
Abstract
Objective:
Methylphenidate (MPH) is commonly used to treat attention-deficit/hyperactivity disorder (ADHD) in all children, including those with velocardiofacial syndrome (VCFS). Yet concerns have been raised regarding its safety and efficacy in VCFS. The goal of this study was to examine the safety and efficacy of MPH in children with VCFS.
Methods:
Thirty-four children and adolescents with VCFS and ADHD participated in a randomized, controlled trial with a 2:1 ratio of MPH versus placebo. All subjects underwent a cardiological evaluation before and after MPH administration. The primary outcome measure was prefrontal cognitive performance following a single dose of MPH or placebo. A follow-up assessment was conducted after a 6-month treatment with MPH.
Results:
Compared with placebo, single MPH administration was associated with a more robust improvement in prefrontal cognitive performance, including achievements in the Hearts and Flowers executive function task and the visual continuous performance task. After 6 months of treatment, a 40% reduction in severity of ADHD symptoms was reported by parents on the Revised Conners Rating Scale. All subjects treated with MPH reported at least one side effect, but it did not necessitate discontinuation of treatment. MPH induced an increase in heart rate and blood pressure that was usually minor, but was clinically significant in two cases. No differences in response to MPH were observed between catechol-O-methyltransferase Met versus Val carriers.
Conclusion:
The use of MPH in children with VCFS appears to be effective and relatively safe. A comprehensive cardiovascular evaluation for children with VCFS before and during stimulant treatment is recommended.
Introduction
Despite their common prescription, very little has been published on the effectiveness and safety of psychiatric treatments such as stimulants in individuals with VCFS (Gothelf et al. 2003).
The use of methylphenidate (MPH) to treat the ADHD symptoms of children with VCFS and ADHD has raised several concerns. First, about 70% of children with VCFS have congenital cardiovascular anomalies and are therefore at possible increased risk for developing arrhythmias when taking stimulants (Vetter et al. 2008). Second, potential side effects of stimulants in the general population include psychotic and affective symptoms common in VCFS. Third, because individuals with VCFS have putatively higher prefrontal cortex (PFC) levels of dopamine due to catechol-O-methyltransferase (COMT) haploinsufficiency, concerns have been regarding the rationale of prescribing an agent that increases brain dopamine level in subjects with VCFS (Funke et al. 2001).
Despite these concerns, only one open-label study has been conducted to investigate the issues (Gothelf et al. 2003). This 4-week open study examined MPH treatment in 12 subjects who suffered from ADHD and VCFS. The treated subjects generally improved, and none of the subjects developed psychotic, manic, or hypomanic symptoms or had to discontinue MPH because of a major side effect.
In the present study, we sought to go beyond the previous one and conduct in-depth assessment of the effectiveness and safety of MPH, with the following aims: (1) To evaluate the efficacy of a single dose of MPH treatment compared with placebo in improving dopamine-dependent PFC cognitive functioning in children with VCFS and co-morbid ADHD, (2) to evaluate the effectiveness and long-term safety of MPH in a larger sample of children with VCFS than previously studied, and (3) to assess the moderator effect of COMT genotype on MPH dopamine-dependent prefrontal cognitive functioning and on the rate of side effects.
Methods
Subjects
Thirty-four children and adolescents with VCFS, 20 males and 14 females aged 5–20 years (mean age±SD: 11.1±3.7 years), were evaluated at the Behavioral Neurogenetics Center, Schneider Children's Medical Center of Israel. The diagnosis of VCFS was confirmed in all subjects using the fluorescent in situ hybridization test. The study protocol was approved by the Institutional Review Board of Rabin Medical Center, with informed consent obtained in writing from all participants and/or their parents or guardians.
Evaluation
Study subjects were randomly assigned to receive MPH (Ritalin®; Novartis Pharmaceuticals, Summit, NJ) or placebo in a 2:1 ratio. The primary outcome measure was change in prefrontal cognitive performance after a single dose of MPH or placebo. Subjects underwent cardiologic evaluation and prefrontal cognitive assessment immediately prior to taking the pill (MPH or placebo) and again after 90 minutes on the pill. MPH was prescribed at a weight-adjusted dose of 0.5 mg/kg, and the mean dosage prescribed was 15.7±5.6 mg. Children who had been previously treated with MPH (n=13, 38.2%) were washed out of stimulants for 3 days prior to the evaluation day. Follow-up psychiatric evaluation was conducted after 6 months of treatment for children who continued MPH treatment beyond the 1-day prefrontal cognitive testing.
Neuropsychiatric assessment
IQ was measured using the age-appropriate versions of WISC-III and WAIS-III (Caplan et al. 1997; Wechsler 1991). All subjects and their parents were interviewed by a child psychiatrist using the Hebrew version of the Schedule for Affective Disorders and Schizophrenia for School-Aged Children, Present and Lifetime (K-SADS-PL) (Kaufman et al. 1997; Shanee et al. 1997). In addition to the K-SADS-PL screening, the ADHD module of the K-SADS-Present was used. The module is comprised of 18 items from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) (American Psychiatric Association 2000) (9 for attention, 6 for hyperactivity, and 3 for impulsivity), with each ranked 0 (“not at all”), 1 (“sometimes”), or 2 (“often”). In addition, the Revised Conners Rating Scale (RCRS) was used at baseline and 6 months after treatment (Goyette and Conners 1978).
Medical assessment
All children were examined by a pediatric cardiologist and had echocardiograms. Electrocardiograms, heart rate, and blood pressure evaluations were conducted just before prescribing MPH and while on MPH.
Side effects
Potential MPH-induced side effects were assessed with the Barkley Side Effects Rating Scale (modified Hebrew version) (Berkley 1988). The scale was administered to the parents at 24 hours after MPH administration and 6 months later.
Prefrontal cognitive outcome measures
The cognitive battery included a Directional Stroop task (using Hearts and Flowers) (Diamond et al. 2007), Visual Continuous Performance Task (VCPT) (Kerns 1998), and Self-Ordered Pointing (Petrides and Milner 1982).
The Hearts and Flowers task
It taxes working memory, inhibition, and cognitive flexibility (Davidson et al. 2006). The task has three levels of difficulty: The congruent, incongruent, and mixed conditions, as has been previously described (Diamond et al. 2007; Kerns 1998; Petrides and Milner 1982; Davidson et al. 2006). In the congruent condition, participants are instructed to press on the same side as a red heart, which appeared for 1,000 milliseconds on the right or left of the computer screen; little or no executive function is required. In the incongruent condition, they are instructed to press on the side opposite that of a flower appearing on the right or left of the computer screen; inhibition of the natural tendency to respond on the same side as the stimulus is required. In the mixed condition, incongruent and congruent trials are randomly intermixed, requiring task switching. After practice, participants performed a block of 20 trials for each condition. Using a self-held button box, participants indicated their response for each stimulus. Responses of ≤200 milliseconds were excluded as being too fast to be in response to the stimulus.
Visual Continuous Performance Task
Participants watched various animals appearing on the computer screen (Kerns 1998, 2007). Eight animals were presented one at a time in pseudo-random order. Each participant was instructed to press a button whenever a horse appeared after a dog. Of the 156 stimuli presented, 30 were targets (a horse after a dog). In addition to reaction time, omission errors, and commission errors, d' values [z-score (False Alarms) − z-score (Hits)] were calculated.
The Petrides-Milner Self-Ordered Pointing Task
The task has three levels of difficulties—6, 8, and 12 lines of drawings (Collins et al. 1998; Diamond et al. 1997, 2004). After touching a picture, the screen refreshed, and then the pictures appeared in new locations.
Data analysis
t-Test was used for between-group comparison of Full Scale IQ (FSIQ) and RCRS scores. Paired t-tests were used for comparing RCRS scores before and after MPH. Prior to analyzing the Hearts and Flowers and self-ordered pointing task results, scores were Z-transformed. VCPT scores were transformed to approximate a normal distribution by assigning the normal distribution value to a proportion value, also known as the probit transformation. Univariate analysis of covariance (ANCOVA) was used to compare cognitive scores between groups. In all ANCOVAs, FSIQ, age, and gender were entered as potential covariates. The McNemar test was used for comparing rate of above chance scores on the mixed condition of the Hearts and Flowers task before and after MPH or placebo administration and for comparing the rate of side effects.
Results
Baseline neuropsychiatric profile
Twenty-eight subjects met the DSM-IV-TR criteria for ADHD—17 (50%) inattentive type, 11 (33.3%) combined type, and 6 (17.7%) ADHD-NOS. Subjects in the MPH (n=22) and placebo (n=12) groups were similar in mean age, FSIQ, gender distribution, severity of ADHD symptoms (RCRS scores), distribution of ADHD subtypes, and rate of psychiatric co-morbidities (Table 1). The psychiatric co-morbidities of the study sample consisted of oppositional-defiant disorder (ODD) (23.5%), specific phobia (26.5%), generalized anxiety disorder (GAD) and social phobia (11.8% each), dysthymic disorder (8.8%), and separation anxiety disorder (5.9%).
FSIQ=Full Scale IQ; RCRS=Revised Conners' Rating Scale 28 items.
Efficacy of single-dose MPH versus placebo in improving prefrontal cognitive functioning
There were no statistically significant differences between the MPH and placebo groups in any of the prefrontal cognitive measures at baseline. After a single dose of MPH, the following effects on PFC were detected.
Hearts and Flowers Task
On the congruent condition (which placed little or no demand on executive functioning), both groups performed well (91.4% and 93.9% correct in MPH and placebo groups, respectively), with no difference between groups after treatment (F=0.047, df=32, p=0.83). In the incongruent condition (which places a demand on inhibition), the standardized delta score of the MPH group was positive, indicating improvement in task performance, whereas the standardized delta score of the placebo group was negative. The difference in the standardized delta scores between the MPH and placebo group was statistically significant (F=4.7, df=30, p<0.05, ES=0.31) (Fig. 1). In the mixed condition of the Hearts and Flowers task (which requires task switching), only 50.0% subjects in the MPH group (11 of 22) and 58.3% subjects in the placebo group (7 of 11) scored above chance at baseline. After MPH administration, 77.3% of subjects scored above chance, and only 66.7% of subjects scored above chance after placebo (p=0.07).
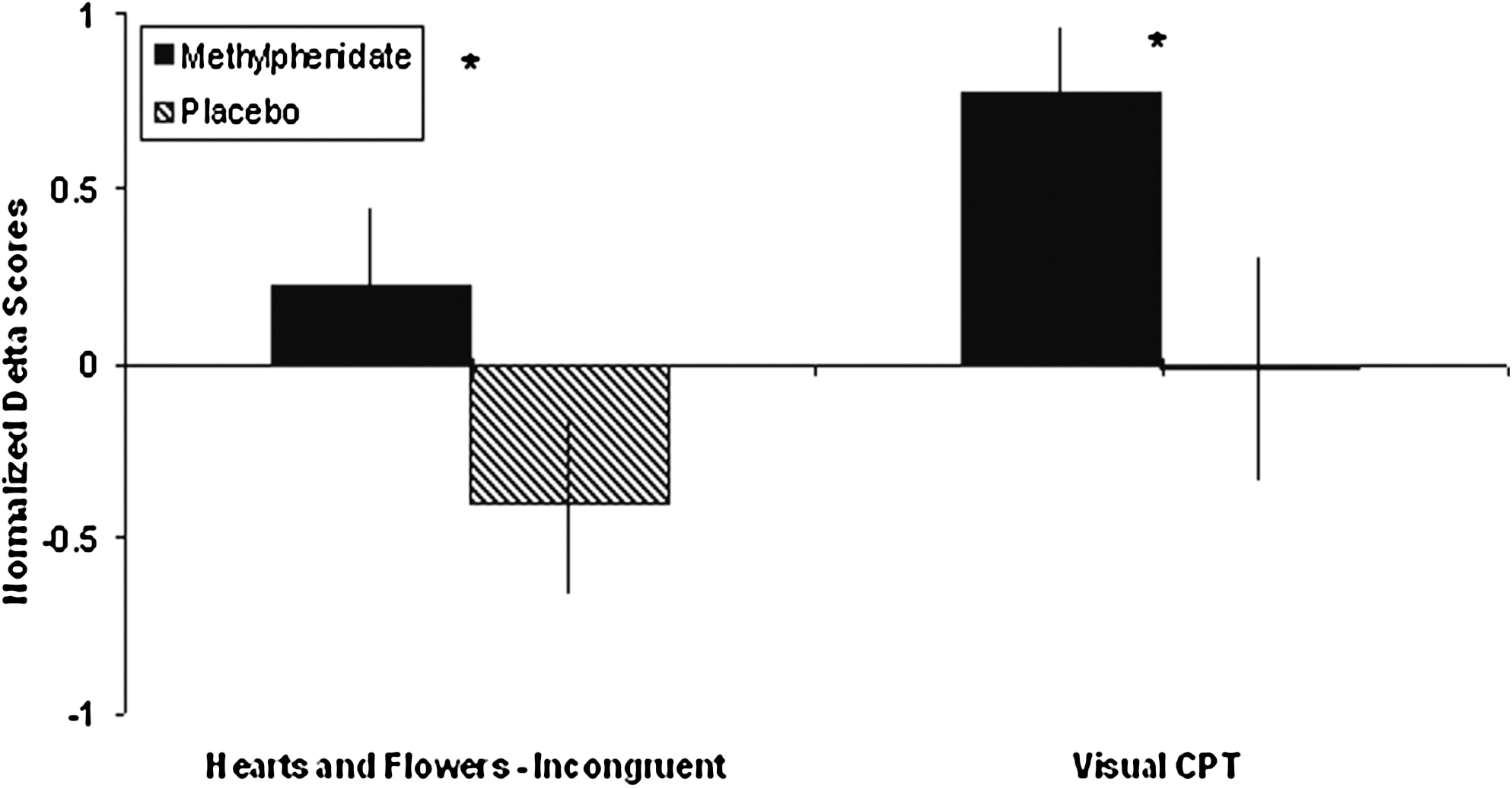
Change in prefrontal cognitive function following single-dose methylphenidate and placebo administration. The scores on the incongruent condition of the Hearts and Flowers task and Visual CPT (d') tests improved in the methylphenidate but not in the placebo group. Visual CPT: Delta sign was reversed to assure that positive sign indicates improvement.
Visual Continuous Performance Task
The d' values of the MPH group improved, whereas those of the placebo group deteriorated (F=4.8, df=31, p<0.05, ES=−0.38).
Self-ordered Pointing (SOP)
Change in performance on this task was minimal and similar in the MPH and placebo groups (F=0.1, df=31, p=0.71).
Clinical effectiveness of MPH
Of the 22 children who were prescribed MPH, 16 children continued MPH treatment beyond the 1-day prefrontal cognitive testing. Six children immediately discontinued following the 1-day testing, because the parents were apprehensive about the potential long-term side effects of the drug. One child discontinued treatment after 2 weeks because of poor compliance. The rest of the subjects, 15 children, continued MPH for the entire 6-month period of the study. Of the 15 subjects, 8 (53.3%) had a psychiatric co-morbidity, including specific phobia (n=4), ODD (n=4), GAD (n=3), and eating disorder not otherwise specified (n=1). None of the subjects was on any other psychotropic medication during the study period. Twelve subjcts completed the RCRS questionnaire. Overall, after 6 months of treatment, there was a significant improvement in ADHD symptoms, as reflected by the RCRS attention, hyperactivity, impulsivity, and total scores (Table 2).
RCRS=Revised Conner's Rating Scale 28 items.
Cardiac safety of MPH treatment
Of the 22 children who received MPH, 12 (54.5%) had congenital anomalies of the heart and great vessels, including Tetralogy of Fallot (n=3), ventricular septal defect (n=3), patent ductus arteriosus (n=2), asymmetric aortic valve (n=2), and anomalies in aortic arch (n=2). The respective values at baseline and 90 minutes after MPH administration were as follows: Diastolic blood pressure (60.6±8.4 vs. 64.6±6.9 mmHg, respectively, p<0.05), systolic blood pressure (108.1±11.2 vs. 108.7±7.9 mmHg, respectively), mean arterial pressure (76.3±7.0 vs. 80.5±7.1 mm Hg, respectively, p<0.05), and heart rate (82.4±13.5 vs. 87.9±17.8 bpm, respectively, p<0.05). There were no changes in QTc (0.40±0.015 vs. 0.40±0.019, respectively) and PR interval (0.13±0.017 vs. 0.13±0.017, respectively) measures. An increase in systolic blood pressure above the two standard deviation means (95th percentile) for age and height (National Institutes of Health 2005) and below the 99th percentile was observed in two boys. None of the children exhibited tachycardia (age adjusted) after MPH administration.
MPH-associated side effects
The rates of side effects within 24 hours and within 6 months after initiation of MPH treatment are shown in Table 3. Overall, MPH treatment was well tolerated, and none of the subjects discontinued medication because of a side effect. As seen in Table 3, immediate side effects tended to persist, reflected by similar “immediate” and “6 months after” rates for all side effects. The most common side effects after 6 months of treatment included poor appetite (93.7%), headache (66.6%), and stomachache (56.2%). None of the patients exhibited psychotic symptoms, or manic, hypomanic exacerbation during the 6-month study period.
Side effects were present in at least 25% of the subjects.
Effect of MPH on prefrontal cognitive functioning and on occurrence of side effects by COMT genotype
There was a significant difference between the COMT Met (n=12) and COMT Val (n=10) subgroups in the change in performance on the Hearts and Flowers task—congruent condition. The COMT Val subgroup performance on this task improved, whereas the Met variant performance deteriorated (F=4.8, p<0.05, ES=0.39) following MPH administration. There were no other statistically significant differences between the COMT Met and COMT Val subgroups on any of the other PFC cognitive test scores.
The COMT Val subgroup also had significantly higher rate of sadness/unhappiness in response to MPH treatment (8 subjects vs. 2 subjects, respectively, p<0.05). No differences were noted between COMT Met and Val subgroups in the rate of other side effects or in the cardiovascular measures.
Discussion
Although ADHD is the most common psychiatric disorder in children with VCFS (Aneja et al. 2007; Green et al. 2009), there are very limited data on the safety and efficacy of treatment with stimulants in this population (Gothelf et al. 2003). This is the first study using a cognitive prefrontal battery and a placebo comparison group to evaluate the efficacy of single MPH administration and the first study examining the safety and effectiveness of continuous (6 months) MPH treatment in individuals with VCFS. Overall, we found continuous MPH treatment to be effective and safe in treating ADHD symptoms in children with VCFS.
Single dose of MPH versus placebo administration
We found that the prefrontal cognitive functions—inhibitory control, working memory, and cognitive flexibility—improved more in subjects with VCFS treated with a single dose of MPH than in those given placebo. These differences were noted on the Hearts and Flowers task (incongruent condition and mixed conditions) and on the VCPT task. Disinhibition and impairment in cognitive flexibility (perseveration) are prominent cognitive deficits in individuals with VCFS (Antshel et al. 2008; Lajiness-O'Neill et al. 2006; Woodin et al. 2001). Deficits in inhibitory control and perseveration are also common in non-VCFS children who suffer from ADHD (Willcutt et al. 2005). These deficits have been shown to respond to MPH treatment in non-VCFS children (O'Driscoll et al. 2005). To our knowledge, this is the first study demonstrating inhibitory control improvement following single MPH administration in children with VCFS.
On the SOP task, there were no differences between the MPH and placebo groups, as expected. This is in line with the findings of Diamond et al., replicated by others (Collins et al. 1998; Diamond et al. 1997, 2004), showing that tasks taxing both working memory and inhibition (i.e., the Hearts and Flowers task and the VCPT) are dopamine dependent, whereas tasks taxing only working memory (i.e., the SOP) are insensitive to PFC dopamine levels.
Continuous MPH treatment
We found MPH treatment to be clinically effective and safe during the 6-month study period. Following 6 months of treatment, there was a mean 40% reduction in severity of ADHD symptoms reported by parents on the RCRS overall index. A similar magnitude of effect of MPH on ADHD symptoms has been reported in non-VCFS children with ADHD (Schachter et al. 2001).
One of the most common psychiatric disorders in children with neurogenetic syndromes is ADHD (Rowles and Findling 2010). Yet there are very few reports on safety and effectiveness of stimulant treatment in children with neurogenetic syndromes. On VCFS, there is only one 4-week open label study demonstrating MPH effectiveness for ADHD symptoms (Gothelf et al. 2003), and on fragile X syndrome, there is one controlled trial demonstrating a 66% response rate to MPH (Hagerman et al. 1988). On Williams syndrome, there are only two publications on stimulant treatment, consisting altogether of six patients (Bawden et al. 1997; Power et al. 1997). To our knowledge, there are no studies on stimulants use in Prader-Willi and Down syndromes.
Safety and side effects profile
We found that all subjects (100%) with VCFS treated with MPH exhibited at least one side effect. This high rate of MPH-induced side effects may be related to haploinsufficiency of the COMT gene, associated with excess presence of dopamine in VCFS-ADHD children, following MPH treatment. Nevertheless, MPH seems to be relatively well tolerated, as none of the treated children had to discontinue MPH because of a side effect. None of the subjects developed psychotic symptoms or a medical emergency following initiation of MPH or at the 6-month follow-up.
The most common side effects observed were poor appetite, headache, stomachache, and depressive symptoms. The rate of all side effects immediately observed following initiation of treatment remained similarly high after 6 months of treatment. Thus, according to our findings, it seems that in children with VCFS, tolerance did not develop to MPH side effects. Similarly, in non-VCFS children, stimulant-induced side effects, especially loss of appetite, persist even 5 years after initiation of treatment (Charach et al. 2004).
In line with our previous study (Green et al. 2009), we found in this study a high rate (∼40%) of emergence of depressive-like side effects. As noted by previous studies, the depressive symptoms may reflect a predisposition of children with VCFS to develop depressive disorders (Green et al. 2009; Jolin et al. 2009). We also found differences in the COMT Met and Val subgroups: The COMT Val subgroup had significantly higher rates of sadness/unhappiness in response to MPH treatment. This finding is in line with the recent report of higher scores of anxiety and depressive symptoms in VCFS children carrying the COMT Val allele (Shashi et al. 2006).
Cardiovascular safety
In this study, we also performed in-depth evaluation of the cardiac safety of single MPH administration in VCFS. Following single MPH administration, we found a minimal increase in mean heart rate and diastolic blood pressure, which is in line with cardiovascular changes occurring in non-VCFS children (Ballard et al. 1976). For children with no compromised left heart function, these cardiovascular changes are relatively minor (Silva et al. 2010). However, in children with cardiological malformations associated with a potential compromise of left heart function, which is not common in children with VCFS, such cardiovascular changes need more careful attention (Nissen 2006). In two children we found a clinically significant increase in systolic blood pressure following single MPH administration.
We therefore recommend comprehensive cardiological evaluations for all children with VCFS prior to and also following the initiation of a stimulant medication. Prior to initiation of a stimulant medication we recommend clinical evaluation by a pediatric cardiologist, that would include echocardiogram and electrocardiogram. We also suggest measuring heart rate and blood pressure evaluations before and following initiation of a stimulant medication. In those cases with clinically significant cardiovascular effects of MPH (e.g., MPH-induced systolic hypertension), further testing (e.g., 24-h ambulatory blood pressure monitoring) should be considered (Vetter et al. 2008; Samuels et al. 2006).
COMT genotype and MPH effect
We did not find that MPH's effect on PFC functioning was related to the COMT Met or Val genotype. Overall, MPH was equally effective for VCFS COMT Met and Val carriers. It may be because our sample size was not large enough to detect small differences in response to MPH that may discriminate the COMT Met and COMT Val subgroups. Alternatively, our findings suggest that although MPH increases PFC dopamine (Balcioglu et al. 2009) levels, it does not negatively affect these functions even in those subjects with putatively high levels of PFC dopamine (i.e., VCFS COMT Met carriers).
Limitations
The placebo-controlled first part of the study indicates efficacy of single MPH administration on PFC functions after 90 minutes. Longer administration of treatment is required to assess long-term cognitive effects of MPH treatment. In addition, our sample size was relatively small, although the largest sample to date of psychiatric treatment studies in VCFS. The sample size limited our ability to detect differences between MPH and placebo groups and between the COMT Met and COMT Val subgroups. A placebo-controlled crossover design would be of value in further MPH studies in this population. Moreover, although MPH was found to be relatively safe for use in VCFS children, the prevalence of the most severe complications is low and may not be captured by this small sample size.
Conclusion
The use of MPH in children with VCFS appears to be effective and relatively safe. In a single administration, compared to placebo, MPH had a positive effect on dopamine-dependent PFC functions in children with VCFS. The chronic use of MPH in children with VCFS and ADHD was found safe during the 6-month follow-up period.
Clinical Significance
This study shows that MPH is effective, relatively safe, and well tolerated in children who suffer from VCFS with comorbid ADHD. Because we observed an increase in blood pressure and heart rate following single MPH administration, which in some cases can be clinically significant, we recommend a comprehensive cardiological evaluation for all children with VCFS prior and also following the initiation of stimulant medication.
Footnotes
Disclosure
Dr. Tamar Green, Ms. Ronnie Weinberger, Dr. Adele Diamond, Dr. Michael Berant, Ms. Leora Hirschfeld, Dr. Amos Frisch, Mr. Omer Zarchi, Dr. Abraham Weizman, and Dr. Doron Gothelf have no institutional or corporate/commercial relationships for the past 36 months that might pose a conflict of interest.
Acknowledgments
This work was done at the Behavioral Neurogenetics Center, Schneider Children's Medical Center of Israel. Statistical expertise was provided by Dikal Geva (IntegriStat, Tel Aviv, Israel). The authors are grateful to Harriet Sugar Miller for editorial assistance.