
Abstract
Objective:
To examine the persistence of three newly initiated stimulant preparations among Medicaid children and adolescents with attention-deficit/hyperactivity disorder (ADHD) diagnosis.
Methods:
A retrospective longitudinal claims analysis was conducted by using Medicaid analytical eXtract data of four states. The study focused on patients between 6 and 19 years of age with ADHD diagnosis and a stimulant prescription from January 2003 to December 2005. Stimulants were grouped into short-acting stimulants (SAS), intermediate-acting stimulants (IAS), and long-acting stimulants (LAS). Persistence was measured by totaling the number of days the patient remained on the index stimulant therapy from the index prescription date provided the refill gap between two consecutive stimulant claims was no more than 30 days. All the stimulant recipients were uniformly followed for 1 year (365 days). Survival time ratios (STR) were calculated by using accelerated failure time models to examine variation in index stimulant persistence for each stimulant class.
Results:
Among the 46,135 patients with ADHD continuously followed for 1 year, 8,260 were SAS users, 4,314 were IAS users, and 33,561 were LAS users. Children who received IAS medications had 4% shorter persistence (STR, 0.96 [95% confidence interval [CI], 0.93–0.98]) when compared with those who received SAS medications, whereas those who received index LAS medications had 29% longer persistence (STR, 1.29 [95% CI, 1.27–1.32]). Multivariate accelerated failure time models revealed that Blacks and Hispanics had consistently lower persistence than their counterparts. Foster care was positively associated with index stimulant persistence in the three stimulant types. Further, addition of another stimulant and other psychotropic medications significantly improved persistence of index stimulant in all three stimulant classes.
Conclusions:
LAS had comparatively longer persistence than other stimulants. An understanding of demographic and clinical characteristics that influence treatment continuation can help improve stimulant persistence rates in ADHD.
Introduction
Psychostimulants are the recognized first line of therapy for ADHD in children (Perrin et al. 2001; Pliszka and AACAP 2007). These are currently available in three different forms: Short-acting stimulants (SAS) or immediate-release (IR) formulations (4 to 6 hours); intermediate-acting stimulants (IAS) or sustained-release formulations (6 to 8 hours); and long-acting stimulants (LAS) or extended-release (ER) formulations (10 to 14 hours). Their differing half lives and resultant duration of action lead to different dosing schedules for the stimulants. SAS require multiple dosing, whereas, LAS are once-daily regimen and are relatively more convenient for administration. Initiating the treatment of ADHD with short–acting, intermediate acting, or long-acting psychostimulant medications is based on patient needs, risk/benefit of treatment, and clinical judgment of the clinician. The safety and tolerability of long-acting medications are similar to those of short-acting medications and may be associated with improvements in medication adherence due to their once-daily regimen and relative convenience of administration. Short-acting medications are less expensive and may allow for more flexibility with the dosing frequency and titration (Swanson 2003; Atzori et al. 2009). There is variation among physician speciality in terms of selection of the short-acting versus long-acting ADHD treatment. In addition, treatment selection is associated with age, with long-acting agents accounting for 78% of prescriptions for pediatric patients (age 0–17) but only 49% of prescriptions for adults (patients aged 18+) (Cascade et al. 2008).
Despite the distinctions in the pharmacokinetic profiles, stimulants' efficacy in treating the target symptoms of ADHD has been well documented (Swanson 2003; Olfson 2004; Faraone et al. 2006b). It has been estimated that 30% to 80% of youth with ADHD respond adequately to the first stimulant tried (Elia 1993; Goldman et al. 1998; Miller et al. 2004; Sanchez et al. 2005). However, the effectiveness of these medications in routine clinical care is realized only if an individual is persistent with the stimulant therapy. Once the pharmacological treatment is discontinued, the treatment benefits also disappear. Poor persistence with stimulants leads to suboptimal symptom management and has also been suggested as a precursor for negative long-term outcomes (Firestone 1982; Atzori et al. 2009). Hence, treatment guidelines and practice parameters indicate that treatment is required as long as the symptoms persist (Brown et al. 1986; Pliszka and AACAP 2007).
A review of past research examining persistence widely reported varying estimates. These can be mainly attributed to the different treatment settings and methodological differences in measuring persistence. In clinical research studies, persistence rates ranged from 53% to 81% after 1 year (Barkley et al. 1990; McBride 1998); 21%–70% at the end of 3 years (Charles and Schain 1981; Satterfield et al. 1981; Thiruchelvam et al. 2001; Jensen et al. 2007; Atzori et al. 2009); and 36% after 5 years (Charach et al. 2004). The retrospective, population-based studies reported much lower persistence rates: 59% continued medication until month 4, which fell to less than 50% in the next 2–6 months (Firestone 1982; Winterstein et al. 2007); and only 12%–43% persisted with the treatment for at least 1 year (Lage and Hwang 2004; Marcus et al. 2005; Sanchez et al. 2005; Winterstein et al. 2007). A limited number of studies identified the factors associated with persistence, namely younger age (Miller et al. 2004; Sanchez et al. 2005; Bokhari et al. 2008), gender (Thiruchelvam et al. 2001; Miller et al. 2004), race (Bokhari et al. 2008), absence of oppositional-defiant disorder (Thiruchelvam et al. 2001), receipt of initial prescription from a psychiatrist (Miller et al. 2004), presence of associated disorders, and not living with parents (Atzori et al. 2009). Only two studies accounted for the different stimulant formulations (Marcus et al. 2005; Sanchez et al. 2005). Both the studies concluded that the ER formulation of methylphenidate was associated with longer persistence than its IR form. Hence, this study examines the persistence of the three stimulant preparations in children and adolescents newly initiated with ADHD treatment in Medicaid. The results of this study could aid in the decision-making process targeted at improving the overall ADHD treatment persistence by understanding demographic, clinical, and medication-related factors that contribute to treatment persistence.
Methods
Design and data source
This retrospective longitudinal claims analysis used 3 years of Medicaid Analytic eXtract data (January 2003 to December 2005) from four states—Texas, New York, California, and Illinois. The study cohort was assembled from the personal summary (Medicaid eligible patient demographics, and eligibility outpatient), inpatient, other services, and prescription claims files. This study was approved by the University of Houston Institutional Review Board under the exempt category.
Study population
Patients with ADHD were identified on the basis of one or more stimulant prescription claims and at least one inpatient or outpatient claim involving a diagnosis of ADHD (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 314.xx) during the study period (Olfson et al. 2009; Winterstein et al. 2009). The fill date of the first stimulant claim was identified as the index prescription claim date. Patients newly treated or with incident ADHD were defined as those children and adolescents who had no previous stimulant drug prescription in the previous 6 months (Perwien et al. 2004). In addition, continuous Medicaid eligibility pre- and post-index date was required. The patients with ADHD had a uniform follow up of 1 year (365 days) from the index date. Inclusion into the study cohort also entailed receiving only one stimulant type of prescription on the index claim date. Thus, the final cohort included children with ADHD and adolescents (n=46,135) 6 to 19 years of age who initiated stimulant therapy anytime between July 1, 2003 and January 1, 2005. The study's sample selection process is outlined in Figure 1.
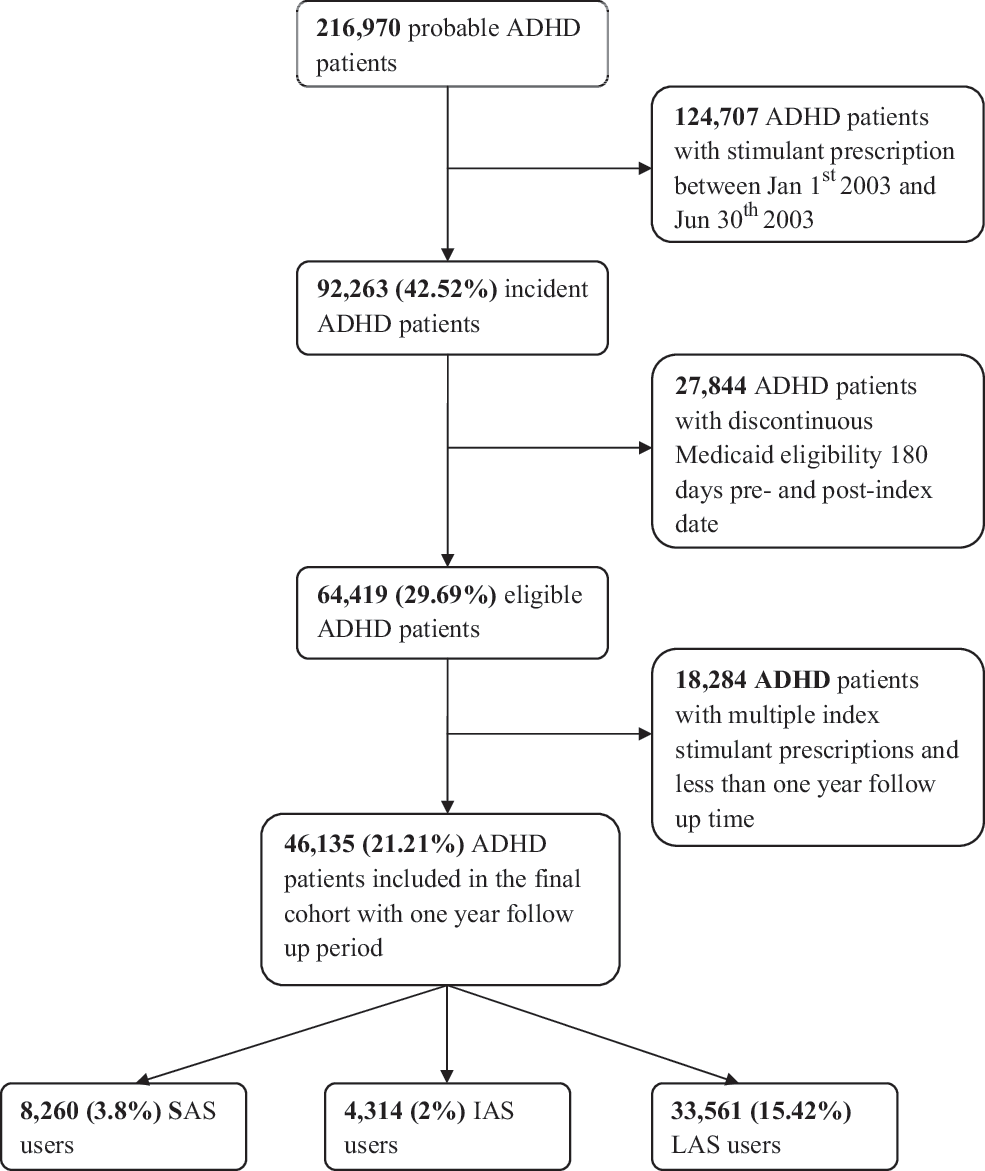
Flow-chart of ADHD study sample selection.
Based on the index stimulant type, the final ADHD population was grouped into three sub-cohorts: Patients who initiated stimulant drug treatment with SAS, IAS, or LAS. All subsequent analyses focused on the characteristics of these three stimulant types. National Drug Codes (NDC) were used to identify all the psychotropic claims of the selected patients with ADHD. For this study, psychotropic medications were defined as pharmacological agents typically used for treating behavioral and emotional disorders in children and adolescents (Chen et al. 2009). The American Hospital Formulary System classification was used to classify the drug classes into stimulants (SAS, IAS, and LAS), nonstimulants, α2-agonists, antidepressants, antipsychotics, anxiolytics/sedatives/hypnotics (ASH), mood stabilizers, and miscellaneous (see Table 1). When a prescription claim of a drug was refilled before the supply of its previous claim was exhausted, the overlapping claim's fill date was shifted to the end date of the previous claim (Leslie et al. 2008). This adjustment for a uniform drug supply was made only in the case of an overlap between two claims with the same NDC.
SAS=short-acting stimulants; IAS=intermediate-acting stimulants; LAS=long-acting stimulants; ER=extended release; SR=sustained release; CR=controlled release; SA=short-acting; XR=extended release.
Outcome measure
Persistence reflects the consecutive refill history during a treatment period and was measured in terms of days of therapy (Sanchez et al. 2005). Persistence for the index stimulant was calculated by summing the number of days the patient remained on the index stimulant therapy from the index prescription date. A maximum gap of 30 days was allowed between consecutive refills of the index stimulant (Marcus et al. 2005; Christensen et al. 2010). When the gap exceeded the permissible limit of 30 days, the treatment episode for the individual was terminated even if the individual was persistent with stimulant therapy at a later stage. The objective of the study was to examine the index stimulant persistence in terms of time to discontinuation of the index medication; Switching from one type of preparation within the stimulant class (e.g., LAS) was allowed, but switching to another class (e.g., from LAS to SAS) was defined as the discontinuation of the index stimulant.
Demographic and clinical covariates
Demographic characteristics included in the analyses were gender (male and female), age (6 to 12 years and 13 to 19 years), race/ethnicity (White, Black, Hispanic, and Other/Unknown), and state (New York, Illinois, Texas, and California). Age at the time of the index prescription claim was determined as the patient age. For beneficiaries with inconsistent information on race/ethnicity, sex, and age, the value during the index prescription year was assigned. In case of an “unknown/other” value, the individual's most repeated designation had a higher priority. Other cohort characteristics included their year of entry into the cohort, as well the season (autumn, winter, spring, and summer) during which the index stimulant prescription was received. In addition, factors such as foster care child benefits, temporary eligibility for needy families (TANF), and State Child Health Insurance Program (SCHIP) were included depending on their eligibility during the month of index date of stimulant prescription.
The psychiatric case mix of the population was characterized by the types and number of coexisting mental health conditions and recent inpatient psychiatric treatment. The presence of a medical claim during the study period was used to identify patients with the co-morbidity based on ICD-9-CM diagnoses code for the following mental health disorders: Depression (296.2, 296.3, 300.4, 309.0, 309.1 and 311), anxiety (300.0–300.2 and 313.0), bipolar disorder (296.0, 296.1, 296.4, 296.5, 296.6, 296.7, 296.8), oppositional conduct disorder (OCD [300.3]), oppositional conduct personality disorder (301.4), oppositional disruptive disorder (ODD [313.81]), conduct disorder (CD [312.xx]), learning disorders (315.0–315.3), psychosis and pervasive developmental disorders (290.xx, 293.xx, 295.xx), substance abuse and dependence disorders (303.xx–305.xx), enuresis (307.6, 788.3), encopresis (307.7, 787.6), and tics (307.2). Recent mental health hospitalization was a proxy measure for the severity or general mental health status of an individual. It was defined as an inpatient claim occurring within 180 days of the index prescription claim date with an ICD-9-CM diagnosis code for any designated mental health disorder (290.xx–319.xx) (Marcus et al. 2005). The first psychotropic medication different from the index stimulant and added before the end of persistent period was defined as the first concurrent psychotropic medication. This definition allows us to identify another stimulant medication type added to the therapeutic regimen if it was different from the index stimulant type.
Statistical analyses
Descriptive statistics were used to examine the various demographic, psychiatric disorders, and psychotropic drugs–related characteristics among three different types of stimulant preparations. The mean persistence along with 95% confidence interval (CI) and median persistence were calculated across three different types of stimulant preparations. Univariate and multivariate Accelerated Failure Time regression models based on the Weibull distribution were performed to examine variation in index stimulant persistence (Allison 2010; Marcus et al. 2005). Univariate analysis compared index stimulant persistence across three stimulant preparations. Separate multivariate analysis was performed for each stimulant preparation such as short-acting, intermediate acting, and long-acting stimulants. The model was adjusted for demographic characteristics, Medicaid eligibility, seasonal characteristics, psychiatric co-morbidities, concomitant psychotropic drug use, and recent history of mental health-related characteristics. In these analyses, the dependent variable was index stimulant persistence defined as time (number of days) to discontinuation of the index stimulant prescription. By exponentiating the resulting parameter estimate for the stimulant preparation group, the regression provided a ratio of the adjusted median time to discontinuation between groups or survival time ratios (STR). All statistical analyses were performed by using SAS version 9.2 (SAS Institute Inc., Cary, North Carolina) with a priori significance level of 0.05.
Results
Demographic characteristics
Figure 1 provides details of the cohort development and sample selection. A total of 216,970 children and adolescents had a clinician reported ADHD diagnosis as well as a stimulant prescription. Of these, 92,263 (42.52%) filled their first stimulant prescription between July 1, 2003 and June 30, 2005. After applying the additional inclusion criteria of uniform follow-up period of 1 year (365 days) from index stimulant prescription, a total of 46,135 patients were obtained. Approximately 73% (n=33,461) of this study cohort initiated ADHD treatment with LAS, compared with the 18% (n=8260) and 9.4% (n=4,314) who were SAS users and IAS users, respectively. Table 2 provides the demographic and clinical characteristics of children and adolescents initiating ADHD treatment with three different preparations of psychostimulant medications. Patients with ADHD with any stimulant prescription were primarily male (73.46%) and 6 to 12 years of age (83.30%). Among the stimulant recipients, almost 13.33% received foster care benefits, almost 18% received TANF benefits, and 2.10% received SCHIP benefits during the month of index prescription. Conduct and learning disorders were frequently reported co-morbid conditions in ADHD children and adolescents.
SAS=short-acting stimulants; IAS=intermediate-acting stimulants; LAS=long-acting stimulants; ADHD=attention-deficit/hyperactivity disorder; CI=confidence interval; ODD=oppositional disruptive disorder; CD=conduct disorder; OCPD=oppositional conduct personality disorder; TANF=temporary eligibility for needy families; SCHIP=State Children's Health Insurance Program.
Stimulant persistence
Table 3 provides the mean and median persistence (number of days) of the index psychostimulant prescription among children and adolescents with ADHD has been diagnosis. The average persistence was approximately 79.97 days (95% CI, 78.37–81.57) for SAS users, 76.59 days (95% CI, 74.50–78.68) for IAS users, and 104.96 days (95% CI, 104.02–105.90) for LAS users. In addition, median time to discontinuation was 52 days for the SAS users, 50 days for IAS users, and 72 days for LAS users during 1 year follow up from the index stimulant prescription. Children who received IAS medications had 4% shorter persistence (STR, 0.96 [95% CI, 0.93–0.98]) when compared with those who received index SAS medications, whereas those who received index LAS medications had 29% longer persistence (STR, 1.29 [95% CI, 1.27–1.32]).
SAS=short-acting stimulants; IAS=intermediate-acting stimulants; LAS=long-acting stimulants; CI=confidence interval; STR=survival time ratio.
Table 4 summarizes the results of the Accelerated Failure Time regression models. Several covariates were independently and significantly associated with index stimulant persistence in the three treatment groups of stimulant preparations after controlling for other factors. Race/ethnicity, age, year of entry into cohort, foster care, starting the index medication during autumn or winter, diagnosis of bipolar disorder or psychosis, and concurrent psychotropic drug use were found to be significantly associated with SAS-related persistence. The persistence of SAS among Black, Hispanic, and other/unknown racial and ethnic groups was found to be lower by 17% (STR, 0.83 [95% CI, 0.79–0.88]), 16% (STR, 0.84 [95% CI, 0.79–0.88]), and 11% (STR, 0.89 [95% CI, 0.81–0.97]), respectively, when compared with their counterparts. Children between 6 and 12 years of age were 14% (STR, 1.14 [95% CI, 1.06–1.22]) more persistent than adolescents in the 13 to 19 year age group among SAS recipients. Among SAS recipients, those who were in foster care were 15% (STR, 1.15 [95% CI, 1.07–1.24]) more persistent than those who were not in foster care. In addition, diagnosis of bipolar disorder or psychosis among recipients of index SAS was associated with increase in persistence by 105% (STR, 2.05 [95% CI, 1.04–4.01]). Further, addition of the medications from other psychotropic classes was associated with increase in persistence with SAS: IAS (23%); LAS (21%); nonstimulants (21%); α2-agonists (28%); antidepressants (26%); antipsychotics (32%); ASH (46%); and mood stabilizers (31%). In addition, there was also variation due to year of cohort entry and season during which the index medication had been started.
Significant at p=0.05.
SAS=short-acting stimulants; IAS=intermediate-acting stimulants; LAS=long-acting stimulants; CI=confidence interval; STR=survival time ratio; TANF=temporary eligibility for needy families; SCHIP=State Children's Health Insurance Program; ODD=oppositional disruptive disorder; CD=conduct disorder.
Among those initiating ADHD treatment with IAS, the Accelerated Failure Time regression analysis revealed a significant negative effect due to race/ethnicity, recent mental health hospitalization, and location of Texas on persistence of IAS. Hispanics and Blacks had on an average of 12% (STR, 0.88 [95% CI, 0.81–0.95]) lesser persistence as compared with their counterparts. The persistence was 8% (STR (0.92 [95% CI, 0.85–1.00]) lower in Texas than California. Persistence was significantly lower (14% STR (0.86 [95% CI, 0.76–0.98])) in those who made an inpatient mental health-related visit in the past months than in those without hospitalization. IAS recipients who were in foster care were 22% (STR, 1.22 [95% CI, 1.11–1.34]) more persistent than those who did not receive such benefits. Adding another psychotropic medication during stimulant treatment was found to be associated with increase in IAS-related persistence ranging from 22% with LAS to 50% with α2-agonist and anxiolytics. Among patients who initiated ADHD treatment with LAS, race/ethnicity, starting the index medication during spring, location of Illinois State, and diagnosis of bipolar disorder had a negative effect; whereas age, foster care, SCHIP benefits, number of co-morbidities, and addition of other psychotropic classes had a positive effect on persistence of LAS. The persistence of black, Hispanic, and other/unknown racial and ethnic groups was found to be lower by 15% (STR, 0.85 [95% CI, 0.82–0.87]), 14% (STR, 0.86 [95% CI, 0.84–0.88]), and 11% (STR, 0.89 [95% CI, 0.84–0.94]), respectively, when compared with their counterparts. In addition, diagnosis of bipolar disorder or psychosis was associated with a decrease in persistence by 28% (STR, 0.72 [95% CI, 0.51–1.00]). There was also variation due to state and season during which the index medication had been started. Children between 6 and 12 years of age were 12% (STR, 1.14 [95% CI, 1.09–1.16]) more persistent than adolescents in the 13 to 19 year age group among LAS recipients. Among LAS recipients, those who were in foster care were 17% (STR, 1.17 [95% CI, 1.13–1.21]) more persistent than those that were not in foster care. Further, addition of the medications from other psychotropic classes was found associated with an increase in the persistence with LAS: SAS (45%); IAS (44%); nonstimulants (19%); α2-agonists (35%); antidepressants (36%); antipsychotics (29%); ASH (45%); and mood stabilizers (25%).
Discussion
This study examined the index stimulant persistence of different stimulant preparations and their association with various demographic and clinical factors in children and adolescents newly started on ADHD treatment. Consistent with past literature, patients with ADHD who had started treatment with LAS continued taking their medication longer (105 days) than their counterparts who had initiated treatment with IAS (77 days) or SAS (80 days) (Pelham et al. 1999; Marcus et al. 2005; Sanchez et al. 2005; Christensen et al. 2010). In this study, those who had started with index LAS medications had significantly longer persistence, and those who had started with index IAS had significantly lower persistence than those who had started with index SAS medications. These differences can be attributed mainly to the pharmacokinetic profiles of the stimulant types (Marcus et al. 2005).
SAS have several limitations including shorter duration of action and fluctuating drug levels; whereas IAS are hindered by a long onset of action, inadequate plasma half life, and inconsistent effectiveness (Lage and Hwang 2004). As a result, both SAS and IAS need to be administered twice to thrice a day. However, most inconveniences can be reduced by the drug delivery profile of LAS (Swanson 2003; Lage and Hwang 2004). The LAS with their once-daily therapeutic regimen are, therefore, much simpler when compared with the dosing schedules of SAS and IAS. Further, a once-daily morning dose improves parental supervision and avoids the need for administration in public (school, college, or in the workplace). It circumvents the psychological and emotional problems associated with multiple daily dosing including social stigma (for being treated for a psychiatric condition in front of their peers), embarrassment (for being “different” from their peers), or poor self-esteem (Sleator et al. 1982; Swanson 2003; Lage and Hwang 2004; Marcus et al. 2005). Thus, the convenience and improved patient acceptance offered by LAS may account for their increased persistence compared with the other stimulant types.
Determining the factors associated with index stimulant persistence has important clinical and health policy ramifications. The Accelerated Failure Time analysis identified the association between various demographic and psychiatric case-mix variables and treatment persistence in the three treatment groups. Race/ethnicity, age, foster care, and concurrent psychotropic use were consistently found to be associated with persistence of index stimulants among the three stimulant groups. This study corroborates the findings of previous research that identified youths with ADHD of Hispanic, African-American, or other racial/ethnic origins to be at-risk population for early treatment discontinuation (Marcus et al. 2005; Bokhari et al. 2008). The differential effects observed between the various racial/ethnic groups may be attributed to varying response rates to the medication, although clinical evidence confirming this disparity is relatively sparse. Conversely, a study by dosReis et al. (2003) reported higher nonsatisfaction rates among parents of nonwhite children taking ADHD medication and indicated parental misconceptions and reservations as possible influential mechanisms. Further research is warranted to delineate the clinical and nonclinical effects, so that appropriate intervention strategies can be developed.
Consistent with previously published literature, younger children were positively associated with increased index treatment persistence of SAS and LAS (Miller et al. 2004; Marcus et al. 2005; Sanchez et al. 2005; Atzori et al. 2009). This may be due to heavy parental influence in the treatment decisions for preadolescents. Adolescents are also more prone to rebel against parental supervision and may opt to discontinue their medication (Sleator et al. 1982; Miller et al. 2004; Sanchez et al. 2005). Children in foster care had consistently higher persistence when compared with those who are not in foster care. The increase in persistence ranged from 15% to 22% among three stimulant preparations. This could be attributed to better monitoring and supervision by foster parents and case workers (Fontanella et al. 2011) or complexity/severity of disorders of children in foster care (American Academy of Pediatrics 2002)
Adding another psychotropic medication to the index stimulant treatment regimen had a positive impact on treatment continuity. Most importantly, addition of SAS or IAS to a therapy indexed on LAS increased the treatment duration with the latter by approximately 45% and 44%, respectively. This second stimulant (which is of shorter duration compared with the ER form) may have been added, as many individuals require a smaller second dose if only to sustain treatment benefits through the late afternoon and/or early evening (Swanson 2003; Adler et al. 2006). This may aid the children and adolescents in participating in after-school endeavors and also improve their concentration. It is also possible that “rebound” effects of the medication during the off-school hours may motivate the parents to administer medication after school. Improved behavior may be attributed to greatly improved patient persistence with LAS. However, addition of LAS to SAS or IAS treatment regimen did not produce such marked improvements in treatment continuity. Although our study design precluded us from identifying the true purpose of the concurrent stimulant, the findings by Christensen et al. may explain the current study's finding. Christensen et al. concluded that titrations, switches, and augmentation were more common for SAS or IAS forms than for LAS and switching occurred more often than augmentation. It is possible that after the initiation of stimulant therapy with SAS/IAS, gradual dosage titrations were made to identify the optimal drug/dose combination, after which a switch may have been made to LAS, and the index stimulant is gradually tapered off. This may partly elucidate why adding LAS to other treatment groups had a smaller effect on improving treatment continuity.
This study found that there is significant improvement on index stimulant persistence when other psychotropic drug classes (other than stimulants) were added in this group. For example, if the concurrent psychotropic drug class was atomoxetine, then treatment duration was higher by 19% to 30%; whereas in the case of a miscellaneous psychotropic, it improved by roughly 50%. A consistent positive association between addition of a concurrent psychotropic medication and persistence was also found in the three stimulant treatment groups. There are two possible reasons for the increased persistence (Greydanus et al. 2007). It is plausible that the second medication was added to manage severe ADHD cases or for co-morbid diagnosis associated with ADHD (Wilens et al. 2003; Adler et al. 2006; Comer et al. 2010). Several studies indicate that co-morbid psychiatric conditions are the strongest predictors of nonstimulant medication use in youth with ADHD (Boles et al. 2001; Guevara et al. 2001; Martin et al. 2003; Radigan et al. 2005). Clinical evidence supports such combined psychotherapy practices involving stimulants including clonidine (to ameliorate severe aggressive behavior in those with ODD or CD) (Hart-Santora and Hart 1992; Kemph et al. 1993; Connor et al. 1999, 2000; Greydanus et al. 2007); antidepressants (for co-morbid depression, moodiness, and OCPD) (Gammon and Brown 1993; Findling and Dogin 1998); and mood stabilizers (to treat coexisting bipolar disorder) (Biederman et al. 1999). This combined pharmacological approach possibly makes ADHD manageable, which, in turn, results in persistence with the index stimulants. Alternatively, it is also possible that the concurrent psychotropic medication was meant for managing treatment-emergent adverse effects or as an augmentation strategy in case of an insufficient response for preexisting symptoms (Wilens et al. 2003; Adler et al. 2006). Examples include clonidine for stimulant-induced insomnia or tics (Leckman et al. 1991; Wilens et al. 1994; Prince et al. 1996); α2-agonists; or ASH for modulating emotions and behaviors (e.g., anxiety, irritability) (Williams and Miller 2003). Further, patients with severe ADHD may require multiple psychotropic medications in addition to stimulants (Goldman et al. 1998; Preskorn and Baker 2002; Cooper et al. 2004; Kutcher et al. 2004; Zito et al. 2008). Therefore, the study finding supports the notion that a rational use of combined pharmacotherapy may indeed be beneficial to manage ADHD and its co-morbid symptoms as well as other coexisting mental health conditions when stimulant monotherapy does not result in desired outcomes.
Administrative healthcare claims databases offer several advantages such as large and diverse sample sizes, long follow-up, and availability of real-world clinical practice data. They are powerful tools for measuring treatment persistence. However, retrospective analyses of these databases are also associated with certain inherent limitations, as they are not primarily designed to address research questions (Iezzoni 1997). One such limitation is selection bias, as the study population was not randomized to a stimulant therapy. The database lacks certain key variables associated with the treatment regimen, such as severity of, and changes in, ADHD symptoms. Hence, unmeasured clinical and physician factors may have confounded the index stimulant persistence for each stimulant type. However, several demographic and clinical factors were controlled to adjust for the variation in each multivariate model for SAS, IAS, and LAS. The study assumes that the medication that is dispensed is actually taken by patients as prescribed and that the patients received no other psychotropic medication besides those available in the claims data (i.e., no out-of-pocket/outside health plan purchases). In addition, this study examined factors associated with persistence of each type of stimulant preparation such as SAS, IAS, and LAS rather than examining the persistence of overall psychostimulant therapy.
The study definition of maximum refill gap of 30 days does not account for extended drug holidays (e.g., summer). Therefore, our results may represent a conservative measure of persistence. Clinically appropriate treatment discontinuation could not be distinguished from premature treatment termination (e.g., lack of symptom alleviation and adverse events) (Miller et al. 2004; Marcus et al. 2005). Our study was limited to Medicaid beneficiaries from four states. The prescribing practices of Medicaid providers may also not be representative of those providers contracted under other types of health insurance programs (Shatin et al. 1998; Zito et al. 1998). So, the results may not be generalized to the whole ADHD population or specifically to the privately insured or uninsured patient populations. The data source provides broad classification for race and ethnicity; hence, the likely differences between the various groups could not be explored. Finally, diagnoses of ADHD and co-morbid mental disorders were identified based on diagnostic codes, and claim forms limit the number of diagnoses that can be documented (Birnbaum et al. 1999).
Conclusion
Successful disease state management requires continued treatment with stimulant therapy for overall better clinical outcomes in ADHD. The study found that LAS had comparatively longer persistence among the three index stimulant types possibly due to its simplified dosing regimen. This study also found significant variation in persistence due to race, age, and foster care consistently across the three index stimulant types. Further research is warranted to address clinical and nonclinical factors contributing to the variation so that appropriate intervention strategies can be developed. Addition of another stimulant or other psychotropic medications to the index stimulant therapy was found to significantly improve persistence. Although this finding supports the notion that a rational use of combined pharmacotherapy may be beneficial in terms of persistence, future research is needed to address long-term efficacy and safety of such practices considering the paucity of data on concomitant use. Overall, an understanding of demographic and clinical characteristics that influence treatment continuation can help improve persistence rates in ADHD.
Clinical Significance
Persistence of stimulant treatment in patients with ADHD is a significant concern. However, a few studies have characterized treatment persistence, especially across the different stimulant formulations with varying dosing regimen. This study found that children using LAS had significantly longer mean and median persistence than the SAS and IAS groups. Consequently, there is a need to start stimulant therapy with the LAS with their once-daily therapeutic regimen for convenience and improved patient acceptance. Although there is a concern in prescribing multiple psychotropic medications, the study found that persistence of index stimulants can be improved with addition of another stimulant type or psychotropic medication. These findings were consistent across the three stimulant preparations in children and adolescents newly initiated with ADHD treatment. For example, addition of SAS or IAS to children on LAS improved persistence, possibly, as adding a short/intermediate acting stimulant provides continued benefit for the remainder of the day. The study findings also revealed the benefits of adding other psychotropics for improved persistence of index stimulant therapy. This can be attributed to the value of the combined pharmacological approach for treatment-emergent adverse effects or as an augmentation strategy. Therefore, this finding supports the notion that a rational use of combined pharmacotherapy may be beneficial in managing ADHD and its co-morbid symptoms.
Footnotes
Disclosure
Swetha Palli, Pravin Kamblei, Hua Chen, and Rajender Aparasu declare no conflicts of interest or financial interests in any product or service mentioned in this article, including grants, employment, gifts, stock holdings, or honoraria.
Acknowledgment
The authors would like to thank Mrs. Golda Hallett for her help in editing a previous version of this article. No funding was received for this study.