
Abstract
Objective:
To compare fast versus slow switching from stimulants to atomoxetine (ATX) in children and adolescents with attention-deficit/hyperactivity disorder (ADHD).
Methods:
This was a randomized, controlled, open-label study in 6–16-year-old ADHD patients, previously treated with stimulants and cross-titrated (fast switch, over 2 weeks, or slow switch, over 10 weeks) to ATX because of unsatisfactory response and/or adverse events. Study duration was 14 weeks with an ATX standard target dose of 1.2 mg/kg/day. Primary measure was the change from baseline in the investigator-rated ADHD-Rating Scale (ADHD-RS) at weeks 2 and 10. Secondary measures included Global Impression of Perceived Difficulties (GIPD) and Child Health and Illness Profile-Child Edition (CHIP-CE).
Results:
The majority of the 111 patients were male (83.8%, n=93) and mean (SD) age was 11.5 (2.38) years. Mean baseline ADHD-RS total score was 36.0 in the fast and 38.0 in the slow group. Adjusted mean change after 2 weeks was −8.1 (−10.1; −6.1) in the fast and −8.0 (−9.9;−6.0) in the slow group (p=0.927), and after 10 weeks −15.0 (−17.4;−12.6) and −14.3 (−16.7;−12.0), respectively, (p=0.692). GIPD scores did not show differences between groups. Significant differences at week 10 were found in the CHIP-CE achievement domain favoring slow (p=0.036) and the comfort domain favoring fast cross-titration (p=0.030). No significant differences were found for adverse events, and differences for systolic blood pressure (BP) and weight were not considered clinically relevant.
Conclusions:
ADHD-RS and GIPD scores improved in both switching groups. No clinically relevant differences between fast and slow switching from stimulants to ATX were found.
Introduction
A properly controlled procedure to switch from stimulants to ATX is important, as difficulties during the transition may lead to discontinuation of medication despite the expected long-term benefits. As the fast cross-titration approach is less complicated, may possibly lead to a better compliance, and involves a reduced drug exposure compared with slow cross-titration, a fast approach might be preferred in clinical practice. Results from Quintana et al. (2007) indicated that a cross-titration to ATX can be successfully completed in 2 weeks. However, the onset of action of ATX might be slower than the loss of stimulant effect on ADHD symptoms, and effect sizes of ATX have been shown to improve continuously over time (Weiss et al. 2005; Montoya et al. 2009). Therefore, a cross-titration period of 10 weeks has been suggested by clinicians involved in previous ATX trials (Weiss et al. 2006).
Prasad and Steer (2008) did summarize the current approaches for switching from stimulants to ATX in a review article. They discuss immediate switching from stimulants to ATX, cross-titration, and sequential up and down titration of ATX and stimulants as possible methods of switching. Concluding that based on the then-available lack of evidence for direct/fast switching approaches, one of the tapering/titration approaches should be used in patients for optimum symptom control (Prasad and Steer 2008). In addition, an analysis comparing the initiation of ATX treatment once daily with a 3 day titration versus twice daily with a 2 week titration based on two and three studies, respectively, found that there were higher rates of adverse events (AEs) for the 3 day titration scheme than with the 2 week titration approach. This combined with the fast cessation of action of stimulants and the increasing efficacy of ATX over several weeks led Prasad and Steer (2008) to suggest that a slow cross-titration should be used in clinical practice.
Furthermore, only limited data are available on combined stimulant and ATX treatment. Carlson et al. (2007) observed no safety issues with regard to the combination therapy. However, given the small sample size, definitive conclusions could not be drawn.
Our study addressed cross-titration (switching) from stimulant medication to ATX by tapering stimulant therapy (full, two thirds, one half, and one third doses) and increasing ATX (0.5 mg/kg/day or 1.2 mg/kg/day) in various combinations with different durations, depending upon the randomized treatment arm (fast switching or slow switching). This study permitted the collection of further information on the tolerability of combination treatments of a stimulant and ATX. The fast switching strategy applied in this study was already explored in a previous pilot study (Quintana et al. 2007). It was shown that patients who switched to ATX in a 2 week period had a significant reduction in ADHD symptoms.
Methods
Study design
The present randomized, controlled, open-label, multicenter, phase IV comparative study investigated the real-life effectiveness and safety of two switching methods, slow cross-titration compared with fast cross-titration from a stimulant medication to ATX in pediatric and adolescent outpatients with American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) confirmed ADHD (American Psychiatric Association 2000). We changed the term for the assessment of disease severity and outcomes from “efficacy” as originally used in the protocol and retained in the Methods section, to “effectiveness” in the Results and Discussion sections in order to underscore that we are not intending to show a direct drug effect in this study.
The study was conducted in 16 centers in Spain, Portugal, the United Kingdom, Australia, and Mexico from September 2008 to September 2010. All patients had to be pretreated with a stable dose of stimulant medication for ADHD. The study consisted of three study periods (see Fig. 1). Study Period I was the screening period (3–14 days), in which treatment with full dose stimulants was continued. Study Period II (switching period) started at baseline (week 0) and patients were randomized in a 1:1 ratio to either the slow switching or the fast switching group. Assignment to treatment groups was determined by a computer-generated random sequence using an interactive voice response system at a central location for all study sites. The randomization was stratified by site.
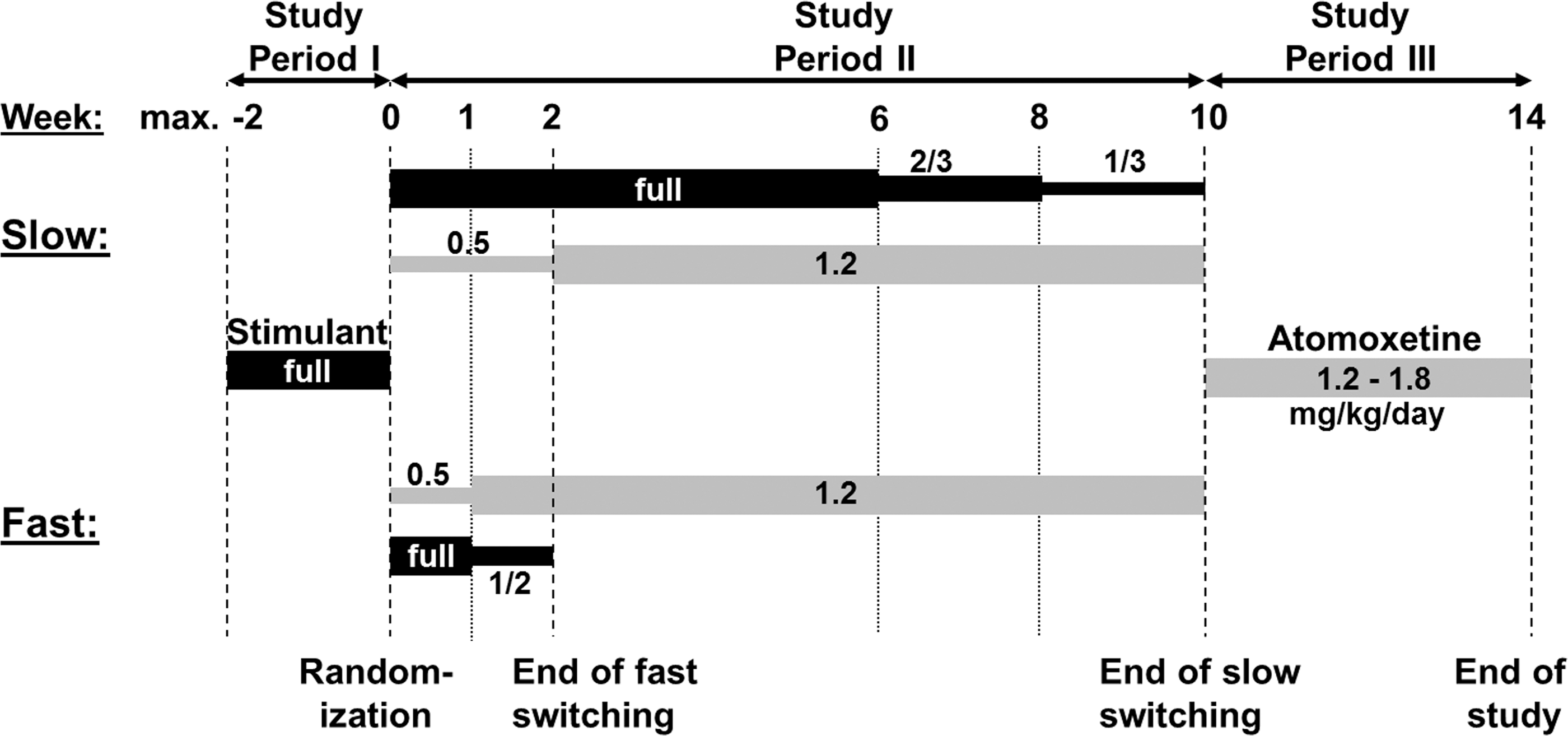
Study design: Dosage of stimulants (black) and atomoxetine (gray) in the fast versus the slow switching group. Stimulant doses are given relative to the dose taken as pretreatment. Atomoxetine doses are given as mg/kg/day. Differing medication regimens were applied from week 1 to week 10.
Both the slow switching and fast switching cohorts started with administration of the full previous stimulant dose plus 0.5 mg/kg/day ATX. In the fast switching cohort this was followed by half stimulant dose plus 1.2 mg/kg/day ATX in the second week, and 1.2 mg/kg/day ATX with no stimulants during weeks 2–10.
In the slow switching cohort, the initial dosage was changed to full stimulant dose plus 1.2 mg/kg/day ATX during weeks 2–6, two thirds of the stimulant dose plus 1.2 mg/kg/day ATX during weeks 6–8, and one third of the stimulant dose plus 1.2 mg/kg/day ATX during weeks 8–10.
ATX was given orally once daily as 10, 18, 25, and 40 mg capsules combined to achieve the body-weight adjusted target dose. Depending upon the use of short-acting and/or long-acting formulations, stimulants were given orally according to the schedule used during pretreatment. During Study Period III (weeks 10–14), stimulants were not administered to any patient and ATX was administered in the same dose as given at the end of Study Period II (weeks 2–10) or in a higher dose of up to a maximum of 1.8 mg/kg/day if the investigator considered a higher dose appropriate according to his or her clinical judgment.
The study was approved by the appropriate ethics committees and was registered at
Patients
Patients were children and adolescents 6 to <17 of age at study start with ADHD of any subtype based on the DSM-IV-TR diagnostic criteria as determined by investigator's clinical assessment and by the Kiddie Schedule for Affective Disorders and Schizophrenia for School Aged Children-Present and Lifetime Version (K-SADS-PL) structured interview (Kaufman et al. 1997) at visit 1. Patients had to have been pretreated with stimulants with unsatisfactory symptom response or experiencing AEs while on methylphenidate therapy to qualify for the study. Patients in need of immediate discontinuation of methylphenidate were not eligible. Patients did not need to meet a formal definition of nonresponse, or a specific minimum dosage required in pretreatment with methylphenidate. Whether patients were considered to have met the criteria of unsatisfactory symptom response was at the discretion of the participating investigators. No specific pretreatment or run-in period within the study was performed.
Patients had to be of normal intelligence (intelligence quotient [IQ] ≥70). Patients with bipolar disorder, psychosis, pervasive development disorder, seizure disorders, suicidal risk, severe allergies, narrow angle glaucoma, a history of alcohol or drug abuse, cardiovascular disease aggravated by increased heart rate or blood pressure, increased sympathetic nervous system activity, clinically significant hypertension, or any unstable medical condition were excluded. Further, patients likely to take additional psychotropic medications or monoamine oxidase inhibitors were excluded.
Patients for whom a structured psychotherapy was planned to be started during the study, also those requiring immediate discontinuation of stimulants because of tolerability problems, and those who took a stimulant dose higher than that specified in the product label, or were taking atypical stimulant regimes not readily amenable to dose reduction, were excluded from participation.
Assessments
The primary objective was to compare the efficacy of two different switching approaches at the end of the fast (week 2) and slow (week 10) transition from stimulants to ATX as measured by Attention-Deficit/Hyperactivity Disorder - Rating Scale IV (ADHD-RS) Parent Version: Investigator-Administered and Scored (Parent:Inv) rating total score change from baseline.
The ADHD-RS is a clinician-administered interview with the patient and the patient's parent (or primary caregiver), and consists of 18 items designed to reflect current symptomatology of ADHD based on DSM-IV-TR criteria. Each item is scored using a range of 0 (reflecting no symptoms) to 3 (reflecting severe symptoms), with total scores ranging from 0 to 54; separate scores may be generated for subscales measuring inattentiveness and hyperactivity/impulsivity (DuPaul et al. 1998).
Further objectives were to assess the efficacy based on ADHD symptoms during slow and fast transition from stimulant to ATX in Study Period II as measured by ADHD-RS Parent:Inv (total and subscales) and the Clinical Global Impressions - Severity scale (CGI-S, Guy 1976), and to assess the broader effectiveness during slow and fast transition from stimulant to ATX in Study Period II as measured by the Child Health and Illness Profile-Child Edition – Parent Report Form Scale (CHIP-CE-PRF).
The CHIP-CE is an instrument that collects self-reported and parent-reported health information about children ages 6–11 (Riley et al. 2006), but has also been successfully used in adolescents (Schacht et al. 2011). The scale comprises 76 items (scored from 1 to 5) included in 5 domains (satisfaction, comfort, resilience, risk avoidance, and achievement) and 12 subdomains. Higher scores indicate positive outcomes. To facilitate interpretation of the scores, they are standardized as T scores to a mean of 50 with a standard deviation (SD) of 10 based on results of a population of healthy children (i.e., a T score of 50±10 indicates normal health).
To assess quality of life of ADHD patients, the change in the perceived difficulties of ADHD during slow and fast transition from stimulant to ATX, the Global Impression of Perceived Difficulties scale (GIPD) parent (GIPD-Par), investigator (GIPD-Inv), and patient (GIPD-Pat) versions were applied (Wehmeier et al. 2008). The GIPD is a five item rating of ADHD-related difficulties assessed in the morning, during school, during homework, and in the evening, and of overall difficulties over the entire day and night. Each item is rated on a seven point scale (1=not at all difficult, 7=extremely difficult) and reflects the situation during the past week.
Treatment satisfaction was measured by the Treatment Satisfaction/Preference Survey (TSPS). The treatment satisfaction part consists of five questions to assess the satisfaction with treatment. Scores from each of the five satisfaction questions (scored from 0 to 4 with low values indicating highest satisfaction) were collected separately. The treatment preference question of the TSPS asked about the preference between medication from the first 6 weeks of the study or the medication the patient was currently taking, and was applied only at the last visit or early discontinuation visit.
In addition, safety and tolerability of slow and fast transition from stimulant to ATX was assessed by analyzing AEs, serious adverse events (SAEs), the Columbia Suicide Severity Rating Scale (C-SSRS), vital signs, body mass index (BMI), and body weight.
The C-SSRS is a scale that captures the occurrence, severity, and frequency of suicide-related thoughts and behaviors. The tool was developed by the National Institute of Mental Health Trial Group for Treatment of Adolescent Suicide Attempters to better categorize suicidal events (Posner et al. 2007).
Statistical methods
All analyses were based on the intention-to-treat (ITT) population, which included all randomized patients who received at least one dose of study drug.
The goal of this study was to give guidance regarding which switching algorithms should be used. Sample size was hence calculated to minimize the probability of erroneously recommending an inferior switching algorithm. To this end, the chance of recommending the wrong treatment was calculated for various sample sizes and expected differences and a total sample of 120 patients was planned. For example, 60 patients per group were required assuming a difference of 0.3 SDs to reduce the statistical probability of an inferior algorithm to be erroneously chosen to 5% using two sided test procedures.
The treatment with the numerically larger mean decrease from baseline at the respective week (2 or 10) was to be declared to be “better or at least similar” in terms of efficacy at the respective week. In case of conflicting results at week 2 and week 10, the treatment that was “better or at least similar” at week 10 was planned to be recommended based on ADHD-RS total score. The mean change from baseline in ADHD-RS total score to all postbaseline visits was calculated based on mixed effects models for repeated measurements (MMRM) based on restricted maximum likelihood estimations, including terms for treatment group, site, baseline score, visit, and visit by treatment group interaction.
Secondary effectiveness analyses
ADHD-RS subscores were analyzed as the ADHD-RS total score. In addition, for the total score and subscores, analysis of covariance (ANCOVA) was applied on the change from baseline and to the last postbaseline non-missing result (last observation carried forward [LOCF]) at each of weeks 10 and 14. The model included treatment and study site as fixed factors as well as a linear term for the baseline score as continuous covariate. The treatment-by-site interaction was tested and removed from the model if not significant at the 10% level. The GIPD mean score, the CHIP-CE-PRF, and the CGI-S were analyzed in the same way as the ADHD-RS total score. For the TSPS satisfaction survey, all five questions were separately summarized using descriptive statistics, and changes from baseline to each of the three postbaseline measurements were analyzed by ANCOVA.
Safety analyses were based on the ITT population. Treatment emergent adverse events (TEAEs, i.e., occurring or worsening after randomization), deaths, SAEs, and other clinically significant AEs (e.g., leading to discontinuation) were collected by general questioning (i.e., no specific AEs were solicited) and analyzed descriptively. AEs were coded according to Medical Dictionary for Regulatory Activities (MedDRA). Percentages for AEs were compared between treatment groups with Fisher's exact test. The time course of vital signs was assessed in the same way as for the secondary effectiveness variables. Separate safety analyses were performed for each dosing combination of ATX and stimulants. Suicide-related thoughts and behaviors based on the C-SSRS were listed by patient.
Results
Of 121 screened patients, 112 patients were randomized. One patient did not receive any study medication, resulting in 111 patients comprising the ITT population. Patient disposition is shown in Figure 2.
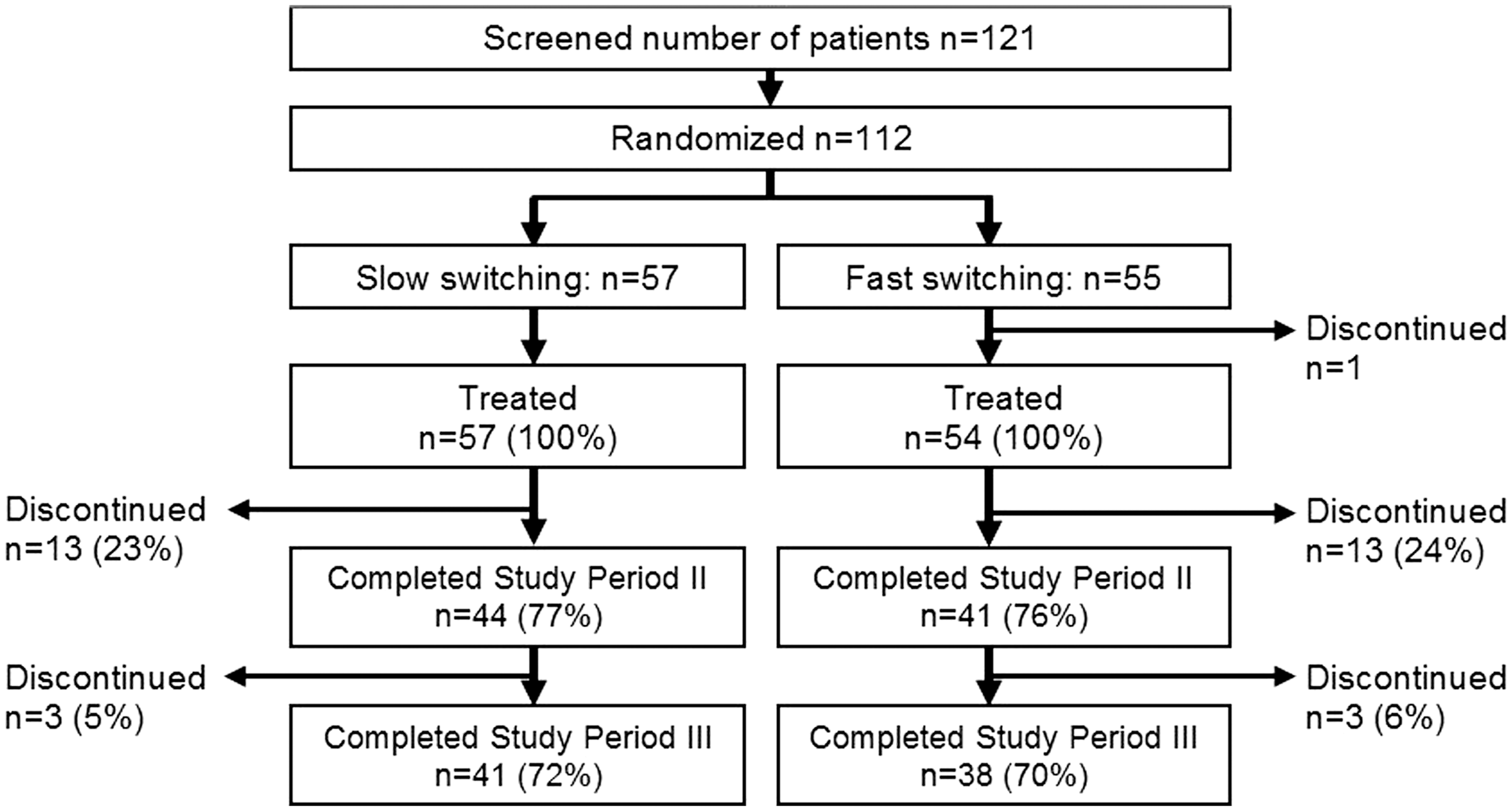
Patient disposition. n: number of patients.
The most frequent (>5%) reasons for discontinuation in Study Period II were protocol violations (slow switching: 6, 10.5%; fast switching: 3, 5.6%; protocol violations reported were in-study dosing errors, methylphenidate pretreatment not amenable to reduction, or disallowed concomitant medication), AE (slow switching: 3, 5.3%; fast switching: 4, 7.4%), and lack of efficacy (slow switching: 0; fast switching 6, 11.1%). All of the discontinuations resulting from lack of efficacy occurred in the fast switching group between week 2 and week 10 (2 in weeks 2–6, 2 in weeks 6–8, 2 in weeks 8–10). During Study Period III, one patient originally in the slow switching group discontinued because of an AE. No other discontinuation was the result of an AE.
Baseline demographics and disease characteristics are shown in Table 1. At study start, most frequently, treatment with long-acting methylphenidate (slow switching: 42, 73.7%; fast switching: 45, 83.3%) or short-acting methylphenidate (slow switching: 12, 21.1%; fast switching: 9, 16.7%) was prescribed. The mean (SD) dose of methylphenidate pretreatment was 34.9 (17.41) mg/day in the slow switching and 33.2 (14.95) mg/day in the fast switching group. The interquartile range was 20–54 mg in both groups.
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD-Rating Scale.
The reason for switching to ATX at baseline was lack of efficacy in 104 (93.7%) patients, and tolerability in 7 (6.3%) patients. At all visits, >95% of patients were compliant with their ADHD medication according to the investigators' assessment. During Study Period III (weeks 10–14), a dose increase of ATX from 1.2 mg/kg/day was necessary in 14 (31.8%) patients of the slow switching and 9 (22.0%) patients of the fast switching group.
Primary analysis: ADHD-RS at week 2 and week 10
The real-life effectiveness of slow versus fast switching was compared at the end of the fast (week 2) and slow (week 10) transition from stimulants to ATX. Descriptive results over time for the ADHD-RS total score for the slow and fast switching groups are graphically presented in Figure 3. ADHD-RS scores improved in both switching groups. At the end of fast switching (week 2) patients improved 8.1 points in the fast and 8.0 points in the slow switching group and the difference in improvement from baseline between switching groups was not statistically significant (−0.1 points in favor of the fast switching group, p=0.927, MMRM analysis). At the end of slow switching (week 10), patients improved on average by 15.0 points in the fast and by 14.3 points in the slow switching group. The respective difference in improvement between switching groups was −0.7 points in favor of the fast switching group and was not statistically significant (p=0.692, MMRM analysis). In the MMRM analysis, no statistically significant difference in ADHD-RS total scores between switching groups was found at any time during the study.
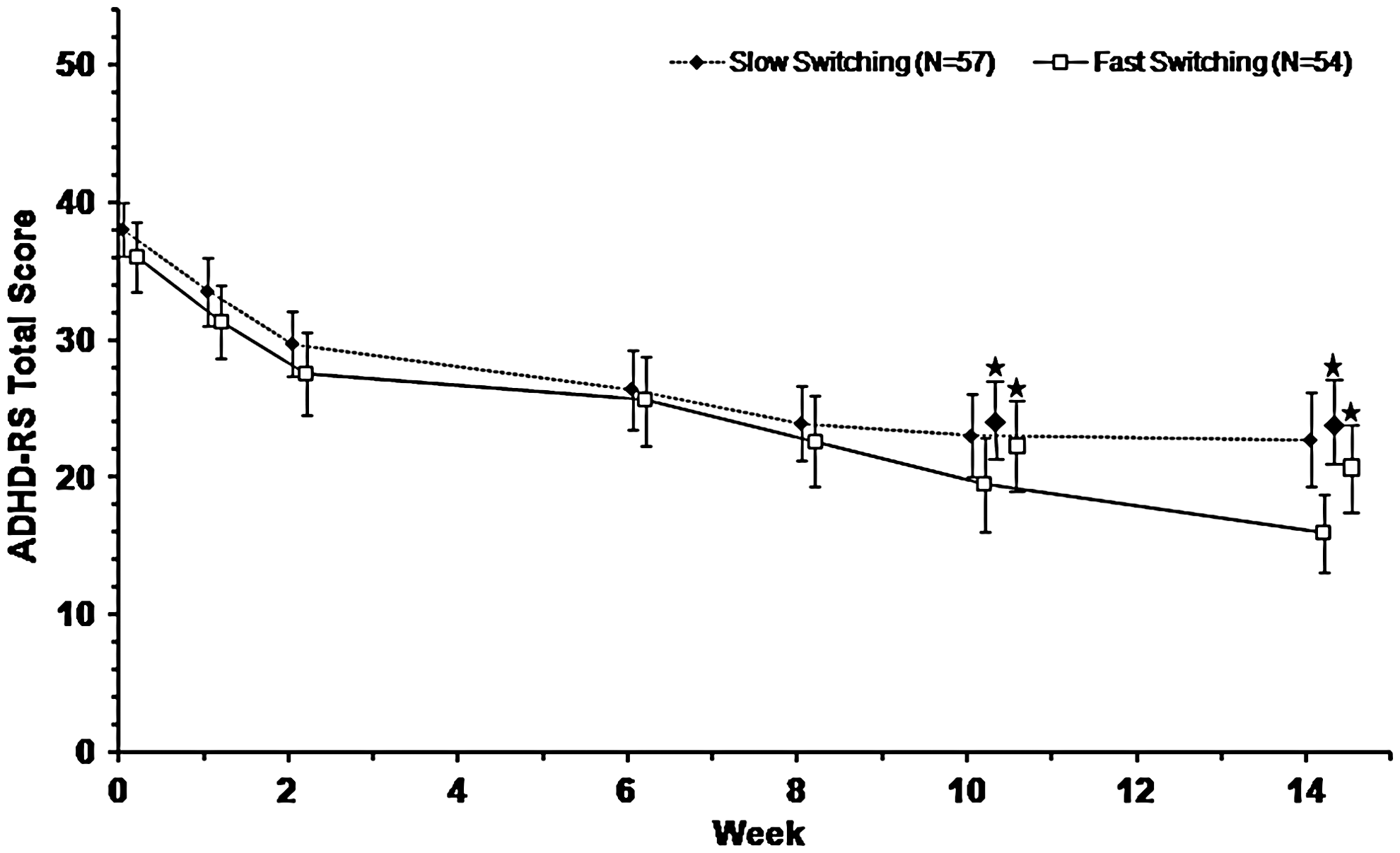
ADHD-RS total score (mean±95% CI) over time. ADHD-RS: Attention-Deficit/Hyperactivity Disorder–Rating Scale (range: 0 [best] to 54 [worst]). SD: Standard deviation; CI: confidence interval. *Values based on LOCF analysis. LOCF: last observation carried forward.
Secondary effectiveness analyses
An overview of the ADHD-RS inattention subscore (ADHD-RS I) and the ADHD-RS hyperactivity/impulsivity subscore (ADHD-RS H/I) at the end of the fast switching and the slow switching period is given in Table 2. No statistically significant differences between patients in the slow and fast switching groups were found in the MMRM analyses.
ADHD-RS, Attention-Deficit/Hyperactivity Disorder - Rating Scale (range: 0 [best] to 54 [worst]); ADHD-RS I, Attention-Deficit/Hyperactivity Disorder - rating scale, inattention score (range: 0 [best] to 27 [worst]); ADHD-RS H/I, Attention-Deficit/Hyperactivity Disorder - Rating Scale, hyperactivity/impulsivity score (range: 0 [best] to 27 [worst]); CI, confidence interval; MMRM, mixed effects models for repeated measurements. aComparison between slow and fast switching group.
Severity of ADHD symptoms did not differ significantly between the two switching groups as measured by CGI-S. CGI-S score (adjusted mean 95% confidence interval [CI]) was improved by −0.7 (−0.9; −0.5) at week 2 both for the slow and fast switching groups (p=0.973), and by −1.7 (−2.0; −1.4) at week 10, also for both switching groups (p=0.898).
Broader effectiveness during slow and fast transition from stimulant to ATX in Study Period II was assessed by CHIP-CE-PRF at the end of the fast switching period and the slow switching period (week 10). An overview of the investigator rated CHIP-CE-PRF domain scores is provided in Table 3. Between-group differences were found in the MMRM analyses only for the CHIP-CE-PRF achievement domain favoring the slow switching group at week 10 by −4.8 points (95% CI: −9.3; −0.3, p=0.036). In contrast, the CHIP-CE-PRF comfort domain results at week 10 were statistically significantly in favor of the fast switching group by 3.4 points (95% CI: 0.3; 6.5, p=0.030). Regarding the CHIP-CE PRF subdomains, the only subdomain exhibiting a statistically significant difference at week 10 was the academic performance subdomain, which was improving more prominently in the slow switching group by −5.1 points (95% CI: −9.2; −1.0, p=0.015) compared with the fast switching group.
CHIP-CE-PRF, Child Health and Illness Profile-Child Edition – Parent Report Form (T score compared with healthy subjects value: 50; lower values show impaired health); CI, confidence interval; MMRM: mixed effects models for repeated measurements. aComparison between slow and fast switching group.
Improvements in perceived difficulties from the patient, physician, and parent perspective were measured by the GIPD scale and did not differ significantly between the slow and fast switching groups at week 2 and week 10 (Table 4).
CI, confidence interval; GIPD, Global Impression of Perceived Difficulties (range: 1 [best] to 7 [worst]); MMRM, mixed model repeated measures. aComparison between slow and fast switching group.
No statistically significant differences in the TSPS treatment satisfaction mean scores were found between switching groups. The treatment satisfaction score (adjusted mean [95% CI]) was improved at week 2 by −0.6 (−0.9; −0.3) for the slow and by −0.5 (−0.7; −0.3) for the fast switching group (p=0.827), and at week 10 by −0.7 (−1.1; −0.3) for the slow and by −0.7 (−1.0; −0.4) for the fast switching group (p=0.810).
The TSPS treatment preference question was answered at the end of the study in favor of ATX compared with the previous treatment with stimulants by 52.6% (30/57) of the patients in the slow switching group and by 66.7% (36/54) of the patients in the fast switching group.
Safety
No statistically significant differences in the overall incidence of TEAEs were found between fast and slow switching groups (see Table 5).
AE, adverse event; MedDRA: Medical Dictionary for Regulatory Activities, MedDRA terms are sorted by incidence in the slow switching group; SAE: serious adverse event; TEAE: treatment emergent adverse event. aFisher's exact test.
The most frequently (>10%) reported TEAEs in the slow switching group by MedDRA preferred term were headache, decreased appetite, upper abdominal pain, and nasopharyngitis. In the fast switching group headache, somnolence, decreased appetite, and abdominal pain were the most frequently reported TEAEs. No statistically significant differences in the incidence of patients experiencing specific TEAEs were found between the fast and slow switching groups. There were no apparent differences in the proportions of patients reporting AEs per week between the slow and fast switching groups over the entire course of the study (see Fig. 4). This was true even between week 2 and week 10, which is the time period when patients in the slow and fast switching groups were receiving different treatments (see Figure 1).
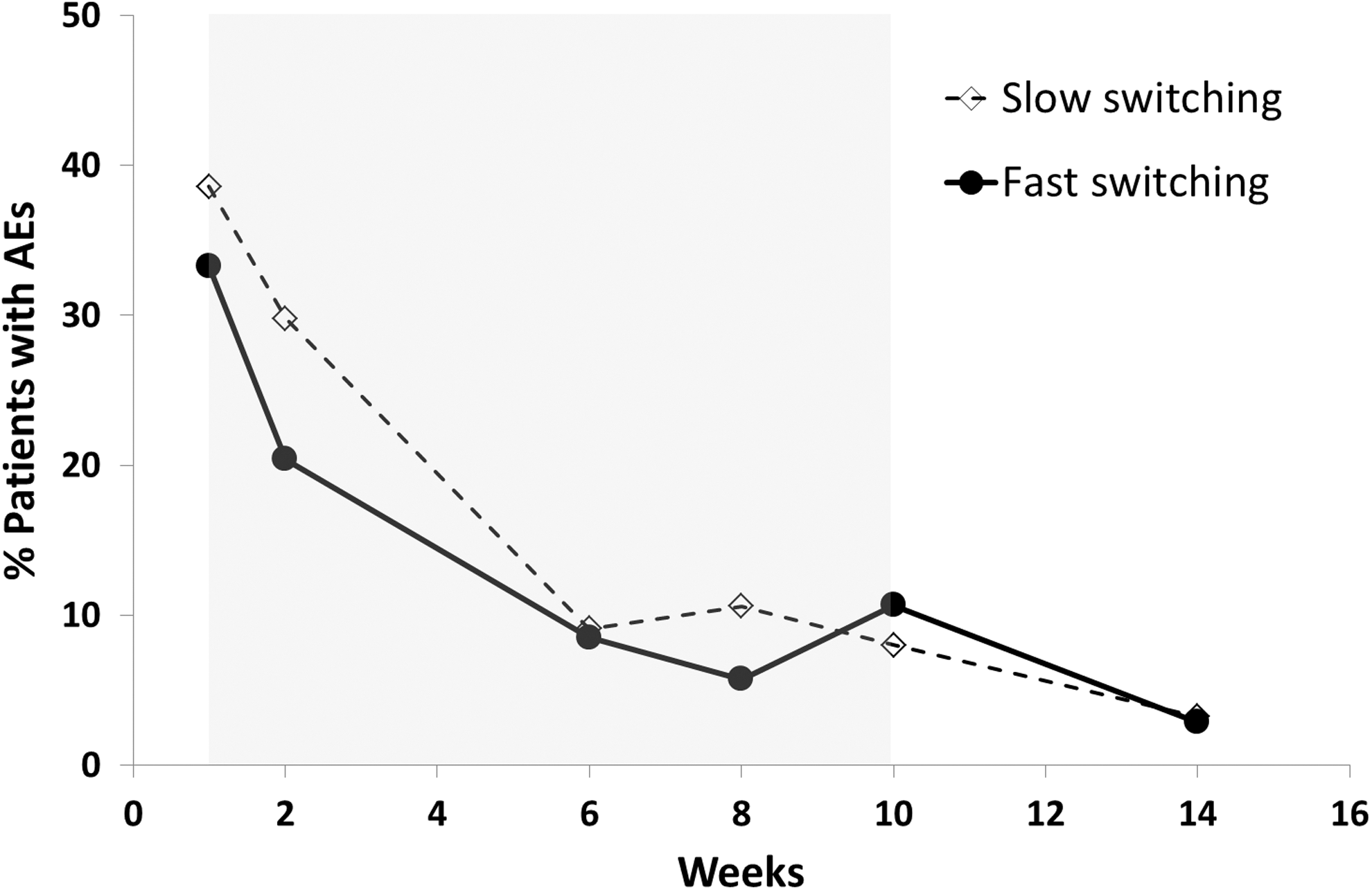
Percentage of patients with adverse events (AEs) over time. The shaded area indicates the time period with different medication regimen applied for fast and slow switching cohorts.
Suicidal thoughts were reported in the C-SSRS by two patients (1.8%), one in the fast and one in the slow switching group.
Overall, eight patients discontinued the study because of AEs, four patients in the slow switching group (two patients abnormal behavior, VIth cranial nerve paralysis, and nausea) and four patients in the fast switching group (altered mood, depressed mood, suicide attempt, and headache).
Of these discontinuing patients, two experienced SAEs. One patient in the slow switching group experienced moderate rash starting 11 weeks after first dose of study medication, followed by severe VIth cranial nerve paralysis (considered as not related to study medication).
For the second patient, an aborted suicide attempt was documented as an SAE. This patient, a 10-year-Caucasian male in the fast switching group, attempted suicide 8 days after the first administration of ATX, which was the day when the ATX dose was increased and the methylphenidate dose was decreased. On that day, the patient was frustrated and angry, proceeded to tie a cord around his neck, and threatened to jump out of a nearby open window. The investigator stated that it was questionable whether the patient wanted to kill himself. The patient had the definite intent to provoke others, as the patient attempted suicide in view of family members and was effectively calmed down by family members. The entire incident lasted <5 minutes. No bodily injury was sustained and the patient was remorseful after the attempt. The patient continued to participate in the study. The investigator stated that the event was related to methylphenidate therapy.
The mean (SD) systolic/diastolic blood pressure increased at week 10 by 1.2(9.03)/2.1(7.61) mm Hg from baseline to 105.7(9.85)/65.9(8.20) mm Hg in the slow switching group, and by 1.6 (9.10)/2.6(8.42) mm Hg to 107.7 (9.91)/65.3(8.77) mm Hg in the fast switching group. A statistically significant between-group difference with a higher increase in systolic blood pressure at week 14 in the fast switching group was found (p=0.040, difference in adjusted means 3.3 mm Hg).
A statistically significant increase in the pulse rate was observed at week 10 both in the slow (3.7 bpm [95% CI: 0.7; 6.7 bpm]) and fast switching group (7.0 bpm [95% CI: 3.2; 10.8 bpm]). No statistically significant differences in pulse rate were found between switching groups using MMRM analysis.
Mean patient weight in the slow switching group did not change significantly at week 10, but patients showed a small but statistically significant decrease in BMI (−0.2; 95% CI: −0.4; 0.0) at week 10. Mean body weight of the patients in the fast switching group did increase but the mean BMI in these patients did not change significantly. Between-group differences in BMI and weight change at week 10 were statistically significant as analyzed by MMRM with an increase in the fast and a decrease in the slow switching group.
Discussion
In our study, no clinically relevant differences in effectiveness and tolerability between patients treated with a fast (2 weeks) versus a slow (10 weeks) cross-titration (switching) approach were found. Consistent results were also seen for quality of life and treatment satisfaction measures, and from the patient, parent, and physician perspectives.
These results were collected in a specific population that failed on stimulant treatment, in >90% because of lack of efficacy. However, patients were not required to have met strict nonresponse criteria to previous stimulant medication in order to enter the study. This reflects the current situation of ADHD treatment in Europe, as in many participating countries methylphenidate is the only stimulant approved for ADHD treatment and a switch to, for example, mixed amphetamine salts, is not easily possible. Patients had on average a high baseline ADHD-RS score of 38, similar to a score of 40 for untreated patients in another study with ATX in Europe (Montoya et al. 2009). In a previous study on patients transitioning from methylphenidate or amphetamine to ATX, the mean ADHD-RS score at baseline was only 33.2 (Quintana et al. 2007), indicating that in our study, patients with more severe ADHD symptoms were recruited.
Despite the different exposure to stimulant medication and ATX in the present study during weeks 2–10, no obvious differences in the overall percentage of patients reporting AEs was found. Even during the time period in which the patients in the slow switching group received the maximum dose of both stimulant and ATX, and patients in the fast switching group received ATX only, no obvious differences in AE reporting were seen.
Regarding individual AE preferred terms, there was a numerically higher incidence of somnolence in the fast switching than in the slow switching group (16.7% vs. 7.0%), which did not achieve statistical significance. For all other preferred terms, no obvious difference between patients in the fast and slow switching groups was found.
In both treatment groups, a statistically significant increase in blood pressure and pulse data was observed. Recently (in November 2011), the European Medicines Agency (EMA) has issued updated information on effects on blood pressure and heart rate of ATX, stating that pretreatment screening and periodic cardiovascular monitoring during treatment should be performed for all patients treated (EMA 2011). The increase in blood pressure was statistically significantly higher at week 14 for the fast switching group (by 3.3 mm Hg). The clinical relevance of these differences between switching groups is unclear, when related to standard values in children from the United States (Rosner et al. 1987; Din-Dzietham et al. 2007; Rosner et al. 2008). In particular, the time point when a difference in BP between switching groups appeared was during a period when the medication in both groups was identical (ATX only).
Our tolerability results are of particular interest, as only limited data on combined stimulant and ATX treatment are available up to now. In a pilot study, Carlson et al. (2007) observed no safety issues regarding the combination therapy of stimulants and ATX. Similar results were seen in our study. Even in the time period when patients in the slow switching group received the maximum dose of both stimulants and ATX, and the fast switching group received ATX only, no obvious difference in the AE reporting was seen. However, the study was not designed to detect differences in safety regarding combination treatment, and because of this, no definitive conclusion can be drawn.
Limitations
General limitations of the present study were the lack of a placebo comparator group, making it difficult to assess the size of the treatment-related portion of the symptomatic improvements seen in the study, as the size of the placebo effect could not be measured. In addition, differences in compliance between the slow and fast switching groups may have contributed to the study results; however, the lack of compliance measurements in the study – such as pill counting or blood concentration measurements – makes it impossible to address those. Finally, the relatively “soft” definition of reasons for changing ADHD medication from stimulants might have induced a relatively large variability that could have obscured differences between switching approaches.
Conclusions
In our study, a switch from stimulant medication to ATX was feasible with both a fast and slow switching approach, and following the switch, ADHD-RS symptoms did improve.
With regard to real-life effectiveness and tolerability results, the fast and slow switching approaches were very similar. It is, therefore, not possible to recommend one approach over the other. Concerns that the onset of action of ATX might not be fast enough to compensate for the loss of stimulant effect were not confirmed. Based on our results, both approaches are feasible, and the decision regarding whether a fast or a slow approach should be used can be made by the physician together with the patient and caregivers based on individual considerations.
Footnotes
Acknowledgment
We thank Thomas Wagner of Trilogy Medical Writing & Consulting GmbH (Frankfurt, Germany) who provided technical medical writing services on behalf of Eli Lilly.
Disclosures
This project was sponsored by Eli Lilly and Company. Vibeke Porsdal, Deborah Quail, Alonso Montoya, Ernie Anand, and Rodrigo Escobar are employees of Eli Lilly. Esther Cardo received research grants from Shire and Eli Lilly. Joaquin Fuentes has worked as consultant for, received research funding from, and provided services to Eli Lilly, Janssen, Astra-Zeneca, Shire, and public/not for profit agencies. Christopher Steer has received research grants from Eli Lilly and Shire and was speaker for Janssen, Eli Lilly, and Shire.