
Abstract
Objective:
The purpose of this study was to assess the cardiovascular effects of drugs used for attention-deficit/hyperactivity disorder (ADHD) in children and adolescents treated in community care centers in Italy.
Methods:
This study was an open, prospective, observational study of youth with ADHD treated with atomoxetine (ATX) and methylphenidate (MPH). Measurements of blood pressure and heart rate, and electrocardiogram (ECG) assessment were performed at baseline and at regular intervals up to 24 months.
Results:
By June 2010, 1758 youth were enrolled in the Italian ADHD National Registry. Statistically significant increases were observed in cardiovascular measures: in the MPH group after 6 months in heart rate (+2.01, p=0.01); in the ATX group after 6 months in diastolic pressure (+1.60, p=0.01) and in heart rate (+2.93, p=0.001), and after 12 months in heart rate (+3.26, p=0.003). Compared with the baseline, 59 patients had an alteration of ECG during the follow-up period. Although at 12 months, the probability of detecting an abnormal ECG was higher in the MPH group than in the ATX group, only 2 out of 30 cases at 6 months with altered ECG were considered to have experienced serious adverse events. One case was treated with ATX and one with MPH, and arrhythmia was the detected abnormality.
Conclusions:
Treatment with MPH and ATX in youth appears to have a small but significant impact on the cardiovascular system. The long-term impact of these medications is unknown. Several clinically meaningless ECG alterations were observed mostly in MPH-treated youth. We therefore suggest evaluating cardiovascular risks at baseline.
Introduction
MPH is a sympathomimetic stimulant agent, which has shown to have an effect on HR and BP (Volkow et al. 2003). An open extended trial with Concerta® in children reported slight changes in systolic BP (+3.3 mm Hg), diastolic BP (+1.5 mm Hg) and HR (+3.9 bpm) (Wilens et al. 2004). A recent review showed that stimulant medications used in healthy children and adolescents with ADHD are associated with mean elevations in BP (≤ 5 mm Hg) and HR (≤10 bpm), without changes in electrocardiographic parameters, and that the expected quota of 5–15% of treated children and adolescents may experience these cardiovascular effects (Hammerness et al. 2011).
ATX is a selective norepinephrine reuptake inhibitor (SNRI), and an effect on the cardiovascular system could be expected. Data available from five placebo-controlled trials showed an increase in diastolic BP in children and young boys (Wernicke et al. 2003). The average increase was low, equal to 2.1 mm Hg, and occurred during the first few weeks of treatment. This effect has been confirmed by a recent review, in which a slight increase of BP and HR at the beginning of the treatment had been reported (Stiefel and Besag. 2010). In particular, in children and adolescents within 12 weeks of administration, an increase of diastolic BP (+2–11 mm Hg) and an increase in HR (+5–9 bpm) was reported by controlled studies and one dose-response study.
No evidence of increased cases of QTc interval prolongation in children and adolescents was found for MPH or ATX treatments (Wernicke et al. 2003; Kratochvil et al. 2006; Stiefel and Besag 2010).
Although this alteration of cardiovascular parameter seems to be minor, stimulant or non-stimulant drugs must be used with particular attention in children and adolescents with underlying heart problems. For this reason, before starting a treatment in subjects with ADHD, and during the follow-up period, a cardiovascular physical examination (BP and heart ratio measurements, and electrocardiogram [ECG] control) is recommended (American Academy of Pediatrics 2000; EMEA 2009).
In Italy, in March 2007, the Italian Drug Regulatory Agency (AIFA) granted market authorization of immediate-release methylphenidate (IR-MPH) and ATX for treatment of children and adolescents (6–18 years-old) with ADHD, and, simultaneously, funded and activated the Italian ADHD National Registry, an open prospective observational study, managed by the Italian National Institute of Health (Istituto Superiore di Sanità [ISS]) and supervised by a national expert panel, whose main aim is to practice active pharmacovigilance (Panei et al. 2004).
The Italian ADHD National Registry developed a web site (see
The first aim of this study was to evaluate the effects of MPH and ATX on BP and HR in a prospective cohort of treated children and adolescents with ADHD, and to detect possible abnormalities of ECG, such as prolongation of the QTc interval.
Patients and Methods
The study was approved by the Ethical Committee of the ISS. It was an observational prospective study conducted in Italy. All children and adolescents treated with ADHD drugs were included in this study and were drug naïve. Children and adolescents ages 6–18 years (n=1758), with a diagnosis of ADHD, were recruited between June 2007 and June 2010 across Italy from 87 regional reference centers. The participating centers signed an agreement with the Italian Ministry of Health and were certified to diagnose ADHD and manage patient pharmacological treatment.
All subjects seen in a reference center were referred to the center by the subject's neuropsychiatrist for a suspicion of ADHD, or came on a voluntary basis.
Upon clinical history and clinical interview (95.5% of cases), or semistructured interviews such as Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) or Parent Interview for Children Symptoms, Revised for DSM-IV (PICS-IV) tests (in 62.1% and 7.6% of cases, respectively), or other questionnaire (10.1% of cases), or rating scale such Swanson, Nolan, and Pelham, Version IV (SNAP IV) (49.2% of cases), a diagnosis of ADHD was made according to the American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria. To be diagnosed with ADHD, all subjects had to present symptoms with the following characteristics: 1) onset before the age of 7 years, 2) duration for at least 6 months, 3) pervasiveness (presence in more than one setting, e.g., at home, at school, at social level), 4) significant functional impairment. All subjects were screened for other mental disorders, and subjects with a different spectrum disorder (e.g., autism) were excluded. Furthermore, for the analysis, subjects with follow-up problems such as only one follow-up visit, or a follow-up of <6 months; or subjects with an altered ECG at baseline and with no ECG assessment; or those with no information on drug therapy, were excluded.
All subjects with ADHD started a multimodal intervention (including at least one of the following: child training, parent training, family therapy, psychodynamic therapy, or counseling), before or simultaneously with the beginning of pharmacological treatment. Moreover, the subjects who accepted the pharmacological treatment signed an informed consent explaining the aim of the study and the tests to be done in order to evaluate the primary parameters.
In Italy, specific guidelines are not available and the choice of treatment was based on current clinical practice. We identified two groups for treatment.
Treatment A
The first group consisted of subjects treated with MPH and with behavior treatment, simultaneously. The drug compound was MPH chlorhydrate 10 mg tablet. Administration was oral at the dosage of 0.3–0.6 mg/kg/dose/day. The total daily dose (mean 18.4 mg±10.4 mg) could be administered in two or three doses/daily at the discretion of the subject's neuropsychiatrist. Duration of the renewable prescription was 1 month.
Treatment B
The second group consisted of subjects treated with ATX and with behavior treatment, simultaneously. Patients received ATX chlorhydrate 5 mg, 10 mg, 18 mg, 25 mg, 40 mg, or 60 mg tablets. Administration was oral with the following schedule: started with 0.5 mg/kg/day once a day, for at least 7 days, then increasing the dose 1.2 mg/kg/day to find the optimal dose-response (mean total daily dose 38.6 mg±20.5 mg). Duration of the renewable prescription was 1 month.
Data collection
All clinical and relevant information was collected by standard procedures. Cardiovascular screening before the first administration of the drug was performed and included BP (systolic and diastolic values in mm Hg) and HR (in bpm) measurements, and ECG assessment in all subjects (strongly recommended by the Italian National Institute of Health for all Italian reference centers). During the follow-up, clinical assessment was performed monthly, and included measurements of BP and HR. Every 6 months, an ECG assessment was performed. According to guidelines (Blomström-Lundqvist et al. 2003) we defined “sinus bradycardia” as a sinus rate in absolute value <60 bpm, and “sinus tachycardia” as an increase in sinus rate in absolute value >100 bpm.
According to guidelines (Davignon et al. 1979), we defined normal ECG standards for infants and children. Prolongation of QTc interval was defined as any prolongation (in absolute value) with respect to detected value at the screening before the first administration of the drug, in accordance with the main objective of active pharmacovigilance of the study. ECGs with alterations or pathological aspects were read by pediatric cardiologists.
According to guidelines (Surawicz et al. 2009), we defined an incomplete right bundle branch block a rsr’, rsR’, or rSR’ in leads V1 or V2 with a QRS duration between 90 and 100 ms in children and adolescents between 8 and 16 years of age, and between 86 and 90 ms in children <8 years of age.
The clinical monitoring of the register consisted of regular checking, via the web. All clinical data (relative to recruitment and follow-up) of each enrolled subject was entered in an electronic case report form (eCRF) that was located in a protected area of the web site (
The register database was based at the Italian National Institute of Health, Rome, which was also responsible for its protection and management. Data management was implemented by an infrastructure named “Advanced Multicenter Research” (AMR) and developed by Consorzio Inter-universitario per il Calcolo Automatico dell'Italia nord-orientale (CINECA). This application allowed the checking of any informative flow, the imputing of data, and the monitoring of information up to the analysis of the results. The access to the dedicated web site,
Statistical analysis
ECG controls were performed at baseline and every 6 months from enrolment. BP and HR were measured at baseline and then monthly from enrolment.
Categorical variables are presented as absolute and percent frequencies, whereas quantitative variables are summarized as means±standard deviations (SD). Data have been analyzed separately according to three reference periods: from enrolment (time 0) to 6 months, from 0 to 12 months, and from 0 to 24 months of follow-up. As for treatment, subjects were divided into three groups according to the drug(s) received during the reference period under examination: those receiving MPH only (MPH group), those receiving ATX only (ATX group), and those receiving both drugs, but not simultaneously (MIXED group). The other subjects not receiving either MPH or ATX in the reference period, but receiving other psychotropic drugs, were excluded from the following analyses.
For any reference period, only subjects with data at baseline and at least one measurement during the follow-up period (for ECG) or at the end of the period (in case of BP and pulse) were included in the statistical analyses.
Comparisons between MPH and ATX treatment groups in relation to frequency of ECG abnormalities were performed by χ2 test. Relative risk (RR) with 95% confidence interval (95% CI) was computed as effect size estimates.
Comparisons within each group in relation to BP and pulse data were performed by paired Student's t-test to assess variations during the reference period, whereas differences between MPH and ATX groups for BP and pulse changes that occurred during the period were tested using Student's t-test for independent samples. Nonparametric tests (Wilcoxon for paired observations and Mann–Whitney U test for independent samples) were used to confirm results of parametric analyses.
Results
At the end of June 2010, 1758 children and adolescents with ADHD were enrolled in the Italian ADHD National Registry; 1558 (88.6%) were males, and 200 (11.4%) were females. The mean age was equal to 10.7 years (SD + 2.8 years). In relation to age class analysis, the 10–13-year-old children were the most representative (703 subjects), ∼40% of entire population.
Stratified by type of treatment, 840 (47.8%) subjects were treated with MPH, and 918 (52.2%) were treated with ATX. Excluded from the analysis were 1007 enrolled subjects, for the following reasons: Absence of follow-up at 6 months (50.7%), only one follow-up (29.4%), no ECG at baseline (14.0%), an abnormal ECG at baseline (3.7%), and no available information on drug therapy (2.2%). Demographic and clinical characteristics of subjects stratified by subjects included in the analysis and not included in the analysis are described in Table 1. Comparing the two groups, no statistical differences were observed.
ECG evaluation
The follow-up was 0 to 6 months. Three hundred fifty-one (46.7%) subjects were treated with MPH (mean dose 0.4±0.2 mg/kg/dose/day), 350 (46.6%) with ATX (mean dose 0.7±0.3 mg/kg/day), and 50 (6.7%) with both drugs. ECG at 6 months was not available for some patients in all groups; therefore, only 468 subjects were included in the final analysis, with the following distribution: 214 cases in the MPH group, 221 in the ATX group, and 33 in the MIXED group (see Fig. 1). Demographic and clinical characteristics of subjects included in the three different treatment group are described in Table 2. Comparing each variable through the three groups, no statistical significant difference was detected, and for this reason the three groups were similar for gender and age.
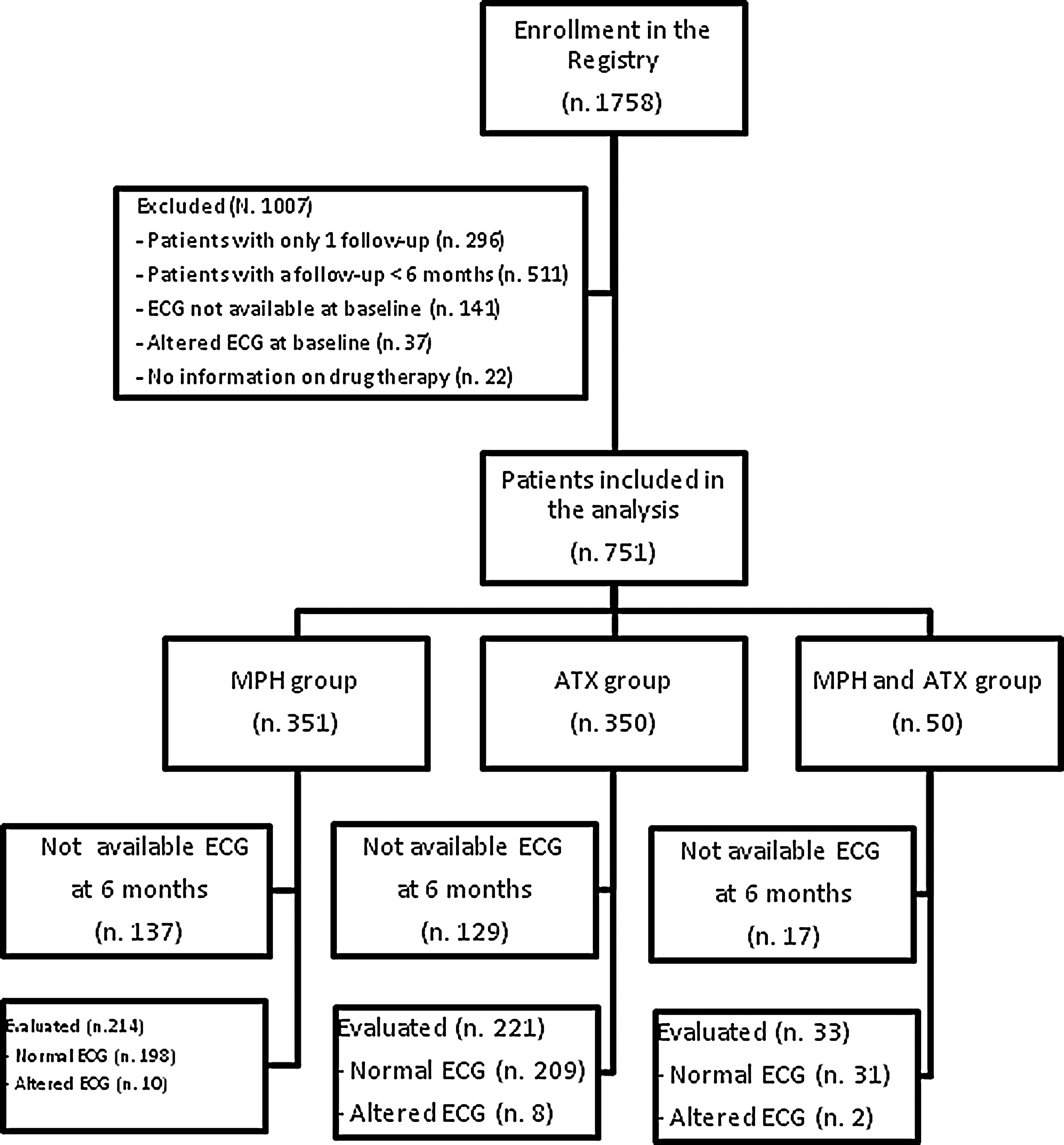
Flow chart of patients at 6 months of follow-up. The figure reports the number of altered electrocardiograms (ECGs) detected at 6 months of follow-up, stratified for each group of treatment (methylphenidate [MPH] group, atomoxetine [ATX] group, MPH and ATX group). The reasons for which the patients were excluded from analysis are also reported.
MPH, methylphenidate; ATX, atomoxetine.
During this period, 20 out of 468 (4.3%) cases had at least one abnormal ECG. Ten cases were in the MPH group (4.7%), eight in the ATX group (3.6%) and two in the MIXED group (6.1%).
Comparing the MPH group with the ATX group, the MPH group showed an RR>1, without relevant differences (RR=1.29, 95% CI: 0.52–3.21; p=0. 58).
Follow-up 0–12 months
Four hundred twelve subjects were included in the analysis, with the following distribution: 190 patients in the MPH group, 169 in the ATX group and 53 in the MIXED group. During this period, 30 out of 412 (7.3%) cases presented at least one altered ECG: 19 cases in the MPH group (10.0%), 7 in the ATX group (4.1%), and 4 in the MIXED group (7.5%). Compared with the ATX group, the MPH group showed a significantly higher risk of ECG abnormalities (RR=2.41, 95% CI: 1.04–5.60; p=0.03).
Follow-up 0–24 months
One hundred fifty-nine subjects were included in the analysis, with the following distribution: 77 cases in the MPH group, 50 in the ATX group, and 32 in the MIXED group. Eleven (6.9%) cases showed at least one altered ECG: eight cases in the MPH group (10.4%), no case in the ATX group, and three cases in the MIXED group (9.4%). The low number of subjects and events makes the point estimate of the relative risk for ECG abnormalities in MPH versus ATX patients unreliable. However, based on these data, we can confidently state that also in this reference period the risk of ECG abnormalities is significantly higher in MPH-treated than in ATX-treated patients (see Table 3).
ECG, electrocardiogram; MPH, methylphenidate, ATX, atomoxetine.
Qualitative description
Table 4 reports the qualitative description of 59 cases, 38 of which were treated with MPH. Twenty-five right incomplete bundle branch block cases, 12 tachycardia cases, 11 bradycardia cases, 6 cases of lengthened QT interval, and 5 conduction disorders were reported. For 12 tachycardia cases, the mean value (±SD) of HR was 106.11 (±4.68), with an increment respect to baseline value of 18.89 bpm. For 11 bradycardia cases, the mean value (±SD) of HR was 53.67 (±4.93), with a decrease respect to baseline value of 11.83 bpm.
First degree atrioventricular block with a PR>200msec.
ECG, electrocardiogram; MPH, methylphenidate; ATX, atomoxetine.
For the prolongation of QTc interval, five out of six cases were treated with MPH, and mean QT interval value was equal to 412 ms (range: 360ms–444ms). In all six cases, QTc values were in the normal range, but were more prolonged with respect to baseline value.
Altered ECGs were reported as being serious adverse events in only 2 out of 30 cases at 6 months. One case was treated with ATX and one was treated with MPH, and arrhythmia was the detected abnormality. In both cases the therapy was interrupted.
Cardiovascular evaluation
We evaluated the BP and HR before the treatment and after 6, 12, and 24 months. Analyzing data separately for each drug, we observed in the MPH group at 6 months a small but not significant increase of systolic pressure (+0.26±13.18) and of diastolic pressure (+0.82±10.99), and a statistically significant increase in pulse (+2.10±15.04). At 12 months, a small (but not significant) increase of diastolic pressure (+1.35±12.40) and in pulse (+1.25±12.69) was confirmed, whereas a small not significant decrease of systolic pressure (−0.49±14.83) was observed in MPH group. After 24 months of treatment with MPH, a small not significant decrease of systolic pressure (−1.00±16.10), and a small statistically significant decrease of diastolic pressure (−3.90±11.23) and in pulse (−3.80±12.82) were observed.
For the ATX group, at 6 months a small not significant increase of systolic pressure (+0.01±12.68), and a small statistically significant increase of diastolic pressure (+1.61±11.25) and in pulse (+2.94±13.11) were observed. At 12 months, small not significant increases of systolic (+0.36±13.52) and diastolic pressure (+0.13±10.83) were confirmed, and a statistically significant increase of HR (+3.26±14.32) was detected. After 24 months, a small not significant increase of systolic pressure (+2.13±9.51), diastolic pressure (+1.11±10.76), and HR (+0.21±13.33) were observed. These data are showed in Tables 5 and 6.
Paired Student t test.
MPH, metylphenidate.
Paired Student t test.
ATX, atomoxetine.
Discussion
There were some factors in the study that limited the conclusions. First, we analyzed 751 children, who matched analysis criteria. To understand the impact on the results, we compared the statistically analyzed population to the one not analyzed, through some parameters, such as age, sex, and type of treatment. No statistical differences were observed. Therefore, we believe that the population analyzed was representative of the patients enrolled in the Italian ADHD National Registry.
Second, we want to emphasize that among the 751 subjects included in the analysis at 6 months ∼37% had not been evaluated because an ECG was not available. This likely represents a reality in long-term community treatment centers for chronic conditions. Moreover, adherence to treatment has not been evaluated, because the study was not designed to allow for it, whereas intention to treat analysis was used to analyze the treatment.
Third, after 24 months of treatment there were few observations, and this could have influenced any possible considerations. Further analyses will be performed in order to consolidate our data.
Our study is based on the Italian ADHD National Registry, an observational prospective study with one of the longest follow-up times (>24 months) reported in the scientific literature, aimed at evaluating the cardiovascular safety of MPH and ATX. All subjects enrolled in the study were drug naïve. This study was performed as a phase IV pharmacovigilance observational study aimed at detecting all changes in the cardiovascular parameters before and during pharmacological treatment. We had also collected and analyzed the variations included in the normal range, because these modifications can represent a clinical warning.
MPH was associated with a mild increase of systolic (+ 0.26 mm Hg) and diastolic (+0.81 mm Hg) BP and HR, over 6 months of treatment. Only the HR, after 6 months of treatment, showed a statistically significant difference from the baseline (+2 bpm). After 12 months of treatment, this trend for diastolic pressure and HR was confirmed, whereas for systolic pressure a moderate decrease (−0.48 mm Hg) was observed. After 24 months, a slight reduction of all parameters, systolic (−1 mm Hg) and diastolic (−3.90 mm Hg) pressure and HR (−3.80 bpm), was observed, which could have been caused by the fact that a small number of subjects was included in the analysis. These changes, especially those observed in the first period of treatment (0–6 months), have also been reported in a recent study conducted in 114 adolescents with ADHD who were treated with extended-release methylphenidate (OROS-MPH) with a follow-up of 6 months (Hammerness et al. 2009a).
Changes after 24 months were unclear, especially where a decrease of BP and HR was detected. However, these results cannot be conclusive, because the subjects included in the analysis at this step of follow-up were too few. Moreover, we cannot verify the adherence of subjects to the treatment over time. However, a normalization of cardiovascular parameters could be expected, partly because of the increasing age of the subjects.
For ATX, in each study period a mild increase of systolic BP, without statistically significant difference, was observed. The difference was equal to +0.90 mm Hg at 6 months up to +2.13 mm Hg at 24 months. The same trend was detected for diastolic pressure, except at 6 months, when a statistical difference was observed (p=0.01). These findings agree with those of two recent publications (Takahashi et al. 2009; Stiefel and Besag 2010), in which an increase in BP was confirmed in the long term. This evidence disagrees with another study, in which an increase of BP occurred in the first weeks of treatment, whereas after >1 year a stabilization of value with no further increase was detected (Wernicke et al. 2003). In our study, the HR showed a statistically significant increase at 6 and 12 months. The variation of pulse was small, between +2.93 bpm and +3.26 bpm, whereas at 24 months a mild not statistically significant increase (+ 0.21 bpm) was observed. This finding is in agreement with others studies (Wernicke et al. 2003; Takahashi et al. 2009; Stiefel and Besag 2010). Moreover, this effect was expected from the pharmacological action of this drug.
It is important to underline that, for both drugs, no serious clinical implication related to changes of BP and HR was observed.
The study showed some changes in the ECG in a group of subjects treated with MPH or ATX, or both drugs. The proportion of abnormal ECG increased over time, at 6 months it was 4.8% and at 24 months of treatment it was up to 9.9%. The probability to observing an alteration in ECG was higher in the MPH patient group than in the ATX patient group, with the difference increasing over time (RR at 6 months was 1.29; RR at 12 months was 2.41; RR at 24 months not available). After 24 months of treatment with MPH, the probability of detecting ECG changes was 10 times higher than with ATX. Despite these findings, no important clinical changes were observed, except in the two observed cases of arrhythmia, for which the pediatric cardiologist suggested a possible correlation of arrhythmia and the pharmacological treatment, and a permanent discontinuation of treatment was advised.
We observed 25 cases of right incomplete bundle branch block. None of these cases were clinically important.
Twelve tachycardia cases and 11 bradycardia cases were observed, and no clinically meaningful changes were observed; however, in all these cases the treatment was interrupted.
We observed 6 cases of prolonged QTc interval on all detected ECG changes; one subject in the ATX-treated group and five subjects in the MPH-treated group. In all six cases, QTc interval value was in the normal range but was prolonged with respect to baseline value, without clinically meaningful changes. In two recent studies that examined the effect of OROS-MPH on the cardiovascular system, no clinically meaningful changes in ECG parameters were observed (Hammerness et al. 2009 a,b).
For ATX use, we reported only one case of prolongation of QT interval without clinical impact. This agrees with other studies, in which there is no evidence that ATX prolongs QT interval (Wernicke et al. 2003; Hammerness et al. 2009b). However, in one other study, a mild prolongation of QT interval (<5 msec) was detected, but without clinical evidence (Takahashi et al. 2009).
Conclusions
Since 2006, the European Medicines Agency (EMA) required, for both drugs, a “black box” warning on the product information about cardiovascular safety (Strattera [atomoxetine] package insert 2003; Ritalin [methylphenidate] package insert 2007). Our study highlights that the use of MPH and ATX in children and adolescents with ADHD seems not to be the cause of clinical cardiovascular implications. Minor increases in HR and BP were observed, cases of sinus tachycardia were observed in only 2.6% of sample and rare ECG abnormalities (4.3% of sample) were detected. While awaiting future studies of long-term impact, clinicians should continue to monitor and be mindful of ongoing debate about the utility/feasibility of ECG screening. Graham et al. suggest that there is no current evidence to support an incremental benefit for routine ECG assessment of ADHD patients prior to initiation of medication (Graham et al. 2011). Thomas et al., in a retrospective study based on current clinical practice of community pediatricians, studied the impact of ECG assessment on children treated with stimulants and found that only 6.4% of patients had an alteration of ECG prior to initiation of treatment with stimulants, and that only one patient out of four had perceived a significant delay of therapy (Thomas et al. 2011). We believe, in accordance with other authors, that prior to treating children and adolescents with ADHD drugs, it is necessary to evaluate the appropriate individual cardiovascular risk (Hammerness et al. 2011) and to define the best assessment of cardiovascular parameters during the treatment, to increase the safety of treatment in children and adolescents (Elia et al. 2010).
Clinical Significance
Regular monitoring of cardiovascular parameters (anamnestic history and BP and HR measurements) is recommended for all patients, but should be considered mandatory, perhaps at more frequent intervals, for subjects at high risk.
Footnotes
Acknowledgments
We thank all participating regional reference centers: Region Liguria (Dr. Barbara Bobba, Dr. Edvige Veneselli, Dr. Maria Josè Baldizzone, Dr. Gianni De Nobili), Region Lazio (Dr. Marco Marcelli, Prof. Maria Giulia Torrioli, Dr. Stefano Vicari, Dr. Sandro Bartolomeo, Prof. Paolo Curatolo, Prof. Anna Fabrizi, Dr. Renato Donfrancesco), Region Emilia-Romagna (Dr. Roberto Parisi, Dr. Dora Suglia, Dr. Modena Nicoletta, Dr. Paolo Stagi, Dr. Flaviana Murru, Dr. Andrea Tullini, Dr.Simona Chiodo, Dr. Antonio Pirisi), Region Veneto (Dr. Ettore Morbin, Dr Luca Milantoni, Prof. Bernardo Dalla Bernardina, Dr. Dino Maschietto, Dr. Cristina Mambelli, Prof. Antonio Condini, Dr. Maurizio Brighenti, Dr. Piergiorgio Miottello, Dr. Roberto Tombolato, Dr Lenio Rizzo, Dr. Andrea Gemma), Region Sicilia (Dr. Sebastiano Musumeci, Dr. Francesca Vanadia, Dr. Giancarlo Costanza, Dr. Donatella Ragusa, Dr. Filippo Calamoneri, Prof. Domenico Mazzone), Region Friuli Venezia Giulia (Dr. Ferruccio Giaccherini, Dr. Marco Carrozzi, Dr. Silvana Cremaschi), Region Lombardia (Dr. Alberto Ottolini, Dr. Daniele Arisi, Dr. Alessandra Tiberti, Dr. Maria L. Terragni, Dr. Paola Morosini, Dr. Corrado Meraviglia, Prof. Carlo Lenti, Dr. Marco Pezzani, Prof. Umberto Balottin, Prof. Paolo Piccinelli, Dr. Giuseppe Chiarenza, Dr. Emilio Brunati, Dr. Vincenzo Montrasio, Dr. Massimo Molteni, Dr. Francesco Rinaldi, Dr. Giorgio Rossi, Dr. Roberto Segala), Region Piemonte (Dr. Flavio Guccione, Dr. Paolo Bailo, Dr. Dante Besana, Dr. Bianca Bassi, Dr. Marco Rolando, Dr. Laura Jarre, Dr. Francesca Ragazzo), Region Sardegna (Prof. Alessandro Zuddas, Prof. Massimo Tondi), Province Alto Adige (Dr. Gianluca Casara, Dr. Donatella Arcangeli, Dr. Ingo Stermann), Province Trento (Dr. Costanza Giannelli), Region Val D'Aosta (Dr. Giovanni Voltolin), Region Abruzzo (Dr. Maria Legge, Prof. Enzo Sechi, Dr. Elena Gennaro), Region Calabria (Dr. Giovanna Campolo, Dr. Antonio La Vitola, Dr. Annalisa Mingolla), Region Puglia (Dr. Angelo Spina, Prof. Lucia Margari, Dr. Angelo Massagli), Region Campania (Dr. Carmela Bravaccio, Dr. Rosario Granato, Dr. Giampina Grimaldi), Region Umbria (Prof. Giovanni Mazzotta), Region Toscana (Dr. Gabriele Masi, Prof. Giovanni Cioni), and Region Marche (Dr. Maurizio Pincherle, Dr. Cardinali Cesare, Dr. Vera Stoppioni, Dr. Tasca Rosolino). We thank Dr. Alessandro Sciahbasi for his support in revising the manuscript, and we thank Mrs. Frederica Regini for editorial assistance.
Disclosures
No competing financial interests exist.