
Abstract
Objective:
Although behavioral deficits in bipolar disorder (BPD) are well described, the specific brain white matter (WM) disruptions have not been completely characterized, and neural mechanisms underlying dysfunction in BPD are not well established, particularly for youth with BPD and aggression. This preliminary study utilized diffusion tensor imaging (DTI) to investigate commissural tracts (corpus callosum [CC] and anterior commissure [AC]) in youth with BPD, because disruption of interhemispheric communication may contribute to the emotional deficits that are characteristic of the illness.
Method:
DTI was used to investigate WM in 10 youth (7–17 years of age) with BPD and 10 typically developing age-matched controls. Tract-based spatial statistics voxel-wise analysis was used to compare fractional anisotropy (FA) of the two groups. We specifically focused on five subdivisions of the midsagittal CC as well as on the decussation of AC, which connects the temporal lobes. Exploratory correlations between FA values and life history of aggression scores were calculated for the BPD group.
Results:
Youth with BPD had significantly lower FA values in the callosal genu and AC. FA values in the AC were negatively correlated with a life history of aggression in the BPD group.
Conclusions:
These results contribute to a growing literature implicating a role for the genu of the CC in BPD and are the first to report WM variations in the AC of children with BPD. Taken together with the correlational data for aggression and the role of the AC in emotional processing, our data provide preliminary evidence for a possible association between the structural integrity of the WM of the AC and aggression in pediatric BPD.
Introduction
The neural basis of BPD is not well understood. In recent years, it has been recognized that white matter (WM) makes an important contribution to cognition and emotion. WM comprises nearly half the brain volume and plays a key role in development, aging, and many neurological and psychiatric disorders across the life span (Filley 2005). Thus, investigating WM may elucidate our understanding of psychopathology in BPD.
Diffusion tensor imaging (DTI) provides information about WM microstructure in vivo (Basser et al. 1994; Huppi et al. 2001), and permits the study of connections among anatomically and functionally defined brain regions (Conturo et al. 1999). Myelin sheaths and cell membranes restrict the diffusion of water perpendicular to the direction of the axons in WM, whereas water diffuses relatively freely parallel to the axons. This directional dependence of diffusion is often quantified as anisotropy, which reflects myelination of axons and the coherence of axonal orientation (Neil et al. 1998). Fractional anisotropy (FA) is a unit-less and normalized measure of diffusion anisotropy (ranging from 0 to 1) that provides information about the degree of fiber organization and integrity. Mean diffusivity that characterizes the size of the measured diffusion tensor has also been used to detect WM abnormality. Diminished anisotropy of water diffusion and increased apparent diffusion coefficient (ADC) has been proposed to reflect compromised WM integrity (i.e., a disruption or disorganization of tracts) (Beaulieu 2002). WM has an extremely high level of structural organization that compartmentalizes and restricts water motion; thus, DTI, which is inherently sensitive to water diffusivity, has great potential for investigating WM contributions to psychopathology, including BPD.
A recent review suggested that the corpus callosum (CC) may play a role in the pathogenesis of BPD (Bellani et al. 2009). The CC is involved in integrating sensory-motor functions, attention, language, and memory-executive functions frequently compromised in BPD. The CC is, by far, the largest WM structure in the human brain, and the midsagittal CC can be further partitioned into segments connecting different parts of the two cerebral hemispheres (Fig. 1a) (Huang et al. 2005). Few detailed analyses at the multiple segments of the CC have been conducted for children and adolescents with BPD, which is somewhat surprising given that investigating these segments may reveal which brain areas are affected by the CC disruption. For example, the genu connects the prefrontal and orbital areas, and the splenium of CC connects the occipital areas. DTI studies of the CC in children and adolescents with BPD report lower FA values in the genu and body (Frazier et al. 2007), higher ADC and reduced fiber coherence in the splenium (Pavuluri et al. 2009), and lower FA values throughout the CC (Barnea-Goraly et al. 2009). It has been suggested that maldevelopment of the CC and potential impaired communication between hemispheres may affect brain maturation in pediatric BPD (Bellani et al. 2009).
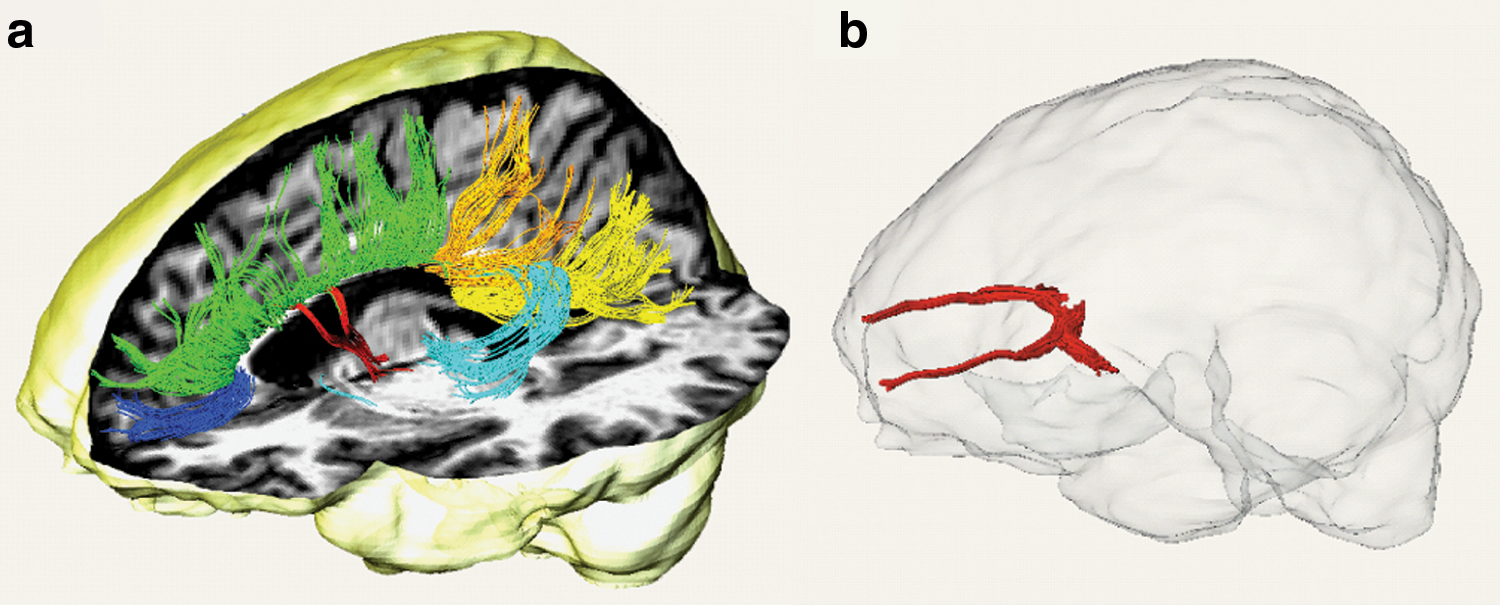
Three-dimensional demonstration of corpus callosum (CC)
To our knowledge, no DTI studies have reported findings in the anterior commissure (AC), a relatively small tract connecting the temporal lobes and amygdala of both hemispheres (the AC connects the middle and inferior temporal gyri) (Fig. 1b) in BPD. The size of the AC has been postulated to play a role in emotional intelligence and social sensitivity (Clark et al. 2010). Since individuals with BPD have deficits in both emotional and social functioning, our exploratory hypothesis is that the AC may play a role in the presentation of the disorder. The lack of reported alterations in the tensor metrics of the AC to date may be related to the small size of this structure and the low inherent resolution of DTI used in clinical practice.
In our preliminary study, we acquired high-resolution DTI scans from 10 youth with BPD and compared the DTI data with that of 10 age-matched healthy control subjects collected as a part of another research study (Rollins et al. 2009). We focused on the commissural tracts, as the studies to date reporting disruption of interhemispheric communication in BPD may be related to the emotional deficits characteristic of the illness. We specifically compared FA values between groups for five segments of the CC and the AC. We hypothesized that there would be decreased FA in the CC for the group with BPD. We did not have a specific directional hypothesis for the AC, as no previous studies have reported DTI findings in this region for individuals with BPD, although we anticipated WM abnormalities in that region. In addition, post hoc correlations between DTI scalars and scores on a measure of aggression were performed for the participants with BPD to explore the relationship between the structural aberration and behavior.
Methods
This study protocol was approved by the University of Texas Southwestern Medical Center Institutional Review Board. Oral and written informed consent was obtained from parents, and oral and written assent was obtained from participants before initiating any study procedure.
Participants with BPD
Ten youth (ages 7 to 17 years inclusive–mean age 13.9±3.6; 60% female) with pediatric BPD were recruited from the Pediatric Bipolar Disorders Outpatient Specialty Clinic at Children's Medical Center in Dallas. We opted to allow inclusion of participants more broadly with bipolar spectrum disorders (BPD type 1, BPD type II, and BPD not otherwise specified [NOS]). Many children and adolescents in the community do not fit the classic Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria for BPD type I and may be diagnosed as having BPD NOS (Lewinsohn et al. 1995). In outpatient clinical settings, this ends up being, by far, the most common presentation. The Course and Outcome of Bipolar Youth (COBY) study describes a phenotypic presentation of children and adolescents with BPD type II and BPD NOS that is on a continuum with that of youth with BPD type I (Axelson et al. 2006). Indeed, the COBY study reported that over a 4-year period, 25% of youth with BPD type II converted to BPD type I, and 38% of those with BPD NOS converted to BPD type I or BPD type II (Birmaher and Axelson 2006).
Participants were evaluated by using the Schedule for Affective Disorders and Schizophrenia for School-aged Children-Present and Lifetime Versions (K-SADS-PL) (Kaufman et al. 1997) to assess clinical diagnoses. We utilized criteria from the COBY study to establish the diagnosis of BPD NOS (Axelson et al. 2006; Birmaher and Axelson 2006). Symptom severity was assessed by using the Young Mania Rating Scale (Young et al. 1978) for current manic symptoms, the Quick Inventory of Depressive Symptoms—clinician rated and adolescent self-report (Rush et al. 2003; Trivedi et al. 2004) for current depressive symptoms, the Clinical Global Improvement-Severity (Leon et al. 1993) scale for global severity, and the Life History of Aggression scale (Coccaro et al. 1997) for aggression. Next, we provide additional information on this lesser known scale.
The Life History of Aggression scale is a clinician-administered semi-structured interview. The scale assesses several domains including temper tantrums, physical fighting, verbal fighting, specific assaults on other people, specific assaults on property, specific assaults on self, suicide attempts, school disciplinary problems, problems with supervisors at work, antisocial behavior not involving police, and antisocial behavior involving police. The range of scores for each item is from 0 to 5 (0=no events; 5=“so many events that they cannot be counted”). The maximum possible score is 55, and total scores greater than 15 can be indicative of high life time aggressive behaviors (Coccaro et al. 1997). The Life History of Aggression scale has been shown to have excellent test-retest stability, inter-rater agreement, and internal consistency reliability (Coccaro et al. 1997).
All evaluations were performed by a trained masters-level research assistant and confirmed by a board-certified child and adolescent psychiatrist (K.S.). Inter-rater reliability on the psychometric instruments was established by rating video-taped interviews, observing interviews conducted by trained raters, and performing interviews while being observed by a trained rater.
All participants in the BPD group had a confirmed diagnosis of BPD type I or BPD NOS. Participants were excluded for history of claustrophobia, autism, schizophrenia, anorexia or bulimia nervosa, current pregnancy or lactation and metal implants, history of alcohol or substance use within the preceding 3 months before the scan, neurological disorder, and a history of head trauma that resulted in loss of consciousness lasting for more than 10 minutes. Table 1 provides the clinical characteristics for the BPD group.
BPD=bipolar disorder; NOS=not otherwise specified; SSRI=selective serotonin re-uptake inhibitors.
Participants with BPD were scanned at the Advanced Imaging Research Center at the University of Texas Southwestern Medical Center by using a 3T Philips Achieva MR system. All were outpatients and on psychotropic medication at the time of scanning.
Healthy controls
Data from 10 healthy controls (mean age 13.6±3.6; 40% female) obtained in the context of a different DTI study were utilized (Rollins et al. 2009). The controls had no lifetime history of any psychiatric disorder based on clinical interview with the participant and parent(s). The healthy controls were scanned at the Children's Medical Center of Dallas imaging facilities on a 3T Philips Achieva MR system using the same scanning protocols.
DTI protocol
In vivo human DTI data were acquired by using a single-shot echo-planar imaging sequence with SENSE parallel imaging scheme (SENSitivity Encoding, reduction factor=2.5). The imaging matrix was 112×112 with a field of view of 224×224 mm (nominal resolution of 2 mm), which was zero filled to 256×256. 2 mm thick slices were acquired parallel to the anterior-posterior commissure line (AC-PC). A total of 60 to 65 slices covered the entire hemisphere and brainstem without gap. Slice number was determined by the height of the participant's brain. The echo time and repetition time were 97 milliseconds and 7.78 seconds without cardiac gating. The diffusion weighting was encoded along 30 independent orientations (Jones et al. 1999) and b value, which indicates amount of diffusion weighting, was 700 s/mm2 (Dubois et al. 2008; Tamnes et al. 2010). Three additional images with minimal diffusion weighting were acquired. Imaging time for each sequence was 4 minutes and 15 seconds. To increase signal to noise ratio (SNR), three repetitions were performed, thus resulting in a total imaging time of 13 minutes. The tensor fitting protocol is identical to that used in our previous study (Huang et al. 2011).
Between scanner comparison
Although both groups were scanned in the same type of scanner (Philips Achieva 3T) using the same scanning protocol, we were concerned that significant results might be resulting from scanner differences rather than true group differences. Thus, we conducted a quality assessment comparing data from the two scanners. A healthy volunteer was scanned on the same day in both scanners using the identical imaging protocol as in this study. We then compared the FA profile for the whole brain and several regions of interest including the genu of midsagittal CC, splenium of midsagittal CC, and cerebral peduncle (CP) in the axial plane of decussation of superior cerebellar peduncle. The differences in FA values were negligible and less than 1.5% across brain regions, thus indicating comparability of the DTI data acquired from the two scanners.
Voxel-wise statistical analysis
Tract-based spatial statistics (TBSS) from the FMRIB software library (FSL,
Comparison of FA values of AC and CC
The comparisons of FA values of AC and CC were performed in the MNI152 template space. In the midsagittal slice, CC was evenly segmented into five compartments along the anterior-to-posterior axis from its most anterior to most posterior boundary (genu and splenium correspond to segment 1 and 5, respectively). FA values at the skeleton voxels of each segment were averaged to represent the CC integrity of this segment. At the axial plane of AC decussation, a box of 15 voxels by 15 voxels, which includes the significant cluster at midsagittal AC, from TBSS analysis was placed. The FA values of skeleton voxels inside this box were averaged for each subject to represent AC integrity. A student t-test was then conducted to compare the integrity of CC segments and AC from the BPD and control groups.
To ensure that the big red clusters in AC and anterior CC (pointed by arrows in Fig. 2) are not spurious false positive outcomes, small-volume FDR correction (Versace et al. 2008; Cullen et al. 2010) was applied. These small volumes were anatomically defined regional masks (highlighted as bright regions in Fig. 2) containing skeleton voxels 100 times larger than the red clusters at AC or anterior region of CC. The FSL statistical tool was used for multiple-comparison correction of the small volume.
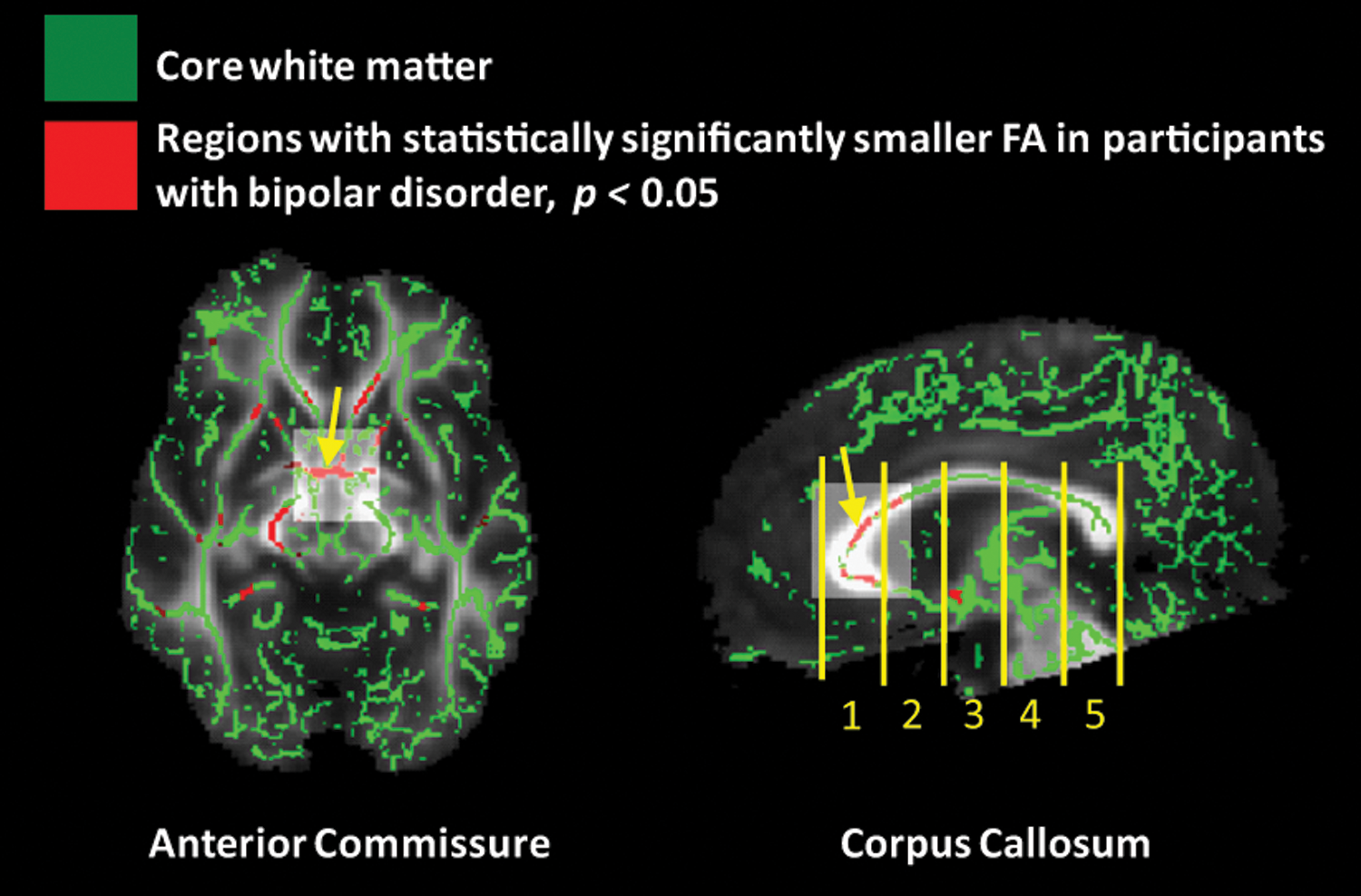
Group analysis results from tract-based spatial statistics. The arrows in both left and right panels point to the clusters of significantly lower fractional anisotropy (FA) in the anterior commissure (AC) (left) and anterior corpus callosum (CC) (right). The small volumes used for multiple comparison corrections of the clusters are bright regions highlighted in both panels. The right panel also shows the segmentation of the CC into five compartments. A color version of this figure can be found in the online article at
Correlation of FA values in CC and AC with life history of aggression for participants with BPD
We performed correlations with the Life History of Aggression scores to assess whether differences in FA values within regions of significant differences between groups were associated with aggressive symptomatology. Spearman's rho correlations (two-tailed) were performed by correlating FA values in the CC (genu) and AC with the total Life History of Aggression score.
Results
We observed statistically significant differences for FA values at CC and AC between the BPD and healthy control participants (Fig. 3). Specifically, as shown in the right panel of Figure 2, the group with BPD had significantly lower FA values in the anterior region of the CC (uncorrected p<0.001), but no statistically significant group differences were observed in the middle and posterior CC. Significant group differences were observed in the AC (left panel of Fig. 2), with the BPD group having lower FA values (uncorrected p<0.001). The FA differences at the two clusters of AC and anterior region of CC (indicated by the arrows in Fig. 2) are significant even after small volume corrections (corrected p<0.05).
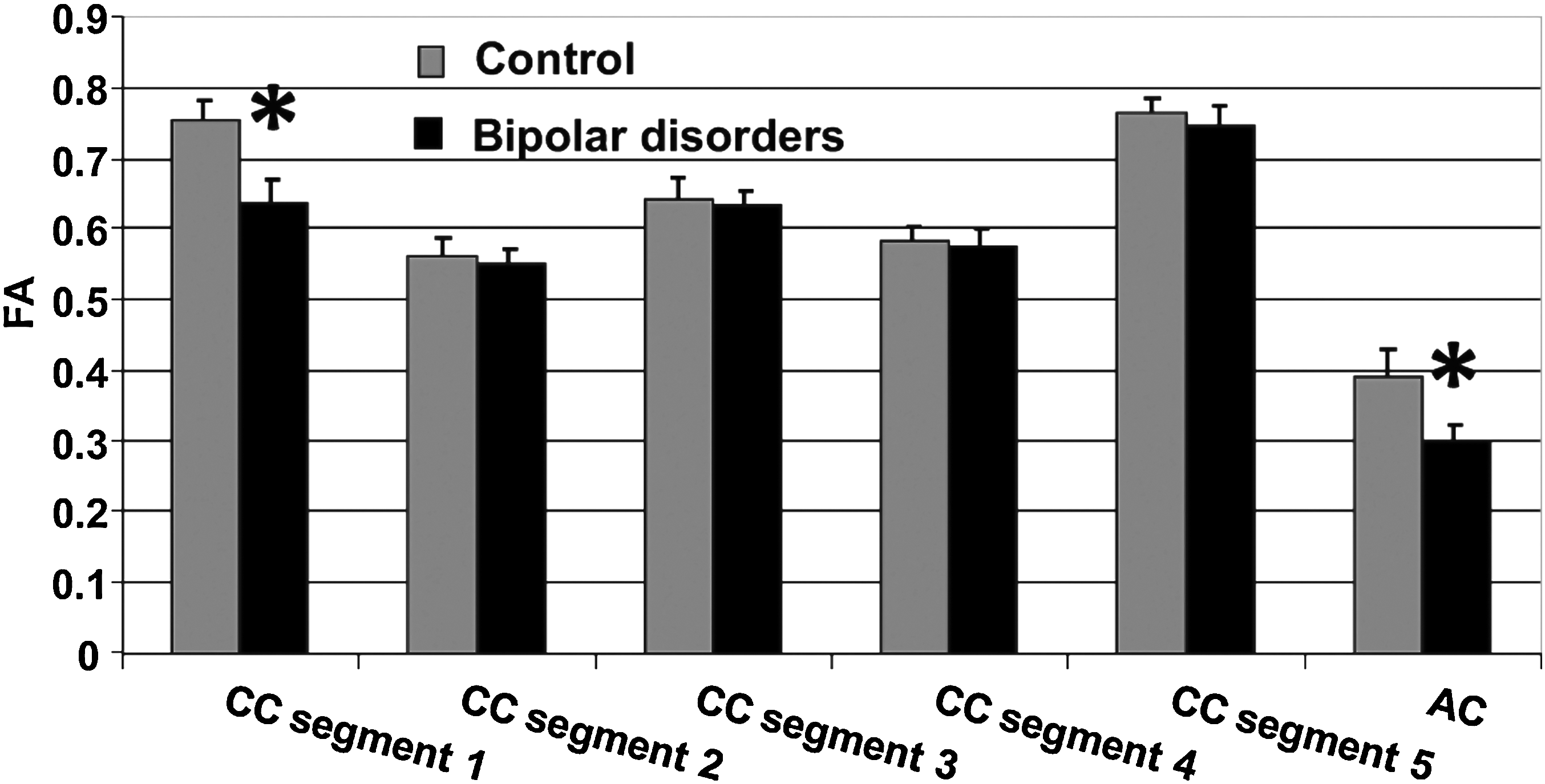
Group comparisons of FA at each segment of midsagittal CC and decussation of AC. Asterisk indicates significant differences (uncorrected p<0.001). FA=fractional anisotropy; CC=corpus callosum; AC=anterior commissure.
Results from our exploratory correlational analyses in the BPD group were also significant for the AC (Fig. 4). Specifically, we observed a significant negative correlation between FA values in the AC and life history of aggression (AC, r=−0.66, p=0.04). The correlation between CC and life history of aggression was in the same direction but not significant (CC segment 1, rho=−0.42, p=0.23).
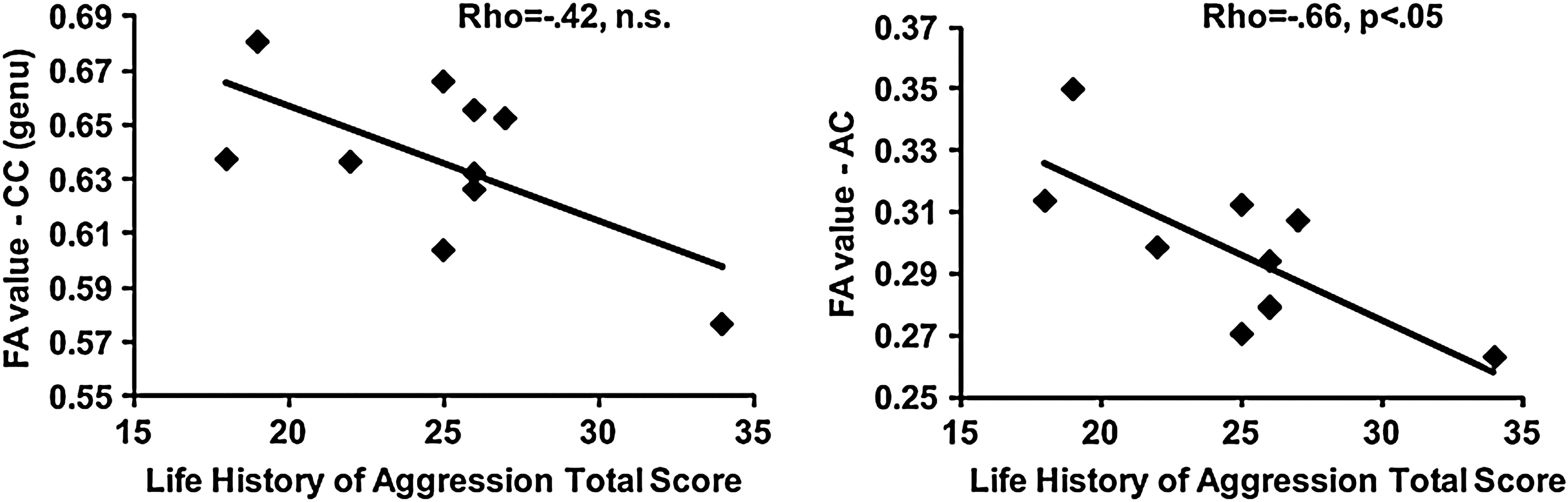
Spearman correlations of FA values in the genu of the CC and AC with life history of aggression total score in the bipolar disorders group. FA=fractional anisotropy; CC=corpus callosum; AC=anterior commissure.
Discussion
These results add to a growing body of literature implicating a role for abnormalities in the CC in youth with BPD. What is different about our preliminary study is that we have included youth with bipolar spectrum disorders with aggression, whereas other DTI studies have reported only on youth with BPD type I and did not report rates of aggression. Our results also suggest a role for WM disruptions in the AC for youth with BPD, which appear to be associated with aggression.
The findings of lower FA values in the genu of the CC for the group with BPD are remarkably consistent with those reported by Barnea-Goraly et al. (2009), who also utilized TBSS. Further, structural studies report reduced volumes specifically in the genu of the CC in BPD (Brambilla et al. 2009). The anterior component of the CC provides interhemispheric connections between the left and right prefrontal cortices thought to integrate hemispheric functioning and to play a key role in the integration of emotional and cognitive information (Womer et al. 2009).
Compromised WM integrity in the AC has not been previously reported, possibly due to challenges achieving sufficient resolution with DTI protocols used in clinical practice. However, the abnormalities we observed in the AC are prominent and statistically significant. Further, inspection of all FA maps in their native spaces suggests that the findings are not due to misregistration. The AC connects the temporal lobes and amygdala of both hemispheres. Since the amygdala plays a role in the mediation of emotional processing in BPD (LeDoux 2000), and volumetric deficits in the amygdala of youth with BPD have been documented (Chen et al. 2004; DelBello et al. 2004; Blumberg et al. 2005; Chang et al. 2005; Dickstein et al. 2005), our exploratory finding of decreased FA in the AC may contribute additional information about the pathophysiology of this illness in children and adolescents.
The fact that AC abnormalities were found to play a role in BPD and correlated with aggression is particularly interesting. To our knowledge, no DTI studies have investigated WM integrity in aggressive youth with bipolar spectrum disorders, a clinically significant group to study as lifetime aggression has been associated with risk for suicidality (Grunebaum et al. 2006). Further, aggressive bipolar youth commonly present to child psychiatric clinics, as their aggression cannot be managed by their primary caretakers, and they appear to be less responsive to treatment (Jensen et al. 2007). The results of our exploratory analyses showing that reduced FA values in the AC were significantly negatively correlated with the Life History of Aggression scores, even in such a small sample, suggest the possibility of an association between the structural integrity of the WM of callosal connections and aggression in youth with BPD. Future studies looking at bipolar youth with aggression with a larger sample will be needed for further examination of potential tract specific impairments in youth with bipolar spectrum disorders and aggression.
It should be noted that there are some potential limitations to this preliminary study which make replication imperative. Although our sample size did provide enough power to detect group differences, the sample size is still limited and may have restricted us from finding disruption in other WM regions where FA changes are relatively smaller but may still be significant given a larger sample. In addition, the completely new findings on the significantly decreased FA values in the AC and the significant correlation between FA in the AC and Life History of Aggression scores were not hypothesized. Other potential limitations relate to the BPD sample that included youth with BP Type I and BP NOS, who were all taking psychotropic medications, and evidencing varying mood states, although the majority were euthymic. We re-ran the DTI analyses excluding the two youth with BP NOS; the results obtained were remarkably similar and remained statistically significant. Previous research suggests that psychotropic medications have limited impact on WM in BPD (Frazier et al. 2007), a finding supported by studies in schizophrenia which also failed to find a significant effect of medication on measures of diffusion (Lim et al. 1999; Foong et al. 2000). Finally, we did not have clinical data regarding family history of psychopathology or head trauma for the healthy comparison group that may affect WM.
Conclusions
These findings are important in that they provide additional evidence of WM disruption of CC genu in youth with BPD and, more specifically, in aggressive bipolar youth. Our exploratory investigations found evidence that the AC is disrupted in youth with BPD and preliminary evidence that the integrity of this tract is significantly associated with Life History of Aggression scores. This initial finding may be related to the purported role of the AC in the integration and processing of emotional information. However, additional studies with larger samples are needed to replicate these findings, as we could find no other studies reporting on bipolar youth with aggression, nor were we able to find other reports of a role for the AC in aggression regardless of psychiatric diagnosis.
Clinical Significance
Aggression is a construct that is a sensitive marker of the severity of BPD and can be reliably measured by utilizing empirically validated rating scales. Youth in whom BPD and Attention-Deficit/Hyperactivity Disorder have been diagnosed are found to exhibit significant levels of impulsive behavior and attention problems, but youth with BPD also exhibited significant levels of aggressive behavior, dysphoric mood (Doerfler et al. 2010), and functional impairments (Jensen et al. 2007). Thus, the pathophysiology of aggression in pediatric BPD warrants research focusing on biological markers that can address its etiology and eventually lead to targeted treatment interventions.
Disclosures
Dr. Saxena receives research support from Shire Pharmaceuticals, GlaxoSmithKline Pharmaceuticals, Pfizer Pharmaceuticals, and Advanced Imaging Research Center at University of Texas Southwestern Medical Center, Dallas, TX. Leanne Tamm, Annie Walley, Alex Simmons, Nancy Rollins have no disclosures. Dr. Emslie receives research support from Biobehavioral Diagnostics Inc., Eli Lilly, Forest Laboratories, GlaxoSmithKline, and Somerset; is a consultant for Biobehavioral Diagnostics Inc., Eli Lilly, Forest Laboratories, GlaxoSmithKline, INC Research, Inc., Lundbeck, Pfizer, Inc., Shire Pharmaceuticals, Validus Pharmaceuticals, and Wyeth Pharmaceticals; and is on the Speakers Bureau for Forest Laboratories, Inc. Xin Fan and Hao Huang have no disclosures.
Footnotes
Acknowledgments
The authors thank the Advanced Imaging Research Center at University of Texas Southwestern Medical Center (UTSW) for providing free scans for this pilot study. They also thank Dr. Paul Nakonezny, an Associate Professor in the Division of Biostatistics at UTSW, for his assistance in the preliminary stages of this work, and Dr. Yan D. Zhao, an associate professor at UTSW, for his assistance in conducting power analyses.