
Abstract
Objective:
Weight gain and metabolic adverse effects of second-generation antipsychotics (SGAs) have become a major concern, particularly in youth. However, the specific contribution of SGAs versus other medications or the underlying illness is unclear.
Methods:
In a chart review study of psychiatric outpatients aged ≤18 years treated with SGAs and psychiatric controls without lifetime SGA, use body mass index (BMI) z-scores between patients and controls were compared in the entire sample, patients without co-medications, diagnostic subgroups, and age subgroups. In patients with follow-up data, weight z-score change was calculated.
Results:
Altogether, 592 Caucasian patients aged 4–18 (mean: 10.0) years with a psychiatric diagnosis were included. BMI z-scores in 96 youth treated with SGAs for 9.0±6.1 months were significantly higher than in 496 patients without lifetime SGA use (0.81±1.1 vs. 0.05±1.2; p<0.0001). BMI z-score differences remained significant in all age groups <16 years old. In sub-analyses, results remained the same after eliminating patients on any co-medication (0.82±1.2 vs. 0.23±1.2; p<0.0001) and in patients with (0.75±1.2 vs. 0.17±1.1, p<0.0001) or without autism spectrum disorders (1.1±1.0 vs. −0.02±1.2, p<0.0001). Significantly more SGA-treated youth were obese (27.1% vs. 9.5%, odds ratio [OR]: 3.55, 95% confidence interval [CI]:2.07–6.08) or overweight (21.9% vs. 8.3%, OR: 3.11, 95%CI: 1.75–5.52). In 24 patients (92.3% antipsychotic-naïve) with 6.6 months follow-up, weight z-score increased significantly from −0.17±1.5 to 0.25±1.4 (p<0.0001) with 12.5% transitioning to overweight or obese status.
Conclusion:
These data show robust and significant differences in sex- and age-adjusted body weight and weight status in young pediatric Caucasian samples with and without use of SGAs independent of Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) (American Psychiatric Association 2000) diagnosis and nonantipsychotic medications. Weight status and metabolic effects of SGAs require careful attention, especially in youth.
Introduction
Nevertheless, the relative contribution of medication side effects, underlying psychiatric illness, and related unhealthy lifestyle behaviors to the increased cardiovascular risk in psychiatrically ill populations is far from clear. It has been argued that pediatric psychiatric patients have a higher baseline weight than healthy youth (Gracious et al. 2010). Adults diagnosed with psychiatric disorders have an increased risk for overweight due to reduced physical activity, unhealthy food intake, or medication side effects compared with the general population (Brown et al. 1999). Similarly, in European studies, an elevated risk of weight gain, obesity, and metabolic side effects has been reported in pediatric patients with bipolar disorder and psychotic disorders using SGAs. (Schimmelmann et al. 2007; Arango et al. 2009; Moreno et al. 2010) On the other hand, European data are missing regarding the risk of overweight in pediatric populations with a psychiatric diagnosis with and without use of SGAs.
It is important to examine both the preantipsychotic treatment risk of overweight and obesity in a European pediatric psychiatric sample as well as metabolic side-effects of SGAs, because there are several population differences between Europe and the United States. Data about these important side-effects in youth are scarce and, at this moment, mainly from the United States. First, the prevalence of overweight children and adolescents is lower in the Netherlands (Hurk van den et al. 2007) compared with the United States (15 vs. 31.7%) (Ogden et al. 2010). Furthermore, while 3% of the Dutch pediatric population meets the criteria for obesity (Hurk van den et al. 2007), obesity is present in as many as 16.9% of youth in the United States (Ogden et al. 2010). Second, people with a Hispanic or Afro-American background, who are much more prevalent in the United States, are at a greater risk than Caucasian people to develop overweight or obesity and cardiometabolic morbidity (Winkleby et al. 1999).
To address this gap in the literature, we performed a retrospective chart review study, with the main aim of testing the hypothesis that body mass index (BMI) z-scores will be significantly higher in children and adolescents diagnosed with a psychiatric disorder using SGAs, compared with psychiatrically ill children and adolescents never treated with SGAs. In children and adolescents, risperidone is the most prescribed SGA. By choosing a control group of pediatric psychiatric patients never treated with SGAs, possible differences in BMI z-scores and weight status due to the use of SGAs can be distinguished from factors that are related to having a psychiatric disorder. As a further aim, we sought to evaluate whether diagnoses, comedications, or patients' age affected the findings.
Methods
Data collection and sample
Data were collected by a chart review from a cross-sectional sample of patients from the outpatient clinic of the department of child and adolescent psychiatry of the University Medical Center (UMC) in Utrecht between May 2009 and May 2010. The UMC Utrecht has a catchment area of approximately 1.2 million people and is a tertiary academic center for child and adolescent psychiatry, with a specialization in the field of autism and disruptive spectrum disorders. Patients are referred by general practitioners, psychologists, and other psychiatric services. Data for this report were restricted to pediatric outpatients <18 years using SGAs for at least two weeks and a control group of pediatric psychiatric outpatients never treated with SGAs. When available, the duration of the use of SGAs was assessed. All patients were diagnosed with a DSM-IV-TR (APA, 2000) psychiatric diagnosis based on clinical assessment of the treating physician. In order to compare different diagnostic groups, patients were divided in different categories based on into different categories based on the clinically most important, primary diagnosis according to DSM-IV-TR criteria (i.e., autism spectrum disorders [ASDs], disruptive behavior disorders, mood disorders, tic disorders, and schizophrenia spectrum disorders). We assessed body weight, height, ethnicity, co-medications, and psychiatric diagnoses by a chart review. A total of 1234 patient records were screened, of which 592 individual patient records were included in the analyses (Fig. 1). Exclusion was based on missing weight data, presence of major somatic illness that could influence weight (e.g., Hashimoto thyroiditis, Sotos syndrome, dysfunctional hypophysis, Bardet Biedl syndrome, undefined growth disorder, and Duchenne’s disorder), treatment with SGAs for 0–2 weeks. 496 patients who never used SGAs, and 96 used SGAs for more than 2 weeks.
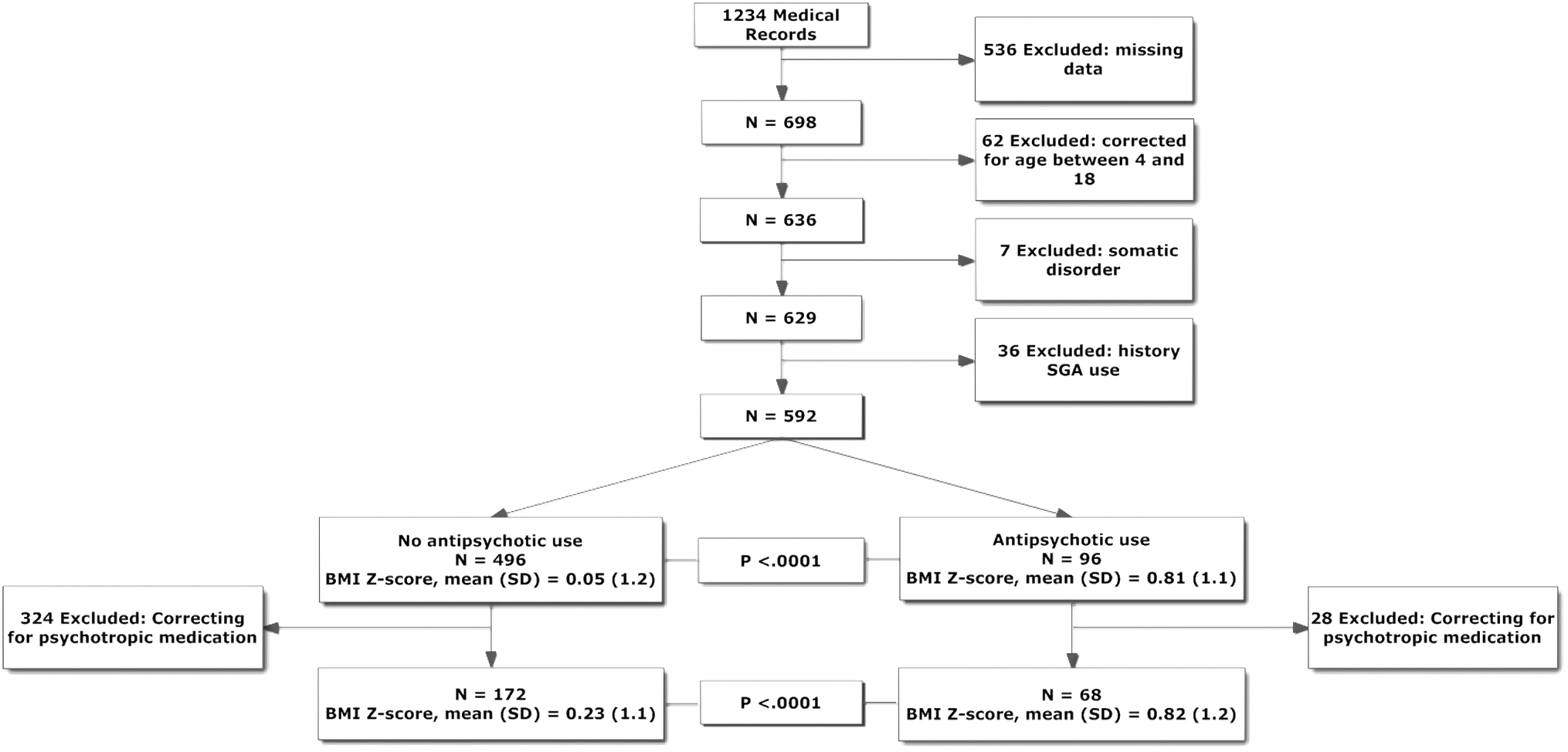
Flow of patients. SGA=second-generation antipsychotics. BMI=body mass index, SD=standard deviation.
Outcome variables
The main outcomes were sex- and age-adjusted weight z-scores, BMI z-scores, and weight status based on BMI percentile grouping, which were all calculated based on a Dutch reference group (Fredriks et al. 2000). Descriptive statistics and tests for normal distribution were performed, including age and gender differences. Weight status was calculated by categorizing the BMI percentiles as follows: patients are underweight when the BMI percentile is below the 5th percentile, between the 5th and <85th percentile is normal weight, between 85th and <95th percentile is overweight, and at or above the 95th percentile the patients are classified as obese (Correll 2008b).
Statistical analyses
In addition to descriptive statistics, categorical and continuous outcomes were analyzed with chi-squared tests and independent samples t-tests, respectively. In the primary analyses, average weight z-scores and BMI z-scores were compared between patients using SGAs for more than 2 weeks (SGA group) and those not using SGAs (nonSGA group). In secondary analyses, proportions of patients in each of the weight status categories (underweight, normal weight, overweight, and obese) were compared across the two treatment groups.
In addition, sensitivity analyses were performed to exclude the influence of co-medications that are known to have an influence on weight, such as methylphenidate and selective serotonin reuptake inhibitors (SSRIs). Moreover, since there was a relatively large group of SGA-treated youth with ASD (81.3%) compared with other study samples (Correll et al. 2009, Laita et al. 2007, Olfson et al. 2006), subgroup analyses were conducted in patients with and without ASDs as well as in different age groups (4–8, 9–11, 12–15 and 16–18 years old).
Finally, to gain further insight in the weight effects of SGAs over time, follow-up data were also collected. Patients with antipsychotic-free baseline and follow-up weight data were used for longitudinal analyses. In these patients, no data of height measurements were available at follow up, resulting in the sole analysis of weight z-scores in the prospective sample. In addition to descriptive statistics, categorical and continuous outcomes were analyzed with chi-squared tests and post hoc t-tests, respectively. This chart review study was approved by the local ethics committee.
Results
Demographic and illness characteristics in the entire sample
The SGA group was significantly older than the nonSGA group (10.9±3.1 years vs. 9.8±3.3 years, p=0.003), and consisted of more males (91.7% vs. 80.8%, p=0.01) and youth of Caucasian race (100% vs. 95.2%, p=0.028), but both groups were predominantly Caucasian (Table 1). In the nonSGA group, the most prevalent diagnosis was a disruptive behavior spectrum disorder (ADHD, ODD) (55.0%). In the SGA group, ASD (autism, Asperger's disorder, pervasive developmental disorder not otherwise specified (PDD-NOS)) was the most prevalent diagnosis (81.3%).
SGAs=second generation antipsychotics, BMI=body mass index, SD=standard deviation.
Diagnosed by Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) Criteria.
Including autism, Asperger's disorder, pervasive developmental disorder not otherwise specified (PDD-NOS).
Including attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder
Including bipolar disorder, depression, anxiety disorder.
Including schizophrenia, psychosis.
Fredriks et al. 2000.
Based on BMI percentile.
The predominantly prescribed SGA was risperidone (82.3%). Patients were treated with antipsychotics for an average of 9.0±6.1 months (median of 8.5 months) before the study assessment (in 26 patients, data on the duration of antipsychotic use were missing) (Table 1).
BMI z-scores and weight status in the entire sample
Weight status of both groups was categorized by calculating BMI percentiles. SGA and nonSGA groups did not differ regarding underweight (P=0.121). Significantly fewer patients on SGAs were of normal weight (47.9% vs. 74.8%, p<0.0001, odds ratio [OR]=0.31, 95% confidence interval [CI]: 0.20–0.49), and significantly more SGA-treated patients were overweight (21.9% vs. 8.3%, p<0.0001, OR=3.11, CI: 1.75–5.52), or obese (27.1% vs. 9.5%, p<0.0001, OR=3.55,CI: 2.07–6.08), as well as obese or overweight (48.9% vs. 17.7%, p<0.0001) (Table 1).
Comparison in mean sex- and age-adjusted weight z-scores and BMI z-scores between the treatment groups showed both a significantly larger weight z-score (0.77±1.1 vs. −0.09±1.3, p<0.0001) and BMI z-score in the SGA group (0.81±1.1 vs. 0.05±1.2; p<0.0001). In a more stringent sensitivity analysis of patients without any co-medication (nonSGA group: n=172; SGA monotherapy group: n=68), patients on SGA monotherapy had significantly higher weight z-scores (0.75±1.2 vs. 0.10±1.3; p<0.0001) and BMI z-score (0.82±1.2 vs. 0.23±1.1; p<0.0001).
BMI z-scores and weight status in patients with ASD
Since there was a significant difference in the most prevalent diagnoses between the SGA group (predominantly ASDs) and the nonSGA group (predominantly DBDs), we repeated the analyses of BMI z-scores and weight status in the group of patients with and without ASDs (Table 2) to eliminate a potential confound due to psychiatric illness. Data of the ASD group and nonASD group were compared, both in SGA-treated youth and those not treated with SGAs.
Based on Fredriks et al. 2000.
BMI=body mass index; SGA=second-generation antipsychotics; SD=standard deviation.
SGA treated youth were significantly older than nonSGA treated youth in both the ASD group (p=0.016) and in the nonASD group (p=0.018). BMI z-scores and weight status of children with an ASD without using SGAs did not differ compared with the other diagnostic groups. Regarding weight status approximately the same results were found between the SGA and non-SGA-treated patients in the ASD group as in the entire sample: there was no significant difference regarding underweight (6.2% vs. 3.8%, p=0.450) and overweight (9.6% vs. 19.2%, p=0.031). However, patients with normal weight (73.6% vs. 51.3% p<0.001), obesity (10.7% vs. 25.6%, p=0.002), and overweight and obesity (20.2% vs. 44.9%, p<0.001) differed significantly between the non SGA versus the SGA-treated patients (Table 2).
Similar to the results in the entire sample, the SGA-treated group had significantly greater weight z-scores (0.71±1.1 vs. 0.06±1.3, p<0.0001) and BMI z-scores (0.75±1.2 vs. 0.17±1.1, p<0.0001) (Table 2). The same was true for the nonASD group (weight z-score: 0.99±1.1 vs. −0.17±1.3, p<0.0001; BMI z-score: 1.1±1.0 vs. −0.02±1.2, p<0.0001). In addition, similar to the results in the entire sample, SGA-treated patients were significantly less likely to be in the normal weight category and significantly more likely to be overweight, obese, or overweight/obese, with ORs between 2.2 and 3.3 in the ASD group and ORs between 5.1 and 10.3 in the nonASD group, mainly consisting of DBDs.
BMI z-score differences in specific age groups
BMI z-scores were significantly higher in the SGA group in all age groups younger than 16 years old (Fig. 2). The BMI z-score was 0.498 higher (p=0.008) in patients 4–8 years old, 0.838 higher (p<0.0001) in patients 9–11 years old, and 0.790 higher (p=0.002) in patients 12–15 years old. In the oldest and smallest age group of 16–19 years old (n=9), the BMI z-score difference of 0.202 did not reach statistical significance (p=0.672).
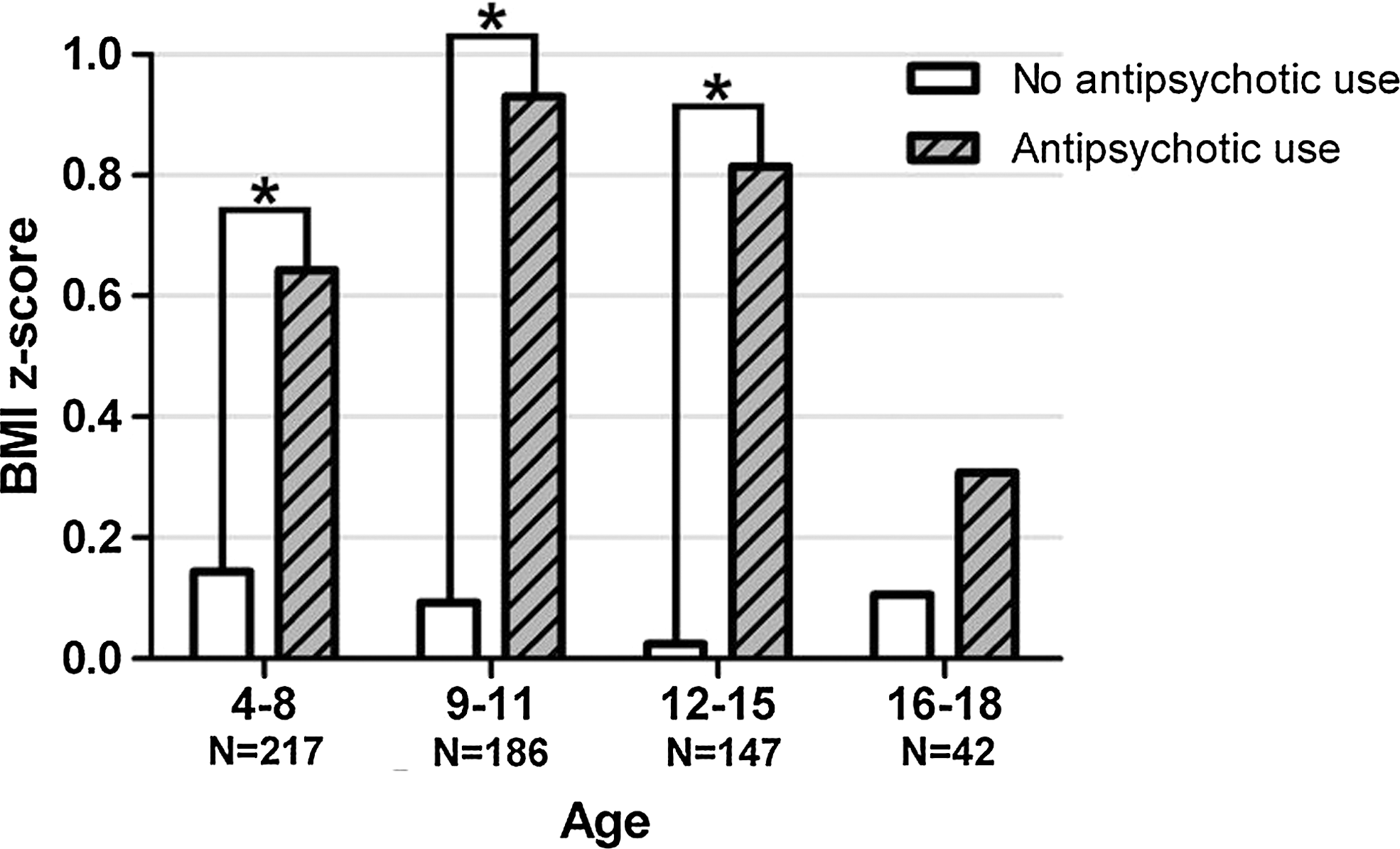
Age categorization of patients with and without the medication of antipsychotics. *=p<0.05.
Follow-up data
In 24 patients (96.3% antipsychotic-naive), antipsychotic-free baseline and follow-up weight data were available (Table 3). The mean follow up after initiating the antipsychotic was 6.6±6.1 months. Longitudinal height measurements were missing. Ten patients (41.7%) were treated with antipsychotic mono-therapy. Fourteen patients also received co medications, including SSRIs (4 patients), methylphenidate (4 patients), and other medications (6 patients) that could influence weight. After SGA treatment, weight z-scores increased significantly (p<0.0001) from 0.17±1.5 to 0.25±1.4 (Table 3). Two patients (8.3%) shifted from overweight to obese weight status, 1 (4.2%) shifted from normal to overweight status, and 1 (4.2%) patient shifted from underweight to normal weight status.
Diagnosed by DSM-IV Criteria.
Including autism, Asperger's disorder, pervasive developmental disorder not otherwise specified (PDD-NOS).
Including attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder
Including bipolar disorder, depression, anxiety disorder.
Including schizophrenia, psychosis.
Fredriks et al. 2000.
Based on weight percentiles, same cut-offs as in BMI weight status.
Benzodiazepine's, biperiden, desloratadine, levothyroxine, and lithium.
Discussion
Pediatric patients using SGAs (mainly risperidone, i.e., 82.3%) had significantly higher sex- and age-adjusted body weight and BMI compared with psychiatrically ill pediatric patients not treated with SGAs. This effect was independent of major psychiatric diagnosis and co-medications, and appeared to be the strongest in the age groups below age 16 (although the power in the oldest age group was small).
With this study, we provide data from a young (overall mean: 10.0 years) European pediatric sample with weight differences in patients with and without lifetime use of SGAs. These data are consistent with previous results from much smaller European samples in which SGA-related weight gain was observed in mainly Caucasian adolescents with bipolar and psychotic disorders (Schimmelmann et al. 2007; Arango et al. 2009; Moreno et al. 2010). In contrast, our sample consisted mainly of children with autistic spectrum disorders treated with risperidone. In The Netherlands the guidelines of the Dutch Association of Psychiatry recommend risperidone as the drug of first choice for children with autism spectrum disorders because the largest body of evidence for efficacy is available from studies with risperidone (Shea et al. 2004; RUPP Autism Network 2002; Nagaraj et al. 2006; Luby et al. 2006). Also, in The Netherlands risperidone is the only SGA approved for behavioral problems in children from the age of 5 years by the Dutch Medicines Evaluation Board (CBG, College ter beoordeling van geneesmiddelen). The other SGAs and typical antipsychotics are prescribed off-label.
Interestingly many U.S. reports describe other diagnostic groups of patients treated with SGAs. Since we had included a control group of children with psychiatric diagnoses not treated with SGAs and, in a subgroup analysis, not treated with any medications, we were able to distinguish the effects of SGA-treatment on BMI z-scores and weight status from effects related to having a psychiatric disorder. Interestingly, the psychiatric antipsychotic-naïve control group in our study already had a higher prevalence rate of obesity (9.5%) than the population-based sample of Dutch children (3%). However, compared with nonSGA treated psychiatrically ill youth, those treated with SGAs had an even higher prevalence rate of obesity (27.1 vs. 9.5%, OR: 3.55) and of overweight (21.9% vs. 8.3%, OR: 3.11). This implies that mental illness itself, illness related unhealthy lifestyle behaviors and/or nonantipsychotic treatments can adversely affect body weight status, but that the antipsychotic-related weight gain considerably adds to this burden in already vulnerable patients (Laita et al. 2007; Correll 2008a,b; Correll et al. 2009; Gracious et al. 2010) The fact that this significant antipsychotic effect was apparent after a mean exposure of only 9.0 months is even more worrisome. The strong and early effect of SGAs, predominantly risperidone in our study, was confirmed in our small prospective subsample in which the weight z-score increase was 0.42 over 6.6 months, replicating results from other prospective data sets in children and adolescents receiving antipsychotics (Fraguas et al. 2011). Since our prospective subsample was relatively small, we did not have sufficient data to evaluate the effect of duration of SGA-use on change in BMI z-score. Earlier studies reported that patients unexposed to antipsychotics are particularly vulnerable to weight gain, and this weight gain begins in the first few weeks (Correll et al. 2009; Tarricone et al. 2010; De Hert et al. 2011).
These findings are generally similar to recent results from another cross-sectional psychiatrically ill U.S. sample (Gracious et al. 2010). Of 114 partially hospitalized youth (mainly Caucasian 84%) aged 12–18 years old, 30.0% were obese and 25.4% were overweight. Of note, only 15% of this group were treated with SGAs. Although other factors, such as smoking, antidepressant use, lack of private insurance, and absence of stimulant treatment, were also associated with overweight/obese status in this sample, antipsychotic exposure was significantly associated with overweight/obese status (OR=4.3 (95%CI: 1.0–18.7). The fact that in this U.S. sample, the rates of overweight and obesity were comparable to our European Caucasian sample in which 100% had been exposed to SGAs suggests that in the United States, additional ethnic (Winkleby et al. 1999) and/or lifestyle factors increase cardiovascular risk status in psychiatrically ill youth even more and beyond antipsychotic exposure. This interpretation is supported by a comparison of the weight z-score increase of 0.42 in our prospective subgroup of 96.3% antipsychotic-naive youth treated predominantly with risperidone with a BMI z-score gain of 0.60 in a U.S. cohort of 100% antipsychotic-naive youth treated with risperidone for half of the time (10.6 weeks) (Correll et al. 2009).
The results of this study need to be interpreted with several limitations in mind. First, this is a retrospective chart review study with all its limitations, including the reliance on chart recorded height and weight data and a limited number of patients with full height and weight information. There were also limited data about co-morbidity, as only primary diagnosis is systematically recorded in the file. It is most likely that the high rate of incomplete data records is a result of lack of a standardized monitoring protocol in this medical center. In clinical practice, patients on medication are more systematically monitored than patients without medication. Second, the control group had a high proportion of disruptive behavior disorder subjects, in which a lower weight status can be expected due to hyperactivity or use of stimulants. Nevertheless, this control group did not have a significantly lower weight status compared with the general Dutch pediatric population; by contrast, there was even a higher prevalence of overweight and obesity. Third, we had only limited longitudinal data available. Fourth, the sample consisted mostly of risperidone treated youth, limiting the ability to compare effects of different antipsychotics, and we did not have any metabolic data to assess the impact of the differences in BMI z-scores and weight status on metabolic health. Finally, we did not have data to assess the mechanism of the weight gain, including its potential relationship to changes in food intake, food choice, exercise behaviors, energy expenditure, or resting metabolic rate. Fifth, since the largest group of patients consisted of patients with ASDs, firm conclusions about other diagnostic groups cannot be drawn. Sixth, we did not include measurement of peptides and markers, such as leptin (Correll et al. 2011), that have been associated with weight gain in risperidone-treated youth (Calarge et al. 2009). Seventh, the sample of the antipsychotic naive subsample followed for 6.6 months was relatively small, calling for extended study data in this particularly vulnerable patient group.
Nevertheless, our study results are strengthened by the fact that we included a psychiatric control group and that we excluded any previous or concurrent treatment with any other psychotropic medications that could influence weight status independent of or synergistic with SGA effects. The question can be raised whether the results of this study are mainly applicable for patients with ASDs. From the literature, there is no indication that children with ASDs have specific metabolic risk profiles that predict overweight or obesity. To date, it is not clear to what degree vulnerability for antipsychotic-induced weight gain is related to diagnosis, previous antipsychotic exposure, or younger age (Correll et al. 2011; De Hert et al. 2011). Moreover, despite the methodological limitations, the robust, significant differences in BMI z-scores and weight status in the SGA treatment group, together with previous findings that, at least in the beginning of treatment, all SGAs appear to have a significant adverse effect on body weight, suggests that the prescription of SGAs in children and adolescents should be limited to those youth in whom other appropriate interventions have failed (Correll 2008a,b; Correll et al. 2009). Unfortunately, it has to be acknowledged that even with a more conservative treatment approach, large numbers of children and adolescents will need treatment with SGAs because of the severity of the psychiatric symptoms and because alternative treatment may be lacking or ineffective. As known from the literature, important individual differences exist in terms of the liability of different antipsychotics for weight gain and metabolic side effects (Correll 2008a,b; Correll et al. 2010; Fraguas et al. 2011). In addition, there also exist differences in the individual susceptibility to weight gain of SGA treatment (Chagnon et al. 2004). This demands a pharmacogenomic approach in order to indentify predictors and mechanisms of antipsychotic-induced weight gain, which could help guide a more individualized prescribing and section of patients and medications. (Correll et al. 2011) However, even simpler tools are available and should also be used. Data exist showing that early weight gain is a robust predictor of later weight gain (Maayan and Correll 2010). Body weight, fasting glucose, and lipids as well as blood pressure and healthy lifestyle behaviors need to be monitored proactively and routinely, especially in the particularly sensitive children and adolescents receiving antipsychotic treatment (Correll 2008b). Although the need for monitoring has been widely publicized, recent data suggest that monitoring practices in youth treated with antipsychotics are low and not much higher than in nonpsychiatric controls treated with albuterol (Moratto et al. 2010). Moreover, although in this large pharmacoepidemiologic sample, glucose and lipid abnormalities were about twice as prevalent in the antipsychotic treated psychiatrically ill youth, the prescription of glucose and lipid modifying medications was not greater compared with the nonpsychiatric control subjects, indicating undertreatment of the sensitive psychiatric population. These data indicate that the field needs to find ways not only to identify pathways and mechanisms for antipsychotic adverse effects on body weight, glucose, and lipid metabolism in order to develop safer medications and treatments to mitigate these side effects with enormous health importance, but also to improve clinician driven monitoring and management of antipsychotic-related cardiovascular side effects, especially in youth.
Conclusion
These data show significantly greater sex- and age-adjusted body weight and abnormal weight status in a young pediatric Caucasian sample treated with SGAs compared to those not receiving SGAs. This effect was persistent after correction for the primary DSM-IV-TR diagnosis and nonantipsychotic medications. In addition, this study provides additional information about European youth with an ASDs and about youth with psychiatric disorders not taking antipsychotic medications. Therefore, these results strengthen the notion that weight status and metabolic effects of SGAs require careful attention, especially in youth.
Clinical Significance
Adverse effects of SGA treatment in youth have been documented in samples in the United States. Here, we provide data from a large European sample of psychiatrically ill children and adolescents treated with SGAs (mainly risperidone) compared with an untreated psychiatric comparison group. Our data show robust differences in BMI z-score and weight status as well as clinical and statistical significant increases in the prospectively followed subgroup. In addition, this study provides data on youth with an ASD, a diagnostic group in which the weight effects of SGAs are not well documented. Finally, our data also show that children and adolescents with a psychiatric disorder and no antipsychotic exposure have an increased BMI z-score compared with healthy children and adolescents from the general population, indicating that, in addition to medication effects, illness and lifestyle factors may play a relevant role. This suggests that regular weight monitoring of psychiatrically ill youth should be mandatory, with added metabolic monitoring in those youth receiving medications that can adversely affect metabolic health, especially antipsychotics, and in those youth who are overweight or obese or gain significant amounts of weight that is in excess of expected weight gain as a part of normal development.
Disclosures
Dr. Correll has been a consultant and/or advisor to or has received honoraria from: Actelion, AstraZeneca, Biotis, Bristol-Myers Squibb, Cephalon, Desitin, Eli Lilly, IntraCellular Therapies; Ortho-McNeill/Janssen/J&J, Merck, Novartis, Otsuka, Pfizer, and Sunovion. He has received grant support from the Feinstein Institute for Medical Research, the National Institute of Mental Health (NIMH), and the National Alliance for Research in Schizophrenia and Depression (NARSAD), BMS/Otsuka and Ortho-McNeill/Janssen/J&J. The other authors have no conflicts of interest to disclose.
Footnotes
Acknowledgments
Wouter G Staal gratefully acknowledges the Netherlands Brain Foundation for sponsoring his research. The authors gratefully acknowledge Dr. Paula van Dommelen, statistician at TNO Quality of Life, for her assistance in calculating BMI z-scores according to the Dutch Growth Study.