
Abstract
Objective:
The EudraVigilance Pharmacovigilance system classifies the seriousness of adverse drug reactions (ADRs) based on the requirement of hospital care. To date, no systematic study has been conducted on the impact of non-serious ADRs, in terms of therapy continuation and course of the underlying disease. We analyzed a pediatric population receiving psychiatric care and subjected to drug treatment, to assess whether non-serious ADRs do or do not have a relevant clinical impact.
Methods:
Data from a 1 year period were collected, which included: Administered drugs, choices made to manage the ADRs, the long-term (6 month) effect of these interventions on the course of the reaction, and their impact on the drug treatment for the underlying pathology.
Results:
Observed ADRs were concordant with those previously described for the same drug classes, and mainly comprised alterations of behavior, mood, and sleep (53%) and excessive variations of appetite and body weight (39%). The type of drug influenced the management decision, as we found that drug discontinuation was the most frequent strategy employed to resolve ADRs, especially with drugs employed in the treatment of attention-deficit/hyperactivity disorders (63%, p<0.05), whereas management of antipsychotics mainly relied upon drug substitution (21%, p<0.01). Also, the type of ADR influenced the management decision, as alterations of behavior, mood, and sleep were seldom managed by maintaining the drug unchanged (10%, p<0.05), at variance with appetite/weight alteration ADRs (unchanged in 41%, p<0.01). Follow-up information revealed that drug discontinuation was most efficient at treating ADRs (no persistent ADRs, p<0.01), but had a severe impact on the course of the underlying psychiatric disease. Conversely, management of ADRs by maintaining the original drug even if at different dosage did not lead to an amelioration of the reactions; however, as it caused a significant clinical improvement (83%, p<0.04) that superseded the ADR in terms of clinical benefit.
Conclusions:
These data suggest that the best strategy to improve both ADR management and the clinical course of patients is to limit, whenever possible, changes to the original therapy. Optimization of the actual therapeutic regimes also might benefit from development of specific pharmacokinetic and pharmacodynamic monitoring programs.
Introduction
Methods
The Scientific Institute E. Medea (Bosisio Parini, LC, Italy) focuses its clinical activity on paediatric psychiatry, and participates in the Monitoring Pediatrics Adverse Events [MEAP] pharmacovigilance project for the reporting of pediatric ADRs to the Italian National Pharmacovigilance Registry, which is part of the EudraVigilance system.
Sample characteristics and data source
A retrospective analysis was conducted on ADRs extracted from the Italian National Pharmacovigilance Registry, limited to reports made by the Scientific Institute E. Medea from March 2011 to March 2012. The considered ADRs met the following criteria: Patients were <18 years of age at the time of ADR occurrence; the referring physician indicated a psychiatric prescription as the suspected drug; and causality assessment of the ADR, applying the Naranjo algorithm, confirmed the drug–ADR relationship. Data collected for ADRs meeting the selection criteria were the following: Psychiatric diagnosis; drugs administered during the occurrence of the ADR and in particular the “suspect drug” (the drug considered responsible for eliciting the adverse reaction); dosage and duration of administration of all drugs; clinical management of the ADR; and reported outcome of the ADR at the time of reporting. Further data were collected from an internal database containing clinical details of each patient, in particular: A follow-up of the ADR, comprising therapy alterations and outcome; a clinical follow-up, including any further variation of drug therapy, which did not concern ADR management; and an evaluation of patient's health conditions in relation to the effectiveness of drug therapy. Data were considered for follow-ups after a minimum of 6 months from the occurrence of the original ADR. Where clinical or follow-up data were incomplete, the reaction or patient was excluded from the analysis. Numbers of ADRs or patients excluded are indicated in each table's legend. Collected non-serious ADRs were analyzed in terms of drug/drug classes involved, type of ADR elicited in relation to drug class, and ADR management with respect to drug class and ADR category. Patients' clinical data were analyzed to determine long-term therapeutic actions and outcomes, in terms of both ADR resolution and global clinical conditions. ADR follow-up outcomes were stratified according to the EudraVigilance system: Complete resolution, improvement, reaction not changed, or worsened. Clinical outcomes were categorized as: Significant improvement, minor improvement, unchanged, or worsened. Treatment groups were defined according to the administration of the therapy causing adverse reactions and of any other drug as follows. “Drug substitution” treatment group comprised patients who had discontinued the original medication and switched to a substitute drug; the group “Additional drugs” comprised those who kept the original therapy, adding further drugs; and the group “Drug not substituted” included patients who did not change their therapy, reduced drug dosage, or discontinued the drug for a short period, without assuming different drugs. Discontinuations were considered only if they had a causality link with an adverse reaction, thereby excluding all seasonal therapy suspensions (mostly regarding the treatment of attention-deficit/hyperactivity disorder [ADHD]). All clinical records were treated in conformity to the local ethics committee guidelines.
Statistical analysis
Categorical data contained in all contingency tables were analyzed by descriptive statistics. In view of the small sample size and of the presence of fields with an occurrence of zero, Fisher's exact test (one tailed) was applied, instead of the regular χ2 test, to determine which fields in the tables displayed non-normal distributions. One tailed tests were adopted, as the clinical actions were not randomized and not taken in a blinded manner, but under the expectation of an effect. p values <0.05 were considered significant.
Results
Psychiatric drugs and ADR type relationship
A total of 66 ADRs were reported to the National Pharmacovigilance Registry during the observational study period. Of these, 56 were classified as non-serious and involved 43 patients; 34 experienced one ADR, whereas 9 developed two or more unrelated events and in response to different drugs. During the same period, 221 patients under comparable pharmacological treatments did not develop any ADR. Figure 1 shows the drug classes involved. Details of patients, diseases, and relative drug treatment are shown in Table 1, which also reports the ADRs observed and their management (discussed subsequently). In order to allow interpretation of collected data, ADRs were arbitrarily categorized into three groups: alterations of behavior, mood, and sleep (i.e., asthenia, drowsiness, anxiety, nervousness, insomnia); excessive variations in weight and/or appetite (both positive and negative); and extrapyramidal symptoms. The principal ADRs observed fell within the categories of disturbances of behavior, mood, and sleep (53%); excessive variations in weight and appetite (39%); and extrapyramidal symptoms (14%). Twelve ADRs (21%) involved multiple symptoms. We analyzed the association between most common drug classes and ADR categories (Fig. 2). Reactions caused by antipsychotics mainly caused excessive body weight/appetite increases (43%), followed by alterations of behavior, mood, and sleep (36%) with a marginal prevalence of sedation over irritability and anxiety. Five patients experienced both weight increases and alterations of behavior, mood, and sleep. Drugs used for the treatment of ADHD led to reactions involving alterations of behavior, mood, and sleep (48%), with a predominance of irritability and hostility, and excessive weight/appetite decreases (38%), with five patients experiencing both types of ADR. Antidepressants mostly caused alterations of behavior, mood and sleep (64%), with an equal distribution among sedation and irritability. Phenothiazines were only reported to cause extrapyramidal symptoms, which have also been elicited in a minor number by antipsychotics (two cases from haloperidol and one from quetiapine). Additional symptoms not belonging to these categories were reported, although to a very low extent (amenorrhea 1.8%, proteinuria 1.8%, extrasystolic arrhythmia 1.8%, hyponatremia 1.8%, tachycardia 1.8%, diarrhea 1.8%, thyroid-stimulating hormone [TSH] elevation 1.8%).

Drug classes causing adverse reactions.
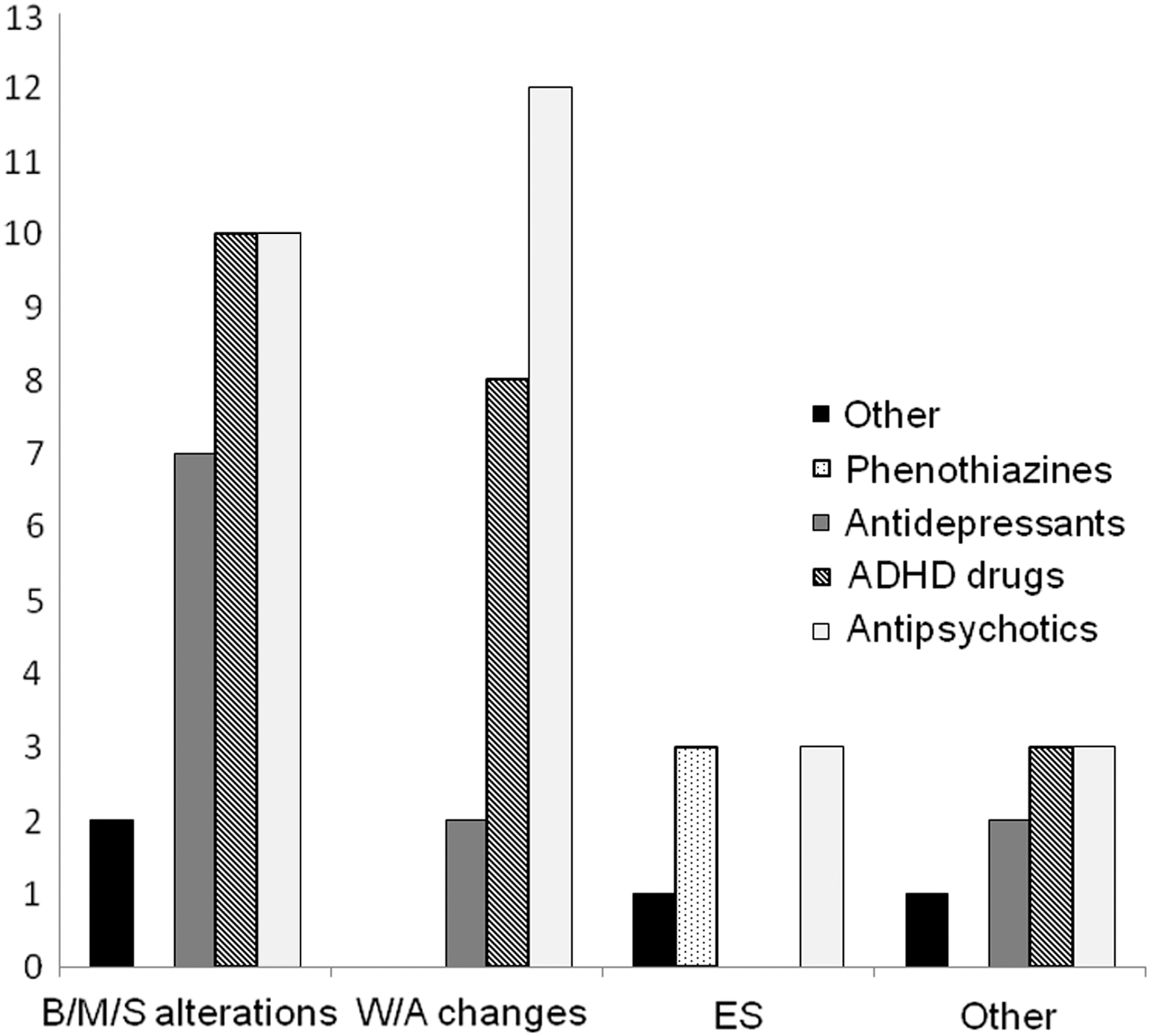
Association between most common drug classes and adverse drug reaction (ADR categories). B/M/S alterations: disturbances of behavior, mood and sleep; W/A changes: excessive variations in weight and appetite; ES: extrapyramidal symptoms.
ADR, adverse drug reaction; ADHD, attention-deficit/hyperactivity disorder; M, male; F, female; DD, drug discontinuation; DR, dosage reduction; DS, drug substitution; AD: additional drugs employed; None, no pharmacological alteration.
ADR management
In most cases, the development of non-serious ADRs led to drug withdrawal (Fig. 3). In 30 out of 56 collected ADRs, the treatment had to be discontinued, and it was replaced by an alternative therapeutic regimen in 5 cases. In 10 cases, a reduction of drug dosage (reduction of drug dosage or frequency of drug administration) was sufficient to resolve or improve the reaction. In the remaining 16 cases, changes in drug type/dosage were deemed not necessary. The management of ADRs in three cases required an add-on treatment, namely dietary supplements, levothyroxine, or valproate. Considering all drug classes, antipsychotics were those leading to the highest incidence of drug substitutions (21%, p<0.01), with ADHD drugs leading to the highest incidence of discontinuation (63%, p<0.05), as compared with the other drug classes. In terms of ADR type, alterations of mood, behavior, and sleep were the types of ADRs more often requiring drug discontinuation (59%), whereas dosage reduction (17%) and drug substitution (14%) were less frequently needed; with these ADRs the drug was maintained unchanged only in 10%, of cases (p<0.05), as compared with other ADR types. Within this group of ADRs, the highest rate of suspect drug discontinuation, as compared with other management choices, was observed with drugs used in ADHD treatment (80%, p<0.05), followed by antipsychotic drugs (61%) and antidepressants (57%) (Fig. 4). The ADR group comprising excessive variations in weight or appetite was the best managed as compared with other ADR types, with the highest rate of drug maintenance (41%, p<0.01), 55% of cases requiring drug substitution or discontinuation, and 4.5% (p<0.05) requiring dosage reduction. Within this group of ADRs, antipsychotics were characterized by the highest incidence of discontinuations and substitutions (67%), whereas ADHD drugs had almost the same rate of drug discontinuation and maintenance, and antidepressant therapies were never altered (Fig. 5).
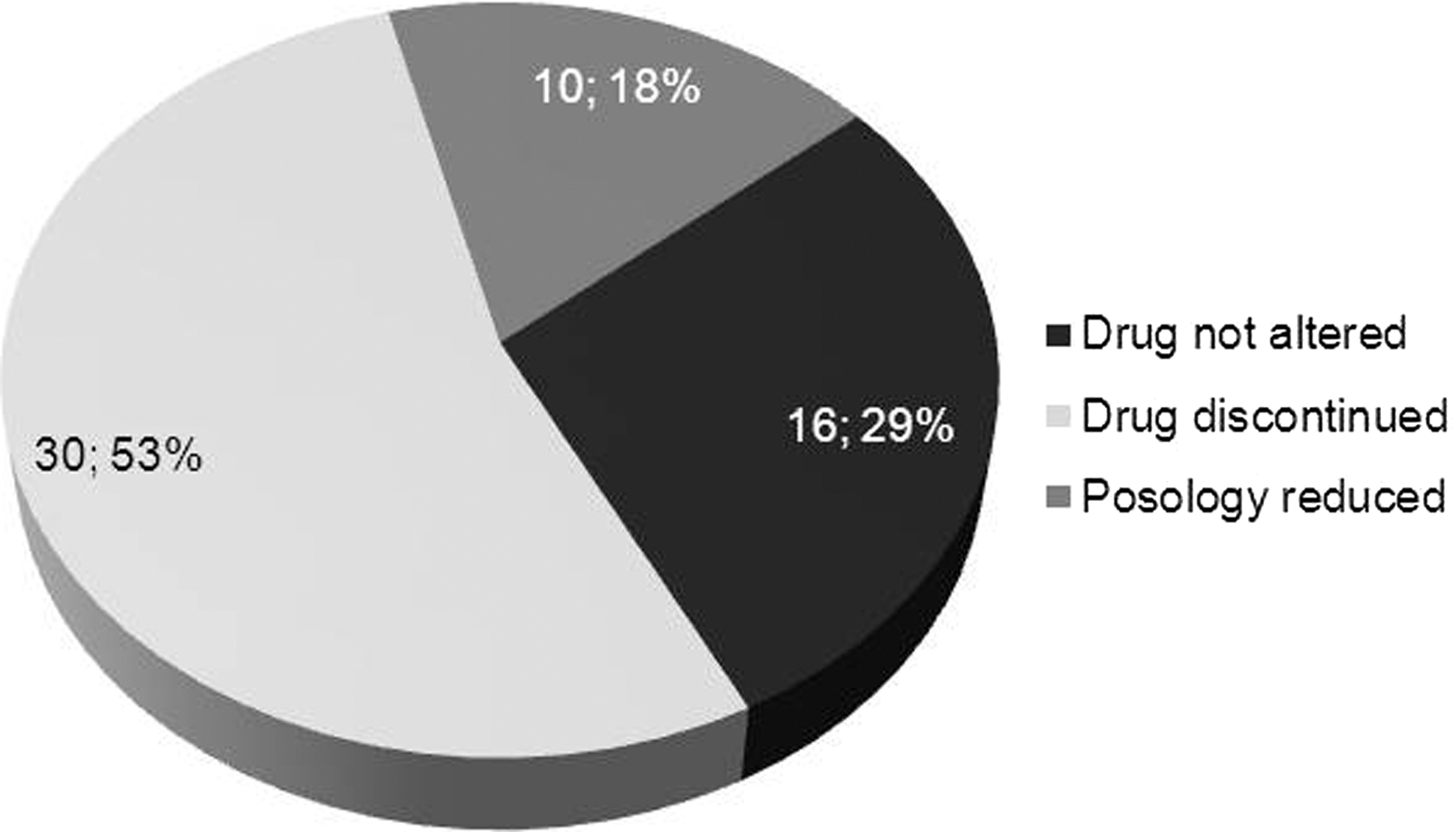
Adverse drug reaction (ADR) management, limited to the drugs that caused the adverse reactions.
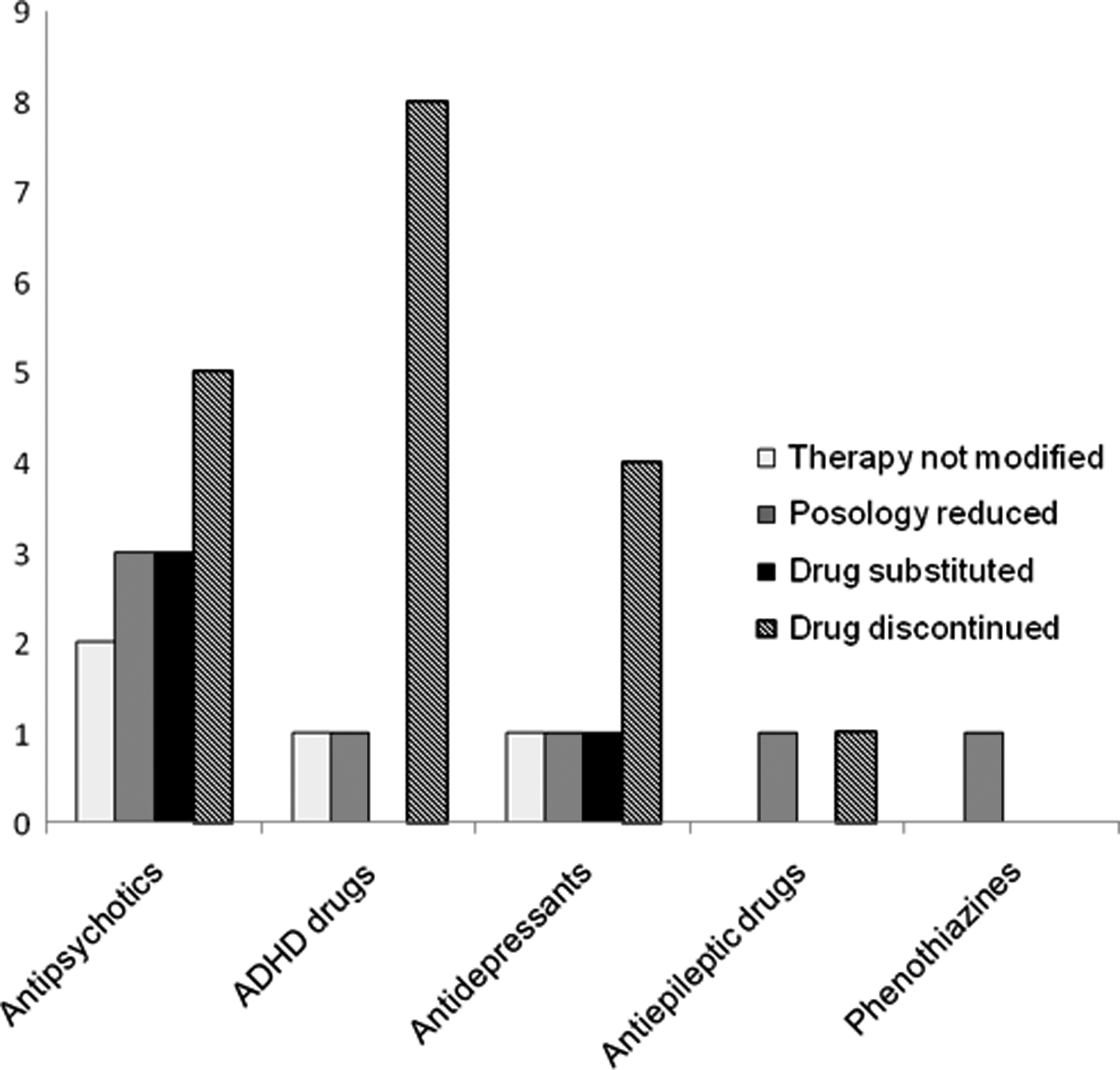
Suspect drugs and adverse drug reaction (ADR) management for the ADR category: Alterations of mood/behavior/sleep.
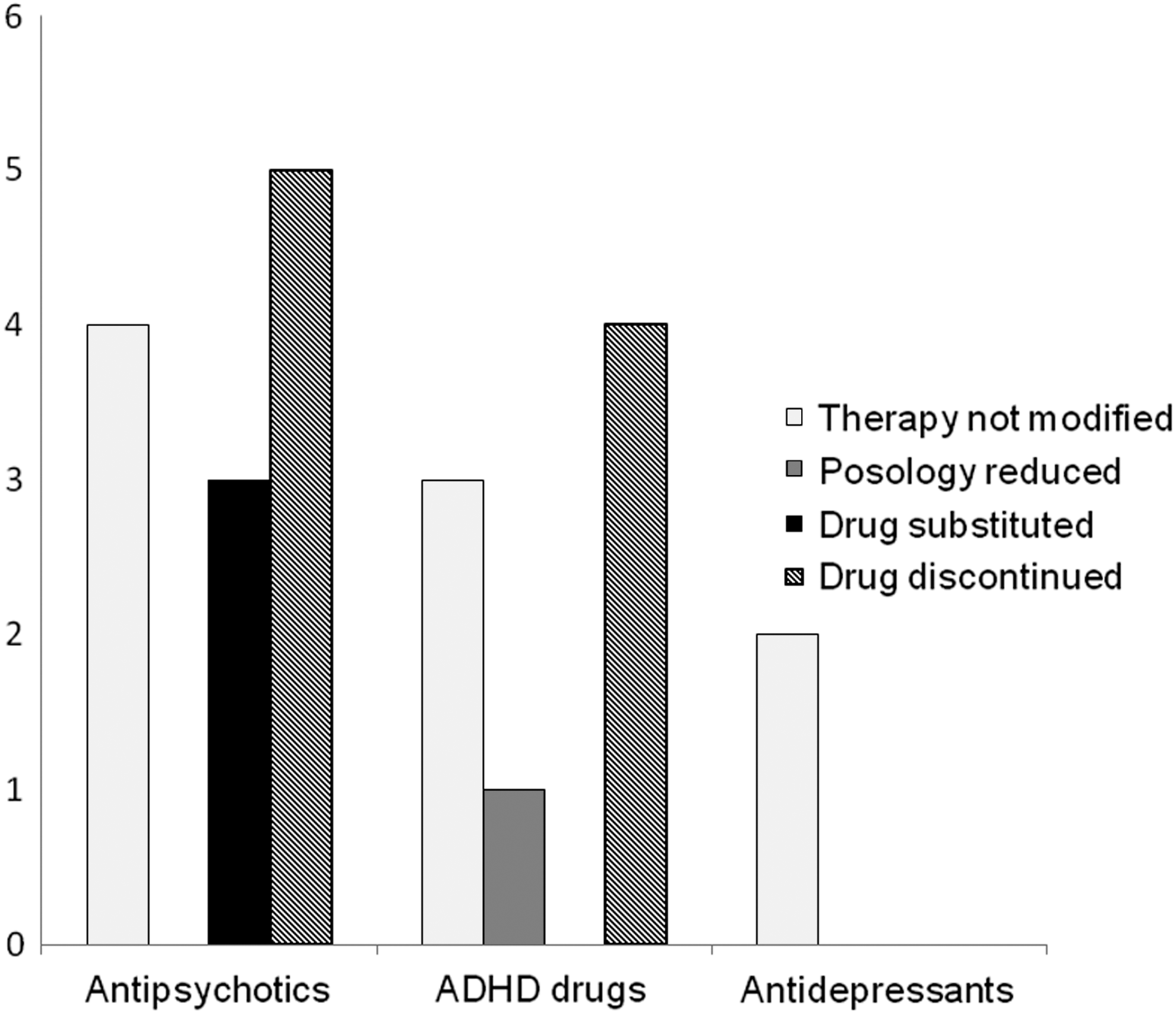
Suspect drugs and adverse drug reaction (ADR) management for the ADR category: Excessive variations in weight and/or appetite.
Long-term effects of ADR management
We examined the consequence of the way ADRs were managed long term (6 months). Evaluating the possible outcomes of the ADRs, continuation of drug therapy was associated with a worsening of the reaction (55%, p<0.01), whereas drug discontinuation never led to a persistence of the ADR (0%, p<0.01) (Table 2). Later changes of the patients' global drug therapy were also evaluated; among the patients who discontinued their suspect drug, most received a substitute drug (75%, p<0.01), or were re-administered the same drug (12%) or given an increased dosage of concomitant medications (12%), at variance with those who did not discontinue the suspect drug. Twelve patients (41%), whose reactions resolved without a drug discontinuation, were subjected to no therapy alterations also at the time of follow-up (p<0.01). Regarding the patients' clinical course, in patients who had their therapy discontinued because of ADRs and later received substitute drugs, the new drug did not improve the course of the disease. Instead, patients in whom the original drug was maintained, even at reduced dosage or with intermittent periods of suspension, showed a significant clinical improvement (83%, p<0.04) (Table 3).
For 7 ADRs no follow-up was available.
Numbers in brackets indicate persistent adverse drug reactions (ADRs). For 9 patients no clinical follow-up was available.
Discussion
Non-serious ADRs are seldom critically evaluated, and their potential impact on the maintenance of therapies and on patients' quality of life is currently unknown. In this study, we have investigated these two issues in a population of children and adolescents referred to the E. Medea Scientific Institute, in which an active program of pharmacovigilance on psychiatric drug monitoring has been established. Our results show that in a substantial number of cases non-serious ADRs led to ADR-related changes in drug dosage, drug type and/or drug discontinuation, or add-on therapies, because of ADR-induced health threats (mainly weight changes, metabolic alterations, or neurological and psychiatric disturbances), often impacting negatively on disease course. Whereas antipsychotic therapies were flexibly managed and drugs substituted, ADHD substitutive therapies often involved drastic drug class changes. Although the ADR categories here reported – alterations in behavior, mood, sleeping habits, metabolism, feeding habits, and weight, as well as hormonal alterations – are well-known occurrences in pediatric patients treated with psychiatric drugs (Aagaard and Hansen 2011; Vilhelmsson et al. 2011; Cohen et al. 2012), no studies addressed their impact on therapy outcome to date.
Particularly interesting among ADR treatment is the result of the management of behavioral and mood alterations. These ADRs may worsen the underlying psychiatric condition. The predominant clinical decision in this situation was to discontinue the suspect drug, or to reduce its dosage as a strategy to resolve these ADRs. Such choice was consciously preferred, even if leading to suboptimal therapeutic regimens for the original disease, in order to prevent the appearance of additional behavioral and neurological problems. Completely different was the management of weight and appetite disturbances, as almost half of these ADRs were managed while maintaining the original drug therapy. The reason for this choice was based on the assumption that the patients could be weaned off the therapy in time to avoid excessive worsening of the metabolic ADRs, which commonly arise after prolonged therapy courses and may have severe consequences (Hasnain et al. 2012). In addition, free light physical exercise was suggested by the physician as an additional measure to treat excessive body weight, although patients were mostly reported to be not compliant to it.
The follow-up confirmed that drug maintenance correlated with ADR persistence, whereas drug discontinuation did not. However, drug discontinuation impacted negatively on the therapeutic outcome, eliciting the need for different pharmacological treatments, which did not lead to clinical improvement of the underlying disease, either because of a reduced efficacy of the new treatment or the development of further ADRs. The evidence stemming from our analysis suggests that the development of new ADRs in cases of drug changes is a particularly relevant issue, as 21% of the patients developed more than one ADR. This contrasts significantly with the clinical cases in which ADR management was achieved by maintaining the original drug, with temporary suspension or changes in dosage. Therefore, it appears that maintenance of the original drug, whenever possible, has to be recommended, from a clinical perspective. A possibility, which was not investigated here, is to apply PK and PD analyses such that changes in drug therapy are prevented. In the literature, monitoring of PK and PD and clinical symptoms has been shown to be beneficial for disease amelioration in adults with serious ADRs, by optimizing the actual therapeutic regime (Rochon and Gurwitz 1995; Hiemke et al. 2011; Seto et al. 2011; Ostad et al. 2012).
Limitations
This study is relative to a small-sized sample, therefore statistical analyses may have suffered from limited power. Furthermore, the high number of patients who were reported not to experience any ADR in the study period suggests a high incidence of underreporting, most likely affecting the milder types of ADR. In addition, our patients comprised many children with autism spectrum disorders and ADHD, who may experience ADRs uncommon in other psychiatric conditions. An unavoidable limitation lies within the retrospective design, which may lead to causality issues; nevertheless, the involvement of several physicians has diminished the impact of custom and habits in determining the management choices for specific drug classes. Limited to ADRs regarding excessive body weight, the possibility of ADR resolution through physical exercise may represent a confounding factor, although its impact is likely minimized by the very low compliance of patients.
Conclusions
Data provided here indicate that in specific clinical settings, such as those described here, the real severity of an ADR is not fully accounted for by the current definition of ADR seriousness. Particularly striking are those situations in which drug substitution appears to be the only viable strategy to resolve the ADRs. The information stemming from this analysis has raised awareness about the issue of non-serious ADRs, their proper handling, and suggested appropriate intervention measures. This is crucial in the case of psychiatric issues, which may pose a serious problem of patient management, as they grow to adulthood, and may also generally translate into a reduction of costs for the healthcare system (Jerrell and McIntyre 2009).
Clinical Significance
We report that non-serious ADRs in psychiatry have a negative impact on therapy continuation, which results in serious consequences for the clinical outcome. We suggest that therapies should be managed in a conservative way, whenever possible. Further studies will be needed to clarify if such conservative measures can be complemented by PK and PD approaches, to improve the course of both ADRs and underlying pathologies.
Disclosures
No competing financial interests exist.