
Abstract
Objective:
Atomoxetine is efficacious in reducing symptoms of attention- deficit/hyperactivity disorder (ADHD), but its effect on visual memory and attention needs more investigation. This study aimed to assess the effect of atomoxetine on visual memory, attention, and school function in boys with ADHD in Taiwan.
Method:
This was an open-label 12 week atomoxetine treatment trial among 30 drug-naíve boys with ADHD, aged 8–16 years. Before administration of atomoxetine, the participants were assessed using psychiatric interviews, the Wechsler Intelligence Scale for Children, 3rd edition (WISC-III), the school function of the Chinese version of the Social Adjustment Inventory for Children and Adolescents (SAICA), the Conners' Continuous Performance Test (CPT), and the tasks of the Cambridge Neuropsychological Test Automated Battery (CANTAB) involving visual memory and attention: Pattern Recognition Memory, Spatial Recognition Memory, and Reaction Time, which were reassessed at weeks 4 and 12.
Results:
Our results showed there was significant improvement in pattern recognition memory and spatial recognition memory as measured by the CANTAB tasks, sustained attention and response inhibition as measured by the CPT, and reaction time as measured by the CANTAB after treatment with atomoxetine for 4 weeks or 12 weeks. In addition, atomoxetine significantly enhanced school functioning in children with ADHD.
Conclusion:
Our findings suggested that atomoxetine was associated with significant improvement in visual memory, attention, and school functioning in boys with ADHD.
Introduction
Attention has also become the focus of current studies concerning the neuropsychological basis of ADHD (Seidman 2006). Attention refers to a collection of distinct cognitive processes, such as selective attention, vigilance, and distractibility (Navarra et al. 2008), and is mediated by distinctive brain areas, including the prefrontal cortex, anterior cingulate, and inferior frontal cortex as evidenced by imaging data (Valera et al. 2005; Banich et al. 2009). The Continuous Performance Test (CPT) provides a well-established method for objectively evaluating attention in ADHD (Eliason and Richman 1987). Children with ADHD typically have slow reaction time and high error rates on the CPT (Nichols and Waschbusch 2004) with moderate to large effect sizes to differentiate individuals with ADHD from those without (Frazier et al. 2004).
Evidence is emerging that improved neuropsychological functioning is associated with better functional outcomes for individuals with ADHD (Semrud-Clikeman et al. 2008), and neuropsychological deficits have been suggested as the independent targets for ADHD treatment (Faraone et al. 2005). Previous studies on experimental animals (Clayton and Williams 2000) and human volunteers (Moor et al. 2005) have converged to suggest a crucial role for norepinephrine in neuropsychological functions. Norepinephrine release is critical at the time of learning for arousal, for reinforcement, and then for triggering the consolidation of memory (Gibbs 2008). Animal studies have shown that norepinephrine efflux is selectively increased during a task measuring spatial memory (Rossetti and Carboni 2005), suggesting that norepinephrine may be involved in the active maintenance of visuospatial information. Activation of neuronal circuits related to norepinephrine release contributed to a significant enhancement of performance on visual memory in rats (Clayton and Williams 2000). Moor et al. have found that intravenous infusion of norepinephrine improved visual recognition memory in healthy participants (Moor et al. 2005). In addition to visual memory, the norepinephrine system has been implicated in brain-behavior models of attention (Coull et al. 2004; Nieuwenhuis et al. 2005). Depletion of cortical norepinephrine has been shown to lead to attentional deficits (Carli et al. 1983). These findings all point to a strong relationship between the neurotransmitter norepinephrine and cognitive functions, including visual memory and attention.
Atomoxetine, a highly selective norepinephrine reuptake inhibitor (SNRI), is a potent inhibitor of the presynaptic norepinephrine transporter (NET), with little affinity for other noradrenergic receptors or for other neurotransmitter transporters (Garnock-Jones and Keating 2009). Although previous studies have shown the efficacy of atomoxetine in reducing the clinical symptoms (Caballero and Nahata 2003; Gau et al. 2007b) and executive dysfunction (Faraone et al. 2005; Chamberlain et al. 2007; Gau and Shang 2010b) of ADHD, there is a relative dearth of empirical studies assessing its effects on visual memory and attention. Animal studies showed that atomoxetine decreased the errors in visual recognition memory (radial arm maze) (Tzavara et al. 2006) and the number of perseverative errors (visual discrimination test) (Seu et al. 2009), increased attentional performance (five-choice serial reaction time test) (Blondeau and Dellu-Hagedorn 2007; Navarra et al. 2008), and remediated attentional deficits (set-shifting test) (Newman et al. 2008).
Human studies have demonstrated that a single clinically relevant oral dose of atomoxetine was associated with improved inhibitory control (stop-signal reaction time) in healthy participants (Chamberlain et al. 2006) and adults with ADHD (Chamberlain et al. 2007), and decreased commission errors (visual CPT) in adults with ADHD (Chamberlain et al. 2007). By using a computer-based CPT (cb-CPT) with an infrared motion-tracking device, a recent placebo-controlled study demonstrated a positive effect of atomoxetine on executive function, inhibitory control, and hyperactivity compared with placebo in children with ADHD (Wehmeier et al. 2011). However, these findings were not supported by studies using auditory CPT (Spencer et al. 1998) and the Conners' CPT (Posey et al. 2006). Therefore, the effects of atomoxetine on improving attention as measured by the CPT were inconsistent. Furthermore, two human studies did not show improving visual memory with atomoxetine in adults using the Rey-Osterrieth Complex Figure (Spencer et al. 1998) and the Brief Visuospatial Memory Test (Kelly et al. 2009). Hence, an investigation of the effects of atomoxetine on visual memory and attention is warranted.
Children with ADHD showed significant impairments in school functioning including academic underachievement (Rapport et al. 1999), repeated grades, (Biederman et al. 1996), and negative peer relationships (Tseng et al. 2011), which have been recognized as one of key reasons for clinical referral (Loe and Feldman 2007; Gau et al. 2010) and therefore, as one of main outcome measures of ADHD treatment (Waxmonsky et al. 2010). Despite evidence of the efficacy of stimulants with regards to problems at school and with peers (Gau et al. 2006b), little is known about the effectiveness of atomoxetine in improving school functioning (Bakken et al. 2008).
In the present study, we assessed the long-term (12 weeks) effect of atomoxetine on visual memory, attention, and school function in 30 boys with ADHD. We used the Cambridge Neuropsychological Test Automated Battery (CANTAB) and the Conners' CPT with good psychometric properties as established in Western populations (Luciana and Nelson 1998; Luciana 2003) and in Taiwan (Gau et al. 2009; Gau and Shang 2010a). We hypothesized that atomoxetine treatment would lead to improvements across measures of visual memory, attention, and school function.
Method
Participants
We recruited consecutively 30 drug-naíve male patients ages 8–16 (mean±standard deviation [SD] 10.70±1.84) with a documented American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) diagnosis of ADHD from the Children's Mental Health Center of National Taiwan University Hospital, Taipei. The majority of their parents had college or higher educational levels (mothers, 50%; fathers, 60%) and were employed as technical personnel (mothers, 50%; fathers, 77%) followed by homemaker for the mothers (50%) and professional jobs for the fathers (23%).
The participants and their mothers were interviewed by using the Chinese version of the Kiddie Schedule for Affective Disorders and Schizophrenia for School- Aged Children—Epidemiological Version (K-SADS-E) (Gau and Soong 1999; Gau et al. 2005, 2007a). Dr. Gau made the best estimate of the diagnoses of ADHD and other psychiatric disorders based on clinical assessments and both K-SADS-E interviews. The best-estimate procedure has been described in detail elsewhere (Gau and Chiang 2009).
Participants were excluded if they had a serious medical illness, such as a cardiovascular disease; had a full-scale IQ score <80; had a history of bipolar disorders, psychosis, any substance abuse, or pervasive developmental disorder; had anxiety disorders based on the DSM-IV criteria at study entry; had a history of any seizure disorder or prior electroencephalogram abnormalities related to epilepsy; or if they had ever used any psychoactive medications before the study.
Of the 30 patients with ADHD, 15 (50.0%) had combined type, 13 (43.3%) had predominantly inattentive type, and 2 (6.7%) had predominantly hyperactive-impulsive type. The distribution of ADHD subtypes in the present study was consistent with previous clinical studies in patients with ADHD (Chiang et al. 2010), suggesting no significant sampling bias in our sample. Eleven patients also met diagnostic criteria for other disorders, including oppositional defiant disorder (n=11, 36.7%), conduct disorder (n=1, 3.3%), and past history of anxiety disorders (n=2, 6.7%). The average full-scale IQ was 105.37±13.55 (range, 80–135) (Table 1).
ADHD=attention-deficit/hyperactivity disorder.
Primary outcome measures
Two CANTAB tasks were used to assess visual memory abilities.
Pattern Recognition Memory (PRM)
The PRM is a test of visual recognition memory in a two-choice forced discrimination paradigm (Sahakian et al. 1988; Egerhazi et al. 2007). At the center of the screen, a series of geometric patterns was presented one after the other for a 3-second viewing interval. Following the presentation of the pattern series, the screen paused for 5 seconds, after which the participant was presented with two geometric patterns. One of the two designs was from the previously viewed list. The other was a completely novel stimulus. The two designs differed in shape but not in color. The participant was asked to touch the design that had been seen. After each trial, the participant was given feedback as to whether their choice was correct or incorrect. Twelve trials, one containing each of the 12 target stimuli, were implemented in each of the two blocks for a total of 24 trials. Accuracy and response latency were recorded. Two major indices were used: 1) the percentage of correct responses across both blocks for pattern recognition score; and 2) mean response latency for correct responses.
Spatial Recognition Memory (SRM)
The SRM tests visual spatial memory in a two-choice forced discrimination paradigm in order to measure recognition memory for spatial locations (Sahakian et al. 1988; Egerhazi et al. 2007). The participant saw empty boxes presented at different locations on the screen, and was asked to remember these places. The participant then saw five stimuli in succession at different screen locations for durations of 3 seconds each. Following a 5 second pause, the participants then saw two boxes, one of which was in a remembered location and the other was novel. The participant was asked to touch the box that was previously targeted. After each trial, the participant was given feedback as to whether their choice was correct or incorrect. A total of 20 trials were presented in four blocks of five trials each. Accuracy and response latency were recorded. Two major indices were used: 1) the percentage of correct target locations chosen across all four blocks for computing the participant's recognition score; and 2) mean response latency for correct responses.
Secondary outcome measures
The secondary outcome measures included school functioning and attention as measured by one CANTAB task and the CPT.
Reaction Time (RTI)
This task is designed to measure the participants' speed of response to a visual target, where the stimulus is either predictable (simple reaction time) or unpredictable (choice reaction time). This task is recognized as a simple single-choice and multiple-choice reaction time task. The task is divided into five stages, which require increasingly complex chains of responses. In each case, the participant must react as soon as a yellow dot appears. In some stages the dot may appear in one of five locations, and the participant must sometimes respond by using the press-pad, sometimes by touching the screen, and sometimes both. Four major indices were presented: 1) simple movement time: the time taken to touch the stimuli in trials in which they appeared in one location only; 2) five-choice movement time: the time taken to touch the stimuli in trials in which one of five possible different stimuli had been presented; 3) simple reaction time: the speed with which the participant responded to the onset of a stimulus in a single location; 4) five choice reaction time: the speed with which the participant responded to a stimulus in any one of five locations.
The Conners' CPT II
The Conners' CPT is a 14-minute, non-X type test presented visually for individuals ≥6 years of age. The participant is required to respond by pressing the space bar every time a letter (non-target) appears on the computer screen, except when the letter X (target) appears. The inter-stimulus intervals (ISIs) were 1, 2, and 4 seconds with a display time of 250 milliseconds. There were six blocks in the Conners' CPT II, with three sub-blocks, each containing 20-letter presentations. The ISIs varied across blocks.
Based on Egeland and Kovalik-Gran's factor analysis (Egeland and Kovalik-Gran 2010), the Conners' CPT II measures might be differentially grouped into the five indicators of focused attention, hyperactivity-impulsivity, sustained attention, vigilance, and change in control. Measures related to focused attention included variability, standard error of hit reaction time (Hit RT SE), perseverations, and omissions; measures related to hyperactivity-impulsivity included commissions, hit reaction time (Hit RT), and response style; measures related to sustained attention included hit reaction time changed by block (Hit RT Block Change) and its standard error, and changes in omission errors (i.e., more omission errors on the final third of the test); vigilance, the definition of which was mildly shifted from the attentional capacity to remain alert toward the impending stimulus information (Collings 2003) to the attentional capacity to maintain a constant speed in facing the challenge of longer ISI, and hence was considered different from sustained attention (Egeland et al. 2009), was captured by Hit RT ISI Change, and hit standard error changed by ISI (Hit SE ISI Change) (i.e., slower and more variable reaction time to longer ISI changes) (Egeland and Kovalik-Gran 2010).
The Chinese Social Adjustment Inventory for Children and Adolescents (SAICA)
The participant's school functioning was assessed through maternal reports on the Chinese-language SAICA. The SAICA, a 77-item semi-structured interview scale, was designed for administration to the parents of children and adolescents ages 6–18 to assess the four domains of their children's functioning: school, spare time, peer relations, and home behaviors (John et al. 1987). The Chinese SAICA has been proved to be a reliable instrument in clinical (Gau 2007) and treatment (Gau et al. 2006a,b) studies in Taiwan. Items are rated on a four-point Likert scale, from 1 to 4. We used the school function domain: 1) academic grades of English, Math, Chinese, Natural Science, and Social Science: 1 for above average, 2 for average, 3 for below average, 4 for failing; 2) attitude toward school work (1 item); 3) school interactions (3 items) including attitude toward teachers, teachers' attitude toward the child, and relationships with other students: 1 for positive, 2 for more positive than negative, 3 for more negative than positive, 4 for negative; and 4) school behavioral problems (11 items): 1 for not a problem, 2 for mild problem, 3 for moderate problem, and 4 for severe problem. The details of the behavioral items of the school behavioral problems are described elsewhere (John et al. 1987). A higher mean score indicates either poorer school function or a more severe school problem.
Procedures
The Research Ethics Committee of National Taiwan University Hospital approved this study prior to the administration of any study procedure or dispensing of the study drug, and monitored this study at all stages, from inception to completion, in accordance with current good clinical practice in Taiwan. The procedures and purpose of this study, as well as a reassurance of confidentiality, were clearly explained to the participants and their parents. Written informed assent was obtained from the participants and consent from their parents.
At baseline (visit 1), the participants were assessed by the CANTAB, CPT, and SAICA, and reassessed on week 4 (visit 2) and week 12 (visit 3) after treatment with atomoxetine. The initial once-daily dose of atomoxetine was 0.5 mg/kg lasting for 7 days, followed by an increase in the dose of atomoxetine to 1.2 mg/kg on day 8 without further changes in doses throughout the study period and to the end point.
Statistical analyses
SAS version 9.2 (SAS Institute Inc., USA) was used to conduct data analysis. The α value was preselected at the level of p<0.05. Using a sample of 180 typically developing children, grades 3–10 (ages 8–16 years; mean±SD, 12.42±1.62 years), without a lifetime DSM-IV diagnosis of ADHD based on the Chinese K-SADS-E as the norm for the CANTAB and CPT assessments, we transformed the raw score of each parameter to its adjusted z score by taking the age and sex of the normative sample into consideration. Sex-adjustment was made to account for the sex difference between the samples. The data of the CANTAB and CPT were expressed by mean±SD of the raw scores and age- and sex-adjusted z scores.
Because of repeated measures for the same subject, we used a linear multilevel model to test the mean differences in the repeated measures of the CANTAB, CPT, and Chinese SAICA at week 4 and week 12, compared with baseline (week 0). Cohen's d was used to compute the effect size (standardized difference between the two means) for the comparisons among the three assessments (baseline, week 4, week 12) with small, medium, and large effect sizes as Cohen's d ≥0.2 to <0.5, ≥0.5 to <0.8, and ≥0.8, respectively.
Results
Visual memory
Table 2 summarizes the comparisons of raw scores and adjusted z-scores, mean adjusted z-score differences (95% CI), and the effect sizes (Cohen's d) of the two CANTAB visual memory tasks across the three visits. For the PRM task, the mean latency of correct responses decreased (Cohen's d, −0.50) and total correct responses increased (Cohen's d, 0.53) significantly at week 4 from baseline. The mean latency of correct responses also significantly decreased at week 12 from baseline (Cohen's d, −0.50). The mean latency of correct responses of the SRM task significantly decreased at week 12 from baseline (Cohen's d, −0.42), but there was no significant change in correct responses (Fig. 1).
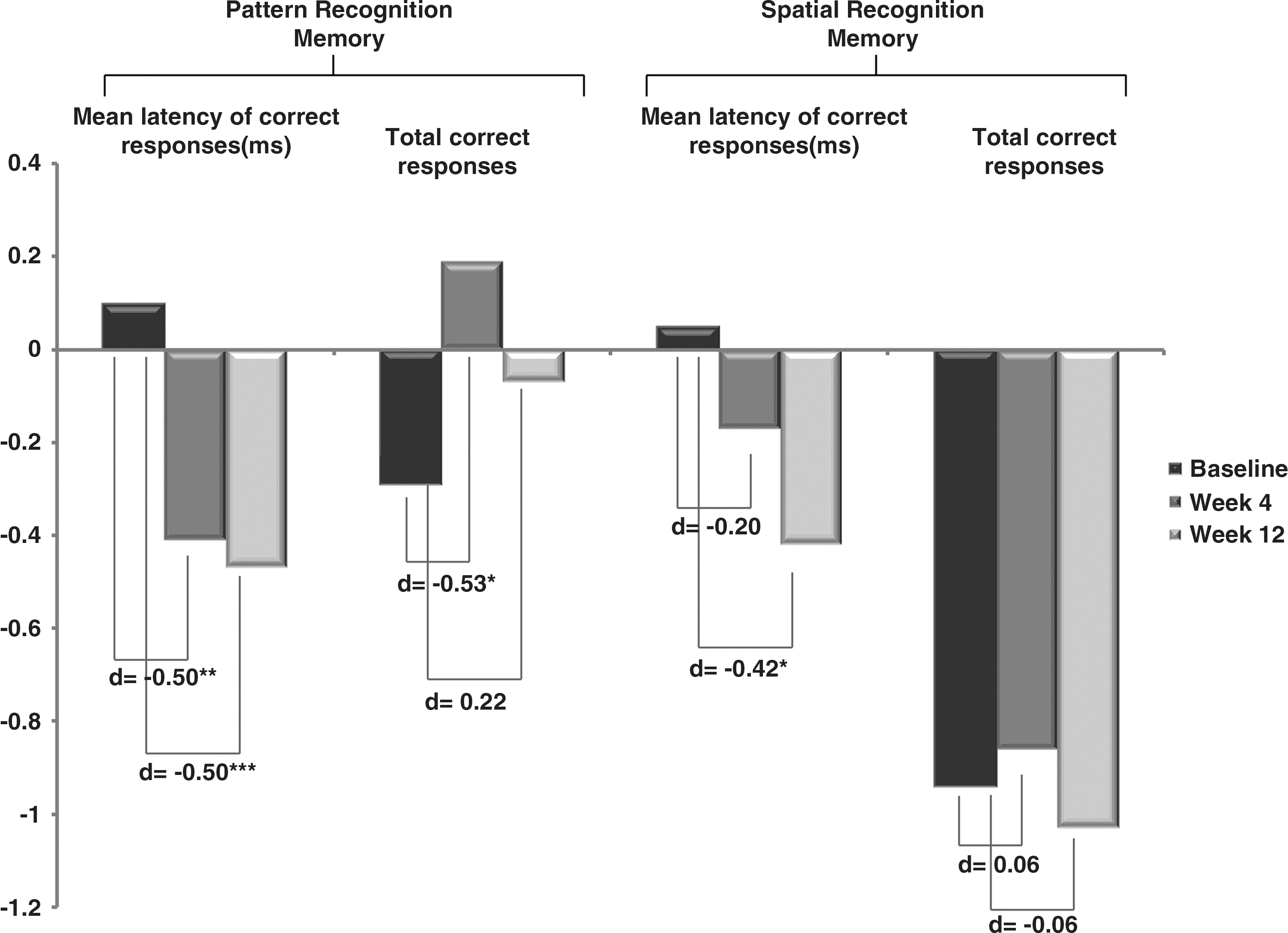
Comparisons of performance in pattern recognition memory and spatial recognition memory across baseline, week 4, and week 12. *p<0.05; ** p<0.01; *** p<0.001. d=Cohen's d.
p<0.05.
p<0.01.
p<0.001.
SD=standard deviation; β=estimate of mean difference of z score; CI=confidence interval; d=Cohen’s d.
Attention
Table 3 presents the comparisons of raw scores and adjusted z-scores of the CPT and RTI across the three visits. As for the CPT, the omission errors, commission errors, and Hit SE ISI Change significantly decreased at week 4 and week 12 from baseline, with small-to-medium effect sizes (absolute Cohen's d ranging from 0.40 to 0.78). The hit reaction time standard errors, variability, detectability (d’), and Hit RT ISI Change significantly decreased at week 4 from baseline, with small-to-medium effect sizes (absolute Cohen's d ranging from 0.38 to 0.51). As for the RTI, the five -choice movement time significantly increased at week 4 from baseline, with small effect size (Cohen's d, 0.37; Fig. 2).

Comparisons of performance on Continuous Performance Test and reaction time across baseline, week 4, and week 12. *p<0.05; ** p<0.01. d=Cohen's d.
p<.05.
p<.01.
SD=standard deviation; β=estimate of mean difference of z score; CI=confidence interval; d, Cohen’s d; RT=reaction time; SE=standard error; ISI=inter-stimulus interval.
School functioning
Table 4 lists the comparisons of mean scores and effect sizes (Cohen's d) of the school functioning subscale of the SAICA across the three visits (baseline, week 4, week 12). The scores of overall school functioning, grades, school interaction, and school behavioral problems significantly decreased at weeks 4 and 12 from baseline, with small-to-large effect sizes (Cohen's d, −0.43 to −0.98). The attitude toward school work score significantly decreased at week 4 from baseline, with medium effect size (Cohen's d, −0.58; Fig. 3).
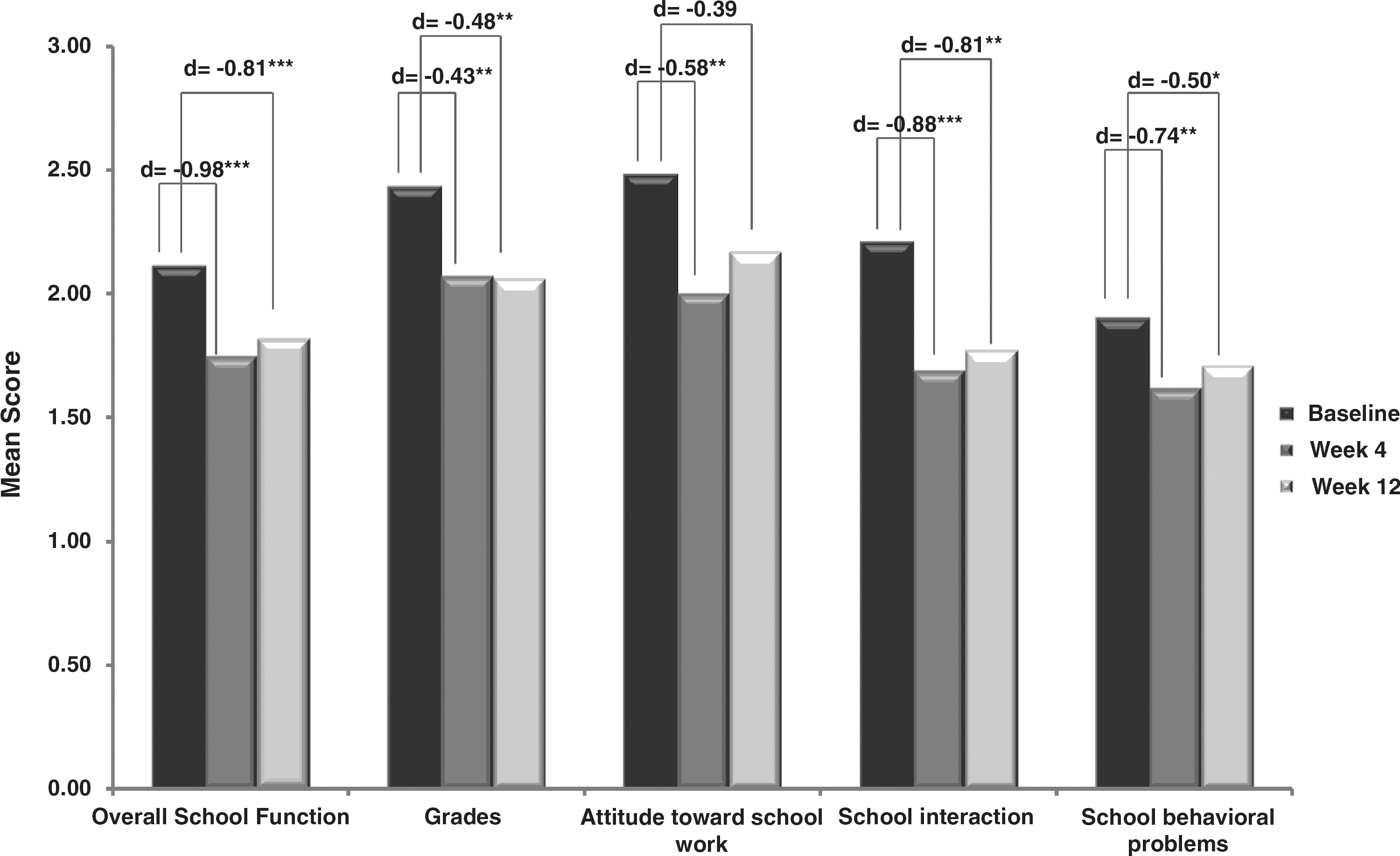
Comparisons of school function across baseline, week 4, and week 12. *p<0.05; ** p<0.01; *** p<0.001. d=Cohen's d.
SD=standard deviation; β=estimate of mean difference of z score; CI=confidence interval; d=Cohen's d.
Discussion
The present study examined the effects of atomoxetine on cognitive performance in children with ADHD, particularly on visual memory and attention tasks, and to assess its effect on school performance. We found that compared with baseline, atomoxetine was associated with a specific pattern of cognitive enhancement in discrete aspects of visual memory and attention in boys with ADHD, including pattern recognition memory (PRM), sustained attention (CPT), hyperactivity-impulsivity (CPT), vigilance (CPT), and psychomotor speed (RTI) noted at week 4; and pattern recognition memory (PRM), spatial recognition memory (SRM), and some measures of sustained attention (CPT), hyperactivity-impulsivity (CPT), and vigilance (CPT) noted at week 12. Our findings also lent evidence to support that atomoxetine was associated with improvement in several aspects of school functioning, that is, academic grades, attitude toward school work, interactions with peers and teachers, and behavioral problems at school. Taken together, our findings suggest that atomoxetine was associated with enhanced performance in several aspects of visual memory, attention, and school functioning.
The present study found that atomoxetine was associated with different response latencies in several tasks. Atomoxetine was associated with shortened latencies for correct responses on the PRM (week 4, week 12), and SRM (week 12) tasks, and with lengthened movement time on the five-choice condition of the RTI tasks (week 4), implying that the association between atomoxetine and response latencies cannot be explained simply by the psychomotor effect. Animal studies have also found that atomoxetine was associated with decreased stop-signal reaction time and with increased go reaction time (Bari et al. 2009).
Unlike the negative findings in adults with ADHD (Spencer et al. 1998), the present study demonstrated the association of atomoxetine with some visual memory functions measured by the PRM and SRM tasks. This disparity may be related to differences in the mean age of participants and the paradigms deployed. The sample in this present study (8–16 years old) was much younger than that reported by Spencer et al. (19–60 years old) (Spencer et al. 1998). We used two CANTAB visual memory tasks whereas Spencer et al. used one (Rey-Osterrieth Complex Figure).
The neuropsychological profile suggests that atomoxetine may be functionally distinct from conventional psychostimulants, with different effects on the visual memory. The significant association of atomoxetine with the mean latency for correct responses on the PRM task found in the current study was not seen with methylphenidate (Rhodes et al. 2004). Our findings support the evidence from an animal study that at doses relevant to those that increased cortical norepinephrine release, atomoxetine improved pattern recognition in rats (Tzavara et al. 2006). Additionally, in contrast to no improvements on the SRM task with stimulant treatment (Kempton et al. 1999; Rhodes et al. 2006), our findings showed that atomoxetine was associated with enhanced performance on this task in terms of speeding up correct responses. Our finding further supports norepinephrine's playing an important role in regulating the spatial recognition memory (Zhang et al. 2008). Taken together, improvement in the latency for correct responses on the PRM and SRM tasks with atomoxetine suggests a more important role for norepinephrine than for dopamine in the cognitive processes required for optimal performance on these visual memory tasks.
Our results showed improvement in the CPT measures among children with ADHD who were treated with atomoxetine, as evidenced by decreased omission errors (week 4, week 12), commission errors (week 4, week 12), Hit RT SE (week 4), variability (week 4), Hit RT ISI Change (week 4), and Hit SE ISI Change (week 4, week 12), and increased detectability (week 4). Therefore, scores indexing focused attention (omission errors, Hit RT SE, variability), hyperactivity-impulsivity (commission errors), and vigilance (Hit RT ISI Change, Hit SE ISI Change) evidenced significant treatment effects, and these findings were consistent with the norepinephrine hypothesis on the regulation of attention (Coull et al. 2004; De Martino et al. 2008), impulsivity (Pattij and Vanderschuren 2008), and vigilance (Sirvio and MacDonald 1999). Our results lend strong evidence to support the findings from animal studies (Blondeau and Dellu-Hagedorn 2007; Navarra et al. 2008) and human studies (Chamberlain et al. 2007) that atomoxetine may be an effective treatment for impairments in attention, hyperactivity-impulsivity, and vigilance in ADHD.
In contrast, Spencer et al. reported that atomoxetine treatment was not associated with improvement on the CPT (Spencer et al. 1998). This disparity may again be attributable to differences in the paradigms deployed (visual task vs. auditory task) (Spencer et al. 1998). Interpretation of CPT performance may be a function not only of medication, but also of variations in the task that increase or decrease the sensitivity of the CPT to the changes in attention (Riccio et al. 2001). Our findings support the sensitivity of the visual CPT to atomoxetine effects in children with ADHD (Chamberlain et al. 2007).
In addition to evaluating the effects of atomoxetine on the neuropsychological deficits related to ADHD, we also examined the effects on school functioning. Consistent with previous studies, our findings showed that atomoxetine treatment was associated with improved school functioning across a variety of domains, including grades (Bakken et al. 2008), school interaction (Waxmonsky et al. 2010), and school behavioral problems (Waxmonsky et al. 2010). These domains of school function have been relatively less assessed in clinical trials of atomoxetine than have the core symptoms of ADHD. Taken together, these results parallel those found in clinical trials of stimulants (Gau et al. 2006b), and support the association of atomoxetine with improvement in school functioning. Because parental reports of their children's functional impairment have a significant relationship to use of special education interventions (Sawyer et al. 2004), enhancing children's school functioning may decrease the need of special education referrals.
Methodological considerations
The strengths of the present study included being the first to examine the effect of atomoxetine on visual memory functions in boys with ADHD with a relatively longer follow-up period; clinical and standardized psychiatric assessments based on child and mother interviews to confirm psychiatric diagnosis; and comprehensive assessments of visual memory and attention using standardized and well-validated neuropsychological tests with a well-established group of typically developing children to transform the raw scores to age- and sex-adjusted z scores (Luciana 2003; Gau and Shang 2010b).
Limitations
Several limitations of this study need to be taken into consideration. First, the major limitation of our present study was the lack of a placebo-controlled trial design, implying that the changes in performance across the three repeated assessments might not be solely attributable to the effect of atomoxetine, but also might be caused by possible learning effects from repeated neuropsychological assessments (Lowe and Rabbitt 1998). Hence, we need to interpret the findings with caution. Several scores appeared to trend toward baseline at week 12. The majority of our 30 boy subjects complained about performing the neuropsychological tests repeatedly because they knew that it would take long. Their lack of motivation may actually have influenced their performance at week 12. Previous studies have shown that motivational incentives were associated with better performance and greater cognitive control in the CPT (Locke and Braver 2008). In addition, other factors may also account for the trends toward baseline at week 12, such as loss of medication effect or loss of learning effect over time. Future studies are needed to explore the factors associated with the trends toward baseline at week 12. Second, although the parent-rated SAICA has been used as a reliable instrument to measure the school and social functioning in our previous clinical (Gau et al. 2006a; Gau 2007b; Lin et al. 2012) and community studies (Tseng et al. 2011; Kawabata et al. 2012) and an open-label drug trial (Gau et al. 2006b), lack of a double-blind design decreased the persuasiveness of this present study because of the potential report bias by the unblinded parents. Third, whereas several studies did not report gender difference in response to atomoxetine in patients with ADHD (Wehmeier et al. 2012), others did find a differential response to atomoxetine by gender (Cheng et al. 2007; Robison et al. 2008). Because the sample in this present study consisted of male subjects only, our findings might not be extended to female patients with ADHD. Fourth, the small sample size decreased the power to detect the difference, and limited our ability to examine the association of atomoxetine with improvement in visual memory and attention as a function of ADHD subtypes or comorbid patterns.
Conclusion
Combining our prior (Gau and Shang 2010b) and current findings in child populations, there is evidence to support the association of atomoxetine with reducing ADHD core symptoms and improving executive functions, as demonstrated in our prior study (Gau and Shang 2010b), and with improving visual memory, attention, inhibition control, and school functioning as demonstrated in the current study. Our findings also support that the CANTAB used in this study is sensitive and specific enough for measuring change in terms of the effect of atomoxetine on improving visual memory. Future studies on factors associated with treatment response are needed to use neurocognitive endophenotypes to reduce the clinical heterogeneity, by identifying homogeneous subgroups of ADHD patients.
Clinical Significance
In summary, this study demonstrated the association of atomoxetine with pattern recognition memory and spatial recognition memory as measured by the CANTAB tasks, sustained attention and response inhibition as measured by the CPT, and reaction time as measured by the CANTAB in children and adolescents with ADHD. In addition, atomoxetine was associated with enhanced school functioning as measured by the SAICA.
Footnotes
Acknowledgment
The authors thank Ming-Fang Chen, M.S., for assistance in data analysis.
Disclosures
This study was supported by grants from the National Health Research Institute (NHRI-EX97-9407PC; NHRI-EX98-9407PC), Taiwan, and an investigator-initiated study sponsored by Eli Lilly & Co. Taiwan (B4Z-TW-0021), which provided the study drug (atomoxetine) at no cost. The study was conducted and data were analyzed by Susan Shur-Fen Gau (S.S.G). This article was drafted by Chi-Yung Shang (C.Y.S) and critically revised by S.S.G. C.Y.S. and S.S.G. have conducted clinical trials on behalf of and were on the speakers' bureau for Janssen-Cilag and Eli Lilly & Co., Taiwan.