The 51st Annual National Institute of Mental Health (NIMH) New Clinical Drug Evaluation Unit (NCDEU) Meeting,Boca Raton,Florida,June 13–16,2011 Posters Most Relevant to Child and Adolescent Psychopharmacology
Available accessAbstractFirst published online December, 2011
The 51st Annual National Institute of Mental Health (NIMH) New Clinical Drug Evaluation Unit (NCDEU) Meeting,Boca Raton,Florida,June 13–16,2011 Posters Most Relevant to Child and Adolescent Psychopharmacology
SilvaRaul R.MD1MarkowitzJohn S.PharmD2MunizRafaelMD3WangChaoPhD3YoonMijaPharmD3WarginWilliamPhD4CavanaughPaul F.PhD3
Academic Behavioral Center, New York, NY
University of Florida College of Pharmacy, Galnesville, FL
Shionogi Inc, Florham Park, NJ
PK-PM Associates, LLC, Chapel Hill, NC
Pharmacokinetic Profile of Clonidine Hydrochloride Extended-Release Tablets in Children and Adolescents with Attention-Deficit Hyperactivity Disorder
Objective: To characterize the oral clearance of clonidine after twice-daily treatment with the extended-release tablet formulation of clonidine (CLON-XR) in pediatric patients with attention-deficit/hyperactivity disorder (ADHD).
Methods: Patients aged 6 to 17 years diagnosed with hyperactive or inattentive/hyperactive ADHD received CLON-XR alone (CLON-XR 0.2 or 0.4 mg/d as a fixed dose) or in combination (CLON-XR 0.1–0.4 mg/d with flexible dosing) with methylphenidate (MPH) or amphetamine (AMP) for 8 weeks. Pharmacokinetic analysis to assess clonidine concentrations and oral clearance was conducted on trough plasma samples obtained ∼12 hours after the previous dose on day 28 of the 56-day study or at early discontinuation (N=188).
Results: Steady-state trough concentrations of clonidine increased proportionally with CLON-XR dose. Median clearance was 0.376 L/h/kg (range, 0.140–1.855 L/h/kg) and was similar in the monotherapy (0.381 L/h/kg) and combination-therapy (0.366 L/h/kg) trials. Overall, clonidine clearance was unaltered by dose, although clearance was 30% greater in children (0.376 L/h/kg) than in adults with hypertension (0.266 L/h/kg; range, 0.147–0.584 L/h/kg). Median clonidine concentration was similar in the monotherapy (569 pg/mL in the 0.2-mg/d and 1225 pg/mL in the 0.4-mg/d groups, respectively) and combination-therapy groups (211-1411 pg/mL; range, 211-4000 pg/mL, depending on CLON-XR dose); however, lower concentrations were observed with MPH (999 pg/mL; range, 245-2520 pg/mL) than with AMP (1240 pg/mL; range, 211-4000 pg/mL).
Conclusions: Clearance of CLON-XR was greater in children than in adults with hypertension; further analysis of age effects on CLON-XR are warranted. There was no evidence of significant alterations in clearance processes when CLON-XR was used in combination with either stimulant, suggesting that adjustment of stimulant dose may not affect clonidine concentration.
Source of Funding: This study was supported by Addrenex Pharmaceuticals, Inc, a Shionogi company.
Learning Objectives:
• To understand the impact of patient age on clonidine clearance after administration of CLON-XR
• To understand the association between dose adjustment of CLON-XR and oral clearance of clonidine when used with stimulants
Literature References:
• Sallee FR. The role of alpha2-adrenergic agonists in attention-deficit/hyperactivity disorder. Postgrad Med. 2010;122:78–87.
• Jain R et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50:171–179.
• Connor DF et al. A pilot study of methylphenidate, clonidine, or the combination in ADHD comorbid with aggressive oppositional defiant or conduct disorder. Clinical Pediatrics 2000;39:15–25.
DanielyanArmanMD1WelgeJeffrey A.PhD2ShearPaula K.PhD2AdlerCaleb M.MD2ChangKiki D.MD3DelBelloMelissa P.MD, MS2
Cincinnati Children's Hospital Medical Center, Cincinnati, OH
University of Cincinnati, Cincinnati, OH
Stanford University, Stanford, CA
Executive Functioning of Adolescents with Depression Associated with Bipolar Disorder
Background: Bipolar disorder (BPD) is a chronic and recurrent condition, affecting family, social and educational functioning of children and adolescents. Deficits in executive functioning, which may include problems with attention, problem solving, conceptualization, organization, planning, and memory, may underlie the wide range of impairment observed in bipolar youth. Previous studies have observed poor executive functioning in manic but not euthymic youth with BPD (1). However, to our knowledge executive functioning in depressed bipolar youth has not been previously assessed.
Methods: Thirty-two adolescents (ages 12–18 years) with depression associated with BPD type I were assessed using the Behavior Rating Inventory of Executive Function (BRIEF) (2). All patients were medication-free at the time of assessment. The BRIEF is a standardized questionnaire used for assessment of children's performance on everyday tasks at home and school and is a measure of their executive functioning skills (3). The BRIEF consists of two indices and eight subscales. The “inhibit,” “shift,” and “emotional control” subscales comprise the Behavioral Regulation Index (BRI). The “initiation,” “working memory,” “planning,” “organization of materials” and “monitoring” subscales comprise the Metacognition Index (MI). The two indices comprise a Global Executive Composite (GEC) score. The BRIEF normative sample has the mean T-score of 50 with a standard deviation of 10. Scores of 65 or greater are considered to be of potential clinical significance.
Results: Adolescents with bipolar depression exhibit clinically significant impairment in executive functioning as evidenced by the GEC score (T=68.7, p<0.0001). Both the MI (T=64.4, p<0.0001), a summary measure of initiation and self monitoring, and the BRI (T=68.3, p<0.0001), a summary measure of cognitive set shifting and inhibitory control were significantly elevated. On the level of individual subscales there were clinically significant (T>65) impairments in the inhibition, shift, initiation, memory and planning subscales, but not in emotional control, organization or monitoring subscales.
Conclusions: Adolescents with bipolar depression exhibited significant impairments in the majority of areas of executive functioning, including the ability to shift cognitive set and to modulate emotions and behavior via inhibitory control (BRI), and the ability to initiate, plan, organize and sustain future-oriented problems solving in working memory (MI). Further studies should focus on whether improvement in the symptoms of bipolar depression as a result of psychopharmacological and/or psychosocial interventions will be associated with improvement of executive functioning, or whether the executive dysfunction persists during periods of euthymia.
Source of Funding: APIRE Janssen Resident Psychiatric Research Scholars.
Literature References:
• Shear PK, DelBello MP, Lee Rosenberg H, Strakowski SM: Parental reports of executive dysfunction in adolescents with bipolar disorder. Child Neuropsychol. 2002 Dec:8(4):285–95.
• DelBello MP, Chang K, Welge JA, Adler CM, Rana M, Howe M, Bryan H, Vogel D, Sampang S, Delgado SV, Sorter M, Strakowski SM: A double-blind, placebo-controlled pilot study of quetiapine for depressed adolescents with bipolar disorder. Bipolar Disord 2009:11:483–493.
• Gioia GA, Isquith PK, Guy SC, Kenworthy L: Behavior Rating Inventory of Executive Function (BRIEF): Professional Manual. Lutz (Florida): Psychological Assessment Resources, Inc., 2000.
SinghManpreet K.MDKelleyRyan G.BASandersErica M.AcquayeTenahBSLiSherrieBAHoweMeghan E.MSWReissAllan L.MDChangKiki D.MDStanford University School of Medicine, Stanford, CA
Resting State Functional Connectivity in Adolescents with Bipolar I Disorder
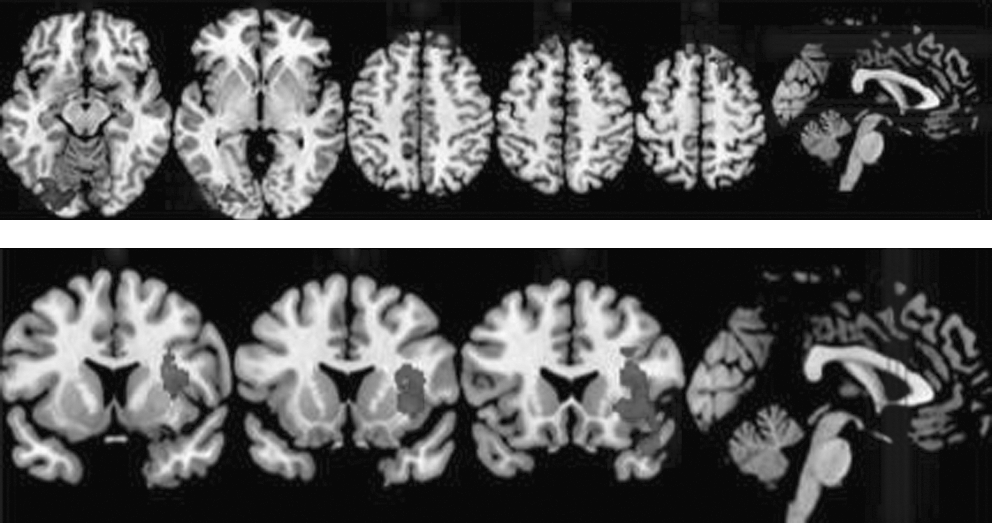
Background: Neuroimaging studies of children and adolescents with bipolar disorder (BD) have demonstrated dysfunction in frontotemporal regions involved in emotion regulation (Dickstein et al, 2010). The goal of this study was to examine resting state functional connectivity in adolescents with BD I compared to healthy controls to identify illness specific spontaneous resting state functional connectivity (RSFC).
Methods: Adolescents (13–18 years old) who were diagnosed with BD I (N=12) and adolescents without any personal or family history of a DSM-IV Axis I disorder (N=18) were examined for group differences in resting state functional connectivity after collection of images using a 3T GE scanner. Functional connectivity analysis was performed using the Functional Connectivity Toolbox (www.nitrc.org/projects/conn). These data were band-pass filtered (0.005–0.10 Hz), corrected for physiological noise and motion using a CompCor strategy (Behzadi et al., 2007). Regions of interest (RQIs) were defined as 10mm spheres of medial prefrontal cortex, posterior cingulated cortex and left and right lateral parietal cortices where the centers were derived and implemented in the toolbox. Bilateral amygdale ROIs were derived from the Automated Anatomical Labeling Atlas. ROI-to-whole-brain analyses were performed with statistical thresholds of p=0.01 for voxel height and p=0.01 Family-wise Error (FWE) corrected for cluster extent.
Results: Relative to controls, adolescents with BD showed increased network connections between the left amygdala and prefrontal and visual cortices (p=0.01 uncorrected signal and p=0.01 FWE extent), and decreased network connections between the left lateral parietal cortex and left insula, inferior frontal gyrus, and superior temporal gyrus (p=0.01 uncorrected signal and p=0.01 FEW extent) (see Figure). Healthy controls showed network connectivity resembling the default mode network (p=0.01 FDR signal and p=0.01 FEW extent). Correlational analyses within the BD group suggest that lithium exposed (N=5) versus unexposed (N=7) individuals appear to have increased RSFC between the medial prefrontal cortex and bilateral insula (p=0.01 uncorrected signal and p=0.01 FWE extent).
Discussion: Altered frontotemporal resting state functional connectivity was demonstrated in adolescents early in the onset of BD I, BD suggesting aberrant neural circuitry that may contribute to the pathophysiology of BD. Lifetime exposure to lithium appears to be associated with increased insula connectivity to the default mode network in bipolar youth. Studies with larger samples are needed to determine the effects of mood symptom ratings, age, gender, and development. In addition, longitudinal analyses examining the consequences of altered resting state functional connectivity in adolescents with BD-I on long-term clinical outcome are warranted.
Source of Funding: American Psychiatric Association Young Minds in Psychiatry Award.
Literature References:
• Behzadi Y, et al. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage;37:90–101.
• Dickstein DP, et al. Fronto-temporal spontaneous resting state functional connectivity in pediatric bipolar disorder. Biol Psychiatry;68:839–46.
MaloneRichard PatrickMD1VermaBeetaMD1GhaffariManelyMD1WestSusan H.PhD1CaterJacquelinePhD2
Drexel University College of Medicine, Philadelphia, PA
Biomedical Statistical Consulting, Wynnewood, PA
Lithium for the Reduction of Aggression in Conduct Disordered Outpatients
Background: Controlled trials of lithium conducted in inpatient settings have shown it to be safe and effective for reducing aggression in youth diagnosed with conduct disorder (CD; Malone et al, 2000). However, outpatient studies of lithium for reducing aggression have been negative. The aim of this study was to investigate lithium as a treatment for reducing aggression in youth diagnosed with CD in an outpatient setting.
Methods: The study used an 8-week double-blind placebo-controlled parallel groups design. There was a 2-week placebo baseline, followed by randomization of subjects who met an aggression criterion to 6 weeks of lithium or placebo. Twice as many subjects were randomized to lithium as to placebo. The setting was an outpatient specialty clinic. In all, 59 subjects enrolled into the study, including 46 males and 13 females, aged 9 to 17.9 years (mean=12.4±2.0 years). All met DSM-IV criteria for CD and had a profile of severe aggression. Of the 59, twenty-nine were randomized to treatments (20 to lithium and 9 to placebo). Lithium dosages ranged from 300 mg to 1800 mg/d. The primary efficacy measures included the Overt Aggression Scale-Modified for Outpatients (OAS-M; Coccaro et al. 1991) and the Clinical Global Impressions (CGI). Treatment responders were defined as subjects who had a 50% reduction in the total OAS-M score and a rating on the CGI of much improved or very much improved. A number of secondary outcomes were also assessed.
Results: Using last observation carried forward, there was not a statistically significant difference in responders between the lithium and placebo groups (33.3% v 22.2%, p=0.7). Likewise, there was not a difference between groups on the total OAS-M score (F[1,135]=0.14, p=0.7), any of the OAS-M sub-scores, or the CGI-Improvement item (40% vs. 22%, p=0.7). Side effects included nausea, vomiting, urinary frequency and first degree heart block.
Conclusions: Lithium was not effective for reducing aggression in this outpatient study. Possible reasons for a lack of response, including poor adherence will be discussed.
Source of Funding: NIMH R29 MH57093 (Pl, Malone). Drug and matching placebo were provided by Roxane Laboratories, Inc.
Literature References:
• Coccaro EF et al. Development of neuropharmacologically based behavioral assessments of impulsive aggressive behavior. J Neuropsychiatry, 1991;3(2):544–551.
• Malone RP et al. A double-blind placebo-controlled study of lithium in hospitalized aggressive children and adolescents with conduct disorder. Arch Gen Psychiatry, 2000;57(7):649–654.
MundtJames C.PhD1EmslieGraham J.MD2ReyesTracy1MayesTaryn L.MS2JoynerKrystleMS2KingJessica2
Center for Psychological Consultation, Madison, WI
UT Southwestern Medical Center, Dallas, TX
Assessing Feasibility, Reliability, and Validity of Computer-Automated Interactive SMS Text Messages to Self-Report Depression Symptoms in Children and Adolescents Using the Quick Inventory of Depressive Symptomatology-Adolescent
Background: The Quick Inventory of Depressive Symptomatology (QIDS) is a patient-reported depression outcome measure validated in both adult and adolescent patient populations. Earlier instrument adaption to accommodate cell phones (QIDS-A17) suggested use of SMS text messaging might be beneficial. This study evaluated the feasibility of automating an interactive, dynamically branching QIDS-A-SMS for use by children and adolescents receiving treatment for depression.
Methods: Participants were patients recruited from a MDD treatment study at the University of Texas Southwestern Medical Center and Children's Medical Center. Participants (and parent/guardian) were interviewed at baseline and 6 weeks later to assess depression severity using the Child Depression Rating Scale-Revised (CDRS-R), QIDS-A-C, and global ratings of depression severity. Participants and parents also completed separate self-report paper forms (QIDS-A-SR-Pat and QIDS-A-SR-Par, respectively). Participants also “text messaged” responses to a series of computer-automated, dynamically branching, text messages to assess symptom severities. The depression measures obtained by clinical interviews, the paper QIDS-A forms, and the QIDS-A-SMS program were compared.
Results: Between February and November 2010, twenty-eight adolescent patients (8–17 years; 15 males, 13 females) provided baseline data; twenty-two returned for follow-up 35–55 days later (M=44.6; SD=4.5 days). 80% of the SMS assessments initiated were completed, requiring a mean of 27.7 minutes and valid replies to 28–35 text prompts. Scale consistencies (Cronbach's alphas) for the CDRS-R, QIDS-A-C, QIDS-A-SR-Pat, QIDS-A-SR-Par, and QIDS-A-SMS were .89, .84, 89. .86, and .78 respectively. Score correlations among the depression assessments were statistically significant (all p-values<.01), ranging from .43 to .90. Clinician and parent-based measures correlated very well (r=.74 to .90), but less well with the patient self-reports (r=.43 to .59). Both patient self-report measures (SMS and paper) correlated well with each other, r=.70. Baseline QIDS-A-C ratings (M=15.1; SD=4.1) were significantly (p-values<.05) higher than both QIDS-A-SR-Pat (M=9.8; SD=5.4) and QIDS-A-SMS Scores (M=12.1; SD=5.5). At follow-up, the ratings were not significantly different. Among patients completing all assessments at both visits, clinician and parent scores showed significant change from baseline to Week 6 but neither of the self-reported QIDS-A measures did so.
Conclusions: Automated, dynamically interactive assessment of symptoms using SMS messaging is feasible. Text messaging can provide reliable self-report data from children and adolescents, and may be helpful for monitoring patient safety or symptom change. Future system should emphasize brevity to reduce respondent burden.
Source of Funding: Support provided through research grants by the National Institute of Mental Health: R01MH039188 (Emslie, Pl) and R43MH086152 (Mundt, Pl).
Literature References:
• Bernstein IH, Rush AJ, Trivedi MH, et al.: Psychometric properties of the Quick Inventory of Depressive Symptomatology in adolescents. Int J Methods Psychiatr Res 19:185–194, 2010.
• Moore HK, Hughes CW, Mundt JC, et al.: A pilot study of an electronic, adolescent version of the quick inventory of depressive symptomatology. J Clin Psychiatry 68:1436–1440, 2007.
• Rush AJ, Bernstein IH, Trivedi MH, et al.: An evaluation of the quick inventory of depressive symptomatology and the Hamilton rating scale for depression: a sequenced treatment alternatives to relieve depression trial report. Biological Psychiatry 59:493–501, 2006.
NewcomerJohn W.MDNicolGinger E.MDYinglingMichael D.FlavinKaren S.SchweigerJulie A.HesslerMartha A.SchechtmanKenneth B.Washington University School of Medicine, St. Louis, MO
Primary Endpoint Results from the Metabolic Effects of Antipsychotics in Children (MEAC) Study
Background: Antipsychotic medications, prescribed to children for on- and off-label treatment of disruptive and aggressive behavior, are associated with increased risk for obesity and related cardiometabolic conditions in this population.1,2 In adults, antipsychotic-related increases in body weight are associated with adverse changes in insulin sensitivity.3 However, to date no studies in children have directly measured whole-body or regional adiposity, or whole-body or tissue-specific insulin sensitivity, during antipsychotic treatment. The NIMH-funded Metabolic Effects of Antipsychotics in Children (MEAC) aimed to characterize changes in adiposity and Insulin sensitivity in children receiving their first course of antipsychotic treatment.
Methods: Antipsychotic-naive subjects ages 6–18 with target symptoms of aggression (Aberrant Behavior Checklist or ABC irritability subscale score ≥18), were randomized to 12 weeks of treatment with aripiprazole, risperidone or olanzapine. Dual energy x-ray absorptiometry (DEXA), abdominal magnetic resonance imaging (MRI), and stable Isotopomer tracing during hyperinsulinemic-euglycemic clamps measured treatment-related changes in adiposity and insulin sensitivity as primary endpoints. ANCOVA was used to test effects of time and treatment condition on adiposity and insulin sensitivity.
Results: Antipsychotic treatment was associated with adverse changes in adiposity and insulin sensitivity in all treatment groups (N=125, mean age 11.5, SD 2.7 years). In addition, medication-specific differences in the magnitude of change from baseline were observed, for example, for increases in DEXA %fat (F[2.119]=8.98, p<0.0001) and decreases in whole-body insulin sensitivity (F[2.94]=2.99, p=0.055). Importantly, treatment produced marked improvement in ABC scores in the pooled group, with a mean decrease of 16.64 points (SD 7.98) that did not differ across medication groups (F[2,120]=0.658, p=0.520)
Conclusions: These results indicate that 12 weeks of initial antipsychotic treatment is associated with increases in adiposity and insulin resistance, changes known to be associated with long term increases in cardiovascular and diabetes risk. Moreover, medication-specific differences in treatment effects on adiposity and insulin sensitivity were observed, in contrast to the similar clinical benefit observed across individual medications. These results underscore the need for careful attention to the balance of potential risks and benefits of antipsychotic treatment in this population, with initial medication choices focused on lower risk medications.
Source of funding: Funded by NIMH Grant Number MH 072912, this research was also made possible by Grant Number UL1 RR024992 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH, RO1MH072912-01.
Literature References:
• Correll CU, Manu P, Olshanskly V, al. e. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA 2009;302(16):1765–1773.
• McIntyre RS, Jerrell JM. Metabolic and cardiovascular adverse events associated with antipsychotic treatment in children and adolescents. Arch Pediatr Adolesc Med 2008 Oct;162(10):929–935.
• Haupt DW, Fahnestock PA, Flavin KA, et al. Adiposity and Insulin sensitivity derived from intravenous glucose tolerance tests in antipsychotic-treated patients. Neuropsychopharmacology 2007 Dec;32(12):2561–2569.
RothmanBrianPhD1OplerMarkPhD, MPH1CorrellChristophMD2ZalsmanGilMD3PandurangiAnandaMD1KohegyiEvaMD4MenlowNicoleMBA1
ProPhase LLC, New York, NY
The Zucker Hillside Hospital, Glen Oaks, NY
Tel Aviv University, Tel Aviv, Israel
Otsuka Pharmaceutical Development and Commercialization, Rockville, MD
Assessing the Reliability of Tanner Staging in CNS Trials: A Cross-Cultural Comparison of European, US, and Indian Raters
Background: Increased prolactin levels associated with some antipsychotic drugs may lead to serious adverse events including gynecomastia, galactorrhea, amenorrhea, and pituitary tumors (Madhusoodanan, et al., 2010; Roke et al., 2009). Despite the need to separate safe psychopharmacological agents from those that might cause problems in sexual maturity, the reliability of instruments used in clinical trials to assess pubertal status (e.g., Tanner Staging) is rarely questioned in research (Slora et al., 2009). To address this gap in the literature, we examined Tanner Staging training data from a global clinical trial. We also Investigated whether cultural factors might impact rater performance.
Method: Following live training at an Investigator Meeting (IM), European (n=54), Indian (n=38), and US (n=14) physician raters assigned Tanner Staging scores to 9 standardized images of male and female subjects via a pen-and pencil Inventory. To assess inter-rater reliability and accuracy, intra-class correlation coefficients (Shrout & Flless, 1979) and concordance with expert ratings were evaluated and compared for each cohort.
Results: While the intra-class correlation coefficient (ICC) for raters (n=106) following training was excellent for the group overall (ICC=.926), differences were found between rater cohorts. European raters were the most reliable (ICC=.975), followed by US raters (ICC=.925), and Indian raters (ICC=.850). With regard to the European and US cohorts, reliability statistics were virtually identical when raters were judging male vs. female subjects. For Indian raters, however, the ICC was lower for female vs. male subjects (ICC=.781 vs. .914, respectively). Concordance data showed a similar pattern. While European and US raters achieved nearly perfect agreement with expert scores regardless of subject gender. Indian raters were less accurate when judging female images.
Conclusion: Results suggest that standardized rater training of Tanner Staging is generally effective, as judged by relatively high levels of inter-rater agreement and concordance. That said, by-country differences were found. Several potential explanations might account for the discrepant results among Indian raters, particularly cultural attitudes and norms regarding cross-gender examinations. Broadly speaking, this study highlights the need to create culturally sensitive training methods when evaluating adolescent pubertal maturation. This will improve raters' ability to accurately detect any possible developmental impacts of antipsychotic drugs.
Source of Funding: N/A.
Literature References:
• Roke, Y., van Harten, P.N., Boot, A.M., Buitelaar, J.K. Antipsychotic medication in children and adolescents: A descriptive review of effects on prolactin level and associated side effects. Journal of Child and Adolescent Psychopharmacology, 2009; 19:403–414.
• Madhusoodanan, S., Parida, S., & Jimenez, C. Hyperprolactinemia associated with psychotropics: A review. Human Psychopharmacology, 2010;25:281–297.
• Slora, EJ., Bocian A.B., Herman-Giddens, M.E., Harris, D.L., Pedlow, S.E., & Wasserman, R.C. Assessing inter-rater reliability (IRR) of Tanner staging and orchidometer use with boys: A study from PROS. Journal of Pediatric Endocrinology, 2009;22:291–299.
RowleyHelenPhD1HealDavidPhD1HackettDavidPhD2
RenaSci Consultancy Ltd, Nottingham, United Kingdom
Shire Pharmaceutical Development Ltd, Basingstoke, United Kingdom
Simultaneous Measurement with Hysteresis Analyses of the Effects of Lisdexamfetamine Dimesylate and D Amphetamine on Striatal Levels of Extracellular Dopamine, Locomotor Activity, and Plasma Drug Concentrations in Freely Moving Rats
Background: Lisdexamfetamine dimesylate (LDX; Vyvanse®, Shire US Inc.) is a prodrug of d-amphetamine currently indicated for attention-deficit/hyperactivity disorder (ADHD).
Methods: The Culex Bambino (BAS Inc) automatically collects intracerebral microdialysate samples together with independently programmable blood sampling from freely moving rats while locomotor behavior is simultaneously monitored. The effects of immediate-release d-amphetamine sulphate (equivalent to 1.5 mg/kg d-amphetamine base i.p.) and LDX (1.5 and 5.0 mg/kg i.p. amphetamine base) on extracellular dopamine concentration in the striatum ([DA]), locomotor behavior, and plasma drug concentrations were compared over 8 hours following dosing.
Results: LDX dose-dependently increased [DA] for up to 300 minutes. Effects of LDX administered at 1.5 mg/kg on [DA] were gradual and sustained with maximal increase at 854% of baseline 75 minutes after dosing. D-amphetamine at 1.5 mg/kg evoked more rapid and substantial increase of [DA] (1291% of baseline at 30 minutes). LDX at 1.5 mg/kg (d-amphetamine base) produced a small increase in locomotor activity, maximal between 90 and 120 minutes returning to predrug levels by 195 minutes. D-amphetamine (1.5 mg/kg i.p.) evoked much greater locomotor activation with an earlier peak (30 minutes) and shorter duration of effect. Hysteresis analyses were conducted on the relationships between 1) plasma d-amphetamine concentration over time vs change in [DA]; 2) plasma d amphetamine concentration vs locomotor activity, and 3) change in [DA] vs locomotor activity. Both compounds yielded anticlockwise hysteresis curves for the first 2 comparisons. However, LDX produced an anticlockwise hysteresis relationship for [DA] vs locomotor activity, while d amphetamine produced a clockwise hysteresis (compared with d-amphetamine, locomotor activity following LDX was less, lagged serum [DA] concentrations, but was sustained as [DA] concentration decreased). This difference between treatments was statistically significant (P<.05).
Conclusions: This study demonstrated that compared with d-amphetamine, LDX produced increases in striatal [DA] later in onset, with a smaller, more sustained peak. Following LDX treatment, rats showed less behavioral activation as striatal [DA] increased, but which was maintained longer as [DA] was declining. The different pharmacodynamic relationship between striatal [DA] and locomotor activity produced by LDX compared with d-amphetamine may have important clinical implications and potential benefits.
Source of Funding: Preclinical research was supported by the sponsor, Shire Development Inc.
GabbayVilmaMD, MS1CoffeyBarbara J.MD1MaoXianglingMS2ShunguDikoma C.PhD2
New York University, New York, NY
Weill Cornell Medical College, New York, NY
Striatal and Anterior Cingulate GABA Deficits as Possible Treatment Targets in Adolescents with Tourette's Disorder: A Proton MR Spectroscopy Study
Background: To date, treatments for Tourette's Disorder (TD) have limited efficacy and are frequently associated with significant side effects. Converging lines of evidence derived from postmortem1 and animal2 studies implicate y-aminobutyric acid (GABA), the major inhibitory neurotransmitter of the central nervous system, in the pathophysiology of TD, but the role of the central GABAergic system has not yet been investigated in vivo. In this pilot study, we assessed GABA levels in adolescents with TD and matched healthy controls (HC) using proton magnetic resonance spectroscopy in two brain regions that have been strongly implicated in TD1: the anterior cingulated cortex (ACC) and the striatum. We hypothesized that adolescents with TD would have significantly decreased ACC and striatal GABA compared to HC.
Methods: Twelve psychotropic medication-free adolescents with TD and 20 HC subjects, ages 12–17, were enrolled in the study. TD subjects met DSM-IV-TR criteria for TD (established with the K-SADS-PL) and had Yale Global Tic Severity Scale (YGTSS) scores ≥10. All participants were right-handed and had negative day-of-scan urine toxicology tests. GABA levels were obtained in the ACC of 12 TD and 20 HC subjects, and in the striatum of 8 TD and 8 HC subjects. All in vivo brain GABA spectra were recorded in 15 minutes from single 18.5cm2 ACC and 9cm3 striatal voxels on a General Electric 3.0 T “EXCITE” MR system, using the standard J-edited spin echo difference method. GABA levels were expressed as ratios relative to unsuppressed voxel tissue water (w). Mean GABA/w values in each voxel for the two groups were compared using rank-based analysis of covariance controlling for age and sex.
Results: As hypothesized, we found significantly decreased mean GABA levels in TD subjects compared to HC both in the ACC (2.38±0.31×10−3 vs. 2.66±0.27×10−3, p<0.02) and the striatum (3.13±0.62×10−3 vs. 3.70±0.54×10−3, p<0.04). Figure 1 shows the individual GABA levels for the two regions (note that ACC data analysis is pending for four TD subjects).
Conclusions: Our findings of decreased GABA levels in adolescents with TD provide the first direct in vivo evidence of GABA alterations in fronto-striatal circuits in TD. Future investigations should further examine the role of the central GABAergic system in TD while focusing on specific constructs of function. Such studies are essential for the development of pathophysiology-guided treatments for TD.
Source of Funding: Tourette Syndrome Association, NIH (KMH077072, KMH077072-0351).
Literature References:
• Kalanithi PS, Zheng W, Kataoka Y, DiFiglia M, Grantz H, Saper CB, Schwartz ML, Leckman JF, Vaccarino FM. Altered parvalbumin-positive neuron distribution in basal ganglia of individuals with Tourette syndrome. Proc Natl Acad Sci 2005;102:13307–13312.
• Veliskova J, Moshe SL. Sexual dimorphism and developmental regulation of substantia nigra function. Ann Neurol 2001;50:596–601.
Veenstra-VanderWeeleJeremyMD1KingBryan H.MD2EricksonCraig A.MD3GinsbergLawrence D.MD4MelmedRaunMD5ScahillLawrence D.MSN, PhD6SikichLinmarieMD7McCrackenJames T.MD8RathmellBarbaraMD9CarpenterRandall LMD9BearMark F.PhD10WangPaul P.MD9
Vanderbilt University, Nashville, TN
University of Washington, Seattle, WA
Indiana University, Indianapolis, In
Red Oak Psychiatry Associates, Houston, TX
Melmed Center, Scottsdale, AZ
Yale University, New Haven, CT
University of North Carolina, Chapel Hill, NC
University of California Los Angeles, Los Angeles, CA
Seaside Therapeutics, Cambridge, MA
Massachusetts Institute of Technology, Cambridge, MA
An open Label Trial of Arbaclofen in Autism Spectrum Disorder Shows Improvements in Multiple Symptom Domains
Background: Fragile X Syndrome is the most common known inherited cause of autism spectrum disorder (ASD). Both drosophila and mice lacking the Fragile X gene show alterations in synaptic plasticity and behavior due to excessive signaling downstream of the mGluR5 metabotropic glutamate receptor (1). GABA agonists may offer one way to offset this increased glutamate signaling. A small molecule screen in drosophila lacking dFMR identified rescue through the GABA-B receptor (2). The GABA-B agonist arbaclofen rescues some behavioral phenotypes in mice lacking Fmr1. A phase II randomized crossover trial of arbaclofen (STX209) and placebo in Fragile X Syndrome found improved ratings of social behavior with arbaclofen. We sought to evaluate response to arbaclofen in children and adolescents with idiopathic ASD.
Methods: An 8-week, open-label flexible dose trial was conducted at 8 sites. Enrollment criteria included a diagnosis of ASD by DSM-IV and Autism Diagnostic Interview (ADI-R), Aberrant Behavior Checklist (ABC) Irritability Score (ABC-1)<16, and age 6–17 years. Up to 2 concurrent psychoactive medications were permitted, but antipsychotics were excluded.
Results: 32 children (29 male) were enrolled, and 25 of 32 subjects completed the study. Two subjects discontinued due to increased agitation or aggression and five discontinued for other reasons. Overall, arbaclofen was well-tolerated. There was 1 serious adverse event (increased aggression), which occurred during planned taper of arbaclofen. In the intent to treat population, there was a significant improvement on the ABC Irritability (24.7±8.3 at baseline, 17.3±10.5 at 8 weeks) and Social Withdrawal (from 18.1±8.2 to 12.6±9.3) subscales. 20 of 32 subjects were rated Much Improved or Very Much Improved on the Clinical Global Impressions-Improvement (CGI-1).
Conclusions: Arbaclofen showed good tolerability and beneficial effects on core and associated symptoms of ASD in this open-label study. A double-blind, placebo-controlled phase II trial in ASD is planned.
Source of Funding: Seaside Therapeutics.
Literature References:
• Dolen G. Osterweil E, Rao BS, Smith GB, Auerbach BD, Chattarji S, Bear MF: Correction of fragile X syndrome in mice. Neuron 2007;56:955–962.
• Change S, Bray SM, Li Z, Zamescu DC, He C, Jin P, Warren St: Identification of small molecules rescuing fragile X syndrome phenotypes in Drosophila. Nat Chem Biol 2008;4:256–263.