
Abstract
Background:
Antidepressant (AD) dispensing for depression in youth declined in the years following the 2003–04 Food and Drug Administration actions regarding increased risk of suicidal behavior.
Objective:
To extend observation of youth AD dispensing and associated characteristics through 2009 to determine if AD dispensing continues to decline, has stabilized, or has rebounded.
Design:
Retrospective time series design. Sample: Youth (n=57,782) ages 10 to 17 inclusive.
Results:
Both new (incident) and refill AD dispensing continued to decline through 2009, with no sign of leveling off. However, among youth who started AD treatment the cumulative supply of AD medication remained consistent across the pre- and postperiods, suggesting that cumulative treatment episode duration has not been degraded—possibly as a function of greater days supply with each new refill in the postperiod. Prescribers dramatically curtailed preauthorized refills in the postwarning period.
Conclusion:
Declines in AD dispensing to depressed youth may not reflect less intensive treatment for those youth who persist beyond the initial dispense. Lower rates of preauthorized refills may have been an attempt by prescribers to encourage return visits to evaluate response and adverse consequences.
Introduction
Following the FDA actions several reports have described significant declines in AD dispenses to youth compared to historical trends, in many cases not accompanied by increases in rates of nonpharmacological treatments (Murray et al. 2005; Thomason 2006; Libby et al. 2007, 2009; Katz et al. 2008; Harman et al. 2009; Busch et al. 2010). Concerns have been raised that this might represent potential undertreatment of depression and lead to unintended, negative public health impacts (Brent 2004; Richmond and Rosen 2005) especially as several community epidemiology reports suggest that increased population use of ADs has been associated with reduced community suicide rates (Olfson et al. 2003; Valuck et al. 2004; Bridge et al. 2005; Isacsson et al. 2005; Gibbons et al. 2006; Hall and Lucke, 2006; Milane et al. 2006; Simon et al. 2006). More studies are needed to clarify whether declines in AD dispensing continue, and if so, whether this represents true undertreatment. The most recent published reports examine AD dispensing trend only through mid-2007 (Kurian et al. 2007; Libby et al. 2007 , 2009; Olfson et al. 2008) and it is unclear whether AD prescribing has leveled off (Nemeroff et al. 2007), continues to decline, or has started to increase again, as was the case prior to 2003.
Several other aspects of this phenomena merit additional study. For example, few reports have clarified how these population-level declines manifest in the course of typical AD treatment episodes for individuals. Are population-level reductions in AD dispensing a result of fewer youth being treated, shorter duration of AD treatment episodes, or some other explanation? Therefore, in this report of youth AD dispensing trends through 2009 in a not-for-profit health maintenance organization (HMO), we examined whether total population level declines in AD prescriptions can be explained primarily as a function of fewer new “starts” of medication treatment episodes (fewer treated youth), more rapid discontinuation of existing AD treatment episodes (shorter episodes of care), and/or changes in days supply of medication per refill (fewer but larger refills). Any of these alone or in combination might lead to a similar pattern of fewer total refills. We also examine trends in the number of “refill limits” associated with first dispenses (allowable refills without prescriber reauthorization), in case this was also associated with any detected changes in AD prescribing.
Methods
Sample
The sampling frame for this study was the membership of a large, not-for-profit HMO in the Northwestern United States from July 1999 through December 2009, inclusive. The HMO membership totaled 454,542 persons at the end of 2009, of which 57,782 (12.7%) were of ages 10 to 17 inclusive—the age range for this investigation. We did not examine dispenses for children younger than age 10 because our prior research indicates low rates of AD prescriptions for prepubertal children (DeBar et al. 2000, 2001). The mean age of youth at first incident AD dispense was 14.83 years (SD=1.88). Data were available for an average of 5.64 years (SD=2.37) for each youth, with a mean of 1.80 years of data (SD=1.60) for each participant following first incident AD dispense. The total sampling frame was 390,594 life years (sum of each individual's years of observation). The sample was 63.49% female. Race/ethnicity data available were recorded in the electronic medical record (EMR) for 47.3% of participants, of which 4.4% were Hispanic, 2.6% Non-Hispanic African American, 4.1% Non-Hispanic other minority race, and 88.9% Non-Hispanic White.
We limited our case-finding to the 94% of HMO members with pharmacy benefits. We allowed gaps in HMO enrollment of up to 3 months. We excluded a small number of individuals registered in our research center's “do not contact” list. For the primary results reported here we included only those youth who were dispensed ADs and had an associated EMR-recorded diagnosis of unipolar depression or a related mood condition. We included International Statistical Classification of Diseases and Related Health Problems, version 9 (ICD-9) diagnoses shown in Table 1, which we refer to hereafter as “mood diagnoses”. We included the less specific of these diagnostic codes (such as depression not elsewhere classified, 311; atypical depressive disorder, 296.82) because these codes are regularly employed by HMO primary care providers who in brief encounters may lack sufficient information to discern more exacting diagnostic distinctions, such as between major depression and dysthymia (DeBar et al. 2000, 2001). The HMO Human Subjects Committee approved all study procedures of this retrospective, data-only investigation.
The 5th digit “x” indicates that all values in this field were included; for example, 296.21. 296.22, etc.
International Statistical Classification of Diseases and Related Health Problems, version 9 (ICD-9).
EMR system
Since 1997 this HMO has had an EMR, which stores all clinical information for each member. ICD-9 codes are embedded in the diagnosis selection screen for immediate coding of medical conditions into problem lists and encounters, and clinicians electronically enter all patient orders. These data and the problem list allow us to identify all noted or treated outpatient diagnoses. Membership records include each member's gender, date of birth, race and ethnicity, and dates the member joined and left the health plan due to disenrollment or death. Group codes also identify Medicare and Medicaid members. The linked outpatient pharmacy database records all prescriptions dispensed by HMO outpatient pharmacies, including dose, agent, days supply, formulation, etc. Historically, 90% to 95% of members filled their prescriptions at HMO pharmacies (Freeborn and Pope 1994); interim data from an ongoing clinical trial confirm that this is still so (Clarke 2011).
AD dispensing
We extracted pharmacy data to identify youth with one or more dispenses of any AD that were eventually included in the FDA warnings. Medications included all dosage levels and formulations of amitriptyline, amoxapine, bupropion HCl, chlordiazepoxide/amitriptyline, citalopram hydrobromide, clomipramine, desipramine HCl, doxepin, duloxetine, escitalopram oxalate, fluoxetine HCl, fluvoxamine maleate, imipramine pamoate, imipramine, isocarboxazid, maprotiline, mirtazapine, nefazodone HCl, nortriptyline, olanzapine/fluoxetine, paroxetine HCl, paroxetine mesylate, perphenazine/amitriptyline, phenelzine sulfate, protriptyline, quetiapine, selegiline, sertraline HCl tranylcypromine sulfate, trazodone HCl, trimipramine, and venlafaxine HCl. Of all these medications only fluoxetine (Prozac) and escitalopram (Lexapro) have FDA indications for depression in minors. All other listed AD medications would be “off label” when used with children and adolescents. Selective serotonin reuptake inhibitors (SSRIs) were the dominant AD class (79.3% of all dispenses). Because all AD classes other than SSRIs were prescribed relatively infrequently (0.2% to 7.3% for each nonSSRI group) we did not conduct separate subanalyses.
We classified dispenses as either an initial (“incident”) dispense in a new episode of care with no dispenses of medications of the same class in the previous 6 months, or as a refill of the same agent or another medication within the same drug class, to allow for switching within the same episode of care. Initial dispenses generally consisted of 30 days supply of medication. Among incident dispenses 52.4% were categorized as low dose (e.g., 10 mg fluoxetine or equivalent; (Weilburg et al. 2003; Robinson et al. 2006) typically meant to titrate slowly upward, 43.0% of starting doses were mid-range (e.g., 20 mg fluoxetine or equivalent), 1.9% of initial dispenses were in the high range, and 2.8% were of unknown dose. Tapering of dose was accounted for in our calculation of days supply. Therapeutic dose was calculated using the dose at the beginning of the titration period.
Days supply
We examined cumulative days supply of dispensed medication in the 6 months following the initial new dispense; for example, the start of a new episode of pharmacotherapy. A small number of youth take ADs for longer than 6 months; however, we anticipated that any changes in days supply of medication associated with the FDA actions would be evident in the first 6 months of each pharmacotherapy episode. For each of the first 6 months we also classified youth as “covered” if they had medication in possession for any portion of that month. Cumulative days supply was calculated by combining multiple fills when the patient refilled their medication. Patients who switched from one AD to another, or titrated from a low starting dose were included in the calculation but were not separately analyzed. Excess supply from a previous dispense was included in the calculation if a patient refilled prior to exhausting their supply. A maximum cumulative gap of 15 days was allowed in the days supply calculation.
Preauthorized refills
HMO prescribers are able to authorize additional refills (none, 1, 2, or more) at the time of the initial dispense. We examined the number of preauthorized medication refills at the time of the initial AD dispense for changes over time. We elected to examine this factor based on anecdotal reports suggesting that prescribers were limiting these refills after the FDA actions.
Analysis plan
We employed an interrupted time series approach to examine changes in the slope of each event of interest before and after the key transition event. Data were aggregated to the monthly level. We employed SAS versions 9.1 and 9.2 and used “Proc Autoreg” for the segmented (interrupted) regression. Although the earliest communication about ADs was issued in June 2003, the black box requirement was not implemented until October 2004. Within this HMO the pharmacy therapeutics committee issued several internal email communications regarding AD safety to prescribers beginning in July 2003. Therefore, we selected October 2003 (the date of the first FDA warning) as the key interruption point, for consistency with the time frame used in earlier reports (e.g., Libby et al. 2007, 2009). For all comparisons of pre- and postinterruption point changes we separately examined for immediate discontinuous change (e.g., significant increase or decrease right at the interruption point) and significant differences in slope of events for approximately 4 years prior and 6 years after the interruption point. Similar to other reports (e.g., Libby et al. 2009) we examined all AD dispensing among youth with a unipolar depression diagnosis and related disorders, as these are both the most common AD indication. However, we examined diagnosis rates among the entire youth membership (Fig. 1) because this was the appropriate denominator to detect population-wide diagnostic changes.
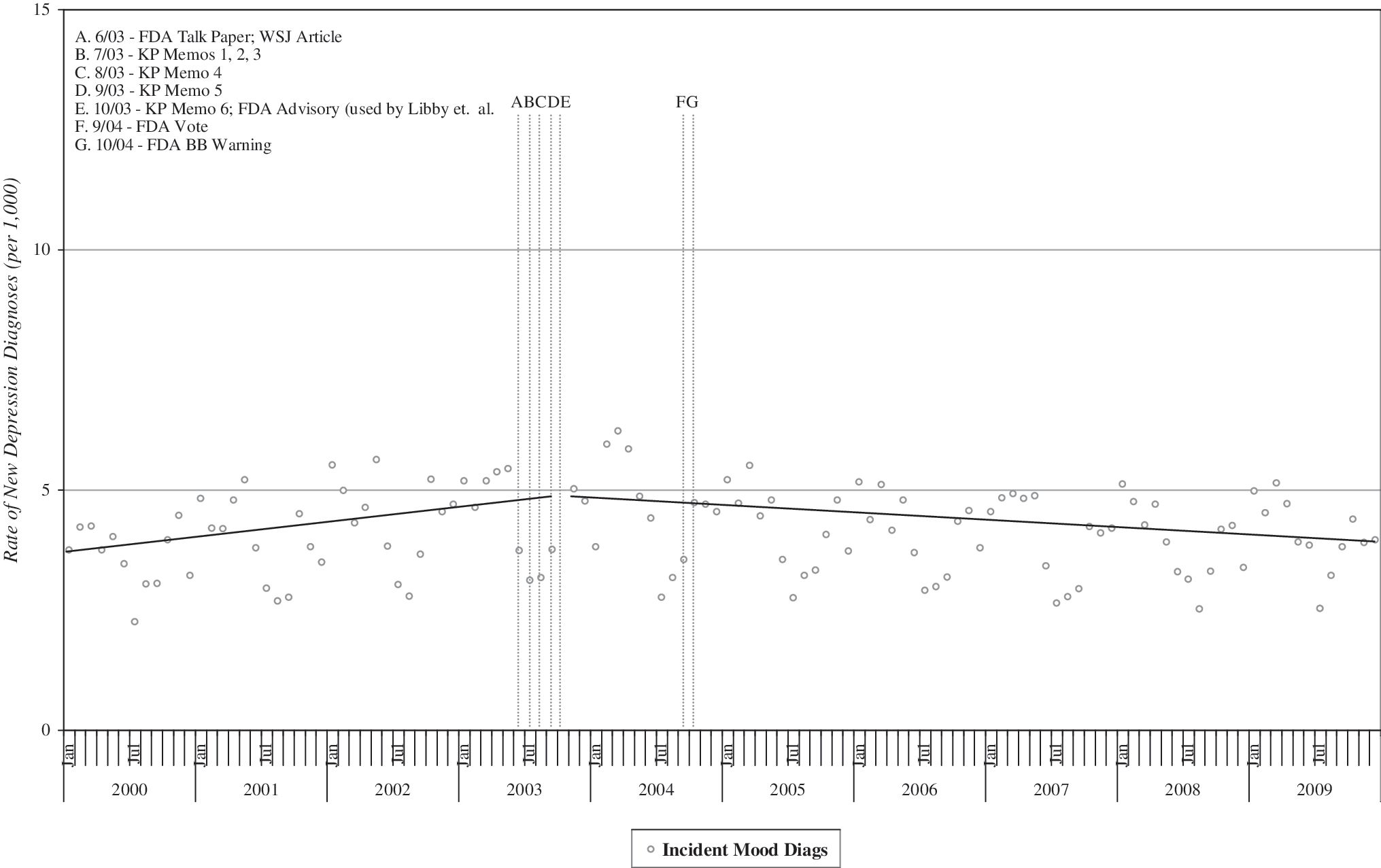
Rate of incident unipolar depression and related mood diagnoses, per 1,000 youth enrolled in the healthplan.
Results
Table 2 presents the results of interrupted time series models for the several diagnostic, AD dispensing, and dispense characteristics examined in this report.
AD=antidepressant; DX=diagnosis.
Unipolar depression and related diagnoses
Declining AD dispensing may be a function of changes in rates of diagnoses for which this treatment is commonly prescribed. Therefore, we began by examining rates of new or “incident” unipolar depression and related diagnoses (Table 1). “Incident” diagnoses were defined as those with no instance of these diagnoses recorded in the EMR in the previous 6 months. We observed no significant discontinuous change at the interruption point (Fig. 1), but a significant reversal in slope (p<0.001) with rising diagnosis rates prior to the interruption point and declining rates after (Table 2).
AD dispensing
Figure 2 presents the rates of initial, refill, and total AD dispenses per 1,000 youth with mood diagnoses, and the trend lines for the periods before and after the interruption point. We found significant immediate declines of initial dispensing only for new (incident) dispenses (p<0.05). However, we did find a significant reduction in slope from pre-to postinterruption (p<0.0001) for all 3 dispense types. Visual inspection of the curves does not suggest any leveling off of the declines in the final year (2009) of the observation window.
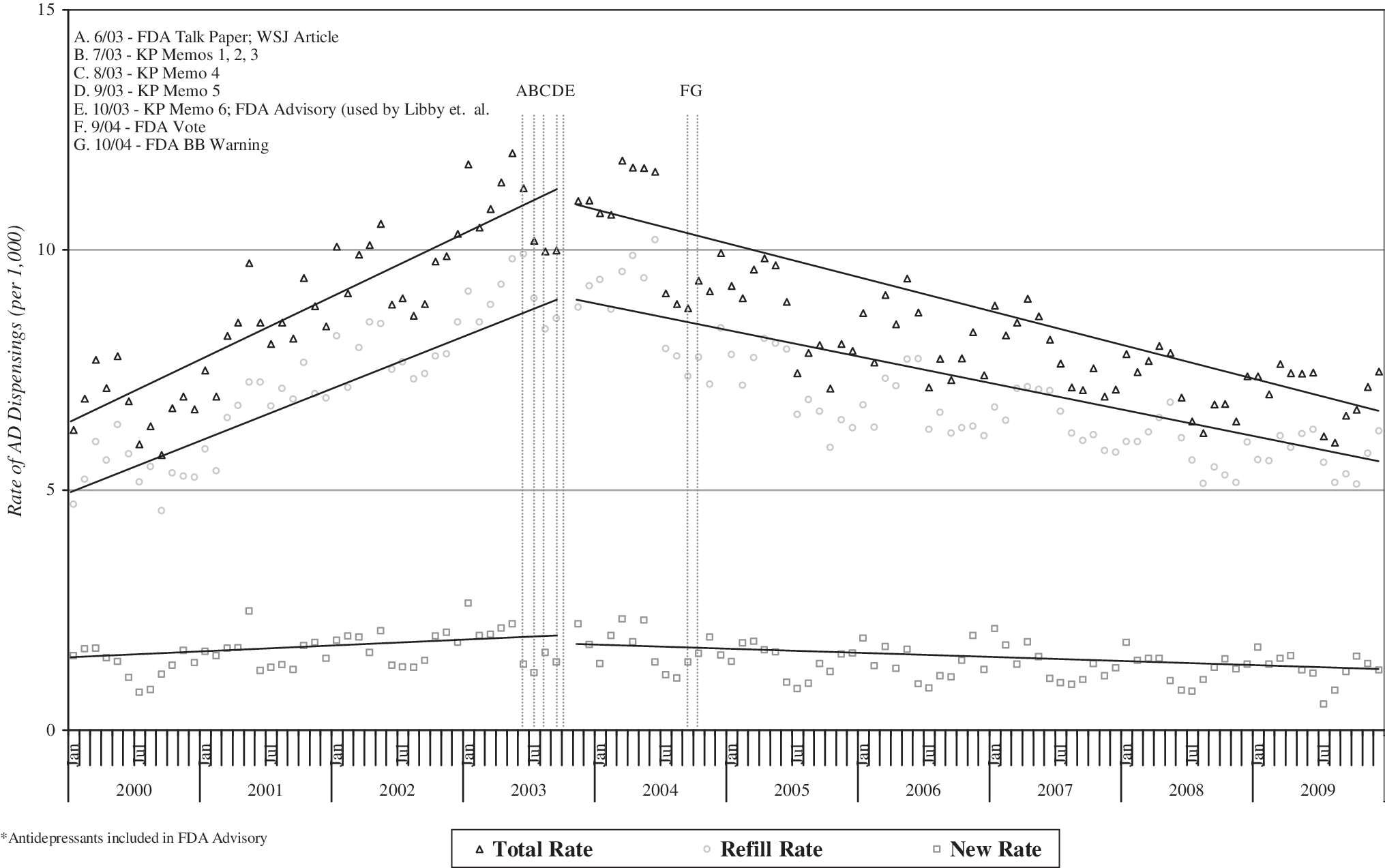
Rate of antidepressant (AD) incident, refill, and total dispensing, per 1,000 youth with unipolar depression and related mood diagnoses.
Initiation of pharmacotherapy
Figure 3 displays the percentage of youth with an incident diagnosis who were dispensed an AD within 30 days, indicating timely initiation of appropriate pharmacotherapy soon after a relevant disorder was diagnosed. We observed both a significant immediate drop-off after the interruption point (p<0.0001) and a significant reduction in slope from pre to postinterruption (p<0.0001).
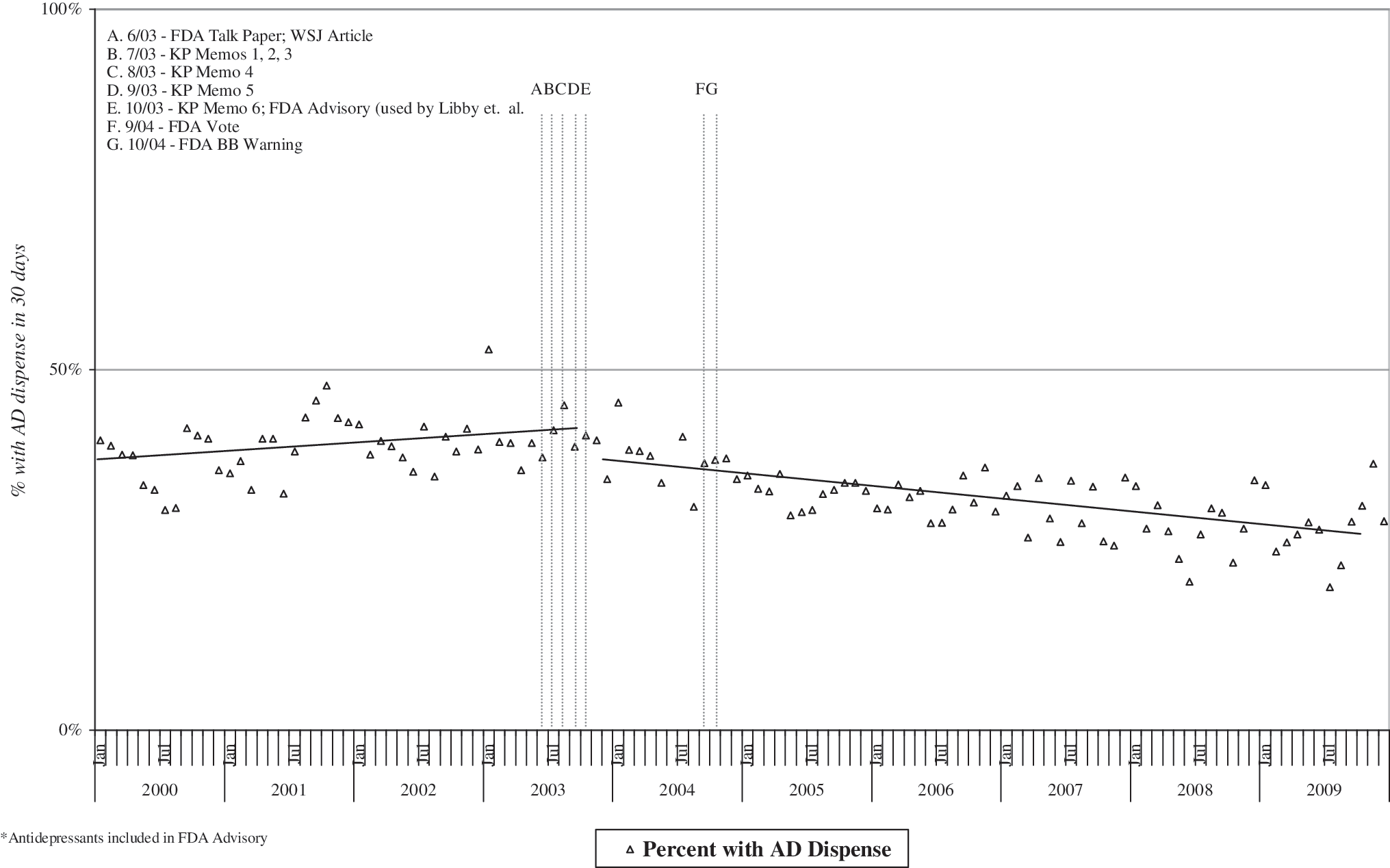
Proportion dispensed ADs within 30 days of incident diagnosis, among youth with unipolar depression and related mood diagnoses.
Days supply
Figure 4 presents the average days supply of AD medication dispensed to each youth during the 6 months following each incident AD dispense, reflecting the persistence of pharmacotherapy over time. No significant difference was found before and after the FDA advisory for this summary measure.
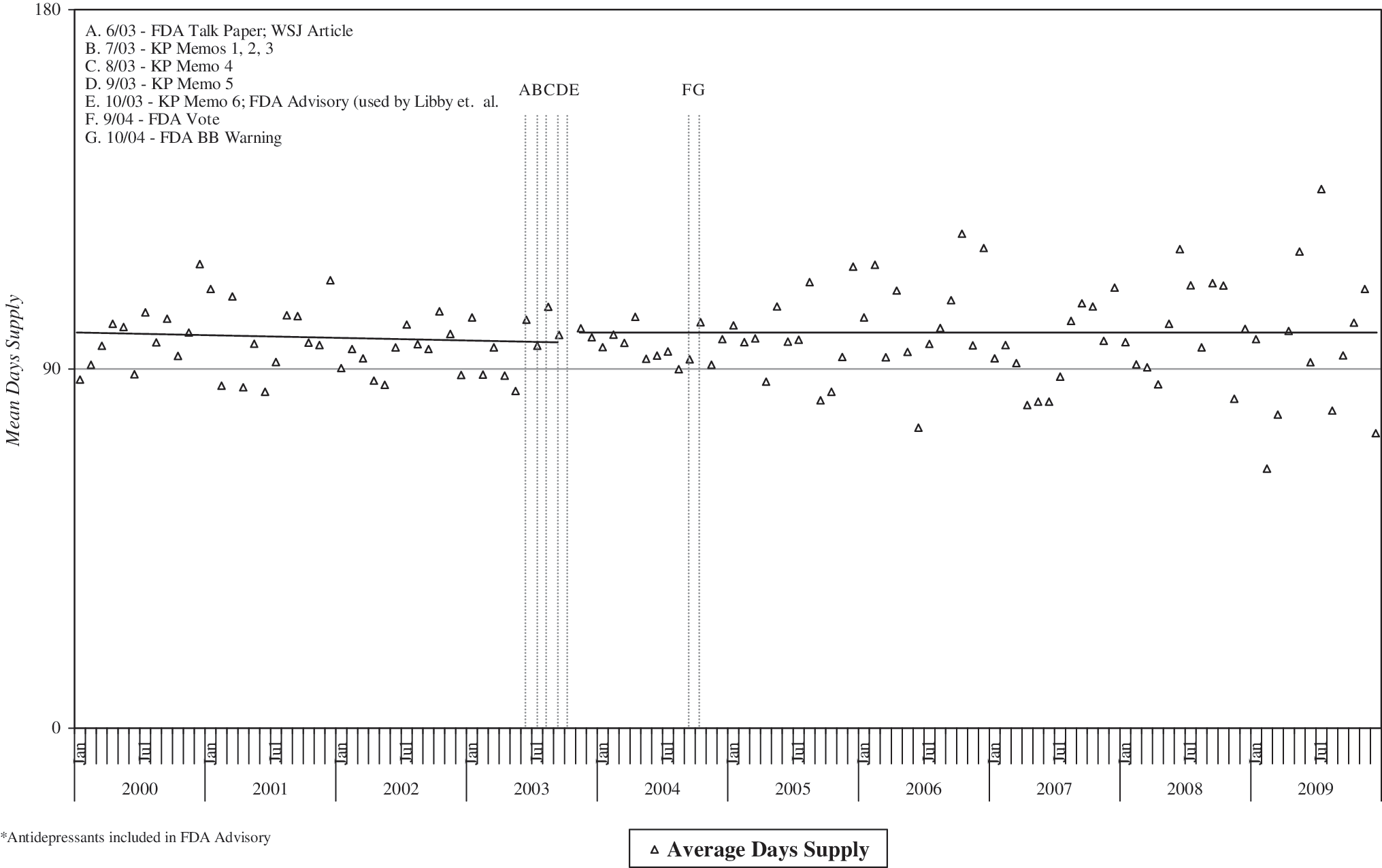
Mean days supply of ADs within 180 days after incident AD dispense, among youth with unipolar depression and related mood diagnoses.
Seeking to better understand this lack of change in cumulative days supply, we separately examined mean days supply associated with each incident and refill AD dispense (Fig. 5). We found a marginally significant increase in the days supply associated with each incident dispense just after the interruption period (p<0.05) but no significant change in slope between the pre- and postperiods. For each AD refill we found a significant immediate increase in mean days supply (p<0.01) as well as a significant increase in the slope of mean days supply from pre- to postinterruption (p<0.0001).
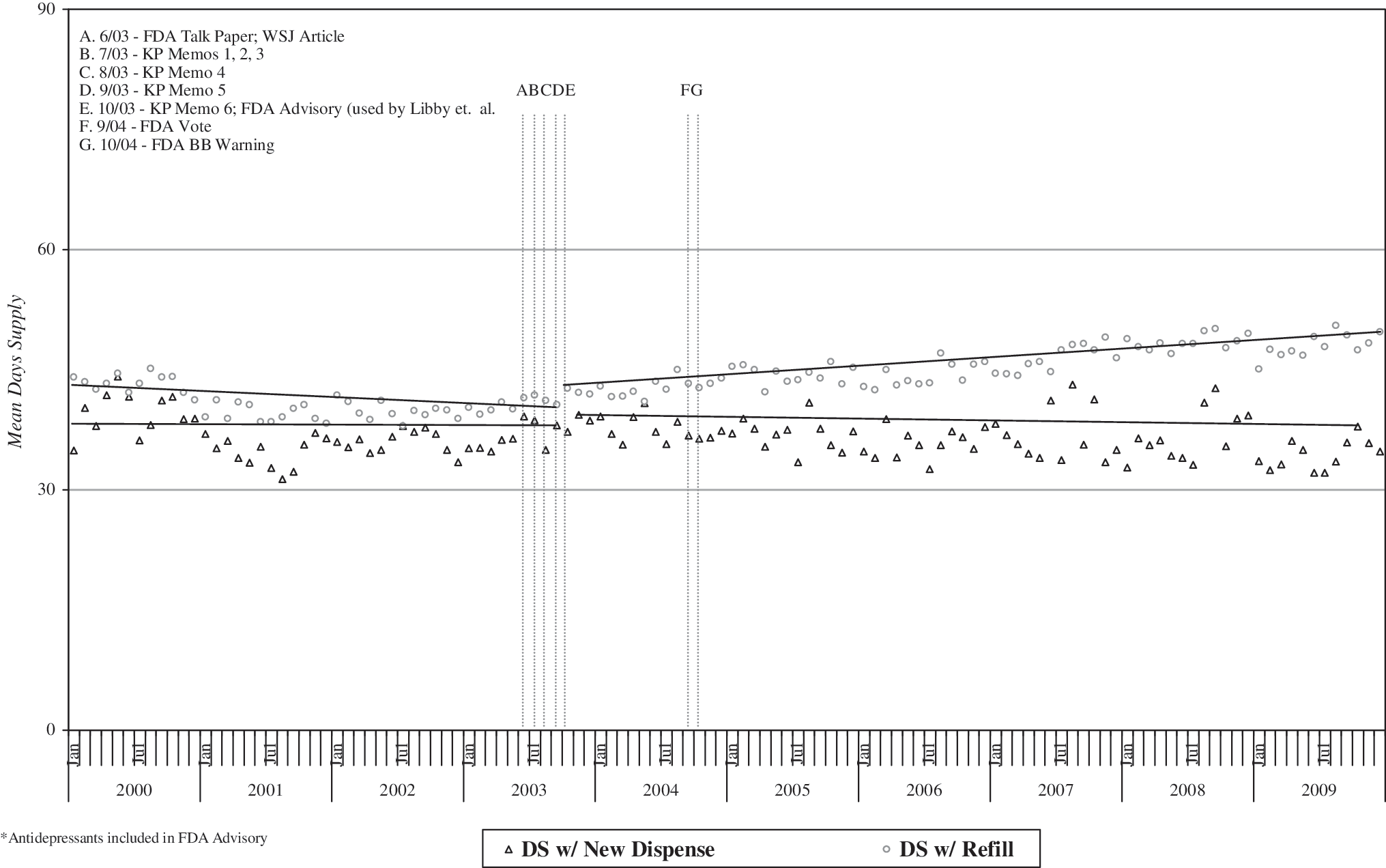
Mean days supply (DS) for each new and refill AD dispense, among youth with unipolar depression and related mood diagnoses.
Youth covered by an AD medication
Figure 6 presents the rate per 1,000 of all HMO youth, whether they had a mood diagnosis or not, who had AD medication in possession in any given month. There was no immediate decline in coverage after the interruption point. However, we did observe a significant reduction in slope from pre to postinterruption (p<0.0001).
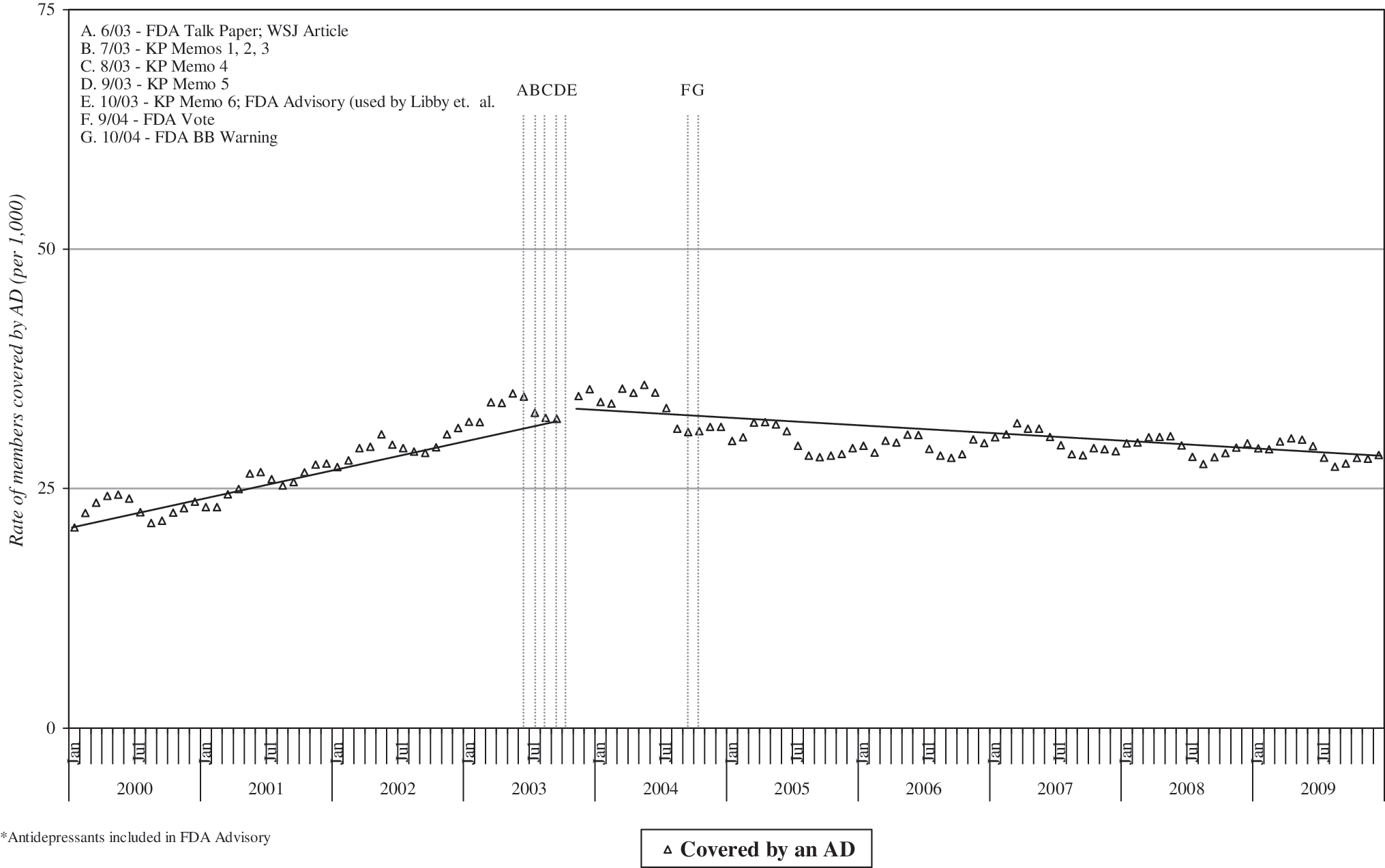
Proportion covered by an antidepressant (AD) medication, per 1,000 youth with unipolar depression and related mood diagnoses.
Preauthorized refills
We classified refill authorization data as either no refills beyond the initial dispense without prescriber reauthorization (“zero refills”; see Fig. 7), or one or more preauthorized refills (average preauthorized refills, Fig. 8). Initial prescriptions with a single refill authorization remained virtually unchanged across the observation window. In contrast, there was a dramatic increase in the slope of initial dispenses with zero preauthorized refills (p=0.01), from a preinterruption average of 25.5% to a postinterruption average of 46.7% of all AD prescriptions. While the mean number of refill preauthorizations visually appears to precipitously decline in the postinterruption period (Fig. 8), this change in slope did not reach statistical significance. In sensitivity analyses, however, we found a large significant level change using a nonstandard interruption point of January 2006 (p<0.001).
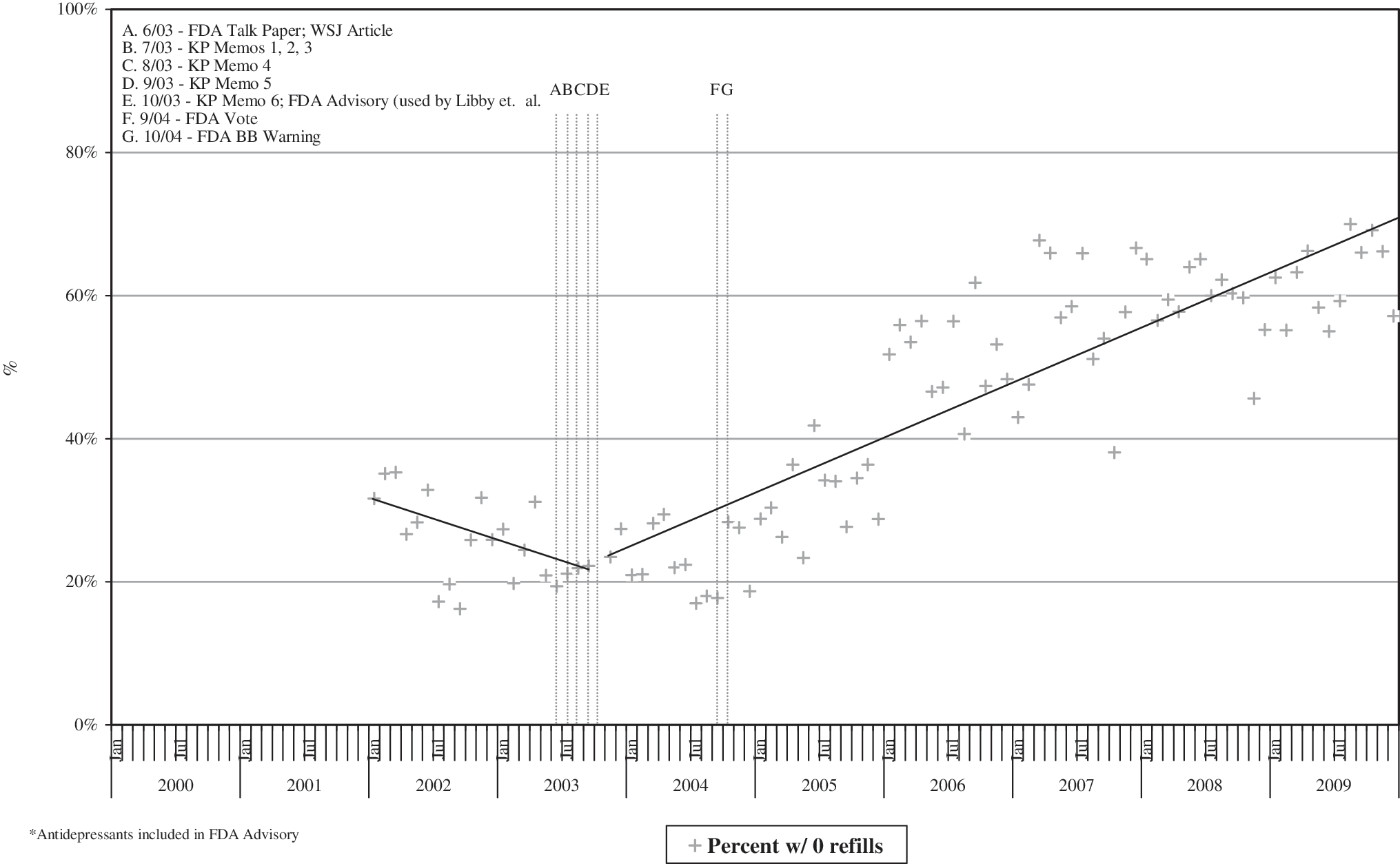
Proportion of incident of antidepressant prescriptions with zero refills, among youth with unipolar depression and related mood diagnoses.
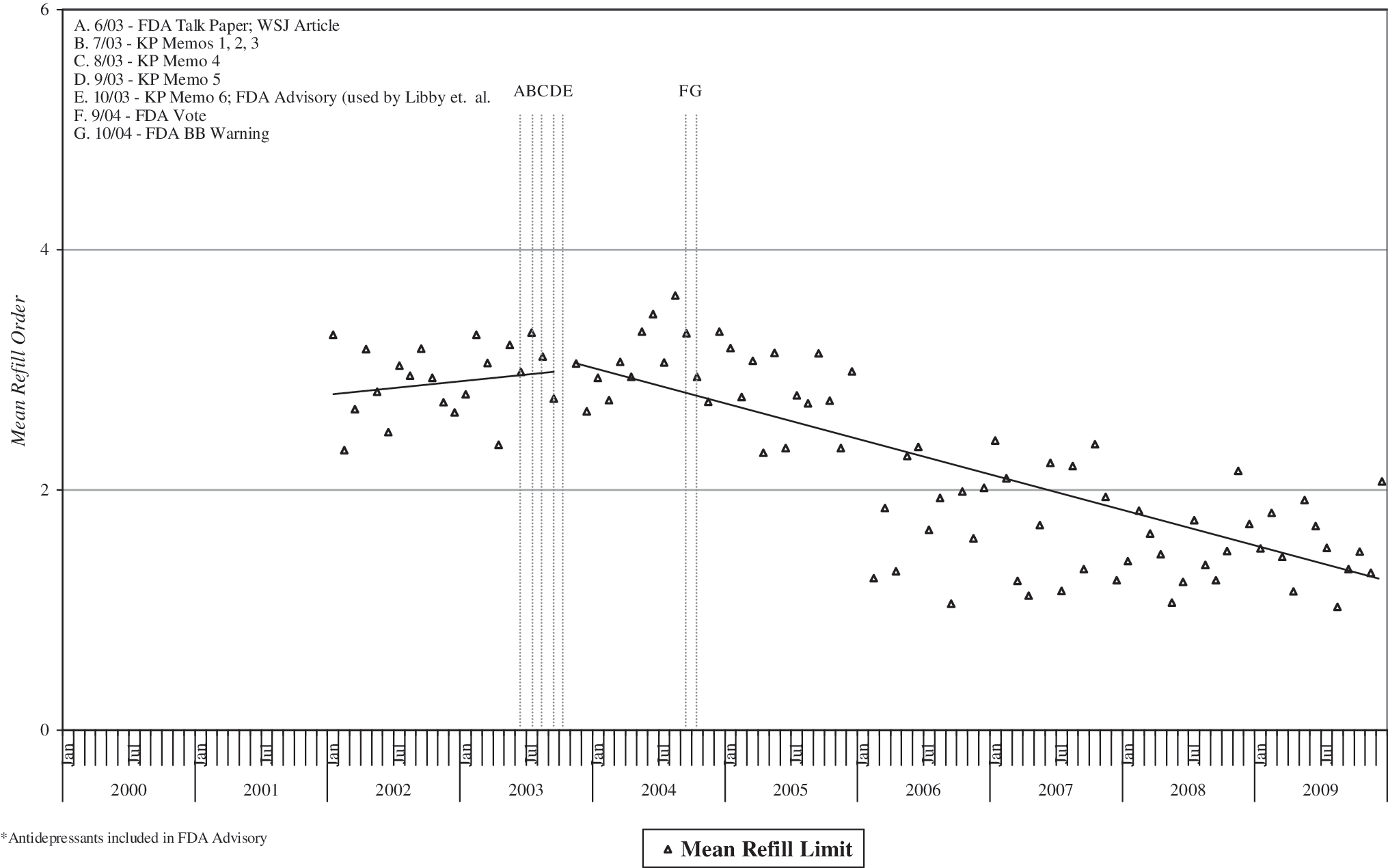
Mean preauthorized refills with incident antidepressant prescription, among youth with unipolar depression and related mood diagnoses.
Discussion
Consistent with many other reports (Olfson et al. 2002; Zito et al. 2002; Delate et al. 2004; Ma et al. 2005) in the years just prior to the 2003–04 FDA actions we observed increased total AD dispenses and increased rates of youth depression diagnoses. Likewise, in the postinterruption period we observed declines in both depression diagnosis rates and AD dispenses, also similar to other reports (Kurian et al. 2007; Libby et al. 2007; Olfson et al. 2008; Libby et al. 2009). This report extends the observation window through 2009—approximately 6 years after the FDA actions—during which the general trend of declining AD dispenses continues. We see no signs of either a rebound or a leveling off, with rates of AD dispensing in 2009 declining to the levels last seen in 2000.
Across the interruption point we observed a significant change in the slope of the proportion of youth with depression diagnoses started on incident episodes of AD. However, a visual inspection of Figure 2 suggests that—while statistically significant—the magnitude of these changes may not be very great. In contrast, a much greater proportion of the decrease in total AD dispenses appears to be accounted for by the decrease in the number of AD refills, with marked declines in the postinterruption period.
One might assume that this substantial drop in AD refills after the FDA action would lead to shorter cumulative treatment episodes. However, mean days supply (Fig. 4) suggests that the cumulative duration of AD treatment episodes has not changed much over this 9-year period. How can this be so? Overall, it appears that while fewer refills were dispensed in the post-FDA period, those refills that were dispensed had an average days supply significantly greater than in the prewarning period (Fig. 5) collectively resulting in little net change in total days supply over the 6 months postinitiation of treatment.
Overall, the picture for postinterruption AD dispenses appears to be declining rates of both incident and refill dispense events. This is accompanied by significant decline in the average days supply of incident dispenses—but a significant increase in average days supply per each refill dispense. Put another way, this reflects overall more conservative early prescribing, but more generous supply per each refill dispense (but overall fewer refill events). Because risk of suicidal behavior and other adverse events is typically highest early on in the treatment episode (Simon et al. 2006) this initial conservatism may be a response to the FDA warnings. Overall, fewer youth are being treated with ADs, but those that persist beyond the initial 30 days appear to receive a course of treatment that is equivalent (in days supply, at least) to episodes of care prior to the FDA actions.
One possible contributor to the decline in totals of AD refill dispenses in the postwarning period may be found in the reduced rate of prescriber preauthorized refills. Healthcare providers in this HMO can electively write prescriptions with additional authorized refills that may be refilled at an HMO pharmacy without the need for an additional visit to write a continuing prescription. In the period before the black box warning the safety profile of SSRIs, the most commonly prescribed AD, was thought to be relatively benign and initial prescriptions were typically written with 2 to 3 authorized refills (Fig. 8), typically for 30 days supply each. Refill limits associated with initial prescriptions began declining with the first FDA warnings in late 2003 and continued to generally decline through the mid-2009. At the end of our observation period (late 2009) the average was less than one preauthorized refill. Correspondingly, the number of incident prescriptions with zero preauthorized refills dramatically increased in the postwarning period (Fig. 7). Anecdotal reports suggest that, mindful of FDA guidelines for more frequent safety evaluations early in treatment (Busch et al. 2010), HMO prescribers may have been reducing or eliminating these additional refill permissions as a means of encouraging patients to return for a follow-up visit so the clinician could evaluate for benefit, tolerability, and safety and then (if warranted) write a continuing refill prescription. While we can only speculate, it may be that some families chose not to make these return visits and were therefore unable to refill the initial AD prescriptions. If so, this strategy for increasing checkup appointments may have indirectly contributed to the observed reduction in refills since late 2003 (and thus fewer individuals covered by continuous pharmacotherapy; Fig. 6). Consistent with this interpretation, reports in other settings suggest that the frequency of follow-up visits to providers has not increased in the post-2003 era, despite the FDA guidelines (Morrato et al. 2008).
This report is limited by its reliance on a single HMO representing just one U.S. geographic area. Although the sample was relatively large it was adequate to detect only large changes in events. This suggests the need for replication in much larger samples. One such effort is underway in the HMO Research Network (
Another potential weakness is our reliance on EMR-recorded clinical diagnoses of depression, assigned by the prescribing physician. Clinical diagnoses are often considered inaccurate, particularly compared to research diagnoses obtained via structured assessment methods. Likewise, we have little ability to evaluate the impacts of modifiers such as disorder subtype, severity, and co-morbidities. Nonetheless, this is typical of the diagnostic information available in pharmacoepidemiology research, doubly so because this is a retrospective study where there is no opportunity to supplement clinical diagnoses with self-report measures or independent evaluation.
Overall, this report is generally consistent with other reports of significant declines in AD dispensing to depressed youth. This report may bring fresh information in its focus on the details of different dispensing types (initial, refills), changes in preauthorized refill limits, and in our ability to identify continuous AD treatment episodes and examine cumulative days supply per individual.
Conclusions
AD dispensing to depressed youth continues to decline, with no sign of leveling off through 2009. However, among youth who do start an AD treatment episode the cumulative supply of medication has remained stable over time, suggesting that treatment episode duration has been preserved. Prescribers in this healthplan have dramatically curtailed preauthorized refills, possibly as an attempt to encourage return visits to reauthorize refill dispenses. Unfortunately, this may have contributed to declining refills rates in the postwarning period.
Clinical Significance
The declining rates of AD dispensing observed in this study, along with the reduced rates of depression diagnosis, might suggest widespread undertreatment. However, we have no data regarding the clinical appropriateness of AD dispensing. These declining rates could reflect an appropriate narrowing of AD prescriptions to just those more severely disordered youth who are most likely to benefit, and corresponding reduced prescribing among youth with milder depression who may not need, or be less likely to benefit from, ADs. Consistent with this possibility Valluri et al. (2010) found that reduced AD dispensing was most strongly observed among youth with less severe depression. Unfortunately, we were unable to identify reliable EMR indicators of depression severity and thus cannot directly test this question in this sample. Future research should focus on AD treatment appropriateness and changes in overall population changes in AD prescribing.
Footnotes
Disclosures
Greg Clarke, John Dickerson, Christina M. Gullion, and Lynn L. DeBar have no disclosures to make about conflicts of interest.
Acknowledgments
We very much appreciate the patients, providers, and staff of the Kaiser Permanente Northwest healthplan.