
Abstract
Background:
Attention-deficit/hyperactivity disorder (ADHD) is a pediatric psychological condition commonly treated with stimulant medications. Negative media reports and stigmatizing societal attitudes surrounding the use of these medications make it difficult for parents of affected children to accept stimulant treatment, despite it being first line therapy.
Objective:
The purpose of this study was to identify factors that influence parental decision making regarding stimulant treatment for ADHD.
Methods:
A systematic review of the literature was conducted to identify studies: 1) that employed qualitative methodology, 2) that highlighted treatment decision(s) about stimulant medication, 3) in which the decision(s) were made by the parent of a child with an official ADHD diagnosis, and 4) that examined the factors affecting the decision(s) made. Individual factors influencing parental treatment decision making, and the major themes encompassing these factors, were identified and followed by a thematic analysis.
Results:
Eleven studies reporting on the experiences of 335 parents of children with ADHD were included. Four major themes encompassing influences on parents' decisions were derived from the thematic analysis performed: confronting the diagnosis, external influences, apprehension regarding therapy, and experience with the healthcare system.
Conclusions:
The findings of this systematic review reveal that there are multiple factors that influence parents' decisions about stimulant therapy. This information can assist clinicians in enhancing information delivery to parents of children with ADHD, and help reduce parental ambivalence surrounding stimulant medication use. Future work needs to address parental concerns about stimulants, and increase their involvement in shared decision making with clinicians to empower them to make the most appropriate treatment decision for their child.
Introduction
Although these behaviors may appear to be synonymous with those of a child lacking parental discipline (McLeod et al. 2004; dosReis and Myers 2008), research has shown that ADHD is in fact characterized by abnormalities in brain structure and neurotransmission that emerge through a combination of biological, genetic, and environmental factors (Furman 2005; Curatolo et al. 2010; Nigg et al. 2010). Despite this, many parents experience feelings of inadequacy or self-blame for their child's behavior and find their parenting responsibilities emotionally taxing (Sawyer et al. 2002). Public resistance towards the use of medications as a solution for ADHD, emerging from negative media coverage and lack of understanding about the biological causes of the disorder, serve to strengthen the negative sentiments displayed by parents of affected children (Johnston et al. 2008).
Stimulant medications are considered to be first line therapy in ADHD (Kaplan and Newcorn 2011) but despite this, they are the most contentious of the available treatment approaches (Daley 2006). These medications are especially portrayed in a negative light by the media and public opinion despite evidence in the literature that highlights that only mild and short-lived side effects occur early in treatment (Merkel and Kuchibhalta 2009). Aside from concerns surrounding side effects, many perceive that these medications are used as a means of control to benefit parents rather than children themselves (Daley 2006). This notion is reverberated by parents who commonly convey concern about the belief that stimulant medications turn children into “zombies” and worry that their child will be stigmatized against as a consequence (Daley 2006; Olaniyan et al. 2007). Parents are also cautious of how friends, family, and members of the public would perceive their parenting capabilities in the event that they were to initiate therapy for their child (Peters and Jackson 2009).
Although the efficacy and safety of these medications have been established (Merkel and Kuchibhalta 2009; Merkel 2010), the pressures placed on parents of affected children often make it difficult for them to make the decision to initiate treatment (Bennet et al. 1996; McGuinness 2008). This is of particular concern, as parents play a key role in discussing, implementing, and maintaining treatment plans that are set up with the child's physician. As the decision to initiate medication for ADHD is variable and at times difficult for parents (Braaten and Rosén 2000; Johnston et al. 2008), it is important for healthcare professionals (HCPs) to understand the factors that influence parental decision making when it comes to initiating or continuing ADHD medication. Whereas many studies exploring efficacy of ADHD medications have been performed, data on the factors that influence parental decision making regarding ADHD medications are more limited.
The purpose of this systematic review is to explore findings from qualitative studies investigating the factors influencing parental decision making when deciding on stimulant therapy for their child. Qualitative studies typically employ focus groups or in-depth interviewing which, compared with quantitative studies, allow greater insight into the personal perspectives, attitudes, feelings, and beliefs of the individuals involved (Morton et al. 2010). This is an essential component of research in this field, which commonly involves individual and complex parental experiences surrounding decision-making processes when considering treatment options for their child. The focus of this review on stimulants stems not only from these medications being first line therapy for ADHD, but perhaps more importantly from the controversy surrounding them despite this classification. By exploring findings from qualitative studies in this area, a greater conceptual understanding of the topic can be achieved (Sandelowski et al. 2006; Zimmer 2006). The findings of this review can provide HCPs with evidence on how best to deliver information to parents and their children while also facilitating communication and encouraging parent and child involvement in shared decision making.
Methods
Literature search and search strategy
A literature search was conducted using MEDLINE®, Embase, PsycINFO®, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane electronic databases. As ADHD was not officially recognized until 1980 when it was published as a disorder in American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. (DSM-III) (American Psychiatric Association 1980; Knutson and O'Malley 2009), the search for each database was limited between January 1980 and September 2011. The following MeSH terms and key words were used to identify relevant studies:
Inclusion and exclusion criteria
This review includes studies that have met all of the following requirements: 1) Used qualitative methods, for example, interviews or focus groups, 2) a treatment decision about stimulant medication for ADHD needed to be made (whether the decision was to begin or continue therapy), 3) treatment decisions were made by the parent, caregiver, or legal guardian (for convenience referred to as parent henceforth) of the affected child, 4) there was an official ADHD diagnosis for the child, and 5) there was an examination of the factors involved in the parental treatment decision-making process. The following types of studies were excluded: Those including parents with a child at risk of developing ADHD; those that examined decision making unrelated to stimulant medication, for example, in relation to cognitive behavioral therapy, dietary modifications, or complementary medicines; those that used structured questionnaires as the sole method for data collection or reported only quantitative data; and those that did not directly elicit information from the parents.
Methodological quality assessment
The consolidated criteria for reporting qualitative (COREQ) research framework (Tong et al. 2007) was used to assess the reporting quality of each selected study. This is a 32 item checklist used to assess the rigor of qualitative studies by covering three main domains: research team and reflexivity, study design, and data analysis and findings. The items covered also allow assessment of the transferability of study findings to different healthcare settings (Morton et al. 2010).
Data extraction
The included studies were examined in detail, and a structured summary was created to allow comparison across the studies (Harden et al. 2004). The following information was extracted from each included study: Country where research was conducted; number of participants; data collection and analysis methods; and the principal, individual factors influencing parental treatment decision making. Major themes encompassing these individual factors were assigned and noted for each study. A thematic framework was established using the major themes, and a thematic analysis was conducted to elicit the prominent themes, as outlined in the literature (Harden et al. 2004; Parsons et al. 2007). Data from each study were summarized against each of the major themes identified, and higher level themes that better reflected the data were examined (Richie and Spencer 1994). The major themes were then finalized and participant quotes representing each theme were extracted to illustrate the themes further.
Results
Study Selection
The search strategy yielded a total of 348 citations (see Fig. 1). Of these, 304 were excluded after review of their titles and abstracts. The full texts of the remaining 44 citations were examined in more detail and of these, 33 were excluded because they did not examine parental treatment decision making (n=16), were not specific to stimulant medications (n=11), or were duplicate or non-primary research articles (n=6).
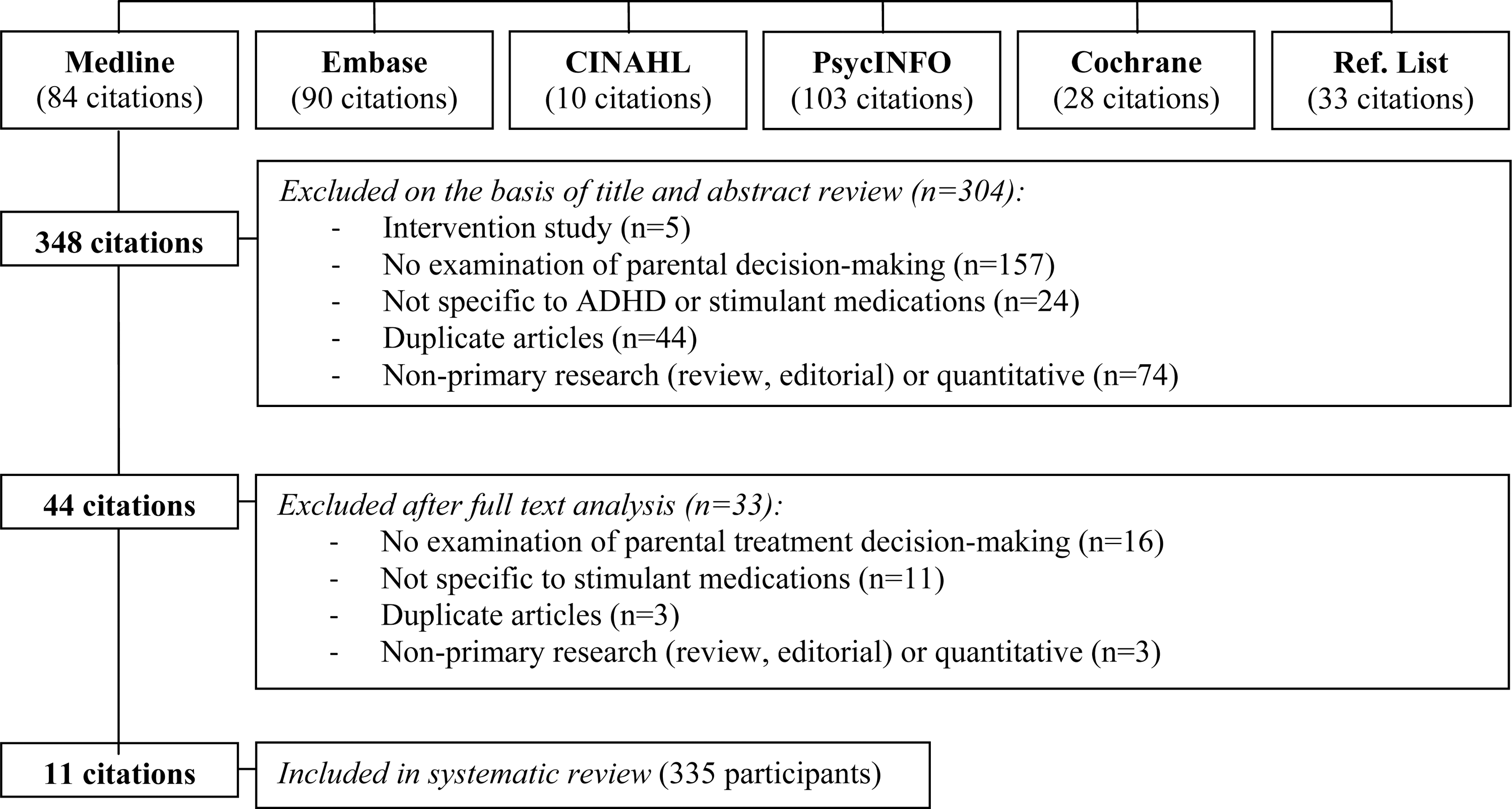
Results of search strategy and process for the identification of studies included for review. Please note that the 11 citations report on the findings of 10 studies. Ref. List=Citations sourced from the reference lists of relevant articles.
The remaining 11 studies (Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011) met the inclusion criteria and were included in the review (see Table 1). The publications by dosReis et al. (2009, 2010) report on alternate findings of the same investigation. Therefore, although the 11 included publications present the findings of 10 investigations, the total number of studies will be referred to as 11 henceforth for ease of reference.
The two publications, dosReis et al. 2009 and dosReis et al. 2010, report on alternate findings from the same investigation.
ADHD, attention-deficit/hyperactivity disorder.
The majority of these studies were conducted in the United States (n=6) followed by Australia (n=2), Canada (n=1), Denmark (n=1), and England (n=1), and all were published within the last decade. Eight studies used interviews as their method of inquiry (Singh 2003; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; dosReis et al. 2009, 2010; Fiks et al. 2011), whereas the remaining three studies used focus groups (Bussing and Gary 2001; Charach et al. 2006; Brinkman et al. 2009). A total of 335 participants were included in the studies, and sample sizes were relatively similar across the selected studies as shown by an average of 34 and a median of 31 participants per study. Most studies involved both parents deciding to initiate treatment and parents deciding to continue treatment for their child (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008; dosReis et al. 2009; Fiks et al. 2011).
Comprehensiveness of reporting
There was variability among the studies in fulfilling the criteria on the COREQ checklist. Extent of reporting completeness varied between 14 and 28 of the 32 items on the checklist as presented in Appendix B. All 11 studies reported their sample size, method of approach, and the participants' characteristics. Audio recording, presentation of participant quotations, and observation of clear theme derivation from the data collected were also noted by all 11 studies. Seven studies included a description of their data coding procedures (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011). Only one study reported returning transcripts and results to participants for checking and feedback (Charach et al. 2006).
Factors affecting parental treatment decision making
Four major themes encompassing the factors involved in parental treatment decision making in ADHD were identified: confronting the diagnosis (denial, skepticism about the existence of ADHD, parental/familial disagreement, reliance on preconceptions), external influences (negative media coverage, influence of social networks, advice from child's school), apprehension regarding stimulant therapy (side effects, impact on child's future, stigma, financial costs of treatment), and experiences with the healthcare system (exploring alternative treatment options, mistrust of medical evaluation, previous poor experience with a HCP, lack of information and support). The individual factors within the major themes discussed in each study have been highlighted in Table 2. Participant quotes corresponding to these factors and their interpretation are presented in Table 3.
ADHD, attention-deficit/hyperactivity disorder; HCP, healthcare provider.
ADHD, attention-deficit/hyperactivity disorder; HCP, healthcare provider.
Confronting the diagnosis
The preliminary step in the parental treatment decision-making process was that of confronting or coming to terms with the initial ADHD diagnosis (Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011). A prominent factor involved in this stage was that of denial, whereby parents could observe functional impairments in their child but often displayed great difficulty accepting that it was the result of a defined disorder. In some instances, parents were skeptical about the existence of ADHD as an actual condition and whether it could, therefore, be validly diagnosed and treated. Receiving a diagnosis of ADHD also meant that there was often familial disagreement, again with regard to accepting the diagnosis and the consequent actions to be taken to address the issue. Influencing these deliberations were the preconceptions held by parents through previous contact with parents of children affected by ADHD and through their own personal views regarding the topic.
Denial
Three of the 11 studies described parental difficulty in accepting their child's ADHD diagnosis as a factor that affected treatment decisions (Charach et al. 2006; Taylor et al. 2006; Brinkman et al. 2009). This parental denial stemmed from a range of behaviors and understandings; however, at the fundamental level, parents found it difficult to reconcile the stereotypical image of a child with ADHD with the behaviors of their own child (Taylor et al. 2006). The parents who compared their child's behavior with the behaviors emphasized by sensationalized media reports often felt that their child's diagnosis was inaccurate or invalid (Taylor et al. 2006). Also contributing to parental denial was a common feeling of being overwhelmed by the diagnosis (Charach et al. 2006) and active attempts by parents to fight the diagnosis (Brinkman et al. 2009) to maintain the “non-ill identity” of their child.
Skepticism about ADHD as a condition
Some parents displayed great hesitancy accepting the existence of ADHD as a condition (Bussing and Gary 2001; Singh 2003; Taylor et al. 2006; Jackson and Peters 2008; dosReis et al. 2009). For many parents, this diminished the validity of their child's diagnosis in their own minds. Some parents did not view their child's behavior as being an illness (dosReis et al. 2009), and even though the parents could recognize that their child was poorly behaved, they often attempted to justify these behaviors in other ways (Singh 2003). Singh (2003) found that fathers tried to justify their sons' bad behaviors by blaming indulgent mothering approaches and by a belief in a “boys will be boys” attitude. Other parents expressed that they felt their children's behaviors were a result of poor parenting (Taylor et al. 2006). Parents spoke about the uncertainty they felt about “rushed” diagnostic evaluation procedures (Bussing and Gary 2001) and how this negatively influenced their acceptance of the diagnosis and their ultimate decisions to initiate therapy with stimulants.
Parental/familial disagreement
In confronting their child's diagnosis, parents often needed to deal with conflicting opinions of their spouses in addition to the views of other family members and close friends. The five studies that explored this revealed that often, one parent was in agreement with the diagnosis made by the HCP while the other parent was in complete opposition to it (Singh 2003; Charach et al. 2006; Jackson and Peters 2008; Brinkman et al. 2009; Fiks et al. 2011). Parents conveyed that at times they felt that their child was “caught in the middle” between the opposing views of the two parents (Fiks et al. 2011). Often this clash of parental opinions led to confusion with the child's treatment plan and had negative consequences on the child (Brinkman et al. 2009). This situation became more complex with the introduction of the views and opinions of close family and friends (Charach et al. 2006), which often conflicted with HCP advice or the opinions of the child's parents (Jackson and Peters 2008). Dilemmas commonly arose in these situations, with the parents needing to arrive at some point of agreement (Singh 2003) for the next steps to be taken in what they perceived to be the best interests of the child.
Reliance on preconceptions
Parental preconceptions regarding the nature, causes, and treatments of ADHD heavily influenced the parental decision-making process as explored in eight studies (Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010). It was clear that parental preconceptions tied in with each of the aforementioned factors involved with confronting the diagnosis. Parents often relied on information learned from previous contact with a parent of a child diagnosed with ADHD to determine whether their child had been accurately diagnosed, and also to gauge the likelihood of their child requiring treatment with stimulants (Bussing and Gary 2001; Taylor et al. 2006; Brinkman et al. 2009; dosReis et al. 2009). Other parents' preconceptions were derived from information in the media, principally regarding the overprescription of stimulants for children and side effects of treatment (Charach et al. 2006; Jackson and Peters 2008; dosReis et al. 2010). Parents also had their own personal apprehensions and beliefs about ADHD (Singh 2003) that were not influenced by external sources. These preconceptions impacted upon each factor involved in confronting a diagnosis of ADHD for parents, and ultimately shaped the decisions made.
External influences
The decision to initiate or continue therapy was also strongly affected by apparent external influences (Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2010; Fiks et al. 2011). Negative media coverage surrounding overprescription of stimulant therapy and side effects made it difficult for parents to agree to initiate and, in some instances, continue therapy for their child. Adding to the ambivalence experienced by parents was the influence of social networks. This affected parents' ability to come to terms with the diagnosis and often led them to question the appropriateness of medication for their children. Advice or pressure from the child's school whether through parents observing impediments to their children's academic performance or through verbal feedback from teachers, also influenced parental treatment decisions.
Negative media coverage
Inaccurate and sensationalized media reports surrounding ADHD and its treatments had a major impact on parental decision making (Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2010). There was a common feeling among parents that media reports presented ADHD in a negative light, often in the context of undesirable and at times violent or criminal behavior (Jackson and Peters 2008). This negativity not only surrounded the condition, but also its treatments. Many parents expressed that the media displayed the worst possible outcomes of stimulant treatment (Taylor et al. 2006). Common parental concerns stemmed from media reports that claimed that stimulants were being overprescribed in children (Charach et al. 2006) as a result of some doctors' lax prescription practices (Taylor et al. 2006). Other media reports sensationalized side effects of stimulant treatment including its “zombie-like” effects (dosReis et al. 2010) and potential addictive properties (Brinkman et al. 2009).
Parents felt that media reports not only focused on side effects of treatment, but that they also evoked a communal sense of parental blame for initiating stimulant treatment for their children. Concern about media portrayal of stimulant medications as an easy way out for families who were reluctant to invest time and effort to address the children's troublesome behaviors was common among parents (Charach et al. 2006; Taylor et al. 2006). Exposure to such media reports increased the complexity of the treatment decision-making process for parents, as it raised parental doubts and concerns about the need for medication and medication side effects, and made parents become conscious of how others judged their parenting capabilities.
Influence of social networks
The views and opinions of members within parents' social networks regarding the appropriateness of treatment options also influenced parental decision making (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009; Fiks et al. 2011). This external influence either encouraged parents to proceed with stimulant therapy or deterred them from initiating this treatment path. Family members and friends often swayed parents' decisions by reinforcing the negative media portrayals of stimulants and by questioning the ADHD diagnosis (Bussing and Gary 2001). According to the parents in these studies, older family members were more likely to reject the need for medication and to attribute the condition to poor parenting (Brinkman et al. 2009). Some parents relied on religious figures for advice about stimulant treatment commencement for their child (Leslie et al. 2007). Other parents actively sought information from a family member in the medical profession (Fiks et al. 2011). Parents felt that they were often pressured from many directions to make the right decision. Some parents expressed that their friends and family did not fully appreciate their struggles, which meant that, at times, the parents' decisions remained unchanged (Charach et al. 2006; Taylor et al. 2006).
Advice from child's school
Many parents first became aware of their child's condition via the child's school. As explored in six studies (Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009), advice from the child's teacher was common, particularly as in this environment the child's academic and social progress can be easily noted. Despite this, parents described that they received conflicting messages from school personnel. Some parents stated that they were simply notified by the child's teacher that the child was experiencing some academic and/or social difficulties and that the child may require stimulant therapy (Hansen and Hansen 2006; Leslie et al. 2007). In other instances, parents felt that they were being constantly pressured by school personnel to place the child on stimulant medication (Bussing and Gary 2001; Jackson and Peters 2008). This made some parents question whether school personnel were keeping the best interests of the child in mind or whether they simply wanted a quick fix solution to relieve the child's teacher from needing to address the child's difficulties in the classroom (Charach et al. 2006). Other parents trusted and acted upon the advice of school personnel based on the belief that they would be familiar with the signs of ADHD and the appropriate course of action to be taken, from experience with many schoolchildren (Brinkman et al. 2009). Interestingly, some parents stated that the school personnel themselves advised against placing the child on stimulant medication (Charach et al. 2006; Leslie et al. 2007), which led the parents to believe that stimulant medications were either unnecessary or detrimental to their child's health.
Apprehension regarding stimulant therapy
The specific concerns parents had about stimulant therapy were also very influential in terms of the treatment decisions made, and were explored in all 11 studies. As previously noted with regard to negative media coverage and influences of social networks, parents were apprehensive about the potential short- and long-term side effects of stimulants. Additionally, parents held concerns about the consequences of stimulant treatment, including the impact it would have on the child's future and the potential for addiction or development of a drug abuse problem in the long term. Stigma associated with stimulant therapy was another commonly displayed concern by parents, with fear of how others were going to view both themselves and their children if they were to commence treatment. For some parents, financial costs of stimulant treatment made them re-examine their treatment choice.
Side effects
Parental concern about side effects of stimulant therapy was examined in 9 of the 11 studies (Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010). The most common concerns parents had about potential side effects prior to commencing treatment surrounded “zombie-like” effects (Charach et al. 2006; dosReis et al. 2009, 2010), growth stunting (Hansen and Hansen 2006; Leslie et al. 2007; dosReis et al. 2009) and liver damage (Brinkman et al. 2009; Bussing and Gary 2001). Parents feared that their child would appear “drugged” while taking stimulants and that the medication would change the child's personality (Jackson and Peters 2008). The parents' experiences with side effects after commencing stimulant therapy commonly involved observing stomach aches (Bussing and Gary 2001; Charach et al. 2006), reduced appetite (Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006), weight loss (Hansen and Hansen 2006), sleeping disturbances (Charach et al. 2006; Hansen and Hansen 2006), zombie-like effects (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008) and development of facial tics (Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006). For some of these parents, the positive effects of the stimulants on their child's behavior and progress outweighed these side effects, whereas for others, this led to treatment discontinuation.
Impact on child's future
As explored in seven of the studies, parents considered not only the short-term effects of stimulant therapy but the long-term consequences of this treatment for their child (Bussing and Gary 2001; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010). Generally, parents were uncertain about the negative health impacts of long-term treatment, their child's ability to persist with long-term treatment, and the potential for addiction in the future. Some parents were concerned that future research would reveal that stimulants have negative health outcomes with prolonged use, and that they would feel extreme guilt for “ruining” their child by placing the child on stimulants (Bussing and Gary 2001). Further, some parents associated stimulant treatment with development of criminal behaviors and potential incarceration (Bussing and Gary 2001). Parents also expressed worry about how their children were going to manage their medication as they grew older (Hansen and Hansen 2006; Taylor et al. 2006). In some instances, stimulants were viewed as a temporary measure until the child could reach a certain academic milestone such as entry into high school or university (Hansen and Hansen 2006). Whereas other parents were concerned about the ability of their children to remember to take their medication as prescribed once they moved away from home and whether this medicine taking would interfere with their daily routine and lifestyle (Hansen and Hansen 2006). A common belief held by parents was that stimulants were addictive and had the potential to lead to drug abuse. This association was more apparent in situations where parents knew of drug addicts or substance abusers within their extended family (Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009).
Stigma
Closely linked to the negative media coverage and the influence of social networks is the stigma that was experienced by parents of children with ADHD when deciding to commence stimulant therapy. The seven studies exploring this revealed that people often questioned the parents' judgment in starting their child on stimulant therapy and emphasized the negative effects of treatment as reflected in the media (Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Taylor et al. 2006; Jackson and Peters 2008; Brinkman et al. 2009; dosReis et al. 2010). In this way, parents were stigmatized, with claims that they were to blame for their child's condition and that they would give their child medication for convenience rather than deal with their child's behavior. Most of the stigma parents conveyed concern about however, regarded their child being labeled after commencing stimulant therapy (Charach et al. 2006; Taylor et al. 2006; Brinkman et al. 2009; dosReis et al. 2010) and the social isolation that might ensue as a consequence (Singh 2003).
Financial costs of treatment
Two studies examined the influence of financial costs of stimulant treatment on parental treatment decision making (Leslie et al. 2007; Fiks et al. 2011). Some parents from low-income families and/or those with limited or no health insurance coverage could not afford to pay for their child's medication (Leslie et al. 2007). Interestingly, even some parents with high incomes expressed that stimulant medications were too expensive and, in one instance, a mother decreased her children's dosages because of these costs (Fiks et al. 2011).
Experiences with the healthcare system
Parental treatment decision making was strongly influenced by the experiences of parents with various aspects of the healthcare system as explored in all 11 studies. Many parents mistrusted their child's medical evaluation and the advice of the responsible HCP. Often, parents' decisions were affected by poor interactions with HCPs in which there was a lack of information exchange or inadequate communication skills. Many parents first wanted to explore treatment options other than stimulant therapy, and the outcomes of these alternatives shaped parents' decisions to either commence or avoid stimulant therapy. The availability of support and information for parents within the healthcare system was another factor that influenced treatment decisions.
Alternative treatment options
At times, parents wanted to explore all avenues of treatment prior to commencing stimulants (Charach et al. 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters 2008; Brinkman et al. 2009). Parents appeared to adopt a “less or no harm” approach to medication by wanting to exhaust all non-medication options of treatment (Charach et al. 2006; Jackson and Peters 2008). Some enforced behavioral change techniques often in conjunction with counseling by a psychologist or assistance from an occupational therapist (Taylor et al. 2006; Leslie et al. 2007). Other parents tried herbal or “natural” remedies for the improvement of their child's ADHD symptoms (Taylor et al. 2006). If parents did not observe improvements with these remedies, it was often the case that only then would they consider stimulant therapy (Taylor et al. 2006; Brinkman et al. 2009). Also, in some cases, these herbal remedies were deemed to be too expensive by the parents and therefore difficult to sustain as a long-term treatment option (Taylor et al. 2006).
Mistrust of medical evaluation
For many parents, the medical evaluation procedures used by the diagnosing HCP were perceived to be inaccurate. In seven studies, parents disclosed that this gave them room to question the validity of the diagnosis made (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010). Commonly, parents expressed that HCPs were too quick to diagnose and medicate their child (Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Leslie et al. 2007; dosReis et al. 2010). Parents had an expectation that evaluations would be rigorous and thorough; however, through their personal experience, many were dissatisfied with the use of short questionnaires or checklist items to help determine whether their child required medication (Bussing and Gary 2001; Charach et al. 2006; dosReis et al. 2010). This reinforced the belief many parents had about the lax prescription practices of certain HCPs (Charach et al. 2006; Taylor et al. 2006). In turn, parents commonly displayed uncertainty about their child's diagnosis (Brinkman et al. 2009; dosReis et al. 2009).
Poor experience with a HCP
Parents' poor experiences with HCPs mostly surrounded issues with communication and problems with the nature of the dialogue between them (Taylor et al. 2006; Leslie et al. 2007; Brinkman et al. 2009). Some parents felt that the diagnosing HCP was reluctant to fully disclose information or engage in an informative discussion with them (Taylor et al. 2006; Brinkman et al. 2009). HCPs were also perceived to trivialize parental concerns, an approach that parents found to be disempowering (Taylor et al. 2006). In some instances, language barriers made communication difficult (Leslie et al. 2007), whereas in other instances, parents felt intimidated by the HCP and felt that they were not being listened to (Brinkman et al. 2009). These less than desirable interactions often left parents confused, and at times unwilling to comply with the recommendations of the HCP, as they felt their opinions had not been taken into consideration.
Lack of information and support
A desire for more information about stimulant medications was common among parents (Leslie et al. 2007). They expressed that information provided needed to be comprehensive and unbiased (Fiks et al. 2011). Parents also noted that they wanted HCPs to direct them to support groups with parents of children with ADHD, and that had experience with stimulant and other forms of treatment (Leslie et al. 2007).
Discussion
To our knowledge, this is the first systematic review of qualitative studies exploring the factors influencing parental decisions surrounding stimulant treatment in ADHD. Many parents of children with ADHD display hesitancy when a decision to commence or continue stimulant therapy for their child needs to be made (Bennet et al. 1996; McGuinness 2008). This is supported by the results of the 11 studies included in the review, which revealed that parental treatment decision-making processes are complex and influenced by a large number of factors. Despite contextual differences in the selected studies, examination and collation of their findings revealed topics that were common for parents across the different settings, supported by considerable overlap in their opinions and perspectives. Of all the factors explored in these studies, there were five factors that appeared to consistently impact upon parents' treatment decisions: 1) The impact of negative media and consequent stigma, 2) the influence of social networks, 3) the observation of (or fear of) side effects, 4) parental mistrust of medical evaluations, and 5) parents' ability to access relevant information and support.
Parents' exposure to negative media reports often deterred them from initiating or continuing stimulant treatment, with some raising concerns about the safety of these medications and others questioning parents' motives for wanting to medicate the child. The influence of the media on parents' treatment decisions cannot be taken lightly, with a study by Sciberras et al. (2010) revealing that 54% of parents relied on media reports as their primary source of ADHD-related information. These media influences increased the complexity of the treatment decision-making process for parents by raising doubts about the need for stimulant medication, and evoking concerns about side effects and also about how others perceived their parenting capabilities.
These attitudes were also apparent in parents' descriptions of the influence of their social networks. When seeking the advice from family and friends about the appropriateness of stimulant therapy for their child, parents were mostly met with a chorus of strong objections and reprimands about their parenting. This is supported by Peters and Jackson (2009) who revealed that there is a culture of parental blaming by friends and family members in situations involving children with ADHD, blame that is often specifically directed toward the mothers of affected children.
Closely linked with the aforementioned factors were parental perceptions of stigma associated with stimulant therapy. Parents were concerned about how others would view their parenting capabilities if they were to medicate their child, and importantly, how their child would be labeled as a consequence of taking medicine. These perceptions of stigma were observed to strongly influence parents' treatment decisions and are supported by the findings of Eiraldi et al. (2006), which highlighted that parents of children with ADHD concerned about stigma were less likely to seek healthcare services for their child.
Side effects of stimulant medications, whether anticipated or witnessed, also influenced parental decisions to initiate or continue therapy. Despite extensive research that has been done ensuring the safety of stimulant medications (Wolraich and Doffing 2004; Merkel 2010; Stiefel and Besag 2010), parents still have great concerns about potential side effects of stimulants prior to commencing treatment. Observed side effects after commencement of stimulant treatment often led to parents discontinuing treatment of their own accord, without first referring to the prescriber. The parental concerns surrounding medication side effects are in line with those side effects explored in the literature (Kaplan and Newcorn 2011). However, the results of the studies revealed that prior to treatment initiation, parents often did not have sufficient information about the likelihood of side effects occurring. In turn, some parents perceived the associated risks to be too high and avoided stimulant treatment altogether. It is also apparent that parents often terminate treatment independently as a result of not being given sufficient or adequate information from their HCPs.
Parents' treatment decisions were also influenced by their relationship with the diagnosing HCP and their personal assessments of medical evaluation and diagnostic procedures. Some parents perceived HCP evaluation procedures using certain checklists or questionnaires to be rushed, incomprehensive, and inadequate to justify their child's need for stimulant medication. This dissatisfaction made parents uncertain about their child's need for medication and about their ADHD diagnosis altogether (Charach et al. 2006; Taylor et al. 2006). This sentiment is supported by a number of sources in the literature that raise concerns about the rigor of the diagnostic criteria for ADHD and the potential for overdiagnosis and overprescribing as a consequence (Frances 2010; Morrow et al. 2012; Moynihan et al. 2012). Despite ongoing debate regarding this topic, the concerns held by parents about ADHD diagnosis are justifiable, and suggest that diagnostic procedures may need to be revised and strengthened.
The impacts of these parental perceptions are often worsened by poor experiences with the diagnosing HCP. Parents explain that these experiences are mostly confined to inadequate communication with the HCP, with some complaining that their HCP is unwilling to listen to their concerns, and others describing the approach of their HCP to be intimidating (Brinkman et al. 2009). These parental experiences are corroborated by studies in the literature that comment that communication between parents of ill children and some HCPs in the pediatric setting requires greater attention (Coulter and Koester 1985; Coulter et al. 1999).
Further, some parents note that HCPs often do not disclose enough information to address their concerns. Studies highlight that HCPs often do not deliver upon the information needs of parents, as they commonly underestimate parents' desire for information, have limited consultation times, and may lack the appropriate knowledge of a particular condition and its treatment (Coulter et al. 1999). In the studies examined, it was common for parents to express a desire for comprehensive, unbiased information about stimulant medications. Importantly, parents highlighted that they have limited avenues of support in the form of contact with other parents of children with ADHD, and wanted their HCP to direct them to such support groups (Leslie et al. 2007). Without access to such avenues of support and accurate information, parents cannot clear misconceptions they may have, or address their concerns regarding stimulant therapy, and may avoid treatment as a consequence.
Implications of the Review
There are several strategies that could be implemented to help address parents' concerns about initiating and continuing stimulant treatment for their children.
The impact of media reports and social networks, which have the potential to disseminate inaccurate information and reinforce misconceptions, could be alleviated by HCPs making particular effort to prompt parents to raise any concerns about information they may have come across elsewhere and to address these issues in a manner consistent with the parents' level of understanding.
More specifically, parental concerns surrounding side effects of stimulant treatment should be addressed in line with recommendations in current ADHD clinical practice guidelines (e.g., Canadian ADHD Resource Alliance [CADDRA] 2011; Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011; National Health and Medical Research Council [NHMRC] 2012). Parents who are yet to initiate stimulant treatment for their child and who express concern about anticipated side effects should be informed that different responses to medications are realistic and expected and that as a consequence, different individuals will have different risk/benefit profiles associated with medication use (CADDRA 2011). Parents should be reassured about the dose-dependent nature of potential side effects and guided through the initial medication titration process to ensure their cooperation in achieving optimal medication management (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011).
Parents should be informed that if the trial of one stimulant is not effective or causes concerning side effects, a trial of an alternative stimulant may lead to a positive response as witnessed in at least 50% of such cases (Greenhill et al. 1996). Parents should also be reassured that their child's progress will be monitored through regular follow-up visits, initially once a month and then once every 3 months once optimal response has been reached, where response to different doses of medication including adverse effects will be addressed (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). Duration of treatment could also be discussed with parents, emphasizing the intention that medications will only be continued in the instance of demonstrated benefits clearly outweighing any unacceptable adverse effects.
Parents' concerns about stigma surrounding ADHD and stimulant medications are perhaps more difficult to address. HCPs should acknowledge that a diagnosis of ADHD may be stigmatizing for some families, and this should be an important point of discussion between the HCP and the parent. There remains a strong need for a more holistic approach toward adequately addressing experiences of stigma associated with pediatric mental health issues in general, a notion which has been expressed in previous research (dosReis et al. 2010). A lack of understanding about ADHD and its treatments often forges stigmatizing attitudes among community members (dosReis et al. 2010). Therefore, the implementation of educational public health programs may help reduce stigma and the associated guilt that parents may experience, by disseminating accurate information about ADHD and dispelling common misconceptions.
Strengths and Limitations of the Review
This review highlights the broad range of factors influencing treatment decisions made by parents of children with ADHD with regard to stimulant therapy, allowing a much broader understanding of the topic compared with that provided by individual primary studies in isolation. A comprehensive search of the literature was conducted using predetermined criteria and the inclusion of peer-reviewed articles, to ensure selection of high-quality studies. By examining each study using a published framework for the assessment of qualitative studies' reporting comprehensiveness (Tong et al. 2007), the quality of the included studies was further ensured. The focus of the review on qualitative studies provided greater in-depth understanding of the topic by illustrating the parents' personal experiences. The emergent themes from the collective findings of the primary studies were sourced from the decision-making experiences of 335 participants, which, despite differences in context, showed significant overlap from the individual studies. Data extraction and theme development procedures used in this review were based on the approaches of previous “views-based” qualitative systematic reviews and guides (Harden et al. 2004; Gaston and Mitchell 2005; Parsons et al. 2007).
The authors recognize that much debate surrounds the appropriateness and value of qualitative reviews, particularly with relation to comparing the findings of studies conducted in different contexts and using different methodologies (Dixon-Woods and Fitzpatrick 2001; Dixon-Woods et al. 2001). However, some suggest that the significance of qualitative studies' findings is strengthened when they are brought together in a review (Parsons et al. 2007). The value of the information provided here is that it provides a broader perspective on the major issues affecting parents' decisions about stimulants.
The review was limited to the decision-making processes surrounding stimulant therapy, and, therefore, no conclusions can be made regarding the decision-making experiences in relation to other treatment avenues such as the use of non-stimulant medications or psychotherapy. The literacy level of most participants was difficult to ascertain; therefore, no comment can be made in relation to the impact of literacy level on the parents' decision-making processes.
Conclusions
This systematic review emphasizes that with regard to stimulant treatment for ADHD, parental treatment decision-making processes are complex and influenced by a variety of factors. These factors include negative media coverage, parental interactions with members of their social networks, concerns about side effects and stigma, mistrust of medical evaluations, and lack of medicine-related information. It is also apparent that the needs of parents of children with ADHD are often not being met in many instances. Future research needs to focus on ways to address parental concerns aroused by negative media coverage and influences of social networks. Strategies such as the implementation of educational public health programs targeting stigma surrounding ADHD require greater attention, along with development of methods to foster positive parent–HCP interactions and allow greater involvement of parents and children in their own care. Finally, comprehensive, reliable information about stimulant medications and greater access to support groups is required for parents to clarify any misunderstandings they may have and make the decision they deem to be in the best interests of their child.
Clinical Significance
The parents of children affected by ADHD often have difficulty accepting first line stimulant treatment for their children because of its negative portrayal in society. This systematic review provides a comprehensive exploration of the factors that influence parents' decisions toward stimulant medication use. This information can help clinicians identify and address areas of parental concern surrounding stimulant use. The findings may also assist clinicians in enhancing information delivery to parents of affected children and help reduce parental ambivalence surrounding stimulant medication use.
Footnotes
Disclosures
No competing financial interests exist.
Appendix A
The exact search strategy used for obtaining citations from the MEDLINE® database is listed below.
Appendix B
| Reporting criteria | Number (%) n=11 | Studies reporting each criterion |
|---|---|---|
| Research team characteristics | ||
| Facilitator or interviewer identified | 9 (82) | Bussing and Gary 2001; Singh 2003; Charach et al, 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Credentials identified | 9 (82) | Bussing and Gary 2001; Singh 2003; Charach et al, 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Occupation | 9 (82) | Bussing and Gary 2001; Singh 2003; Charach et al, 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011. |
| Gender | 7 (64) | Bussing and Gary 2001; Hansen and Hansen 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; |
| Experience and training | 7 (64) | Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009; Fiks et al. 2011; |
| Relationship with participants | ||
| Relationship established prior to study commencement | 3 (27) | Bussing and Gary 2001; Jackson and Peters, 2008; Brinkman et al. 2009 |
| Participant knowledge of interviewer | 8 (73) | Bussing and Gary 2001; Charach et al, 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011; |
| Theoretical framework | ||
| Methodological theory identified | 8 (73) | Singh 2003; Charach et al, 2006; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Participant selection | ||
| Sampling method | 9 (82) | Bussing and Gary 2001; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Method of approach | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011; |
| Sample size | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011; |
| Non-participation rates | 6 (55) | Brinkman et al. 2009; dosReis et al. 2009, 2010; Jackson and Peters, 2008; Leslie et al. 2007; Taylor et al. 2006 |
| Setting | ||
| Setting of data collection | 9 (82) | Brinkman et al. 2009; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; dosReis et al. 2009; dosReis et al. 2010; Fiks et al. 2011; |
| Presence of non-participants | 2 (18) | Bussing and Gary 2001; dosReis et al. 2009. |
| Description of sample | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Data collection | ||
| Interview guide | 7 (64) | Bussing and Gary 2001; Hansen and Hansen 2006; Leslie et al. 2007; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Repeat interviews | 2 (18) | Singh 2003; dosReis et al. 2009 |
| Audio or visual recording | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Field notes | 2 (18) | Singh 2003; Charach et al. 2006 |
| Duration | 8 (73) | Bussing and Gary 2001; Singh 2003; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; dosReis et al. 2009, 2010 |
| Data saturation | 5 (45) | Hansen and Hansen 2006; Taylor et al. 2006; Brinkman et al. 2009; dosReis et al. 2009, 2010 |
| Transcripts returned to participants | 1 (9) | Charach et al. 2006 |
| Data analysis | ||
| Number of data coders | 7 (64) | Bussing and Gary 2001; Hansen and Hansen 2006; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Description of the coding tree | 7 (64) | Bussing and Gary 2001; Charach et al. 2006; Taylor et al. 2006; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Derivation of themes | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006;Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Software used | 3 (27) | Bussing and Gary 2001; Leslie et al. 2007; Fiks et al. 2011 |
| Participant checking or feedback | 1 (9) | Charach et al. 2006 |
| Reporting | ||
| Participant quotations presented | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009; 2010; Fiks et al. 2011; |
| Data and findings consistent | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011; |
| Clarity of major themes | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. 2006; Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; Brinkman et al. 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |
| Clarity of minor themes | 11 (100) | Bussing and Gary 2001; Singh 2003; Charach et al. Hansen and Hansen 2006; Taylor et al. 2006; Leslie et al. 2007; Jackson and Peters, 2008; 2009; dosReis et al. 2009, 2010; Fiks et al. 2011 |