarizes major clinical and demographic data.
MPH, methylphenidate; IR, immediate release; ret, retard; CBCL, Child Behavior Check List; SD, standard deviation.
Medication protocol and experimental procedure
The MPH-LA product investigated in this trial (Medikinet® Retard; MPH-ret) is a preparation with a two-step dynamic to release MPH. MPH-ret contains equal portions of immediate-release pellets and an extended-release active substance (i.e., enteric coated pellets). The immediate release pellets cause a first plasma peak after 30 minutes, whereas extended-release substance induce a second peak 3–4 hours later (Pelz et al. 2008). Using a math test and an ADHD rating scale in a classroom setting, an MPH-ret and MPH-IR bioequivalence test demonstrated similar bioavailability (Döpfner et al. 2003) and the high efficacy of MPH-ret throughout the day. Herein, the total dose of MPH-ret was given in the morning and the MPH-IR doses were spread over the course of the day. Thus, MPH-ret seems to be as effective as MPH-IR (Döpfner et al. 2004). After 7 hours the concentration of both formulations was still 4 ng/mL and after 12 hours about 2 ng/mL (Döpfner et al. 2003).
Using an alternating randomization procedure, we assigned participants to either the MPH-IR group or the MPH-LA group (MPH-ret). Treatment started with low initial MPH doses (5 mg) and was increased in 5 mg steps until the best clinical response was obtained (measured with a behavioral questionnaire; FBB-HKS by Döpfner and Lehmkuhl 2000). The MPH dosage varied between 0.61 and 1.17 mg/kg bodyweight per day; however, the mean dosage did not differ between ADHD groups (t(34)=1.11; p=0.273; see Table 1). Before testing, we gave all children a minimum of 0.3 mg/kg MPH-IR or MPH-ret each day for at least 1 week to ascertain their drug tolerance. Most of the children (n=29) had a history of stimulant usage of >6 weeks before the experiment.
On the day of assessment, all children had breakfast in the morning. We directly administered medication after the morning assessment at 8 a.m. This dose was the only dose administered for the MPH-ret group, whereas the children in the MPH-IR received a second dose at 12 p.m. The dosages in the MPH-IR group were similar. All children participated in four assessments: Before drug administration (7:45 a.m.), 2, 6, and 8 hours after the drug administration. One day before the assessment began, the children performed the cognitive test procedure once. This was done to exclude test performance increases between 8 and 10 a.m. to test experience (Günther et al. 2005a). Between the four measurements the children participated in their daily routine of their inpatient treatment program. Outpatients were hosted in our inpatient department for the day and participated in the routine of the department. Controls were measured in their school environment and went back to their class after each measurement. The control group followed the same time assessment schedule without medication.
Dependent measures
To examine one dependent variable for each of the main ADHD symptoms, we combined a CPT with a MTS (“QbTest” developed by QbTech AB in Gothenburg, Sweden [Bergfalk 2003]). In this computer-based test, participants responded as quickly as possible by pressing a button each time we presented a 100-ms go stimulus (i.e., a filled gray circle) but were not to press anything when a 100-ms no-go stimulus (i.e., a filled gray circle with a black cross) appeared. The inter-stimulus interval was 1,900 ms. The task was composed of 450 stimuli with an equal numbers of go and no-go trials. We randomized presentation order. The test duration was 15 minutes. At the same time, the MTS recorded movements via a reflector attached to a participant-worn headband during the CPT. The position of the reflector was sampled 50 times per second with a spatial resolution of 1/27 mm per camera unit. The headband reflector was situated ∼100 cm in front of and 40 cm below the camera lens to record movement toward and away from the camera (Bergfalk 2003).
To measure inattention, we examined the standard deviation (SD) of reaction time in ms. Performance variability reflects behavioral symptoms such as difficulty sustaining attention, forgetfulness, disorganization, and careless errors (Castellanos et al. 2005). The commission error rate of the CPT (Dougherty et al. 2008) describes impulsivity. We calculated the commission error rate by dividing the number of incorrect button presses by the number of nontargets. The path length (i.e., distance) the headband reflector moves during the test characterizes hyperactivity. A previous study with 25 children with ADHD between 6 and 12 years demonstrated that these dependent variables are sensitive measures to detect medication effects in children with ADHD (Heiser et al. 2004). Significant changes due to MPH medication were detected for all parameters.
Statistical analysis
We analyzed data using PASW 18. An independent t-test, analysis of variance (ANOVA), Pearson's χ 2 assessed demographic, and clinical characteristics (mg MPH/kg body weight and inattention score of the CBCL; age and IQ; sex and co-morbidity, respectively). Repeated-measures ANOVA evaluated inattention, impulsivity, and hyperactivity with group (i.e., normal controls, MPH-IR, and MPH-ret) as the independent variable and time of measurement (i.e., 8 a.m., 10 a.m., 2 p.m., and 4 p.m.) as the within-subject factor. Levene's test compared the between-group error variance. A one-way ANOVA compared baseline measurement values of the three groups. Post-hoc comparisons checked for significant F-values. If we detected an interaction between group and time of measurement, we repeated the repeated-measures ANOVA without the control group to examine differential effects between the two medications in more detail. We separately analyzed the control group to investigate its associated dependent measure change over time.
Results
Change in hyperactivity, impulsivity, and inattention over time in the control group
We did not find a significant change across time for impulsivity (F(2;55)=0.14; p=0.938); however, we did detect a trend for hyperactivity (F(3;55)=2.36; p=0.089) and attentional performance (F(3;55)=2.81; p=0.047). Inattention was stable in the morning (p>0.05), significantly worsened between 10 a.m. and 2 p.m. (p<0.05), and improved again at the 4 p.m. measurement.
Differences between control and ADHD groups (MPH-IR and MPH-ret) without medication
Before the intake of MPH medication at 8 a.m., both ADHD groups significantly differed from the control group in inattention (F(2;55)=7.59; p=0.001), impulsivity (F(2;55)=3.42; p=0.040), and hyperactivity (F(2;55)=6.46; p=0.003). Conversely, no differences were detected between MPH-IR and MPH-ret groups (p>0.10). Thus, the two ADHD groups were comparable but significantly impaired with respect to all three ADHD symptoms compared to the control group as assessed by the QbTest.
Inattention during the course of the day
We found no group differences across all time points for inattention (F(2;53)=2.53; p=0.089). In addition to the differences at 8 a.m. (see above), we did not detect differences between controls and the medication groups (p>0.227). However, we found a significant effect of time (F(3;159)=15.13; p<0.001) and an interaction between group and time of measurement (F(6;159)=5.86; p<0.001). This interaction effect can best be explained by MPH medication. Due to the premedication differences between the medication groups and the controls at 8 a.m., a substantial drop in reaction time variability followed in the medication groups after receipt of MPH.
To examine differential effects between the medications, we reanalyzed the data without the control group. We did not find a group effect across time (F(1;34)=0.46; p=0.504). Further, we were still able to detect the effect of time (F(1;34)=16.78; p<0.001), whereas the interaction effect disappeared (F(1;34)=1.03; p=0.384). Thus, we found no differences between MPH-IR and MPH-ret groups during the day. Both ADHD groups showed a significant improvement in attention between 8 and 10 a.m. (p<0.001) and no significant change in attention from 10 a.m. to 4 p.m. (p>0.05). See Table 2 and Figure 1 for more details.
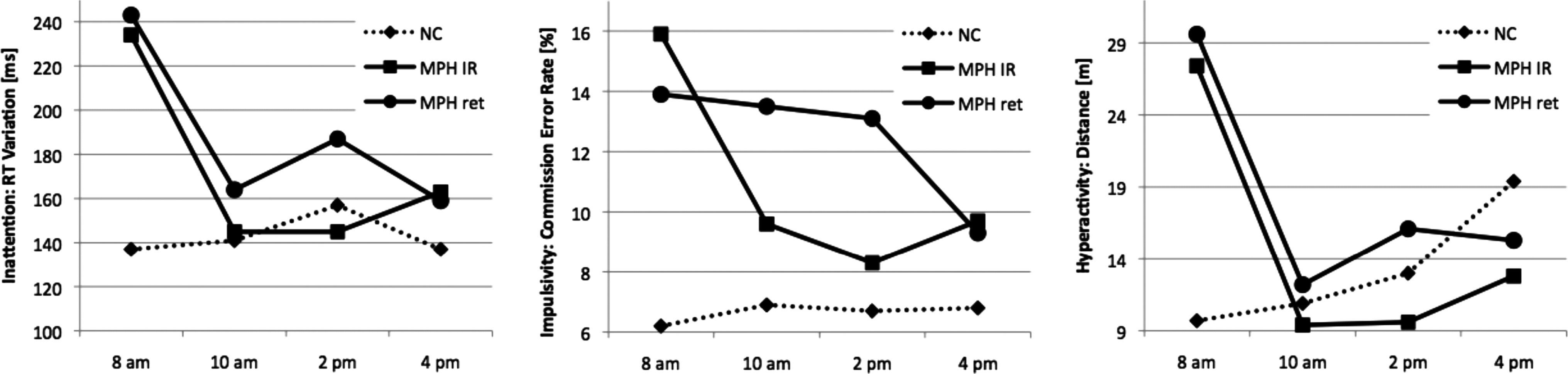
Results of inattention (left), impulsivity (middle), and hyperactivity (right) across the four measures. For inattention, we detected a postlunch dip at 2 p.m. (left) and an increasing hyperactivity across the day (right) for NC. Before drug administration (8 a.m.), groups with ADHD had a significant lower performance compared to NC. We found no differences between MPH-ret and MPH-IR for inattention and hyperactivity. After drug administration, children with ADHD reached a normal level at 10 a.m. for inattention and hyperactivity and the behavior did not change through 4 p.m. The results of the MPH-IR group for impulsivity are comparable to other outcomes (inattention and hyperactivity), whereas the performance of the MPH-ret group did not show improvement at 10 a.m. and 2 p.m. NC, normal controls; MPH, methylphenidate; IR, immediate release; ret, retard; ADHD, attention-deficit/hyperactivity disorder.
Inattention was measured as the reaction time (ms) variation, impulsivity as the commission error rate percentage, and hyperactivity as the length (m) the reflector moved during the test.
MPH-IR, methylphenidate immediate-release; MPH-ret, methylphenidate long-acting.
Impulsivity over the course of the day
With respect to impulsivity, we did not detect differences between the groups (F(2;53)=1.59; p=0.214); however, impulsivity did change across the day (F(3;159)=4.31; p=0.006) and this change differed among the three groups (F(6;159)=3.31; p=0.004). Interestingly, this change was caused by the differences between controls and the medication groups (see Fig. 1 for details). After excluding controls from the analysis, we found a significant effect of time across the day (F(1;34)=5.41; p=0.002) and an interaction effect between the two medication groups and time (F(1;34)=2.78; p=0.032). The impulsivity of children in the MPH-IR group significantly decreased between 8 and 10 a.m. (p<0.05). The performance remained stable until 4 p.m. and was comparable with that of controls (p>0.326). In contrast, the impulsivity of children in the MPH-ret group did not change until the third measurement and significantly decreased between 2 and 4 p.m. (p<0.05). Moreover, the SD at 2 p.m. was significant higher in the MPH-ret group (SD=14.5) compared to the MPH-IR group (SD=8.5; Levene's test: p=0.012; see Table 2).
Hyperactivity over the course of the day
We did not detect group differences for hyperactivity (F(2;53)=1.29; p=0.284); however, the effect of time on hyperactivity across the day was significant (F(3;159)=9.81; p<0.001). Further, we detected an interaction effect between time of measurement and group (F(6;159)=5.32; p<0.001). This interaction was due to deviations in both medication groups compared to the control group. The performance of both medication groups was comparable to controls at 10 a.m., 2 p.m., and 4 p.m. (p>0.248). When we reanalyzed the data without the control group, we were only able to detect an effect of time (F(1;34)=15.7; p<0.001). There was no interaction (F(1;34)=0.05; p=0.825) or differences between groups (F(1;34)=1.00; p=0.324). Hyperactivity decreased between 8 and 10 a.m. for both medication groups (p<0.001) and did not increase between 10 a.m. and 2 p.m. (p>0.242) and 2 and 4 p.m. (p>0.132). Like impulsivity, however, the SD for the MPH-ret group was significantly higher than the SD for the MPH-IR group at 2 p.m. (p=0.032).
Discussion
We examined whether MPH-ret is as effective as MPH-IR in reducing ADHD symptoms over the course of a day. Moreover, we included a control group to rule out the possibility that any observed effects were due to circadian fluctuations. First, we conducted a training assessment the day before the study to minimize improvement due to test experience. Thus, we did not detect changes in test performance between 8 and 10 a.m. in the control group. We did not find changes in impulsivity across the day in controls. Nevertheless, in concordance with previous studies (Hasher et al. 2007), we detected changes in attentional performance throughout the day. In our study, the control group attention decreased around midday and the attentional capability returned to baseline in the afternoon. Other studies found comparable results of early afternoon or postlunch dips in simple vigilance tasks (Monk et al. 1996) and more complex tasks, such as driving performance (Lenne et al. 1997). Additionally, we found a trend of increasing motor activity across the day for controls. This parameter was the only one to linearly increase across the day. Because there was no performance decrement across the day in controls, a motor activity increase due to the loss of participation motivation seems unlikely. In contrast to our study, increasing or decreasing diurnal motor activity has been previously found in children with psychiatric disorders more often than in healthy children (Teicher et al. 1993; Teicher 1995).
In line with previous results (Reichenbach et al. 1992; Teicher et al. 1996; Castellanos et al. 2005; Dougherty et al. 2008; Brocki et al. 2010), we found significant differences in inattention, hyperactivity, and impulsivity between children with ADHD and controls. Two hours after the initial dose, inattention and hyperactivity significantly decreased for both medication groups. Further, the behavior of children in both the MPH-ret and MPH-IR was comparable to controls. Moreover, this improvement remained stable at 2 and 4 p.m. These results support previous studies showing that different MPH-LAs are at least as effective as MPH-IR (Buitelaar and Medori 2009). However, we detected a differential effect between the two medications for impulsivity. In the MPH-IR group, the results for impulsivity are concurrent with day profiles for inattention and hyperactivity. There was a significant decrease in the number of commission errors 2 hours after drug administration and no change in performance at 2 and 4 p.m. In contrast, we did not detect improvement for the MPH-ret group in the morning and impulsivity significantly decreased in the afternoon between 2 and 4 p.m. To our knowledge, this MPH medication day-profile has not been previously described. Most studies report an improvement in impulsivity due to MPH medication using go/no-go tasks, stop-signal tasks, and sustained attention tasks (Epstein et al. 2006; Rhodes et al. 2006; DeVito et al. 2009). On a behavioral level, previous work reports increases in impulsivity or MPH-efficacy decrement over the course of a day (Pelham et al. 2001; Teicher et al. 2006). However, using a combination of motion tracking and CPT, some studies have found that impulsivity (measured as the number of commission errors) did not change after MPH administration in contrast to inattention and hyperactivity, (Matier et al. 1992). In addition, Sunohara et al. (1999) found that a high dose (0.56 mg/kg) but not a low dose of MPH (0.28 mg/kg) was associated with reduced impulsivity. At first glance at our data, impulsivity simultaneously decreases with a decreasing MPH-ret plasma level. Interestingly, Teicher et al. (2006) showed a comparable slope. These authors simulated different MPH-LAs, and in contrast to a decreasing plasma level, they observed an increase in performance level at the end of day, specifically after >8 hours postmedication onset. One possible explanation of this contradictory effect could be that performance is optimally modulated by lower, not higher, MHP doses for some neurocognitive tasks. In line with this hypothesis, previous studies (Tannock et al. 1995; Konrad et al. 2004; Günther et al. 2010) have suggested that stimulants modulate more complex attentional parameters (e.g., inhibition and impulsivity) according to an inverse U-shaped pattern. Inhibitory performance significantly increased under a low dose condition, whereas performance decreased under a high dosage. Taken together, the differential dose-dependent effects of MPH on neurobehavioral functioning might be due to different representations of attentional functions in the brain and due to the complex pharmacological actions of MPH at different brain sites. One may speculate that more complex attentional functions of the prefrontal cortex (e.g., inhibition), in particular, show a different dose-response curve from functions of the intensity dimension (e.g., alertness or sustained attention) or from hyperactivity. Thus, the MPH plasma level might have been too high in the MPH-ret condition between 10 a.m. and 2 p.m., as MPH-ret is a MPH-LA with one of the highest plasma levels 1 hour after administration (Banaschewski et al. 2008), with a later decrease in plasma level induced the optimal performance level.
This study has several limitations. First, the measures of inattention, impulsivity, and hyperactivity are routinely used in research; however, the discussion of the clinical validity of neuropsychological measures is still an open issue (Rommelse et al. 2008). Although the literature strongly supports the parameters used (see Stefanatos and Baron 2007 for a review), the definitions of attention (Van Zomeren and Brouwer 1994) and impulsivity (Kindlon et al. 1995) are complex. Different results are detected if these constructs are investigated according to a model-oriented approach for ADHD, wherein the different aspects of ADHD (inattention, impulsivity, and hyperactivity) are operationalized to measure them in standardized way. The magnitude of hyperactivity differs between naturalistic settings and structured academic settings (Porrino et al. 1983; Halperin et al. 1992); nevertheless, measuring the participant's motor activity while they are engaged in a continuous performance task (e.g., CPT) increases the ecological validity in laboratory settings. To research the efficacy of medications across the day, simplifying these constructs and putting them into practice to assess children four times a day is necessary. Further, the examined groups were rather small; thus, the effects of increasing hyperactivity across the day in controls and the divergent results of impulsivity measures for MPH-ret should be replicated. To test the hypothesis that decreasing medication plasma levels in the MPH-ret group were responsible for reducing impulsivity in the afternoon, including plasma measures in future studies is necessary. Finally, the results could not be generalized to other MPH-LA formulations with different pharmakinetic profiles.
Conclusions
In sum and bearing these limitations in mind, normal circadian fluctuations could influence typical ADHD symptoms such as inattention. When one is interpreting medication efficacy, consideration of normal diurnal changes may be informative. Both of the medications that we examined are comparable in their treatment of hyperactivity and inattention. For these two domains, patients with ADHD reached the performance level of the control group 2, 6, and 8 hours after medication onset. In contrast, MPH-IR seems to have an advantage over MPH-ret in impulsivity treatments. For a child with impulsive behavior, these results could be an argument against MPH-ret. Likewise, a child with inattentive and hyperactive symptoms seems to benefit from either MPH-IR or MPH-ret. These results underscore the conclusion that MPH may independently modulate impulsivity, inattention, and hyperactivity. Thus, precisely assessing ADHD symptoms over the course of the day to find the optimal titration and stimulant formulation for a child with ADHD is crucial.
Footnotes
Disclosures
Thomas Günther, Berrak Kahraman-Lanzerath, and Eva Lotte Knospe declare that no conflicts of interests exist.
Beate Herpertz-Dahlmann is a consultant to Eli Lilly and has received industry research funding from AstraZeneca, Eli Lilly, Novartis, and Janssen Cilag.
Kerstin Konrad received speaking fees from Eli Lilly, Novartis, and Medice.