
Abstract
In a former study, we reported decreased platelet vesicular monoamine transporter 2 (VMAT2) density (Bmax) in patients with ADHD. The current study aimed at measuring platelet VMAT2 in the disruptive behavior disorders (DBDs) to assess whether this finding is specific to ADHD or generalizable to the broader DBD concept. The study included 13 patients with DBDs aged 10–12 years and 16 healthy volunteers aged 8–17 years. All participants underwent a thorough clinical evaluation using Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime version for diagnosis, the Nisonger Child Behavior Rating Form, the Clinical Global Impressions Scale-Severity version, and the DSM-IV ADHD Scale (DAS). The study group's DAS scores did not differ from those of the control group. There was no significant difference between the patients with DBDs and the control group either in VMAT2 density (Bmax) or affinity (Kd) as measured by high-affinity [3H]TBZOH binding. We conclude that the formerly reported decreased platelet VMAT2 Bmax in patients with ADHD may be specific to ADHD and not present in DBDs. Larger-scale replication is needed.
Introduction
Some studies have related antisocial behavior in children to low levels of serotonin and epinephrine. Altered urinary catecholamine (CA) response to psychological challenges was found in children with CD (McBurnett et al. 2005). Low serotonin was demonstrated in aggressive patients (Coccaro et al. 1997), but this finding was not replicated (Berman et al. 1997). The key transporters in the accumulation of both catechoamines and serotonin are the VMATs (VMAT2) located on the membranes of the synaptic vesicles (Liu and Edwards 1997). Although VMAT1 is found in the adrenal medulla, VMAT2 is present in CA and serotonin (5-HT) neurons in the brain. This transporter has modest substrate specificity and can transport CA, indoleamines, and histamine into pre synaptic vesicles, using trans-membrane H+gradient. Down-regulation of VMAT2 results in less monoamine availability in the synapse and constitutes a target for the antipsychotic and antidyskinetic drugs reserpine and tetrabenazine (Liu and Edwards 1997). We demonstrated that human platelets can be used as an accessible peripheral model for the VMAT (Rehavi et al. 1998; Zucker et al. 2001a, 2002) and measured it in two children's psychiatric disorders: Tourette's disorder and ADHD (Toren et al. 2005; Ben-Dor et al. 2007).
In a previous study of VMAT2 in children with ADHD and controls, we have demonstrated that [3H]TBZOH binding capacity (Bmax) was significantly lower (17%) in the ADHD group as compared with the controls. There was no difference between the two groups in the affinity (Kd value) of [3H]TBZOH to its binding site. An inverse correlation was found between the ADHD symptom score and the Bmax values. It remains unclear whether the under-expression of platelet VMAT2 in children with ADHD is specific to ADHD or will be found also in all children with DBD.
In attempting to find an answer to this question, the present study aims at assessing the VMAT2 binding and affinity in children with DBDs versus control group. To the best of our knowledge, no former study measured VMAT2 in any DBD.
Experimental Procedures
Participants
Twelve boys and one girl (n = 13) aged 10–16 (14.1 ± 2.2) years in whom CD, ODD, or disruptive disorder NOS were diagnosed participated in the study group. The diagnosis was established by a senior child and adolescent psychiatrist in accordance with the DSM-IV-TR criteria (American Psychiatric Association 2000) and further confirmed through the use of Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime version (Kaufman et al. 2000) Hebrew version (Shanee et al. 1997). All participants had been drug free for at least 2 months before the study. Exclusion criteria included the presence of co-morbid psychiatric disorders (e.g., anxiety and mood disorders, substance abuse, psychotic disorders, and attention deficit disorder with and without hyperactivity) and any chronic physical disease.
Ten male and six female (n = 16) volunteers from the community, aged 8–17.5 (12.3 ± 3.2) years, served as controls. The controls underwent a comprehensive interview to exclude the presence of any psychiatric or physical disorder.
The study was approved by the Institutional Review Board. Written informed consent was obtained from the parents, and assent was obtained from all participants.
Psychometric Instruments
Rating scales for CD were completed for all participants (study and control groups), concomitantly with collecting their blood samples: (a) The Nisonger Child Behavior Rating Form (NCBRF)—an informant behavior rating scale, consisting of 66 questions on a Likert scale, ranging from 0 to 3 and assessing antisocial behavior of children and adolescents (Tasse et al. 1996). (b) The Clinical Global Impressions Scale-Severity version. Clinician rated scale for severity of behavioral symptoms rated 1–7 with 7 being the most severe (Guy 1976). (c) DSM-IV ADHD Scale (DAS) (Spivak et al. 1999) was used to exclude ADHD symptoms. DAS is a clinician-administered rating scale including the 18 items (score range 0 to 3) of the DSM-IV criteria for ADHD (9 for inattention and 9 for hyperactivity/impulsivity).
All rating scales are valid and reliable in children and adolescents and are widely used in child psychiatry research.
Platelet membrane preparation
As previously described (Toren et al. 2005), blood samples (25 mL) were collected between 8:00 and 10:00 AM into tubes containing an anticoagulant solution of 16 mM citrate buffer and 1 mM EDTA. Platelet-rich plasma was separated from blood cells by low-speed centrifugation (350 g for 10 min), diluted 1:1 in HEPES buffer 50 mM pH 8.0, and centrifuged at 1,700 g for 20 min. The pellet was disrupted with Brinkman polytron in 20 mL HEPES buffer 50 mM pH 8.0 containing 300 mM sucrose (buffer A) and centrifuged twice at 27,000 g for 20 min. It was then re-suspended in 4.5 mL buffer A to yield a protein concentration of about 1 mg/mL.
[3H]TBZOH binding
For [3H]TBZOH binding, 100 μL membranes were incubated at 25°C with 50 μL of [3H]TBZOH (eight concentrations, 0.5–8.0 nM) (specific activity: 20 Ci/mmol; American Radiolabeled Chemicals Inc., St. Louis, MO) and 50 μL buffer A. After 30 min of incubation, the mixture was filtered using vacuum on glass fiber filters (GF/C). The filters were washed four times with ice-cold buffer A, and the radioactivity was counted in scintillation liquid using a β-counter (Packard 1600 TR). Nonspecific binding was measured in parallel samples in the presence of 1 μM tetrabenazine (Fluka, Buch, Switzerland). This ligand was shown to inhibit [3H]TBZOH binding to human platelet VMAT2 in a competitive manner (IC50 = 10 nM) (Zucker et al. 2001b). The nonspecific binding at Kd value (3.2 nM) did not exceed 20%. Protein concentration was determined according to the Bradford's method (Bradford 1976). The ligand affinity (Kd) to VMAT2 and [3H]TBZOH binding capacity (Bmax) were assessed by Scatchard analysis.
Statistical analysis
SPSS statistical software, edition 19.0 for Windows (2010 by SPSS Inc., Chicago, IL) was used. Between-group comparisons of continuous variables and χ
2 for gender distribution analysis were done using two-tailed unpaired Student's t-test. All results are expressed as mean ± SD with 0.05 significance level. Pearson correlation was employed to assess correlation of the NCBRF with biological markers. For power analysis, we used the Power and Precision software (version 4.0) by Biostat Inc. (
Results
Descriptive
There was no significant age difference between the DBDs and control groups (t = −1.74, df = 27, p = 0.1). However, gender ratios differ significantly (χ 2 = 7.7, df = 1, p = 0.005). None of the DBDs group was found to have a diagnosis of ADHD according to clinical evaluation, history, and Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime version interview.
Rating scale scores
The NCBRF scores were significantly higher in the DBDs group than in the control group (24.66 ± 9.52 vs. 2.37 ± 2.65, respectively, t = 26 df = −8.956, p ≤ 0.01). The Clinical Global Impression Scale-severity scores were also higher among the NADD participants (6.15 ± 1.21 vs. 1.0 ± 0, respectively, t = 27, df = −17.05, p ≤ 0.01). In contrast, the DAS rating scale scores were not significantly different between the two groups (12.58 ± 13.55 vs. 5.25 ± 4.94, p = NS). Controlling for age or gender did not change the results significantly (data not shown).
[3H]TBZOH binding
Analysis was performed for all but one subject from the NADD group and one from the control group due to technical reasons (Figs. 1 and 2). There was no significant difference between the DBDs and the control groups by either platelet VMAT2 density (Bmax): 856 ± 234 versus 831 ± 184 fmol/mg protein, respectively (t = −0.307 df = 25, p = 0.76) (Fig. 1) or affinity (Kd): 3.34 ± 0.69 versus 3.63 ± 0.56 nM, respectively (t = 1.197 df = 25 p = 0.24) (Fig. 2). Controlling for age or gender did not change the results significantly (data not shown).

Platelet VMAT2 density (Bmax) in patients with DBDs versus controls. t = −0.307, df = 25, p = NS. DBDs = disruptive behavior disorder; VMAT2 = vesicular monoamine transporter 2.
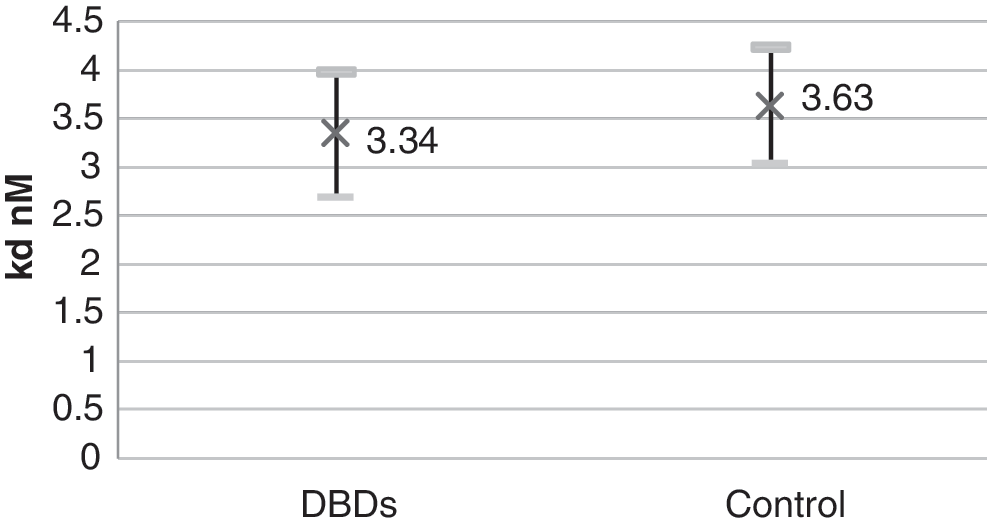
Platelet VMAT2 affinity (Kd) in patients with DBDs versus controls. t = 1.197, df = 25, p = NS.
Due to the small sample size, we were unable to perform an analysis of subgroups of the children with DBDs (i.e., ODD, CD). A larger sample is needed to address the question of whether these subgroups are different.
The calculated power for accepting the null hypothesis (no difference between groups) of this sample in alpha level of 0.05 is 93.9% (Cohen 1987). This result is based on 17% change in Bmax found in a similar sample size of ADHD cases (Toren et al. 2005), the reported Bmax means reported here, and two tailed analysis. No correlation was found between NCBRF scores and Bmax (data not shown).
Discussion
This study found no difference in either Bmax or Kd of the platelet VMAT2 between children with DBDs and healthy volunteers.
Based on these findings, we conclude that the formerly reported decreased platelet VMAT2 Bmax in patients with ADHD (Toren et al. 2005) may be specific to ADHD and not found in DBDs. This neurobiological difference between ADHD and the other DBDs may explain why changes in neurotransmitters found in aggressive patients and children with CD are not replicated (Berman et al. 1997; Coccaro et al. 1997; McBurnett et al. 2005). It may also provide an insight into the fact that methylphenidate and amphetamine that are very effective in ADHD are usually ineffective when the disruptive behavior disorders is not accompanied by ADHD as a comorbidity (Popma and Vermeiren 2008).
Limitations
The main limitation of this study is the relatively small sample size. However, since we found a difference in VMAT2 Bmax also in other studies with similar sample sizes (Zucker et al. 2002; Toren et al. 2005; Ben-Dor et al. 2007), it seems that the small sample size may be acceptable here as well. The calculated power seemed high (see Results section), yet a false negative finding cannot be disregarded. Another limitation is the use of platelet measurement rather than direct brain measurements that were obviously not possible in live children. We have, however, demonstrated that human platelets can be used as an accessible peripheral model for the brain VMAT2 (Rehavi et al. 1998; Zucker et al. 2001a, 2002). Thus, we may assume that our findings reflect the VMAT2 brain levels as well. It is highly recommended to replicate our findings in larger independent samples.
Clinical significance
Recent studies on non-human primates demonstrated the complexity of the neurotransmitter variations in ADHD (Gamo et al. 2010), suggesting that this disorder is biologically unique and treatment efficacy is well associated with the neurotransmitter imbalance. The known clinical difference and the neurobiological difference demonstrated in our study may raise again the question of whether the DBDs should remain together under the same subheading in the DSM-V or should they be separated into ADHD and DBDs. When developing new therapeutic strategies and medications, further studies should attempt to reveal biological correlates in patients with DBD with and without ADHD. In contrast to children with ADHD (Toren et al. 2005), no change occurred in VMAT2 in the children with DBDs, thus it seems that VMAT2 is not involved in the pathophysiology of DBDs. It is well established that children with ADHD benefit from treatment with stimulants that affect monoamine release and uptake (Gamo et al. 2010; Koda et al. 2010), whereas no benefit is usually gained from such treatment in children with DBDs (Popma and Vermeiren 2008). In the future, the possibility may exist for platelet VMAT2 to serve as a biomarker in predicting response to stimulants in children with ADHD (Toren et al. 2005) but not in children with DBDs.
Footnotes
Disclosures
All authors declare no conflict of interest with regard to this article.
Acknowledgments
The authors thank Michaella Gerchak for scientific and English editing. This study was partially supported by the Judie and Marshall Polk Research Fund for Children at Risk.