
Abstract
Objective:
The purpose of this study was to estimate the prevalence and incidence of new diagnoses of attention-deficit/hyperactivity disorder (ADHD) and assess drug treatment of ADHD in the 3–17 year age group in Germany.
Method:
We analysed data from the German Pharmacoepidemiological Research Database (GePaRD) for the years 2004–2006. The GePaRD includes claim records of 14,000,000 members of four statutory health insurances, representing 17% of the German population. The assessment of ADHD diagnoses was based on International Classification of Diseases version 10 (ICD-10) codes in outpatient and hospital data.
Results:
In 2005, the age-standardized prevalence and incidence of new diagnoses were 2.5% and 9/1000 person-years, respectively. Both measures were 3–4 times higher for males than for females. Incidence of new ADHD diagnoses increased linearly up to the age of 8 years for boys and 9 years for girls and decreased abruptly thereafter. In the calendar quarter of the initial ADHD diagnosis, 9.4% (95% confidence interval [CI] 8.9–9.8%) received methylphenidate or atomoxetine and 36.8% (95% CI 36.1–37.6%) received at least one prescription of either drug within the first year. Initiation of drug treatment and choice of drug were similar for both sexes.
Conclusions:
ADHD is a common condition among children and youth in Germany. There are substantial differences by sex in the prevalence and incidence of new ADHD diagnoses, but only a small difference in drug treatment among those diagnosed with ADHD. A relatively low percentage of children receives drug treatment in the first year after the initial diagnosis of ADHD.
Introduction
A variation across countries in ADHD prevalence was reported, but most of the observed differences are likely the result of methodological differences in the classification of the disease (American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders [DSM] versus International Classification of Diseases [ICD] criteria), the assessment of the diagnoses (based on diagnostic scales, reported by parents, or recorded in administrative databases) or the studied population (clinical samples, school samples, or population-based samples) (Polanczyk and Rohde 2007; Polanczyk et al. 2007; Skounti et al. 2007). The specific classification system is the most basic determinant for the assessment of ADHD diagnoses, whether it is based on diagnostic scales, reported diagnoses, or medical records. Prevalence based on medical diagnoses from regular clinical practice is called “administrative prevalence” in contrast to prevalence obtained by an actual assessment of the population (Schlander et al. 2010). The latter can also include subjects who did not seek treatment during the studied period or have no regular access to health care. In surveys, prevalence is typically estimated as lifetime prevalence of retrospectively reported diagnoses, or as point prevalence based on scores of psychometric scales above a predefined threshold for ADHD, whereas analyses of administrative databases usually report period prevalence based on all diagnoses in the given year. Given that symptoms of ADHD can diminish or resolve over time (Faraone et al. 2006), the period and lifetime prevalence of ADHD are not directly comparable. Furthermore, the lifetime prevalence based on parental reports is subject to reporting bias.
In Germany, representative data on lifetime and point prevalence of ADHD in the 3–17 year age group were obtained from the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) (Schlack et al. 2007; Huss et al. 2008). In the main module, the lifetime prevalence was estimated from parental reports on lifetime diagnoses of ADHD, and in an additional module of the KiGGS named BELLA. Estimation of the point prevalence was based on an ADHD symptom checklist (FBB-HKS/ADHS) (Dopfner et al. 2008). Apart from these studies, some earlier non-representative surveys addressed the prevalence of ADHD (Baumgaertel et al. 1995; Gortz-Dorten and Dopfner 2009). Furthermore, in regional studies, diagnoses recorded in health insurance data were analysed (Koster et al. 2004; Schlander et al. 2007; Schubert et al. 2010), but so far, there are no data for the whole of Germany.
In administrative databases, patients can be identified as having a diagnosis only if they seek treatment or continue with treatment. Whereas DSM classification requires that symptoms of ADHD exist before the age of seven, there is an ongoing controversy that symptoms can also sometimes start later (Bell 2011; Kieling et al. 2010; Polanczyk et al. 2010). Irrespective of the onset of symptoms, children and adolescents can be diagnosed for the first time with ADHD at different ages. This delayed diagnosis of ADHD can be described in terms of age-specific incidence of new ADHD diagnoses. Furthermore, ADHD is a disorder with a substantial persistence of symptoms into adulthood (Kessler et al. 2005; Faraone et al. 2006; Schmidt and Petermann 2009; Biedermann et al. 2010). Nevertheless, because of partial remission of symptoms, adaptation and coping with symptoms, or non-compliance despite persisting symptoms, patients might discontinue the medication and also stop other treatments. If they do not see an accredited specialist because of ADHD and receive treatment covered by the insurance, their treatment cannot be identified in the database. Discontinuation of treatment (not only drug treatment but also seeing a physician because of ADHD diagnoses) among children and adolescents with ADHD is common but still insufficiently studied (Adler and Nierenberg 2010), and it is of interest to study to what degree such discontinuation can be assessed using a relatively short series of administrative healthcare data.
Administrative healthcare databases are also typically used in pharmacoepidemiological studies, focusing on the prescription rates of drugs used in the therapy of ADHD or on the increase of these prescription rates over time (Zito et al. 1997; van den Ban et al. 2010). Prescriptions can be studied in the context of the whole population or in ADHD cases specifically. Such studies were also conducted for Germany (Schubert et al. 2003; Schmidt-Troschke et al. 2004; Janhsen 2007; Schubert et al. 2010). At the same time, little is known about the initiation of medication when the child or adolescent was diagnosed with ADHD for the first time.
The aims of our study were 1) to provide estimates for the age-specific prevalence of ADHD from a healthcare database covering all regions of Germany, 2) to estimate age-specific incidence of new diagnoses of ADHD in the database, 3) to assess the continuation of ADHD diagnoses in the database by comparing age-specific incidence of new diagnoses of ADHD with age-specific prevalence, and 4) to analyze the initiation of drug treatment in newly diagnosed cases of ADHD.
Method
Data source
The database used in this study is the German Pharmacoepidemiological Research Database (GePaRD). The database was described elsewhere (Ahrens et al. 2007; Pigeot and Ahrens 2008; Behr et al. 2010; Garbe et al. 2011; Kraut et al. 2010). In brief, the GePaRD is a large healthcare database consisting of claims data from four German statutory health insurance (SHI) providers. At the time of the study, the database contained data for the calendar years 2004–2006 and included ∼14,300,000 million people from all regions in Germany, representing ∼17% of the German population. For each insuree, demographic information (age, sex, district of residence) as well as information on hospital admissions, ambulatory physician visits, and ambulatory prescriptions was available. The hospital data included information about the admission and discharge dates, the reasons for admissions and discharges, and codes for diagnostic and therapeutic procedures with their respective dates. Ambulatory diagnoses can only be allocated quarterly, whereas ambulatory treatments, procedures, and prescriptions have exact dates. All diagnoses, ambulatory as well as inpatient, were coded according to the German modification of the International Classification of Diseases version 10 (ICD-10-GM). Prescription data were available for ambulatory prescriptions, which are registered for reimbursement by the SHIs. The data contained the date of prescription, the date of dispensation, the amount prescribed and an identification number for the prescribing physician. According to the German law, the use of SHI data for research purposes requires permission of the data owner and the responsible regulatory body. In the GePaRD, the data are pseudonymized and a data protection concept is safeguarding the privacy rights of the individuals. The use of data for this study was approved by the Federal Ministry of Health and all SHIs that contributed data. No further informed consent was necessary because the study was performed with routine data.
Study population
For the analysis, children and youth aged 3–17 years in 2005 were selected (n=2,170,437, 100%). For the estimation of the prevalence, a continuous insurance period of at least 1 year including December 31, 2005 (n=1,964,607, 90.5% of the initial sample) was required for each study participant. For the estimation of incidence of new diagnoses, this period had to include at least 2 years, at least 1 year before and at least 1 year after the diagnosis (n=1,876,868, 86.5%). ADHD diagnoses were classified as new in 2005 when there were no ICD-10 codes for ADHD (F90.0, F90.1, or F90.9) and no prescriptions of methylphenidate or atomoxetine in the preceding 365 days before the diagnoses (n=1,817,054, 83.7%). Only subjects with available information on sex and the federal state of residence were included (n=1,958,868, 90.3% for the prevalence estimation and n=1,811,747, 83.5% for the incidence estimation).
Ascertainment of ADHD cases and drug treatment
Children or adolescents with ADHD were identified based on ICD-10-GM codes: F90.0 (disturbance of activity and attention), F90.1 (hyperkinetic conduct disorder), and F90.9 (hyperkinetic disorder, unspecified). In the database, diagnoses can be qualified as “suspected” or “ruled out”, but these qualifiers are not always recorded, and, therefore, excluded diagnoses still appear in the data set. Therefore, we used a conservative algorithm instead of a single diagnosis to ascertain ADHD cases. First, we excluded all diagnoses with an explicit qualifier “ruled out” or “suspected.” Second, an ADHD case was identified when one of the following conditions was fulfilled: 1) a single inpatient diagnosis F90.0 or F90.1, 2) two outpatient diagnoses in two different quarters within 1 year or two outpatient diagnoses in the same quarter but by two different physicians (in such a case additionally the code F90.9 was allowed) or in the same quarter and by the same physician, but with two different codes for ADHD or an outpatient diagnosis followed by an inpatient diagnosis within a period of 365 days, and c) a prescription of methylphenidate or atomoxetine combined with an outpatient or inpatient diagnosis of F90.0 or F90.1 within 365 days. The date of the earliest diagnosis (for outpatient diagnosis, middle of the corresponding quarter) or prescription used for the identification of the case was considered as the index date for estimation of new diagnoses. Persons who did not fulfil any of the above criteria were considered as not having ADHD. In order to describe drug treatment after the first diagnosis of ADHD, we studied the initiation of treatment in patients with new diagnoses.
Data analysis
Age-specific prevalence and incidence of new diagnoses were stratified by sex. In the calculation of the prevalence, the end-of-year population was used as denominator for each year. Person-time under risk was used as denominator for the calculation of incidence of diagnoses. Regional (for each federal state) and sex- and age-specific estimates were weighted by population weights obtained from the Federal Statistical Office to obtain estimates for Germany.
Lifetime prevalence at a specific age was constructed from incidence of new diagnoses by age and sex, assuming that age-specific identification of new diagnoses was constant in the last few years.
The continuation of ADHD diagnoses in the database was studied by comparing lifetime prevalence at a specific age with the observed age-specific prevalence at this age, starting at the youngest age and proceeding to the age of 17 years. First, the prevalence in the first 1-year age group was compared to the prevalence in the next 1-year age group minus new cases in this age group. Because the fraction of diagnoses persisting from one 1-year age group to the next did not differ by age, a common parameter was fitted across the age spectrum by minimizing the Euclidian distance between model-based and observed age-specific prevalence.
The Kaplan–Meier method was used to analyze the time from the new diagnosis until the first prescription of methylphenidate or atomoxetine. All analyses were conducted with SAS Version 8.02.
Results
Prevalence and incidence of new diagnoses of ADHD
In 2005, the prevalence of ADHD in the 3–17 year age group was 2.5%. There were 0.9 new diagnoses of ADHD per 100 person-years (Table 1). The prevalence was approximately four times higher in males than in females; the difference between sexes was slightly smaller for the new diagnoses. In both sexes, the incidence of new diagnoses increased nearly linearly with age up to the peak in 8-year-old boys and in 9-year-old girls and decreased thereafter (Fig. 1). The prevalence displayed a more curvilinear pattern, with a less sharp peak in 10-year-old boys and in 9-year-old girls (Fig. 2). When using only a single F90.0, F90.1, or F90.9 diagnosis, one would obtain a nearly 50% higher prevalence. Based on the observed age-specific incidence of new diagnoses, the calculated lifetime prevalence by the age of 17 was 18.8% for males and 6.4% for females (Fig. 2).
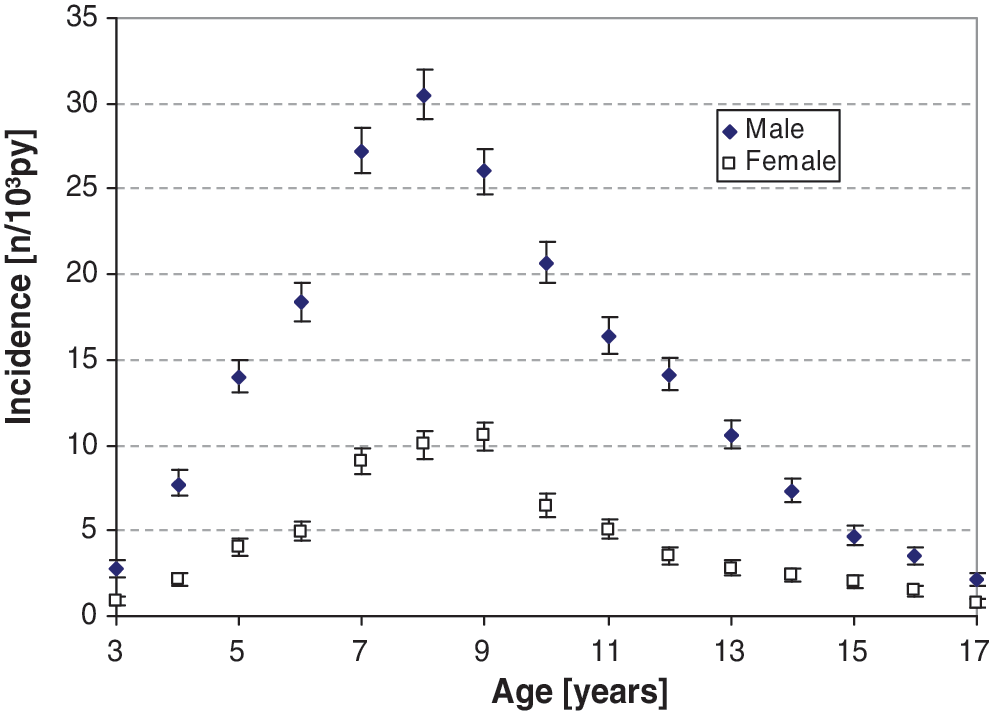
Age-specific incidence of attention-deficit /hyperactivity disorder diagnoses by sex (estimate and 95% confidence interval, per 1000 person-years).
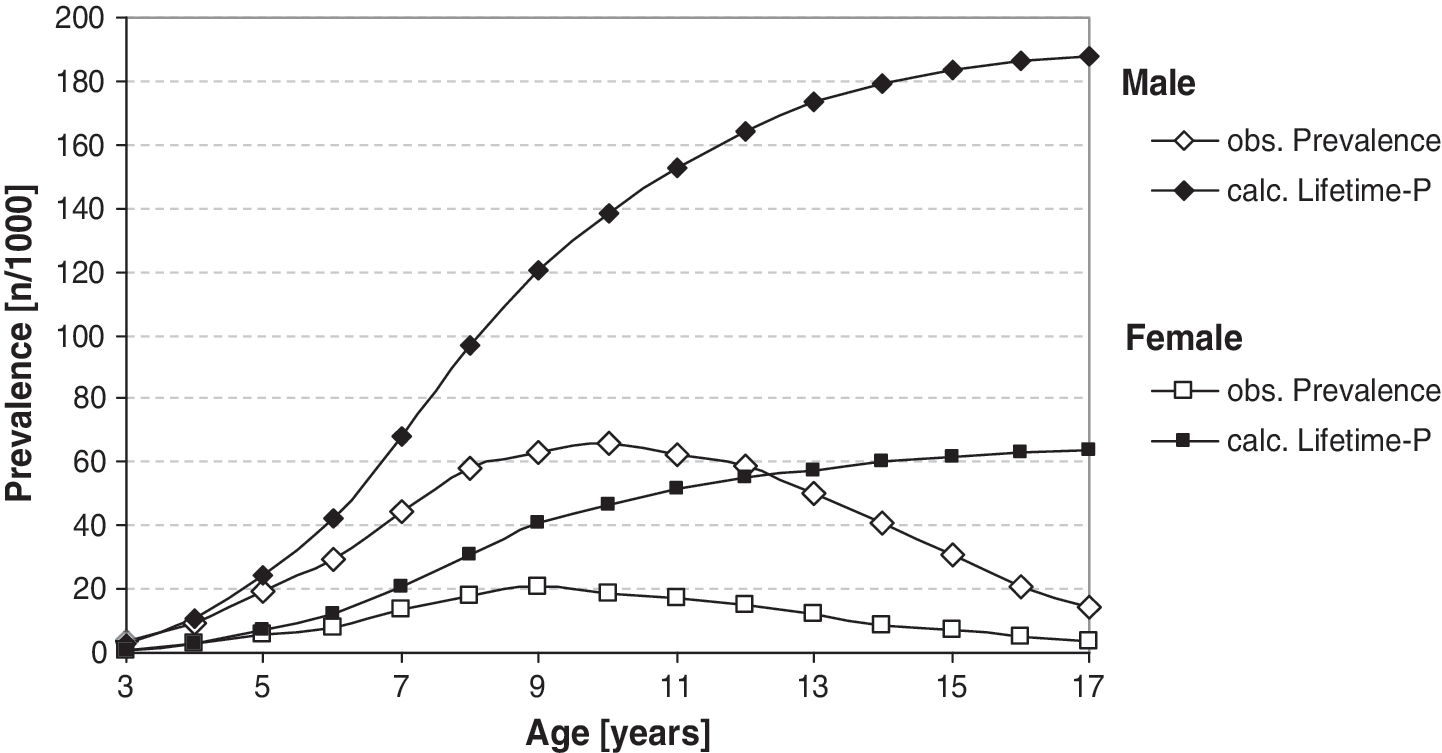
Observed (obs.) prevalence and calculated (calc.) lifetime prevalence (Lifetime-P) of attention-deficit /hyperactivity disorder by age and sex.
In a few cases both methylphenidate and atomoxetine were prescribed at the same time.
Continuation of ADHD diagnoses in the database
As expected, the comparison of the lifetime prevalence with the observed prevalence at the specific age indicated that there is a substantial fraction of children and youth with ADHD who do not continue treatment, as indicated by contacts with an accredited specialist because of ADHD, or by drug prescriptions. There was no indication that the continuation of treatment depended upon age (data not shown), but there was a slight dependence on sex: the probability of continuing treatment when moving into a 1-year higher age group was estimated at 61% for females and 70% for males. Given these parameters, the observed age-pattern of prevalence was fitted well by the prevalence estimated from new diagnoses and treatment continuity.
Initiation of drug treatment among patients with new diagnoses of attention-deficit/hyperactivity disorder
Among all patients with a new diagnosis of ADHD in 2005, 37% received at least one prescription of methylphenidate or of atomoxetine within 1 year after the initial diagnosis (Table 1). The initiation of drug treatment was only marginally more frequent in males than in females. Among those who received drug treatment, 91% were treated with methylphenidate and 9% with atomoxetine, without any difference by sex. The proportion of cases with new ADHD diagnoses who received treatment within 1 year was <10% up to the age of 5 years, increased steeply between 5 and 8 years, and then more slowly thereafter (Fig. 3). As for receiving drug treatment at the time of initial diagnosis with ADHD, this occurred in 9.1% (95% confidence interval [CI]: 8.2–10.1%) of new cases among girls and 9.4% (95% CI: 8.9–10.0%) of new cases among boys, and there was an approximately constant increase in the fraction receiving drug treatment during the first year (the increase was slightly faster in boys than in girls). Within 365 days of the index date, 34.1% (95% CI: 32.6–35.6%) of females and 37.7% (95% CI: 36.8–38.5%) of males with ADHD received at least one prescription of methylphenidate or atomoxetine (Fig. 4).
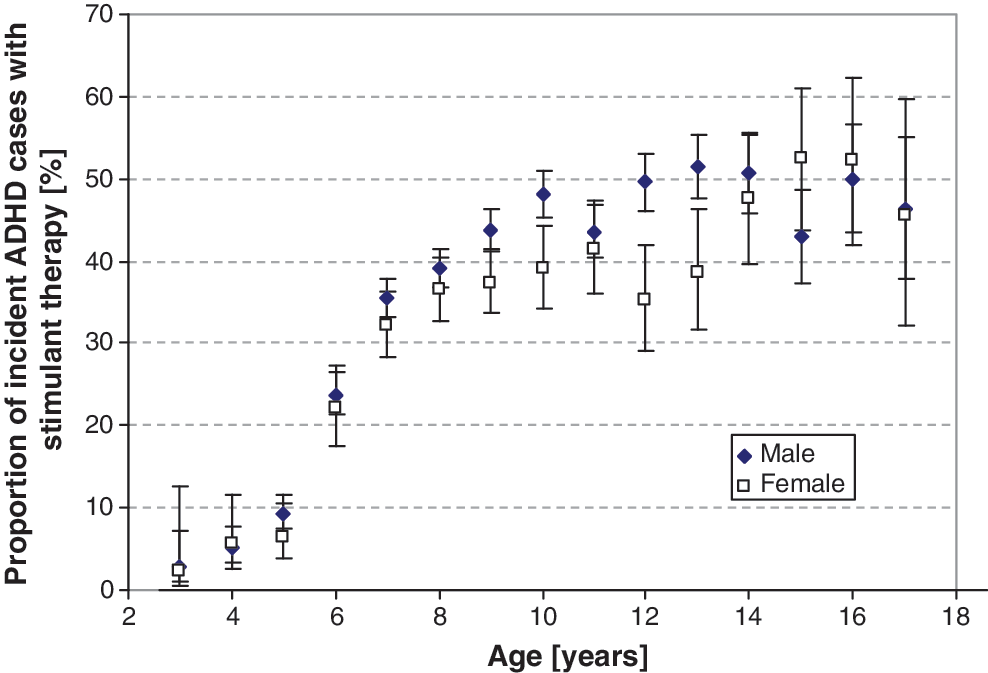
Proportion of patients with new attention-deficit/hyperactivity disorder (ADHD) diagnoses receiving stimulant therapy within 1 year of the initial diagnosis by age and sex.
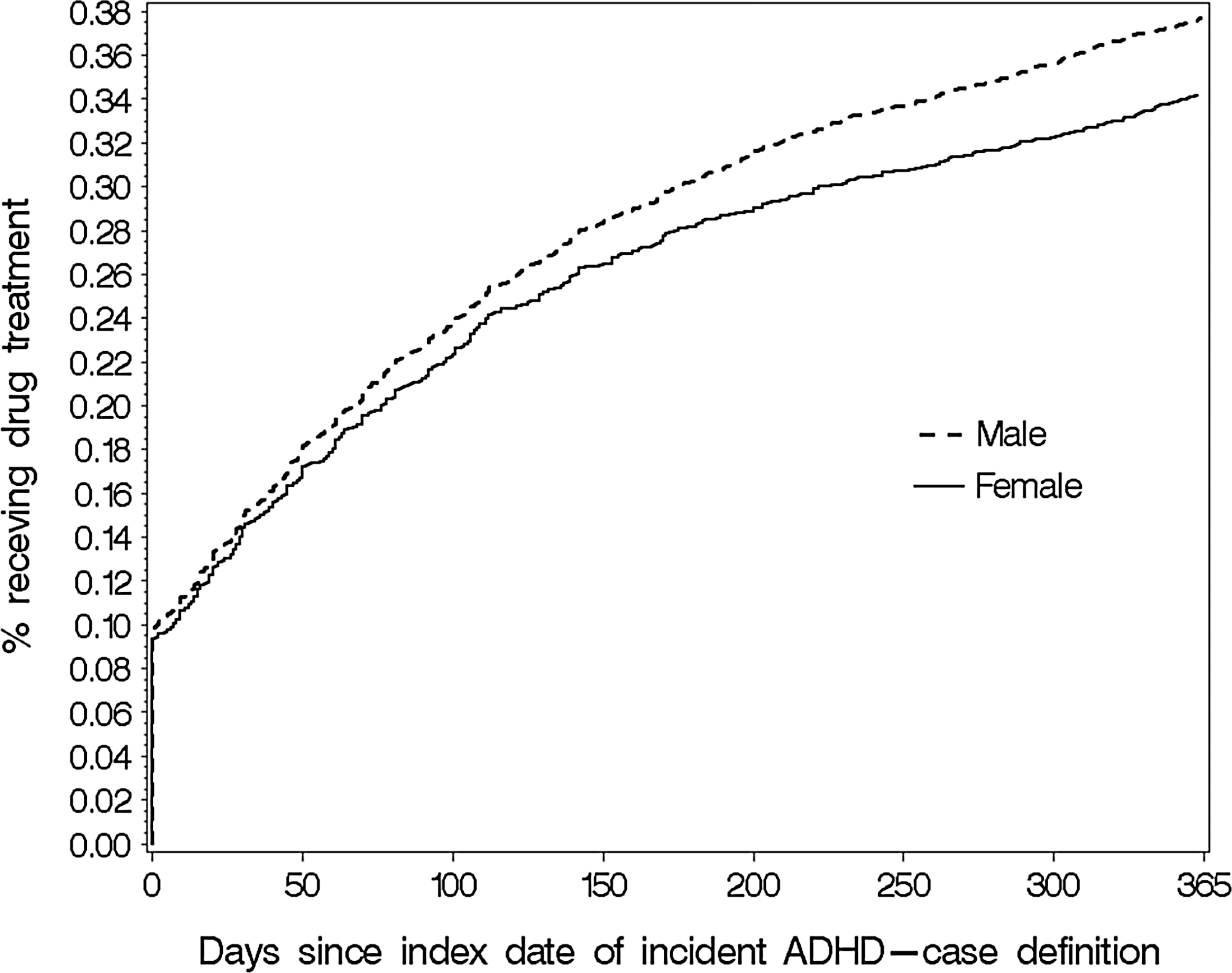
Initiation of treatment during the first year after a new diagnosis of attention-deficit /hyperactivity disorder (ADHD) by sex (based on Kaplan–Meier estimates).
Discussion
The current analysis supplements previous regional analyses using healthcare data and representative surveys based on parental reports in providing estimates of prevalence and incidence of new ADHD diagnoses in Germany using a large healthcare database covering the whole of Germany. Furthermore, we assessed the time period for which ADHD diagnoses were continued, and described the initiation of treatment in the new ADHD cases over time, which was not reported in previous studies.
Our analysis of ADHD prevalence used a more conservative algorithm for ascertaining ADHD than previous regional studies based on healthcare data. Still, the obtained estimate was slightly higher than in the previous regional studies (Koster et al. 2004; Schubert et al. 2010). This might indicate the effect of regional differences in Germany, also observed in other countries (Fulton et al. 2009). In comparison with the older of the regional studies, time trends also may play a role (Koster et al. 2004). The age-pattern of prevalence was similar to that in previous reports (Schlander et al. 2007; Schubert et al. 2010) and displayed a wider peak in prevalence, which is also characteristic of more recent years in other studies (Schubert et al. 2010). Overall, the prevalence was lower than the worldwide pooled prevalence of 5.3% (95% CI: 5.0–5.7%) for those <18 years of age estimated by Polanczyk and Rohde (2007), but this might be explained by the differences between ICD and DSM coding systems and prevalence based on surveys using scales rather than records of diagnoses (Dopfner et al. 2008).
Age-specific incidence of new diagnoses of ADHD is not reported in the literature. Based on scale scores, Roberts et al. (2009) reported an overall yearly incidence of 1.18% for symptoms of ADHD for males and females aged 11–17 years, which is only slightly higher than our estimate of 0.9% in the 3–17-year-olds. In general, it has to be kept in mind that diagnostic incidence does not necessarily reflect the true onset of ADHD. Interestingly, in our study there was a continuous increase in the incidence of new diagnoses by age from the age of 3 years rather than a sharp increase at the age of 6 years, which is the typical age of starting school in Germany. Additionally interesting is the abrupt change of the upward trend of new diagnoses at the age of 8 years in boys and 1 year later in girls. These abrupt changes are obscured in the age-specific prevalence and require more attention in future research. Of note is also that new cases of ADHD were diagnosed up to the upper age range of our study (17 years). It is possible that in some cases, previously diagnosed individuals do not visit the doctor and do not receive medication for a longer period. During this time period there is no indication of diagnoses or treatment, and upon their return to the doctor, they will appear as newly diagnosed cases.
The estimated lifetime prevalence calculated from age-specific incidence of new diagnoses exceeded those from survey data in Germany (Huss et al. 2008), but is in line with other studies indicating a very high frequency of ADHD in children and adolescents (Visser et al. 2010). Since the age-specific incidence of new diagnoses in our study was estimated for 2005, the lifetime prevalence reflects diagnostic behavior in 2005. Clearly, the lifetime prevalence will increase when the age-specific incidence of diagnoses increases.
We found that only in approximately two thirds of all cases, records of ADHD diagnoses continued from one age group to the next. Patients for whom records of ADHD diagnoses appeared in the database sought treatment for ADHD (including drugs and other forms of treatment). Although it is possible that there were prescriptions without records of corresponding diagnoses in the database, in general, specific diagnoses are required for prescriptions. At the same time, the lack of records of diagnoses is not equal to the cessation of symptoms. Based on the estimated rates for the persistence of diagnoses, after 2 years, the ADHD diagnoses disappeared in the database for 51% of boys and 63% of girls. Similarly, after 5 years, 83% of boys and 92% of girls would not have records of current ADHD diagnoses. In contrast, the literature indicates a much higher persistence of ADHD symptoms, with even one to two thirds of all cases persisting into adulthood (Weiss et al. 1985; Biedermann et al. 1996; Mannuzza et al. 1998; Surman et al. 2009; Biedermann et al. 2010). A similar disproportion between the treatment cessation and the persistence of ADHD was observed in the United Kingdom (Wong et al. 2009). However, there are forms of treatment that do not result in records of diagnoses in health insurance data; therefore, the picture of treatment cessation is not complete in our database.
Our analysis showed that in 2005, drug treatment was started in some patients with new ADHD diagnoses at the initial diagnosis, but only 37% received at least one prescription of methylphenidate or atomoxetine within 1 year after the initial diagnosis. Previous studies assessed drug treatment of ADHD in a different way – for example as general drug treatment prevalence or the continuity of prescriptions after the first prescription (Habel et al. 2005; Faber et al. 2006) – not addressing the issue of initiation of treatment after the first diagnosis. Currently, there are strong efforts to ensure more strict criteria for stimulant treatment of ADHD in Germany (Gemeinsamer Bundesausschuss 2011). The pattern of initiation of drug treatment might therefore have changed in more recent years. By including drug treatment as one option for the confirmation of outpatient ADHD diagnoses in the case ascertainment algorithm, we possibly introduced some bias toward a higher fraction of drug treatment in our sample, and increased the fraction of those receiving treatment immediately after the first diagnosis.
Strengths and limitations
The main strength of this analysis is the large database, covering all of Germany and a substantial fraction of the German population. The database consists of healthcare records of four SHI companies. Although some selection processes regarding the membership in these companies are possible, the database was shown to be representative for Germany regarding sex and age distribution, hospital admissions, and drug prescriptions (Pigeot et al. 2007; Schink et al. 2009). Drug prescriptions include all prescription drugs covered by health insurance companies, including short- and long-acting methylphenidate and atomoxetine, irrespective of the possible re-imports; therefore no underestimation has to be expected. Unequal geographic coverage of the federal states of Germany was accounted for by using population weights from the Federal Statistical Office. In contrast to the ascertainment of ADHD based on diagnostic scales, the prevalence estimated in this study was based on diagnoses provided by physicians. These records are not subject to reporting bias as are parental reports. On the other hand, the data in the GePaRD were not collected for research but for reimbursement purposes, and may suffer from imprecision of diagnoses or from errors caused by reimbursement modalities. One example of such imprecision is the incomplete coding of qualifiers of diagnoses as “suspicion” or “exclusion.” In order to obtain robust estimates, we used a conservative algorithm for the assessment of ADHD cases, which in turn could have led to an underestimation of the prevalence. Furthermore, the diagnoses recorded by physicians do not reflect the whole spectrum of children and youth with ADHD, only those who seek medical help. Because the data were only available for the period from 2004 to 2006, we were not able to calculate trends of new diagnoses, prevalence, or drug treatment of ADHD. Given that the algorithm considered necessary for the assessment of valid diagnoses required up to 1 year after the incident diagnosis, we were not able to assess directly the continuation of this status in the studied time. The continuation rate of ADHD diagnoses was estimated indirectly from age-specific prevalence and new diagnoses by age. The indirect estimation is based on the assumption of constant rates in time and may be subject to bias in the presence of cohort and period effects. The short period of observation also limited the possibility of assessing whether periods >1 year would substantially change the incidence of new diagnoses. The database is currently being expanded to the years 2007–2009, which will allow direct assessment of continuity of diagnoses in the future. Whereas longer time series will allow additional analyses, the loss to follow-up will increase. Patients can change their insurance provider; in consequence they would appear as lost to follow-up in our database. There is the problem, if they use another insurance also included in the GePaRD, that they will not be recognized as previous patients. For shorter time series as in this study, these processes play a minor role. Finally, drugs licensed for ADHD treatment in Germany include methylphenidate, atomoxetine, and amphetamines. In contrast to in the United Kingdom (Wong et al. 2009) there are unfortunately no specific codes for amphetamines in Germany. Because of the lack of specific coding for amphetamines, we were only able to assess treatment with methylphenidate and atomoxetine, which might have compromised the picture of drug treatment of ADHD in Germany. However, in Germany, the prescription rates for amphetamine to treat ADHD are very low, most probably not exceeding 5% of the treated cases (Wolff 2008).
Conclusions
ADHD is a common condition among children and youth in Germany. There are substantial differences by sex in the prevalence and incidence of new ADHD diagnoses, but only a small difference in drug treatment among those diagnosed with ADHD. In 2005, incidence of new diagnoses increased linearly up to the age of 8 years in boys and 9 years in girls and decreased abruptly thereafter. A relatively low percentage of children received drug treatment in the first year after the initial diagnosis of ADHD. In 9.4%, this treatment was initiated in the same quarter as the initial diagnosis of ADHD. Based on indirect estimation, of those with an ADHD diagnosis at the age of x years, an estimated 61% of girls and 70% of boys have records indicating an ADHD diagnosis at the age of x+1.
Clinical Significance
In addition to the prevalence and incidence of ADHD, this database study provides insight into the treatment pathways of ADHD-initially diagnosed children by showing that two thirds of all patients who received an ADHD diagnosis in 1 year do not appear in the database in the following year. That the proportion of children who received drug treatment at the time of the initial diagnosis increased with age might be an indicator for the higher need of support in school-aged children.
Disclosures
Dr. Banaschewski served in an advisory or consultancy role for Bristol Myers-Squibb, Desitin, Lilly, Medice, Novartis, Pfizer, Shire, UCB, and Viforpharma. He received conference attendance support and conference support or received speaker's fees by Lilly, Janssen McNeil, Medice, Novartis, Shire, and UCB. He is/has been involved in clinical trials conducted by Lilly, Shire and Novartis. The present work is unrelated to the stated grants and relationships. Dr. Garbe served in an advisory or consultancy role for Novartis, Bayer-Schering, and Nycomed. She received research funds for epidemiological studies from Bayer-Schering, Glaxo, Mundipharma, Sanofi-Pasteur, and Sanofi-Aventis. Mrs. Kraut received funding for the annual conference of the German Society of Epidemiology in 2010 from Sanofi-Pasteur MSD. The present work is unrelated to the stated relationships. The other authors declare that they have nothing to disclose.
Footnotes
Acknowledgments
The authors are grateful to all SHIs that provided data for this study: the Allgemeine Ortskrankenkasse (AOK) Bremen/Bremerhaven, the DAK-Unternehmen Leben, the Techniker Krankenkasse (TK), and the hkk. The analysis was conducted within the “German Population Based Long Term Follow-Up of ADHD (GEPOLO-ADHD)” study funded by the Bundesministerium für Bildung und Forschung (BMBF), project number: 01ER0817.