
Abstract
Objective:
A study on chromosomal abnormalities has raised concerns that medication with methylphenidate (MPH) for attention-deficit/hyperactivity disorders (ADHD) might increase the risk of cancer. We performed a rigorous test of the association between cancer and MPH and other drugs used for ADHD, based on data from nationwide Danish registers.
Methods:
Data were linked from five registers containing information on a total of 21,186 patients with ADHD, their drug prescription rates, and associated cancer diagnoses between 1994 and 2010. The cohort included subgroups treated with MPH only, amphetamines only, other ADHD-specific drugs only, antidepressants only, antipsychotics only, mixed medication, and a control group of patients with ADHD who had never taken medication. Frequencies of cancer diagnoses in these groups were compared. In addition, hazard risk (HR) ratios for developing cancer, and survival rates in these subgroups, were analyzed.
Results:
The mean observation time varied between 1.3 and 10.8 years for the various drugs. Cancer rates in the total group amounted to 1.27 per 10 000 person-years before and to 4.33 per 10 000 person-years after onset of treatment. The frequency of cancer was significantly higher (p=0.05) after than before medication only in the antipsychotics subgroup. Furthermore, for mixed medication, the cancer frequency in a small subgroup was significantly higher (p<0.05) after onset of medication than in the unmedicated subgroup. The Cox regression analysis indicated that none of the drugs represented risk factors, whereas higher dose (p<0.001) and older age (p<0.05) were risk factors for developing cancer.
Conclusions:
The concern that children taking MPH and other drugs over long periods of time could be at a significant risk of developing cancer is not substantiated by these findings in a large and representative sample, which had been diagnosed and treated over a period of 17 years.
Introduction
Recently, concern has been raised by a study of chromosomal abnormalities in peripheral lymphocytes in a small group of 12 children taking daily doses of MPH of between 20 and 54 mg, with each child serving as his or her own control and no use of a medication-free group as controls (El-Zein et al. 2005). The authors concluded that three chromosomal abnormalities, namely, chromosome aberration, sister chromatid exchanges, and micronuclei frequencies were induced as a result of MPH treatment. However, it remained unclear whether this well-documented biomarker for cancer risk would actually translate into an increased risk of future cancer in children receiving MPH treatment over an extended time period. Furthermore, the study by El-Zein et al. (2005) has been criticized for its serious experimental shortcomings, and both difficulties of interpreting its results and the uncertainties of its implications for public health have been emphasized (Preston et al. 2005; Jacobson-Kram et al. 2008).
Following the same strategy, a first replication study in 12 children and 7 adults with a recent diagnosis of ADHD and all naïve to MPH studied the cytogenic effects on peripheral lymphocytes before and 3 months after initiating MPH treatment (Ponsa et al. 2009). This study revealed no evidence of chromosomal aberrations in their sample. Further studies found no increased frequency of micronuclei in 21 children with ADHD, all naive to MPH, after 3 months of treatment (Walitza et al. 2007), in an enlarged sample of 31 children after 3 months of treatment (Walitza et al. 2009), and after an extended observation period of 12 months in 12 children (Walitza et al. 2010). None of the three studies revealed an elevated cytogenic damage. Another experimental study also failed to replicate the genotoxic findings among 47 children after 3 months of methylphenidate and amphetamine treatment (Witt et al. 2008).
The findings of all these experimental studies are limited because of relatively small sample sizes and short observation periods, so that the ultimate potential risk for developing cancer cannot be evaluated. Therefore, epidemiological studies are clearly needed to elucidate the association of any cancer with MPH treatment in large and representative samples. Unfortunately, currently there are only two epidemiological studies addressing this issue. An older study identified 529 patients treated with MPH within a larger cohort of patients who had been exposed to 215 different drugs. In a follow up over 13–15 years, the study found no increased incidence of cancer in this subgroup of MPH users (Selby et al. 1989).
A more recent study used a much larger cohort of patients in the San Francisco bay and parts of California`s Central Valley (Oestreicher et al. 2007). The authors compared cancer rates at 18 sites among 35,400 MPH users who had taken it before age 20, to rates among the local United States health provider membership in unexposed individuals (age, sex, and calendar year standardized), and found 23 cancers among MPH users, versus 20.4 expected. MPH use was associated with an increased risk of lymphocytic leukemia, based on eight observed cases. The medical records of these exposed cases did not reveal any lymphocytic leukemia risk factors (prior cancer, radiotherapy or chemotherapy, or Down syndrome). The authors concluded that there is no moderate or strong association between MPH use and cancer risk in children, although their ability to examine dose and duration of use or risk at specific sites was limited by small numbers of participants. Furthermore, the authors called for further study of MPH use and lymphocytic leukemia risk to determine whether their results are caused by chance alone. The limitations of the study include no clear description of the representativeness of the sample, no base rate calculation of cancer in the ADHD sample, and a shortage of detailed treatment information.
To our best knowledge, so far, the issue of an increased risk for cancer under medications other than stimulants for ADHD has not been raised in the literature. However, antidepressants are frequently used as a second line drug for ADHD, and antipsychotics are also frequently used by clinicians for this condition. For the latter, it is known that, for example, taking clozapine entails an eight times increased risk for acute myeloid leukemia (Nielsen and Boysen, 2010).
Given the current limited epidemiological evidence on whether or not there is a significant association between MPH treatment and cancer, the objective of the present study was to take a new look at the issue based on large and representative data from nationwide registers in Denmark. In this approach, data on treatment for ADHD with psychoactive drugs other than MPH, including antidepressants and antipsychotics, and both dose and duration of treatment, were available, so that further control comparisons could be performed.
Methods
Data sources
The study was approved by the Danish Data Protection Agency, National Board of Health and Statistics Denmark. In Denmark, at birth each individual is assigned a unique identification number (CPR) which makes it possible to identify the individual across various registers. The patients included in this study had to be included in the Integrated Database for Labour Market Research (IDA database) in order to extract birth year and gender information. For the present study, we used data from four additional registers.
Danish Psychiatric Central Register (DPCR)
This database was used for the identification of all patients diagnosed with ADHD in the period between 1994 and 2010. The time period was chosen because the register has included the diagnosis of hyperkinetic disorders in the current International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), since 1994. The definition of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) used in the United States, and hyperkinetic disorder according to the ICD are not fully identical, with the latter being less inclusive than the former. In clinical practice, clinicians in Denmark are asked to diagnose according to ICD-10 criteria. However, over the years, they have inclined also toward using the term “ADHD,” including its DSM criteria and rating scales that have been derived from these criteria.
Prescription Database
This register contains information on all individually prescribed medications. ADHD drugs in this register are defined according to the World Health Organization (WHO) Anatomic Therapeutic Chemical classification system. The following drugs (anatomical therapeutic chemical [ATC] code) were considered: methylphenidate (NA06BA04 and NA06BA11), amphetamines (NA06BA01, NA06BA02, NA06BA03, N06BA06, N06BA10 and N06BA12), other ADHD-specific drugs available (pemoline NA06BA05, modafinil NA06BA07, fenozolone NA-06BA08, and atomoxetine NA06BA09), antidepressants (NO6A), and antipsychotics (NO5A).
Based on the entire observation period, the analyses considered the following six subgroups: 1) MPH only treatment, 2) amphetamine only treatment, 3) other ADHD-specific drugs only treatment, 4) antidepressants only treatment, 5) antipsychotics only treatment, and 6) no medication. A large subgroup of patients receiving various combinations of drugs was not considered in the analyses because of not allowing clear interpretations of drug effects. The prescription database does not contain data on drug dosages but, rather, on the total number of sold defined daily dosages (DDD) according to recommendations of the WHO Collaborating Centre of Drug Statistics Methodology (WHO Collaborating Centre for Drug Statistics Methodology 2011). The DDD for MPH is 30 mg. The DDD reflects the total exposure to drugs over time without considering discontinuous periods of treatment. Furthermore, we calculated the total time period for the various drug treatments irrespective of doses and discontinuation of drug exposure.
The National Patient Registry (NPR)
All cancer diagnoses are based on the ICD-10 classification codes. Both any cancer diagnosis and the specific site and type of neoplasms according to this classification were considered for analysis.
The Mortality Register
This register includes dates and causes of death of participants and was only used in the analysis using survival methods. We followed the patients from either onset of medication or birth (in the no medication subgroup) until either cancer or death occurred. If none of these events occurred, the data for these individuals were censored on December 31, 2010.
Statistical analyses
Descriptive statistics including frequencies, means, and standard deviations were computed for each intervention group. The times before and after onset of drug treatment were compared by use of z-statistics (Wilcoxon signed rank test). Frequencies of any cancer diagnosis were calculated for the time before or after onset of drug treatment for ADHD. Differences between frequencies of cancer in these two groups and between frequencies of cancer in the after onset of drug treatment condition and the no medication group were compared using Fisher's exact test. The impact of the various drug interventions on any cancer was studied by using survival analysis based on Cox regression measuring hazard risk (HR) ratios adjusted for time varying covariates, Kaplan–Meier statistics, and the log rank test. Statistical analyses were performed by use of the Stata statistical software version 11.
Results
A total of n=21,186 patients with an ADHD diagnosis in the years between 1994 and 2010 covered by the NPR were suitable for the main analysis. We identified a total of n=15,319 patients who received at least one prescription for MPH, amphetamines, other ADHD drugs, antidepressants, or antipsychotics, or a combination of drugs. In this sample, n=7418 (50.95%) received MPH only, 28 (0.19%) amphetamines only, 115 (0.79%) other ADHD-specific drugs only, 704 (4.84%) antidepressants only, and 426 (2.93%) antipsychotics only. A subgroup of n=6628 (43.27%) patients received various combinations of these drugs over time and were called the “mixed drugs subgroup.” and a total of n=5867 patients with ADHD who had never received any medication served as a control group. The final sample size used for the present analyses was n=21,186 including 15,940 (75.24%) males and 5246 (24.76%) females.
The duration of recommended drug doses in terms of DDD and the total time period before and on treatment are shown in Table 1, indicating that MPH was the major drug of choice in the observation period. Amphetamines were rarely used, because there were no commercial products available, and pharmacy prescription had to be used. In a sizeable proportion of the sample, antidepressants and antipsychotics also had been prescribed.
Kruskal–Wallis test: χ2=3487.79, df=5,
Comparisons of the periods before drugs and on drugs.
ADHD, attention-deficit/hyperactivity disorder; DDD, defined daily doses.
The various drug subgroups differed significantly in age at onset of medication, with MPH and amphetamines prescribed in childhood, other ADHD-specific drugs in adolescence, and antidepressants and antipsychotics in early adulthood. All means and standard deviations of the years on DDDs were lower than the period after onset of drug treatment. The mean period on drugs varied between 1.29 and 10.78 years for the five drug subgroups. With the exception of a reverse situation with the amphetamines, all observation periods before onset of drug treatment were significantly longer than the periods on the various drugs.
In the total sample, 68/21,186 patients (0.32%, or 1.80/10,000 patient-years) with a diagnosis of cancer were identified. There were 29/21,186 patients (0.14%, or 1.27/10,000 patient-years) who had received their diagnosis before any drug treatment. An additional 30/21,186 patients (0.14%, or 4.33/10,000 patient-years) developed cancer after the onset of any drug treatment and 9/21,186 patients (0.04%, or 1.18/10,000 patient years) developed cancer without ever having received any medication. The numbers and rates of any cancer diagnoses in relation to onset of drug treatment in the six subgroups with various drug interventions and in the group without any medication are shown in the upper part of Table 2. Only in the antipsychotics subgroup was the frequency of any cancer significantly higher after than before the onset of drug treatment. Furthermore, only the mixed subgroup had a significantly higher cancer rate than the group without any medication. However, the rates of cancer before and after onset of medication did not differ significantly in the MPH subgroup.
Fishers exact test comparing A and B.
Fishers exact test comparing B and C.
ADHD, attention-deficit/hyperactivity disorder.
The frequencies and percentages of the various subtypes of cancer in relation to onset of drug treatment are shown in the lower part of Table 2. Under all four conditions, malignant neoplasms of lymphoid, hematopoietic, and related tissues were most frequent, followed by neoplasms of the male or female genital organs and the skin. There was no specific pattern of cancer diagnoses in the no medication subgroup and there were no significant differences when comparing the specific cancer frequencies before and after onset of drug treatment, on the one hand, and after onset of drug treatment and under no medication, on the other hand.
After removing the 28 and 115 patients who had only received amphetamine or other ADHD- specific drugs from the cohort because of no observed cancer cases in these treatment groups, a follow-up study was performed with the remaining 21,043 patients by using Cox regression analysis adjusted for time varying covariates (i.e., treatment group, age at onset of medication, and duration of treatment, i.e., years on DDD) and year of birth, and stratified on sex. To study the particular drug risk on cancer, it was defined that patients became at risk of cancer at birth in order to have the same follow-up period for all participants. Only the MPH, the antidepressants, the antipsychotics, the mixed subgroup, and the no medication subgroups were included because the two other subgroups (amphetamines or other ADHD-specific drugs) did not develop any cancer after onset of drug treatment. This procedure resulted in a sample of 21,043 patients. The treatment group of reference was the no medication subgroup. The use of treatment group as a time varying covariate ensured that each patient was in the no medication subgroup until the date of onset of medication, when he or she switched to MPH, antidepressant, antipsychotic, or mixed treatment. In the same way, age at onset of medication and duration of medication was set to 0 whenever an individual was not receiving treatment. The findings show that none of the various drug conditions represented a risk factor, whereas dose (represented by years on DDD) and earlier birth (older age), were risk factors for developing cancer (Table 3).
DDD, defined daily doses.
Figure 1 provides information coming from survival analysis depicting the time from onset of drug treatment until cancer was diagnosed in the four drug groups included in the analysis and in the subgroup with no medication. The log rank test was applied to test the equality of the survivor functions across the subgroups, and the finding indicated significant differences in the survival curves of the various drug subgroups (χ2=60.23, df=4, p<0.001).
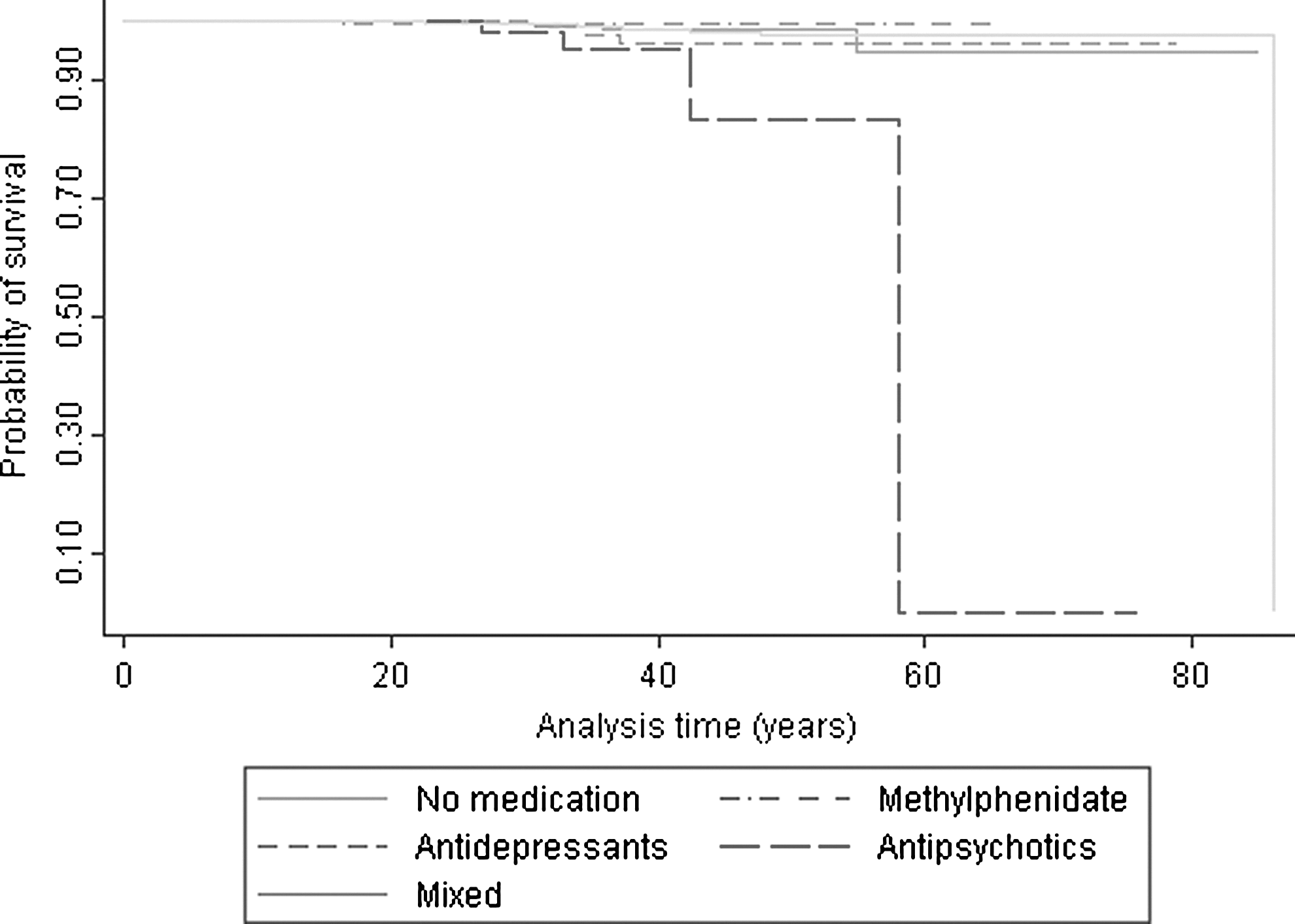
Survival analysis findings (Kaplan–Meier curves) for various drug subgroups.
Discussion
This is the first epidemiological study on the association between treatment of ADHD with MPH or other drugs and cancer, based on a large and representative nationwide dataset. A unique possibility to link various register-based datasets in Denmark allowed specific tests of the claim based on a small study with children that the exposure to MPH might be associated with the development of cancer (El-Zein et al. 2005). Data on various other drugs used for the treatment of ADHD and from an unmedicated group of patients with ADHD were analyzed for comparison. The mean DDD observation time of MPH exposure was 2.7 years. For antidepressant or antipsychotic drug exposure, the mean DDD observation period was shorter, whereas it was longer for the subgroup receiving mixed drugs. Because ADHD is diagnosed predominantly in childhood, most of the observation time took place during adolescence and young adulthood.
The prevalence rates for any cancer and particularly under MPH treatment were rather low. The original speculation for any potentially causal association of MPH treatment and cancer because of an increased rate of chromosomal abnormalities (El-Zein et al. 2005) did not receive support from the present findings for various reasons. First, with an equal frequency of any cancer before and after onset of MPH treatment, there was no indication that cancer in ADHD patients might be the result of MPH treatment. However, it has to be noted that the small number of cancer patients after onset of MPH treatment was significantly higher than under the control condition of ADHD without any medication ever.
Second, the direct comparisons of the various specific cancer rates for patients before or after onset of drug treatment did also show similar rates. All associations were chance findings. The rates were highest but not significantly increased in neoplasms of the lymphoid, hematopoietic, and related tissue. The single other epidemiological study addressing the present research question found lymphocytic leukemia to be most frequent in MPH-treated patients (Oestreicher et al. 2007). However, this observation was not sufficiently controlled, and may have been a chance finding, as the authors acknowledge. In fact, the present findings do not point to a significant association, because the rates for these specific cancers did not differ significantly among those diagnosed with cancer before or after onset of medication and treated with MPH and other drugs used for ADHD. The finding of five patients who developed cancer after onset of medication with antipsychotics may match the results of the register study by Nielsen and Boysen (2010), indicating that clozapine has an increased risk for acute myeloid leukemia.
The risk model based on HR ratios with the no medication subgroup as reference clearly showed that none of the drugs, including their combinations, were risk factors for developing cancer. Therefore, there is another strong argument against any cancerogenic effects of MPH in particular. It became quite evident that among the variables considered in the risk model, only dose and age were relevant. These findings were also controlled for effects caused by varying time periods in drug exposure, duration of treatment, and age at onset of treatment. Therefore, the two general factors of dose and age, rather than any specific drug, contributed to the risk of developing cancer.
The dose effect could imply a generic effect of drug treatment, or simply a greater power effect in this analysis, than for any one drug. An effect caused by multiple drug use would be less likely, because the mixed drug effects in the analysis were not associated with an increased risk. Furthermore, we cannot rule out a potential link between severity of ADHD and cancer because the dataset was based on categorical ADHD diagnoses only and did not contain a severity indicator. However, we controlled in our analyses for use of antipsychotics, excluding that this potential marker of illness severity had a relevant effect on the significant dose–response relationship. In addition, one needs to bear in mind that this was only a post-hoc analysis, and that multiple unmeasured variables are related to the use of higher ADHD medication. Therefore, as we did not find an overall effect of ADHD medications, it could also well be that the dose relationship found in our post-hoc analyses is an artefact. Nevertheless, future studies assessing the association between ADHD medications and cancer risk should pay attention to potential dose effects of ADHD medications, and include measures of disease severity and other variables that could influence both dosing choices of ADHD medications and cancer risk. Finally, the age effect on cancer risk simply implies the greater probability of getting cancer with increasing age.
There are various limitations of the present study. First, the analyses were not based on actual doses of medication, but rather on DDD. Second, despite the much longer observation periods than in all previous small-sized studies, the observation time period of the present study amounted only to a 17 year period of data collection. Observation periods before drug treatment were significantly longer than periods on drug treatment. Among the 15,319 patients receiving drug treatment, a large proportion of ADHD patients were diagnosed only after the year 2005, so that the time to developing cancer was rather short. However, one may argue that cancer latencies may take much more time, as much as up to 20 years, so that more long-term epidemiological follow-up studies may be warranted.
Conclusion
The reported findings indicate that neither MPH nor any other drug commonly used in ADHD treatment has any specific and significant association with cancer within the observed time frame. However, longer observation periods of medicated patients with ADHD with a specific focus on higher doses are clearly warranted.
Clinical Significance
This study found no significant association of medications used for ADHD and cancer. Given the large numbers of individuals diagnosed with ADHD and preferentially treated with medication, this conclusion may reduce concerns about drug treatment among the affected patients, their relatives, and the public at large.
Footnotes
Disclosures
H.-C. Steinhausen has worked as an advisor and speaker for the following pharmaceutical companies: Janssen-Cilag, Eli Lilly, Novartis, Medice, Shire, and UCB. In the past, he has received unrestricted grants for postgraduate training courses or conferences by Janssen-Cilag, Eli Lilly, Novartis, Medice, and Swedish Orphan International. Within the last 4 years, he has not received any financial support for drug studies. Dorte Helenius has no conflicts of financial interest to disclose.