
Abstract
Objective:
The purpose of this article was to describe the relationships between parent-rated executive function (EF) and clinician-rated attention-deficit/hyperactivity disorder (ADHD) symptoms before and after lisdexamfetamine dimesylate (LDX) treatment in children with and without EF deficit.
Methods:
In post-hoc analyses of children with ADHD who participated in a 7 week open-label, dose-optimized (LDX 20–70 mg/day) trial, ADHD Rating Scale-IV (ADHD-RS-IV) change scores were compared (using two-sample t tests) between youth with and without clinically significant EF impairment at baseline. Clinically significant impairment was defined as parent-rated Behavior Rating Inventory of EF (BRIEF) Global Executive Composite (GEC) t scores ≥65. Relationships between baseline and endpoint BRIEF and ADHD-RS-IV scores were examined using Pearson correlations and generalized effect linear model. Safety assessment included treatment-emergent adverse events (TEAEs).
Results:
At baseline, 265/315 participants (84.1%) had a clinically significant BRIEF score. Their mean (SD) ADHD-RS-IV total score at baseline was 42.1 (6.64) for those with, and 36.5 (6.67) for those without, clinically significant BRIEF. At endpoint, ADHD-RS-IV total and subscale scores were significantly improved (p<0.0001) for both those with and those without clinically significant baseline BRIEF scores. Moderately strong, positive Pearson correlations were observed between BRIEF and ADHD-RS-IV total and subscale scores. In the generalized effect linear model, ADHD-RS-IV change scores were significantly correlated with endpoint BRIEF scores (r 2=0.35, β=0.73, p<0.0001). In the subgroup without clinically significant BRIEF t scores at endpoint, parents and clinicians rated 90% and 95%, respectively, as improved. In the subgroup with clinically significant BRIEF t scores at endpoint, parents and clinicians rated 69% and 78%, respectively, as improved. TEAEs were experienced by 269/318 (84.9%) participants; most (82.7%) experienced events mild to moderate in intensity. A total of 12/318 (4.1%) participants discontinued because of TEAEs.
Conclusion:
Clinically significant impairment of EF behaviors in children with ADHD was associated with more severe ADHD symptoms. LDX therapy improved ADHD symptom severity, and at endpoint, fewer participants displayed impairment of EF behaviors (versus baseline). The parent-rated BRIEF may describe clinically important EF behaviors not assessed by the 18-item ADHD-RS-IV.
Introduction
Because of the ease of administration and sensitivity to functional changes that may occur with treatment, behavioral rating scales of EF may have broad clinical utility, both for initial assessment and for gauging effectiveness of treatment regimens (Toplak et al. 2009). Recent findings confirm that behavioral rating scales of EF not only detect impaired EF behaviors but are also sensitive to changes in EF behaviors during ADHD pharmacotherapy in both children and adults (Biederman et al. 2008; Qian et al. 2007; Brown and Landgraf 2010; Gau and Shang 2010; Brown et al. 2011). In one small 4–6 week open-label trial of once-daily osmotic-release oral system (OROS®) methylphenidate in children with ADHD, BRIEF subscores were significantly reduced (e.g., improved) with active treatment (Qian et al. 2007). Similar treatment-related improvements in EF behaviors, based on the BADDS, with administration of a once-daily formulation of mixed amphetamine salts (MAS), have been reported from two large clinical trials in children with ADHD (Brown and Landgraf 2010). In a 7 week, open-label, dose-optimized trial in children with ADHD, lisdexamfetamine dimesylate (LDX) (Vyvanse [package insert] 2012) was effective in reducing ADHD symptoms (as assessed by the ADHD Rating Scale IV [ADHD-RS-IV]), and improving EF behaviors (Findling et al. 2009). Other reports suggest EF improvements also occur with nonstimulant, atomoxetine therapy for ADHD (Gau and Shang 2010; Brown et al. 2011).
Although the parent-rated BRIEF and the clinician-rated ADHD-RS-IV are clinically useful and responsive indicators of change during ADHD treatment (Findling et al. 2010; Turgay et al. 2010; Biederman et al. 2011), information is lacking on whether either assessment alone is sufficient to thoroughly assess patient improvement. Hence, determining the relationship between these instruments, focusing on the overlap in these measures in assessing overall improvement, may provide additional insight on how to meaningfully assess treatment response. A better understanding of how EF changes typically detected with these instruments during standard ADHD pharmacotherapy are related to measures of core ADHD symptoms, and whether EF measures contribute unique clinical information to that obtained by ADHD symptom rating scales when used alone, may contribute to the understanding of how to assess patient improvement in the clinical setting.
The objective of the current post-hoc analysis of a 7 week, open-label LDX trial was to examine the relationship between the investigator-rated ADHD-RS-IV and parent-rated BRIEF when used to assess ADHD symptoms and EF behavioral impairments, respectively, in children with or without executive function deficits (EFD) at baseline. We propose that ADHD symptom improvement may be observed with LDX treatment irrespective of whether participants exhibited EFD at baseline. Moreover, we suggest that individuals whose behavioral EF impairments fail to respond well to treatment may likewise demonstrate less robust treatment effects on ADHD symptoms.
Methods
Study design overview
The post-hoc analyses presented here were conducted on data from an open-label, multicenter, prospective, 7 week, dose-optimized study of LDX (20–70 mg/day) in children with ADHD (Findling et al. 2009). The trial consisted of four phases: 1) screening and washout (1–2 weeks); 2) open-label, dose-optimization; 3) maintenance (7 weeks); and 4) safety follow-up (30±5 days). Following the baseline visit, participants were initiated on 20 mg/day LDX and reported to the site weekly for 7 weeks (weeks 1–7) thereafter. For participants who did not demonstrate an effective response, defined as a ≥30% decrease from baseline in ADHD-RS-IV total score and a Clinical Global Impressions-Improvement (CGI-I) (Guy 1976) score of 1 or 2, doses were increased (in 10 mg increments) up to 70 mg/day, when dose increases were tolerable. Dose escalations were not permitted past week 5. If a participant experienced intolerable effects, the dose was down-titrated to the next dose level (only 1 downward dose taper was allowed). Participants with acceptable response and no intolerable effects were maintained on that dose for the remainder of the study.
The trial was performed in accordance with applicable regulations and applicable International Conference on Harmonization of Good Clinical Practice (ICH GCP) guidelines and with approval of the local internal review board. All study participants and their parents or legal guardians provided written informed consent prior to the conducting of any study procedures.
Inclusion/exclusion criteria
Detailed inclusion and exclusion criteria have been described previously (Findling et al. 2009). Briefly, the trial enrolled medically healthy children aged 6–12 years with a primary diagnosis of ADHD who were free of most psychiatric comorbidities and who had a baseline ADHD-RS-IV total score ≥28.
Symptom and EF assessments
Assessments of symptom severity included the ADHD-RS-IV (DuPaul et al. 1998; Faries et al. 2001), CGI-I scales (Guy 1976), the Parent Global Assessment (PGA) scale, and the parent-rated BRIEF (Gioia et al. 2000). The clinician-rated ADHD-RS-IV consists of 18 items that directly assess the presence of DSM-IV-TR-defined ADHD diagnostic symptom criteria. CGI-I ratings reflect improvement from baseline using a 7 point scale (1 [very much improved] to 7 [very much worse]). The PGA (a parent-rated variation of the CGI-I) reflects parent-assessed change from baseline symptoms using a 7 point scale (1 [very much improved] to 7 [very much worse]). CGI-I and PGA scores of 1 (very much improved) and 2 (much improved) indicate “improvement.”
The parent-rated BRIEF, completed at baseline and final study visit, consists of 86 items rated 1 (never), 2 (sometimes), or 3 (often), with higher scores reflecting poorer functioning. The scale is divided into eight subscales, which in turn are used to calculate two index scores: Behavioral Regulation Index (BRI), based on three subscales (inhibit, shift, and emotional control) and Metacognition Index (MI), based on five subscales (initiate, working memory, plan/organize, organization of materials, and monitor) (Gioia et al. 2000). BRI has been considered a scaled measure of the propensity of inhibitory control to modulate emotions and behavior and the ability to shift from one situation or activity to another as necessary. The MI assesses the ability to use working memory to “initiate, plan, organize, and sustain future-oriented problem solving” (McCandless and O'Laughlin 2007). BRI and MI scores are combined to yield a Global Executive Composite (GEC) score. All scores are transformed and reported as t scores, with the normative group mean established as a value of 50, and the normative group SD set at 10 (Gioia et al. 2000). Scores with a value ≥1.5 SD above the mean (BRIEF GEC t-score ≥65 at baseline) represent a level of EFD considered clinically significant, with those<1.5 SD above the mean (BRIEF GEC t-score<65 at baseline) considered not clinically significant (Gioia et al. 2000).
Statistical analyses
All participants who received ≥1 dose of LDX and had ≥1 postdose ADHD-RS-IV assessment were included in the primary analyses that examined the effects of LDX in this study. The participants were dichotomized post hoc, based on BRIEF GEC scores, as having or not having EFD (t score ≥65 versus t score<65) at 1) baseline and 2) endpoint, in order to examine the relationship of EF (based on BRIEF scores) to ADHD symptoms (based on ADHD-RS-IV scores). ADHD-RS-IV scores at baseline, endpoint, and change from baseline were then assessed by both baseline and endpoint EFD categories. For ADHD-RS-IV total and subscale scores, endpoint versus baseline scores were compared within EFD categories based on paired t tests. Comparisons of ADHD-RS-IV endpoint change from baseline between the EFD categories were made using a two-sample t test. CGI-I and PGA scores were analyzed both within and between the EFD categories using the same methods as were applied to ADHD-RS-IV scores. No multiplicity adjustment was performed on the subgroup statistical comparisons.
Pearson correlation coefficients were determined to describe the relationship between BRIEF scores (GEC, BRI, MI scores, all eight subscale scores) and ADHD-RS-IV scores (total, inattention, and hyperactivity/impulsivity subscale scores) at baseline, endpoint, and for endpoint change from baseline; correlation statistical significance was examined based on one-sample t tests, with level of significance set at p<0.05. Pearson correlation coefficients were computed with p value defined as a result of testing the correlation coefficient as 0 for each pair of data. Further analysis was conducted using a generalized linear model that assessed whether the observed variance of the dependent variable (endpoint change from baseline in BRIEF GEC scores) can be explained by the explanatory variables. ADHD-RS-IV total and subscale scores are the independent variables in the model.
Safety was assessed in the safety population of the parent study (all enrolled participants who took ≥1 dose of LDX) based on frequency and severity of treatment-emergent adverse events (TEAEs; adverse events [AEs] with onset after first date of treatment and no later than 3 days following termination of treatment).
Results
Study population
A total of 318 participants were enrolled; 316 (99.4%) participants received ≥1 dose of LDX and had ≥1 postdose ADHD-RS-IV assessment, and 278 (87.4%) completed the study. Mean (SD) age of participants was 9.1 (1.9) years; 70.7% were male and 70.7% were white. A diagnosis of ADHD combined subtype was seen in 81.7% of participants. The sample overall exhibited a mean (SD) ADHD-RS-IV total score at baseline of 41.2 (6.9).
Baseline and endpoint BRIEF categories
At baseline, 265 of 315 evaluable participants (84.1%) were classified as exhibiting EFD (BRIEF GEC t-score ≥65) versus 50 (15.9%) classified as not exhibiting EFD (BRIEF GEC t-score<65). At endpoint, 78 of 308 (25.3%) participants had EFD, whereas 230 (74.7%) did not. There were 308 participants who had both baseline and endpoint BRIEF GEC scores. Of these, 260 were identified with EFD at baseline, and of these, 187 were without EFD at endpoint. Of 48 participants without EFD at baseline, 5 had EFD at endpoint.
ADHD-RS-IV symptom outcomes by baseline BRIEF GEC categories
As shown in Figure 1, participants with EFD at baseline had higher baseline ADHD-RS-IV total scores than did those without baseline EFD. After the 7 week open-label LDX treatment, participants in both groups exhibited similar endpoint ADHD-RS-IV total scores. The mean reduction from baseline ADHD-RS-IV total score was significantly greater for LDX-treated participants with baseline EFD than for LDX-treated participants without EFD (p=0.004) (Fig. 1). A similar pattern of results was seen with ADHD-RS-IV subscales of inattention and hyperactivity/impulsivity (Fig. 1).
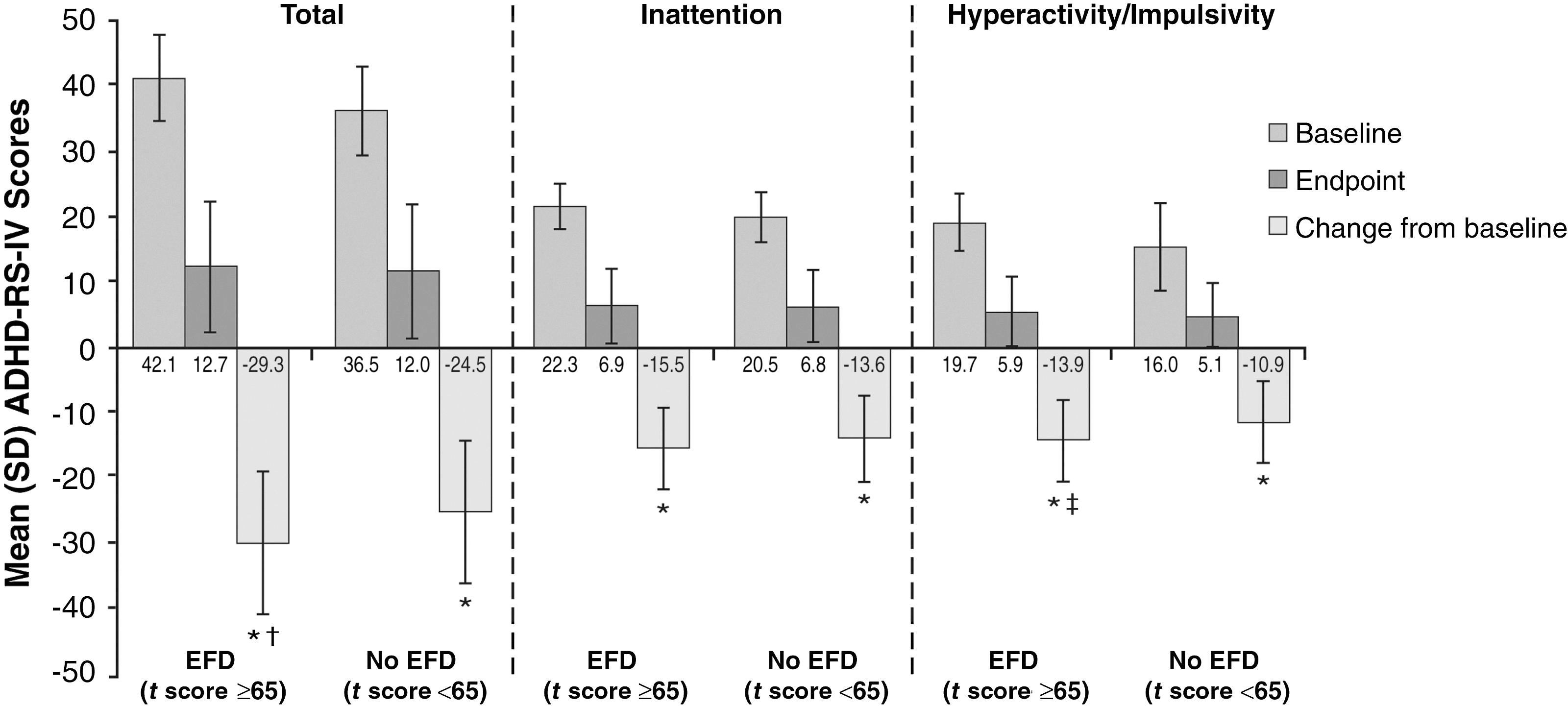
Attention-Deficit/Hyperactivity Disorder Rating Scale, IV (ADHD-RS-IV) total and subscale scores by baseline Behavior Rating Inventory of Executive Function (BRIEF) Gobal Executive Composite (GEC) t score category. Clinically significant executive function deficit (EFD), baseline GEC t score≥65; no EFD, baseline GEC t score<65; error bars indicate standard deviation. n=265 for baseline EFD subgroup; n=50 for baseline no EFD subgroup. *p<0.0001, baseline versus endpoint, within EFD and no EFD categories, based on paired t test; † p=0.004, and ‡ p=0.0022, change from baseline to endpoint, EFD versus no EFD, based on two-sample t test.
ADHD-RS-IV outcomes by endpoint BRIEF GEC category are illustrated in Figure 2. Baseline ADHD-RS-IV total scores were generally similar between participants with and without EFD at endpoint. Changes from baseline showed significant improvements in both endpoint categories, but those with EFD at endpoint showed significantly smaller improvements from baseline than did participants without EFD. A similar pattern of results was seen based on the ADHD-RS-IV subscales for inattention and hyperactivity/impulsivity.
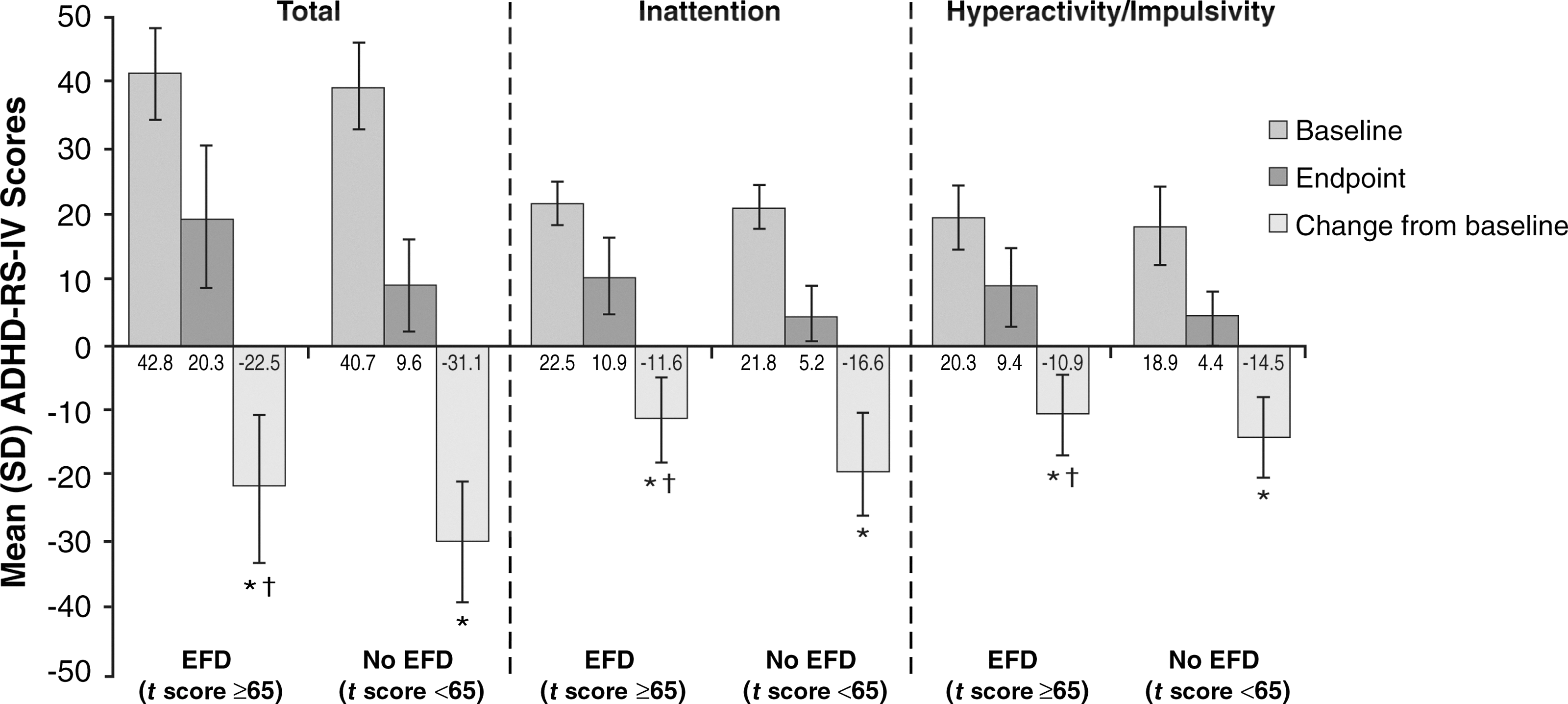
Attention-Deficit/Hyperactivity Disorder Rating Scale, IV (ADHD-RS-IV) total and subscale scores by endpoint Behavior Rating Inventory of Executive Function (BRIEF) Global Executive Composite (GEC) t score category. Clinically significant executive function deficit (EFD), baseline GEC t-score≥65; no EFD, baseline GEC t score<65; error bars indicate standard deviation. n=78 for the EFD subgroup; n=230 for the no EFD subgroup. *p<0.0001, baseline versus endpoint, within endpoint EFD and no EFD categories, based on paired t test; † p<0.0001, change from baseline to endpoint, endpoint EFD versus no EFD category, based on two-sample t test.
Treatment outcomes by clinician and parent global assessment
Table 1 summarizes CGI-Severity (S)/I and PGA scores, by baseline and endpoint BRIEF GEC category. The CGI-S indicates that clinicians rated those with EFD at baseline as more severely impaired than those without EFD. At endpoint, most participants in each group were rated as improved by parents and clinicians (Table 1).
Percentages based on number of observations (excluding those missing) for the relevant assessment.
BRIEF GEC, Behavior Rating Inventory of Executive Function, Global Executive Composite score; CGI-I, Clinical Global Impressions-Improvement; CGI-S, Clinical Global Impressions-Severity; EFD, executive function deficits; PGA, Parent Global Assessment; SD, standard deviation.
For those with and without EFD based on endpoint BRIEF GEC t-scores, baseline CGI-S mean scores were similar. When rated by parents and clinicians, most of those without EFD at endpoint were considered improved (90.0% and 95.0%, respectively). Parents and clinicians rated fewer participants with EFD at endpoint as improved (69.0% and 78.0%, respectively) (Table 1).
Relationship between BRIEF and ADHD-RS-IV scores
Baseline and endpoint change from baseline values for the BRIEF BRI, MI, GEC, and subscale scores generally demonstrated moderate, positive correlations with corresponding ADHD-RS-IV scores (Tables 2 and 3). BRIEF MI scores correlated relatively more strongly with the ADHD-RS-IV inattention subscale whereas BRI scores correlated more strongly with hyperactivity/impulsivity subscale scores. Similar correlations were observed based on raw endpoint scores (data not shown). Linear regression analysis (Table 4) showed that endpoint change from baseline BRIEF GEC scores was significantly related to change in ADHD-RS-IV total scores, and subscale scores for inattention and hyperactivity/impulsivity (all p<0.0001). This analysis found an r2 of 0.35 indicating that 35% of the change in BRIEF GEC t scores at endpoint could be accounted for by the change in ADHD-RS-IV scores at endpoint. Approximately 65% of the change in BRIEF GEC t scores is unrelated to ADHD-RS-IV scores, and represents variability in the change in EF behavior that may be related to other possible factors including error variance factors (e.g., measurement error, inter- or intra-rater differences), individual differences, or those that may be unique to the BRIEF and are not captured by assessment of DSM-IV-defined ADHD symptoms. Change in inattention subscale scores was somewhat more highly related to BRIEF GEC score improvements than change in hyperactivity/impulsivity subscale scores.
ADHD-RS-IV, Attention-Deficit/Hyperactivity Disorder Rating Scale IV; BRI, Behavioral Regulation Index; BRIEF, Behavior Rating Inventory of Executive Function; GEC, Global Executive Composite; MI, Metacognition Index.
ADHD-RS-IV, Attention-Deficit/Hyperactivity Disorder Rating Scale IV; BRI, Behavioral Regulation Index; BRIEF, Behavior Rating Inventory of Executive Function; GEC, Global Executive Composite; MI, Metacognition Index.
The subscales are highly correlated with the total score, hence the same r2 value of 0.35 was calculated for the subscale scores and the total score. However, when regressors are highly correlated, separating the effects of one from the other cannot be precisely accomplished; parameter estimates may be highly dependent on the particular regressors used in the model.
ADHD-RS-IV, Attention-Deficit/Hyperactivity Disorder Rating Scale Rating Scale, version IV; BRIEF GEC, Behavior Rating Inventory of Executive Function Global Executive Composite score; df, degrees of freedom.
Safety and tolerability
Detailed safety analysis has been previously published (Findling et al. 2009). A total of 269/318 (84.9%) participants experienced TEAEs; most (82.7%) experienced TEAEs that were mild or moderate in intensity. No deaths occurred. Two severe AEs (SAEs) were recorded; syncope in one participant and sinus arrest in one participant. Both participants had prior cardiovascular medical history relevant to these events; further details have been reported previously (Findling et al. 2009). A total of 12/318 (4.1%) participants discontinued the study because of TEAEs. TEAEs with incidence≥5% included decreased appetite (42.6%), weight decrease (16.4%), irritability (15.8%), insomnia (15.1%), initial insomnia (11.4%), upper abdominal pain (11.0%), headache (9.5%), and affect lability (7.3%).
Discussion
This post-hoc analysis of a 7-week open-label trial of LDX in children with ADHD demonstrated that impairment of EF behaviors, as assessed using the parent-reported BRIEF, is significantly, albeit moderately, related to ADHD symptom severity, based on the clinician-administered ADHD-RS-IV. At baseline, most participants in the current trial met criteria for EFDs, and these participants exhibited more severe ADHD symptoms (versus participants without EFDs at baseline) as assessed by the ADHD-RS-IV. At endpoint, most participants with no EFD exhibited less severe ADHD symptoms than did those with EFD. CGI and PGA ratings of ADHD severity at baseline and response to LDX treatment at endpoint were also consistent with BRIEF ratings of EF behaviors. BRIEF and ADHD-RS-IV scores throughout the trial were moderately, positively correlated; BRIEF MI scores correlated with inattention subscale scores; BRIEF BRI scores tended to correlate with hyperactivity/impulsivity subscale scores. Overall, endpoint change from baseline in BRIEF GEC scores was significantly related to change in ADHD-RS-IV total and subscale scores. LDX demonstrated a safety profile consistent with long-acting stimulant use.
The clinically significant baseline deficits and treatment-related improvements in EF behaviors observed currently are generally in line with previous trials that examined EF using either the BRIEF or BADDS in children (Qian et al. 2007; Brown and Landgraf 2010) and adults (Biederman et al. 2008; Spencer et al. 2008; Brown et al. 2011) with ADHD. At baseline, 84.1% evaluable participants in the present trial showed EFDs, whereas at endpoint this proportion had decreased to 25.3%. This is similar to the rate of EFDs described by Brown et al. (2010) in a trial of LDX in adults with ADHD, in which at baseline 91.5% of patients had suboptimal EF, based on BADDS (BADDS total scores ≥50); after 4 weeks of open-label treatment with LDX, the proportion with suboptimal EF scores decreased to 26.8%.
Other reports demonstrated that EF impairments identified using the BRIEF or BADDS improved with stimulant or nonstimulant ADHD pharmacotherapy. Qian et al. (2007) showed that, in children with ADHD, open-label, once-daily OROS methylphenidate led to a modest (∼8%), statistically significant improvement from baseline BRIEF GEC scores, in addition to improvements in MI and domain scores for working memory, initiation, monitoring, and inhibition. In contrast, Turgay et al. (2010) previously reported on the BRIEF GEC scores in this current investigation with LDX, showing mean BRIEF GEC scores improved by ∼24%, an improvement of ∼18 points from baseline GEC scores of 74.0 (i.e., EFD), to a mean GEC at endpoint of 56.1 (i.e., no EFD). Study design differences including the smaller number of participants (n=26) and an older age range (8–14 years) in the study by Qian and colleagues (2007) may have contributed to the differences in findings. Other trials in adults with ADHD treated with MAS, extended release (MAS XR) (Spencer et al. 2008) and the nonstimulant atomoxetine (Brown et al. 2011) have described similar, broad, and statistically significant improvements in EF behaviors, based on the BADDS. Improvement of EF behaviors as assessed with the BRIEF or BADDS, likely reflects an enhanced ability of the patient to manage complex daily tasks and social/personal functioning.
A recent report further suggests that behavioral EF rating scales such as the BRIEF are modestly congruent with more traditional neuropsychological EF tests, but are a relatively better predictor of ADHD symptoms and diagnostic status (Toplak et al. 2009) than are traditional EF tasks. In research settings, EF processes are typically measured using neuropsychological tests such as the Stroop color-word test; Wisconsin Card Sorting Test (Nigg et al. 2005; Biederman et al. 2006); digit span and verbal working memory tests; and stop-signal reaction time, continuous performance (Gau and Shang 2010), and trail-making tasks (Houghton et al. 1999). Based on these tests, ∼30–50% of children and adults with ADHD exhibit psychometrically defined EFDs (Nigg et al. 2005; Biederman et al. 2006), which persist over time, and are associated with poor long-term functional outcomes (Biederman et al. 2004, 2006, 2007b).
The usefulness and validity of traditional neuropsychological tests of EF, however, have been questioned (Brown 2006; Barkley and Fischer 2011). For research purposes, such tests are designed to assess a single EF process while controlling or eliminating the involvement of other processes. As such, this may not reflect the true nature of EF, which is dynamic and integrative; during daily activities, multiple EF processes are constantly at work simultaneously. To complete ordinary but complex tasks such as cooking a meal or doing homework, for example, individuals must plan, organize, and perform behaviors to accomplish their goal, while at the same time filtering out distracting stimuli and inhibiting inappropriate responses. Because psychometric tests measure individual neuropsychological processes in isolation and eliminate the potential for interference by competing EF demands, some have argued that these tests fail to capture many patients with real-world behavioral EF impairments, and, therefore, lack clinical utility (Brown 2006).
The current post-hoc analysis confirms and builds on these findings. In line with a previous report from Qian et al. (2007), moderate to strong positive and significant correlations were found between BRIEF GEC index and subscale scores and ADHD-RS-IV total and subscale scores, suggesting a clinically useful predictive relationship between these scales. Generalized linear analysis of variance showed that endpoint change in ADHD-RS-IV total score was significantly related to change in BRIEF GEC scores, accounting for ∼35% of endpoint GEC score variability. As was expected given this relationship, at endpoint, participants with EFDs at baseline (determined by BRIEF GEC scores) showed more improvement in ADHD-RS-IV scores than did those without EFDs at baseline.
The present findings highlight the value and potential importance of using a range of assessment strategies or tools in management of patients with ADHD. These can include obtaining parental ratings of EF behaviors, such as using the BRIEF, in addition to determining the presence and severity of core ADHD symptoms to develop a more complete perspective of treatment-related response that may not be assessed by a symptom scale alone. Paired with clinician ratings of the 18 DSM-defined symptoms of inattention and hyperactivity/impulsivity (as with the ADHD-RS-IV), parent ratings of EF provide a broader perspective on the patient's daily goal-directed behavior and emotional functioning (Gioia et al. 2000). To this point, participants in the current investigation were more likely to be rated as improved by the clinician than by the parents, which may reflect that parents are able to observe a greater range of behaviors in the home, which may be better captured by the BRIEF, than can be assessed by the clinician in the office using the ADHD-RS-IV. ADHD symptoms observable by the clinician, such as talkativeness and hyperactivity, are more circumscribed in scope than the range of behaviors recorded in the parent-rated BRIEF.
Limitations
The findings of the current post-hoc analysis should be considered in light of several investigational design and analytic limitations. The present open-label nature of treatment introduces the possibility of parent and clinician bias toward treatment-related improvement. The short-term, 7 week treatment period employed does not provide information about changes in EF or ADHD symptoms that may occur with longer-term treatment. Moreover, categorical analysis of EF impairment status (e.g., with or without EFDs) does not provide detailed information about behavioral changes in specific EF domains, although this has been described previously by Turgay et al. (2010). The present regression analysis is limited in scope, as discussed previously. It will be of interest to examine more fully the relationship between unique aspects of EF behavior captured using the BRIEF or other behavioral measures of EFD and ADHD symptoms, and how these relationships are impacted by pharmacotherapy in patients with ADHD.
Conclusion
Most participants in the current trial exhibited significant behavioral EF impairments at baseline, as assessed by the parent-rated BRIEF. Notably, significant behavioral EF impairments at baseline were associated with the presence of a greater amount of ADHD symptoms as suggested by the moderate level of positive correlation between BRIEF and ADHD-RS-IV scores. As described in a previous report (Findling et al. 2009), LDX significantly improved ADHD symptoms as assessed by the ADHD-RS-IV from baseline to endpoint (p<0.0001) and at each study visit versus baseline (p<0.0001) as well as improving EFD. However, neither measure alone may be sufficient to characterize symptomatic improvement or remission. Results suggest that at endpoint, most participants no longer met criteria for significant behavioral EF impairments. Endpoint ADHD-RS-IV change scores were significantly related to endpoint BRIEF GEC scores as indicated by the 35% shared variance, although the greater portion of the variance may be attributed to BRIEF GEC change being unrelated to improvements in core ADHD symptoms. These data may suggest that the BRIEF describes certain EF behavioral impairments that are not necessarily captured by the clinician-rated ADHD-RS-IV, but that are salient and manifest to parents.
Clinical Significance
When behavioral EF impairments are identified as a component of the patient's ADHD, clinicians should consider whether the treatment regimen is adequately addressing EF. Clinically, a combination of parent-rated (such as the BRIEF and PGA) and clinician-rated (ADHD-RS-IV and CGI-I) assessments of EF, ADHD symptoms, and global illness severity may provide an understanding of a broader phenotype of ADHD impairments, and serve as a more accurate indicator of response to treatment than can be obtained with symptom assessment alone. The safety profile of LDX in this study was consistent with that seen in other placebo-controlled LDX studies (Biederman et al. 2007a; Findling et al. 2008; Wigal et al. 2009), open-label LDX studies, and with other long-acting stimulant formulations in children with ADHD (Concerta [package insert] 2010; Adderall XR [package insert] 2011; Focalin XR [package insert] 2012).
Footnotes
Acknowledgments
Under the direction of the authors, Karen Dougherty, a former employee of SCI Scientific Communications & Information (SCI), and Michael Pucci, an employee, provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy editing, and fact checking was also provided by SCI. Joyce Zinsenheim, as a consultant to Shire Development LLC, reviewed and edited the manuscript for scientific accuracy. Shire Development LLC provided funding to SCI for support in writing and editing this manuscript. Although the sponsor was involved in the design, collection, analysis, interpretation, and fact checking of information, the content of this manuscript, the ultimate interpretation, and the decision to submit it for publication in the Journal of Child and Adolescent Psychopharmacology were made by the authors independently.
Disclosures
Dr. Robert L. Findling receives, or has received, research support, acted as a consultant, received royalties from, and/or served on a speaker's bureau for Abbott, Addrenex, Alexza, American Psychiatric Press, AstraZeneca, Biovail, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, Forest, GlaxoSmithKline, Guilford Press, Johns Hopkins University Press, Johnson & Johnson, KemPharm Lilly, Lundbeck, Merck, National Institutes of Health, Neuropharm, Novartis, Noven, Organon, Otsuka, Pfizer, Physicians' Post-Graduate Press, Rhodes Pharmaceuticals, Roche, Sage, Sanofi-Aventis, Schering-Plough, Seaside Therapeutics, Sepracor, Shionogi, Shire, Solvay, Stanley Medical Research Institute, Sunovion, Supernus Pharmaceuticals, Transcept Pharmaceuticals, Validus, WebMD, and Wyeth. Ben Adeyi is an employee of Shire and holds stock and/or stock options in Shire. Dr. Bryan Dirks is a Shire employee and holds stock and/or stock options in Johnson & Johnson and Shire. Dr. Thomas Babcock is a Shire employee and hold stock and/or stock options in Shire. Dr. Brian Scheckner is a Shire employee and holds stock and/or stock options in Shire. Dr. Robert Lasser was an employee of Shire with stocks and stock options from 2008 to July 2012; from July 2010 to the present he is an employee of Pharmanet/i3, an inVentiv Health company (no stock or options in Shire or any other company). Dr. Anthony DeLeon is a Shire employee and owns stock and/or stock options in Shire. Dr. Lawrence D. Ginsberg receives or has received research grant support from Alkermes, AstraZeneca, Bristol-Myers Squibb, Cephalon, Eli Lilly, McNeil, Novartis, Otsuka, Pamlab, Pfizer, Seaside Therapeutics, Shire, and Validus; served on a speaker's bureau for Angelini Labopharm, AstraZeneca, Bristol-Myers Squibb, Dey Pharma, Eli Lilly, Forest, GlaxoSmithKline, McNeil, Merck, Novartis, Noven, Pamlab, Pfizer, Shionogi, Shire, Sunovion, Validus, and Wyeth; and is a consultant for Angelini Labopharm, PGxHealth, Sepracor, and Shire.