
Abstract
Background:
Autistic disorder is a neuropsychiatric syndrome characterized by deficits in social interaction; qualitative impairments in communication; and restricted, repetitive, and stereotyped patterns of behavior, interests, or activities. It is classified as a type of pervasive developmental disorder (PDD). All PDDs have a qualitative impairment in social relatedness. However, many individuals with PDDs have interfering symptoms, including irritability (aggression, self-injurious behavior, and severe tantrums). Behavioral therapy is often helpful in decreasing these behaviors; however, sometimes adjunctive medications are needed, because of the intensity and severity of irritability. Numerous medications have been tested on patients with PDDs. Although many of these medications have been demonstrated to be useful, no clear main treatment for PDD has emerged. Despite the efficacy of some of the medicines, acceptability and side effects have proven to be barriers to their use. Yokukansan (TJ-54), a traditional Japanese medicine, is composed of seven kinds of dried herbs. It is widely prescribed in clinical situations for treating psychiatric disorders by acting mainly on the glutamatergic and serotonergic nervous system. Recent studies indicate that TJ-54 may be safe and useful in treating behavioral and psychological symptoms in dementia patients. We aimed at evaluating both the efficacy and the safety of TJ-54 in patients with PDDs.
Methods:
This was a 12 week prospective, open-label investigation of TJ-54 in 20 children and adolescents ages 6–17 years diagnosed with PDDs. Primary outcome measures included the Clinical Global Impressions-Improvement of Illness Scale (CGI-I), Children's Global Assessment Score (CGAS), and the Aberrant Behavior Checklist (ABC) irritability subscale.
Results:
Twenty subjects, ages 6–17 years, received TJ-54 in the dosage range of 2.5–7.5 g/day. The CGI-I was significantly improved from 8 weeks (p<0.001). The mean CGAS was 31.92 at baseline, whereas the mean final score at 12 weeks was 54.52 (p<0.001). The ABC irritability/agitation subscale (subscale 1) was significantly improved from 8 weeks, and the hyperactivity/noncompliance subscale (subscale 4) was significantly improved in 12 weeks. TJ-54 was well tolerated. No subject left the study because of a drug-related adverse event.
Conclusions:
These preliminary data suggest that TJ-54 may be effective and well tolerated for the treatment of severe irritability/agitation and hyperactivity/noncompliance in children and adolescents ages 6–17 years with PDD. However, given the characteristics of this trial, the present findings should be taken cautiously, and larger-scale placebo-controlled studies are needed to elucidate the efficacy and tolerability of TJ-54 in this understudied population.
Introduction
Although there are no approved pharmacological treatments that target the core deficits of autistic disorder, associated secondary symptoms such as irritability may be ameliorated by a combination of behavioral and pharmacological approaches, including the use of atypical antipsychotics (Johnson and Myers 2007). Risperidone and aripiprazole are approved by the United States Food and Drug Administration for the treatment of pediatric patients with irritability associated with autistic disorder, including symptoms of aggression toward others, self-injuriousness, temper tantrums, and quickly changing moods. Different pervasive developmental disorder (PDD) symptom clusters may be responsive to a range of pharmacological agents.
Increasingly, atypical antipsychotics (e.g., risperidone, aripiprazole) are being used effectively in the treatment of tantrums and self-injurious behavior (SIB) (Canitano 2006; McDougle et al. 2008), but often they are accompanied by adverse effects (Aman et al. 2005; Posey et al. 2008). In a summary of randomized controlled trials (RCTs) of medications used to treat aggression and SIB, only three (risperidone, aripiprazole, and metylphenidate) were beneficial, suggesting there is room for further research and improvement (Findling et al., 1997; McDougle et al., 1997; Martin et al., 1999; Potenza et al., 1999; Masi et al., 2001; Barzman et al. 2004; Corson et al., 2004; Findling et al. 2004; Stigler et al., 2004; Aman et al. 2005; Hardan et al., 2005; Anderson et al. 2007). Moreover, these symptoms are reported to have been improved with micronutrient treatment (Mehl-Madrona et al. 2010; Adams 2011).
TJ-54 has been approved in Japan by the Ministry of Health, Labour and Welfare for the treatment of neurosis, insomnia, nighttime crying, emotional distress, and agitation in infants. TJ-54 was developed in 1555 by Xue Kai as a remedy for restlessness and agitation in children (Aizawa et al. 2002). Prompted by the increasing life expectancy of the Japanese population, geriatricians have begun to use this traditional regimen for behavioral and psychological symptoms of dementia (BPSD) in the elderly. For example, Iwasaki et al. reported two cases of BPSD in an extended care unit that were successfully treated with TJ-54 (Tahara et al. 2003; Iwasaki et al. 2005a). Iwasaki et al. reported that TJ-54 improved BPSD and activities of daily living in a randomized, observer-blind, control trial (Iwasaki et al. 2005b).
Basic research on the mechanism of action of TJ-54 has shown that TJ-54 suppresses abnormal hippocampal glutamate release in a zinc-deficient model (Takeda et al. 2008); it was also reported that TJ-54 activates the astrocytic glutamate transporter and shows a neuroprotective effect against glutamate-mediated excitotoxicity (Kawakami et al. 2009). Regarding the effect of TJ-54 on the serotonergic nervous system, it was reported that the compound acts as a partial agonist at the 5-HT1A receptor (Terawaki et al. 2008; Kanno et al. 2009) and shows a suppressive effect through downregulation of the 5-HT2A receptor (Egashira et al. 2008). It is known that Angelica root (one of the crude component drugs of TJ-54) binds to the GABA receptor (Liao et al. 1995). Cognitive dysfunction and BPSD in dementia patients are related to neurological dysfunction and neurodegeneration in the brain. In the postmortem brains of Alzheimer's disease patients, abnormalities were recognized in various nervous systems including the cholinergic, serotonergic, dopaminergic, glutamatergic, and GABAergic systems (Lanctot et al. 2001). According to the basic research conducted so far in order to clarify the mechanism underlying the amelioration of aggressiveness by TJ-54, it was reported to suppress the head-twitch response of mice induced by DOI (5-HT2A/5-HT2C receptor agonist), expression of 5-HT2A receptor in the prefrontal cortex of mice (Kanno et al. 2009), and glutamate-induced death of PC12 cells (Kawakami et al. 2009). Some of the component crude drugs were reported to activate the acetylcholine-mediated neurotransmitter system (Murakami et al. 2005), to bind to GABA, serotonin, and dopamine receptors (Liao et al. 1995) and to prevent N-methyl-
TJ-54 is effective for a number of symptoms associated with borderline personality disorder, including low mood, impulsivity, and aggression (Miyaoka et al. 2008a) and treatment-resistant schizophrenia (Miyaoka et al. 2009a), and neuroleptic-induced dyskinesia in patients with schizophrenia (Miyaoka et al. 2008b). In addition, this drug is sometimes used to treat visual hallucinations in vision loss or Charles Bonnet syndrome (Miyaoka et al. 2009b, 2011) and BPSD, which includes anxiety, in patients with dementia (Iwasaki et al. 2005a,b; Mizukami et al. 2009). Such detailed case observations and clinical trials of this traditional Japanese medicine suggest it as a new treatment for PDD in children and adolescents.
This study aimed to evaluate the effectiveness and tolerability of TJ-54 in children and adolescents with PDDs. Our hypothesis was that TJ-54 would be expected to improve irritability, and that a secondary outcome would be global functioning as measured by the Children's Global Assessment Score (CGAS). This study should be considered a pilot study preceding the development of a future randomized comparative study.
Methods
Materials
TJ-54 extract was provided by Tsumura & Co. (Tokyo, Japan). TJ-54 contains a mixture of dried herbs, 4 g of atractylodis lancease rhizome, 4 g of Poria, 3 g of cnidii rhizoma, 3 g of Angelicae radix (Angelica acutiloba), 2 g of radix bupleuri, 1.5 g of radix glycyrrhizae, and 3 g of uncariae uncis cum ramulus. These herbs are registered in the Pharmacopoeia of Japan version 15 (Mizukami et al. 2009). Similar active ingredients derived from the herbal medicines in extract powders have been confirmed to be contained by thin-layer chromatography analysis to be found in standard solutions for the herbal medicines. The developed plates were either examined by spraying with a 4-dimethylaminobenzaldehyde reagent or dilute sulfuric acid, or irradiated with ultraviolet light. Upon comparison with the standard solutions for the herbal medicines, one spot among the spots from the TJ-54 extract showed the same color tone and Rf value. In addition, the amounts of active ingredients such as glycyrrhizin, saikosaponin b2 and ferulic acid have been determined by high-performance liquid chromatography analysis, and stable contents have been secured. The chromatographic conditions for glycyrrhizin were: Column: A stain less steel column packed with octadecylsilanized silica gel for liquid chromatography Mobile phase: A mixture of H2O, CH3CN and CH3COOH Column temperature: A constant temperature of ∼40°C Flow rate: 1.2 mL/min Detector: An ultraviolet absorption photometer (wavelength: 254 nm)
The chromatographic conditions for saikosaponin b2 were: Column: A stainless steel column packed with octadecylsilanized silica gel for liquid chromatography Mobile phase: A mixture of H2O, MeOH and CH3CN Column temperature: A constant temperature of ∼50°C Flow rate: 1.0 mL/min Detector: An ultraviolet absorption photometer (wavelength: 254 nm)
The chromatographic conditions for ferulic acid were: Column: A stainless steel column packed with octylsilanized silica gel for liquid chromatography Mobile phase: A mixture of H2O, CH3CN and (HCOO)2
Column temperature: A constant temperature of ∼25°C Flow rate: 1.2 mL/min Detector: An ultraviolet absorption photometer (wavelength: 320 nm)
Strict manufacturing processes and quality controls have satisfied good manufacturing practices standards. TJ-54 has been approved by the Ministry of Health, Labour and Welfare as a prescription covered under the National Health Insurance plan. The compounds shown on the chromatogram were classified on the basis of the constituent herbs of TJ-54 (Table 1) (Nagata et al. 2012).
Study design and subjects
Subjects were recruited after a preliminary psychiatric interview and further assessment at the Outpatient Community Mental Health Unit of Shimane University School of Medicine, Izumo, Japan. Subject inclusion criteria were: Age 6–17 years; a diagnosis of PDD according to a semistructured clinical interview (the Autism Diagnostic Observation Schedule [ADOS]/the Autism Diagnostic Interview-Revised [ADI-R]) for DSM-IV criteria; and had no other psychiatric disorders per Kiddie-Schedule for Affective Disorders and Schizophrenia (K-SADS). Patients were excluded if they had any major medical or neurological illness assessed by a questionnaire conducted by their pediatrician.
Demographic and clinical characteristics of the sample are listed in Table 2. This study was approved according to institutional guidelines and recommendations of the Declaration of Helsinki by the Helsinki Committee (Institutional Review Board) of the Department of Psychiatry of the Shimane University School of Medicine. Institutional review board/independent ethics committee approval was received at each site prior to study initiation. All parents/guardians provided written informed consent to participate, and subjects provided written, informed assent when possible.
PDD, penasive developmental disorder; 1Q, intelligence quotient.
Participants
Twenty children and adolescents 6–17 years of age were enrolled. Written informed consent was obtained from the participant's legal guardian, and subjects provided assent when able. Diagnoses of PDD using criteria of the DSM-IV-TR (American Psychiatric Association 2000) were made by a board-certified child and adolescent psychiatrist experienced in the assessment and diagnosis of PDDs. Subjects were required to have a mental age of at least 18 months as determined by the Wechsler Intelligence Scale (WISC-III: Wechsler 1999). Additional inclusion criteria included a Clinical Global Impressions-Severity (CGI-S) scale (Guy 1976) score of at least 4 (“moderately iII”) focused specifically on target symptoms of irritability (aggression, self-injury, tantrums) and a score >17 on the Aberrant Behavior Checklist (ABC) irritability subscale (Aman et al. 1985; Aman and Singh 1994). The CGAS can range from 1, which is the very worst, to 100, which is the very best. Subjects with a DSM-IV-TR diagnosis of other primary psychiatric disorder, active seizure disorder, or significant medical condition were excluded. Nonpharmacological therapy (e.g., psychotherapy and behavior modification) was permitted provided it was stable before screening and consistent throughout the study.
Study design
A 12 week prospective, open-label study design was chosen to gather pilot data on the effects of TJ-54 on children and adolescents with PDD in anticipation of larger-scale, double-blind, placebo-controlled studies of this population. The study duration allowed for gradual titration as well as a 4 week maintenance phase. All subjects underwent a screening and baseline visit. Follow-up visits occurred every 2 weeks during the 12 week open-label trial period.
Dosage
All subjects initially received 2.5 g/day of TJ-54 for 3 days. The dosage was then increased to 5.0 g/day and continued to the end of week 2. The investigators then increased the dosage to a maximum of 7.5 g/day over the next 4 weeks if optimal clinical response had not occurred and intolerable adverse effects had not emerged. The dosage maintenance phase lasted 8 weeks at the optimal dosage.
Primary outcome measures
The primary outcome measures were the Clinical Global Impressions-Improvement (CGI-I), CGAS, and ABC irritability subscale. The CGI-I is a scale designed to assess how much the patient's illness has improved or worsened relative to a baseline state at the beginning of the intervention. In this study, the rater scored the CGI-I with regard to improvement of irritability, including aggression, self-injury, and tantrums. The CGI-I rates subjects from 1 to 7 (1=very much improved; 2=much improved; 3=minimally improved; 4=no change; 5=minimally worse, 6=much worse; and 7=very much worse). The CGAS range from 1, which is the very worst, to 100, which is the very best. The CGAS can be a useful measure of overall severity of disturbance, and it was provided to assist in the process of rating the clinical severity of all the young people. Moreover, it demonstrated both discriminant and concurrent validity. The ABC was used as a primary outcome measure in the aforementioned studies by the Research Units on Pediatric Psychopharmacology (RUPP) Autism Network (2002, 2005) and by Shea and colleagues (2004). The ABC is a 58 item checklist that measures six areas of behavior: Irritability, lethargy/withdrawal, stereotyped behavior, hyperactivity, and inappropriate speech (Aman et al. 1985; Brown et al. 2002) and gives a total composite that has confirmed reliability and validity in regard to the factor structure, distribution of scores, and sensitivity to change. The irritability subscale consists of 15 items on temper tantrums, aggression, mood swings, irritability, property destruction, and self-injury. The CGI-I and ABC were administered at every visit after baseline. The CGAS was administered at baseline and 12 weeks. Behavioral symptoms were assessed by multiple raters (parents, teachers, and/or other caregivers) and averaged. Because follow-up was variable, the intraclass correlation coefficient (Bartko and Carpenter 1976) for total scores, based on 12 randomly selected ratings, was 0.81 (p<0.001) for the ABC and 0.83 for the CGI-I.
Safety assessment and monitoring
Medical and disease history, physical examination, body weight, blood pressure, and electrocardiograms were assessed at baseline. Laboratory studies included a baseline screening for liver disease, metabolic dysfunction (i.e., glycemia, cholesterol, triglycerides), kidney disease, electrolyte imbalance, anemia, adequate blood cell and platelet counts, and prolactin levels. At each visit, a medical-psychiatric-neurological review was conducted, together with an assessment of body weight and a review of adverse events and concomitant medications. The potential adverse effects common to TJ-54 are sleepiness, impatience, spasticity, edema, nausea, and hypokalemia (Hayashi et al. 2010). The above laboratory studies were reassessed at week 12. Adverse effects were systematically reviewed at each clinic visit by the investigators. In addition, the Side Effects Review Form, a listing of potential adverse effects common to TJ-54, was completed.
Statistical analysis
All data were expressed as means±SD. A paired t test was used to compare the differences between the means of CGI-I and ABC subscores before and after treatment. Fisher's exact test was used to examine the difference in the proportion of side effects before and after treatment. The statistically significant difference was set at p<0.05. Statistical analysis of data was performed using SPSS Text Analysis for Surveys 4.0.1.
Results
All participants were Japanese. The sample consisted of 12 males and 8 females, ages 6–17 years (mean 11.65±3.08 years), consistent with the higher male-to-female ratio observed in PDDs. Thirteen subjects were diagnosed with PDD-not otherwise specified (NOS), five subjects were diagnosed with Asperger's disorder (AD), and two subjects were diagnosed with autism. Full-scale intelligence quotient (IQ) scores by WISC-III ranged from 70 to 110, with a mean score of 88.9±13.2. Subjects received a mean final TJ-54 dosage of 5.21±1.30 mg/day (2.5–7.5 g/day). All subjects, including all children, were verbal, and completed the study.
Treatment response
Eighteen (90%) of 20 subjects were considered responders, as determined by a CGI-I score of 1 or 2 and a >25% improvement on the ABC irritability subscale. All subjects were improved by CGAS. All seven subjects diagnosed with AD and autism responded to treatment, whereas 11 of 13 (84.6%) subjects with PDD-NOS responded. The mean CGI-I score at end-point was 1.80±0.56, with 18 (90%) of 20 subjects rated as much or very much improved in regards to interfering target symptoms of irritability (aggression, self-injury, tantrums) (p<0.001) (Fig. 1 and Table 3). CGAS ranged from 29 to 36 (mean 31.92±2.26) at baseline, whereas the mean final score at 12 weeks was 54.52±3.18 (p<0.001) (Fig. 1). ABC Irritability subscales ranged from 18 to 36 (mean score 27.00±7.01) at baseline, whereas scores at week 12 ranged from 10 to 24 (mean score, 17.60±4.83) (p<0.001) (Fig. 2 and Table 3). ABC hyperactivity subscales ranged from 14 to 42 (mean score 25.00±7.12) at baseline, whereas scores at week 12 ranged from 8 to 28 (mean score, 16.80±7.23) (p<0.05) (Fig. 3 and Table 3). There is no difference with age and sex in clinical features, effect of TJ-54, or side effects.
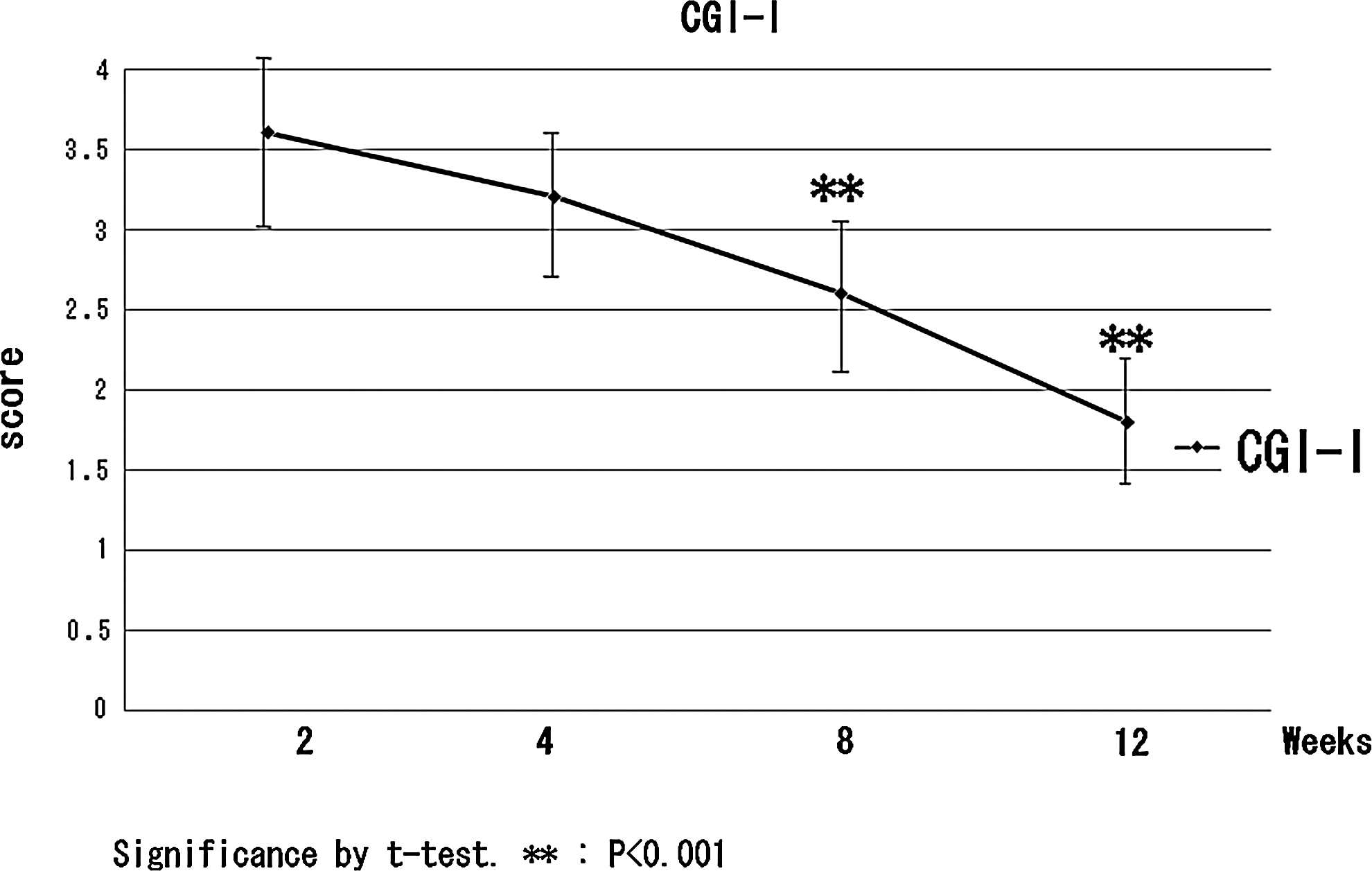
Clinical Global Impressions-Improvement.
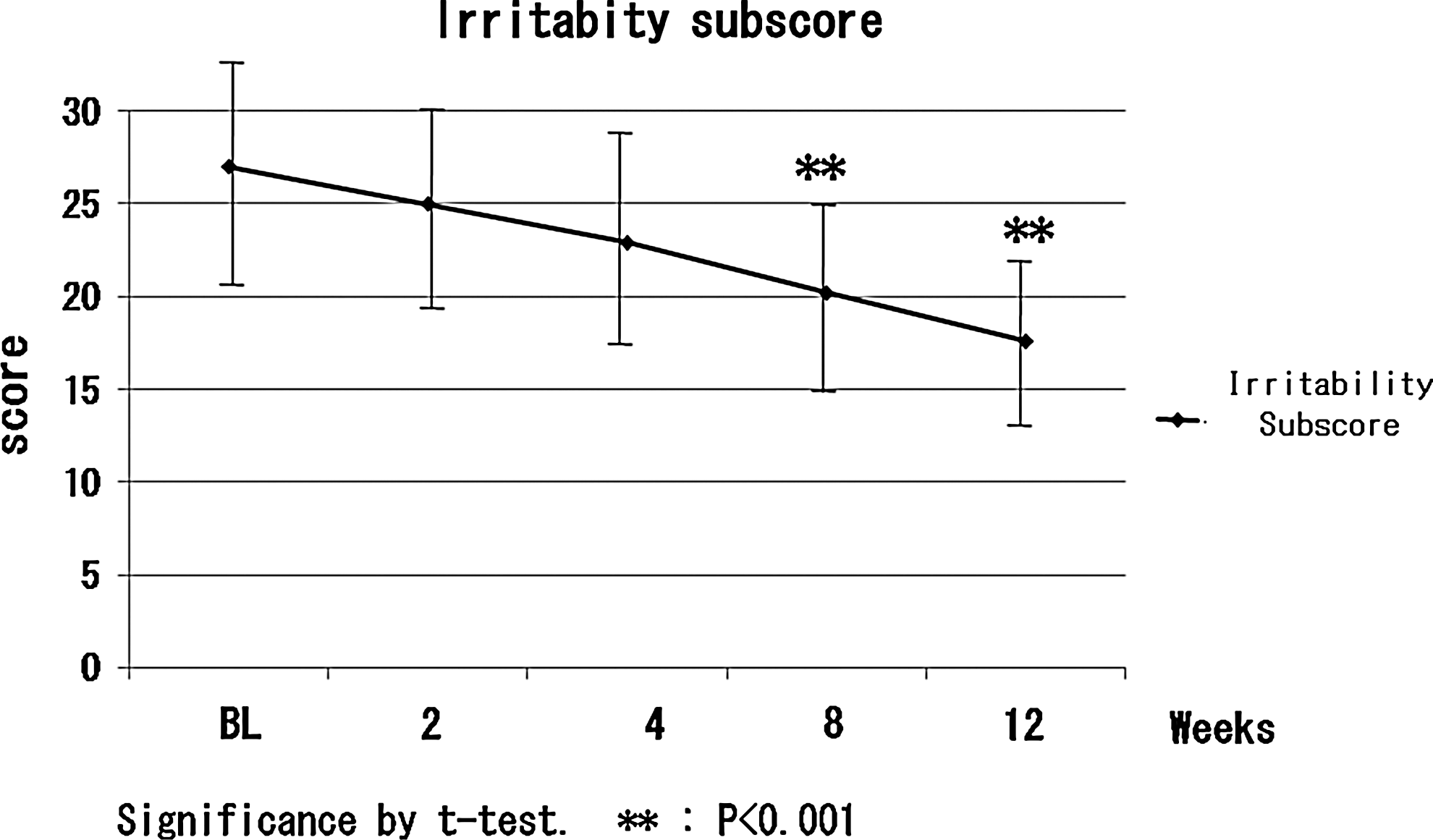
Irritability subscore.
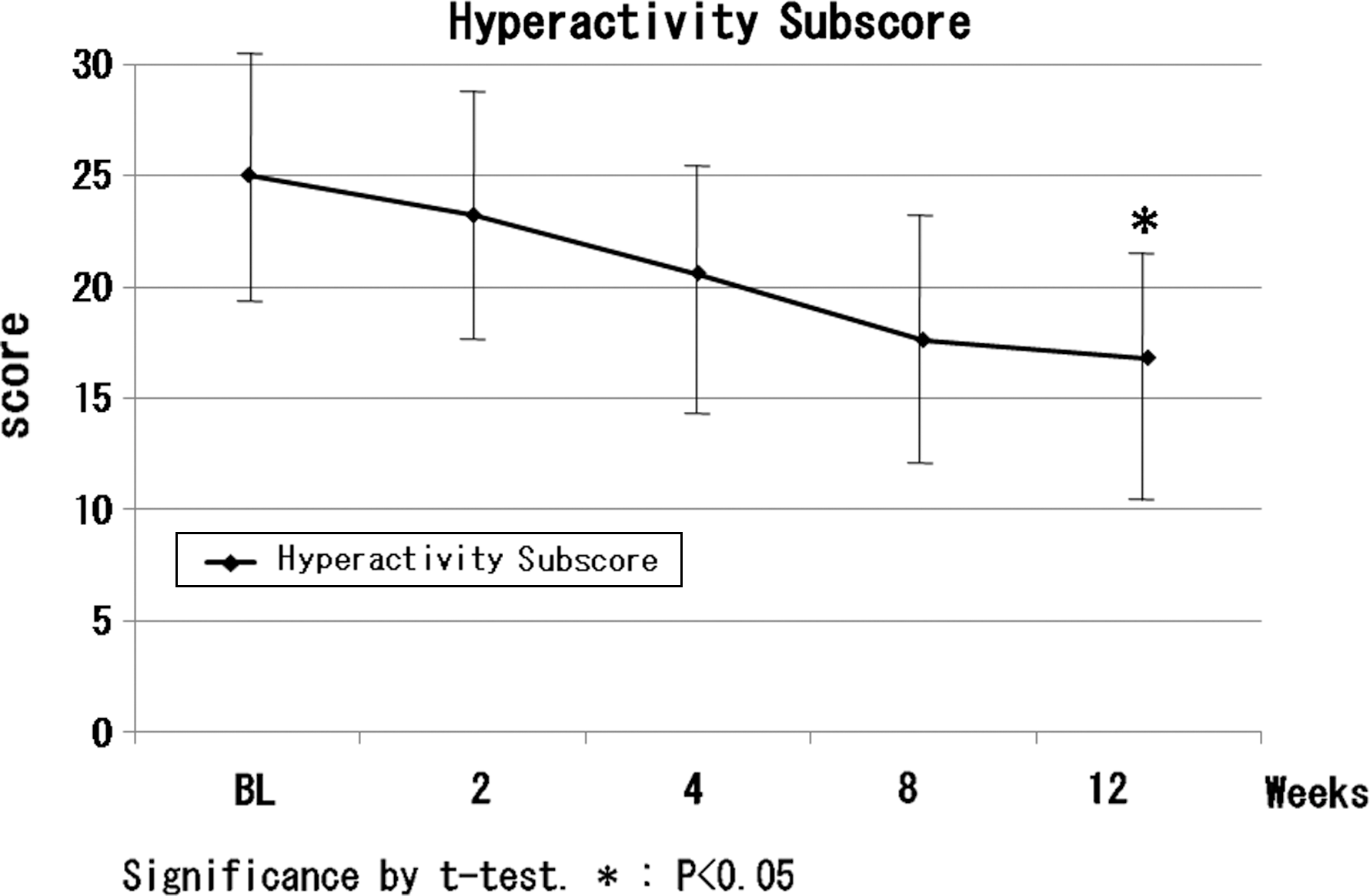
Hyperactivity subscore.
Significance by t test. * p<0.05, ** p<0.001.
Negative values indicate a positive change.
CGI-S, Clinical Global Impressions-Severity; CGI-I, Clinical Global Impressions-Improvement; CGAS, Children's Global Assessment Score; ABC, Aberrant Behavior Checklist.
Safety measures and adverse effects
Laboratory parameters were within the normal range at baseline and remained in the reference range for the whole sample throughout the 12 week trial. There were no reports of serious adverse effects attributable to the study drug. Mild and transient adverse effects were observed in two cases (drowsiness). There were no significant changes from baseline to 12 weeks. TJ-54 was well tolerated overall, with no severe or serious adverse effects recorded during the study. None of the adverse effects was treatment limiting. No subject exited the study because of a drug-related adverse event.
Discussion
The results of this 12-week prospective, open-label study suggest that TJ-54 may be effective for treatment of irritability and hyperactivity, and may be well tolerated for targeting by children and adolescents with PDDs. Although the drug may also be effective in patients with PDDs, our small sample size limits interpretation of data in this PDD.
Treatment with TJ-54 at dosages from 2.5 to 7.5 g/day resulted in significant amelioration of irritability, including aggression, self-injury, tantrums, lethargy, stereotypy, hyperactivity, and inappropriate speech. In light of research suggesting that a disregulation of DA and 5-HT contributes to maladaptive behavior in PDDs (McDougle et al. 2005), TJ-54's unique mechanism of action as a partial D2 agonist, 5-HT1A agonist, and 5-HT2A antagonist (Miyaoka et al. 2009b), may prove important for both its effectiveness and tolerability in PDDs.
Although this is highly speculative, these positive changes in irritability may be the result of TJ-54's mechanism of action as a partial 5-HT1A agonist and suppressor of the glutamatergic system (Miyaoka et al. 2009b). A putative association has been hypothesized between partial agonism at 5-HT1A receptors and improvements in anxiety and depression, as well as the negative symptoms of schizophrenia (Miyaoka et al. 2009b). Moreover, suppression of the glutamatergic system may improve brain excitement and protect neurons. Therefore, it is possible that TJ-54 targets these symptoms, thereby potentially resulting in subjects' increased ability and/or interest in interacting with others. It also may be that by decreasing irritability and hyperactivity, the children and adolescents were better able to improve their social functioning over time. Although the fact that, for all measures but the CGI, the scores were still high after treatment, may show milder action than atypical antipsychotics. Overall, TJ-54 was well tolerated, with no severe or serious adverse effects associated with the drug. Although no major side effects were seen in this short trial, this does not mean that some as yet to be determined side effects might not appear after long-term use.
This study has several limitations that could potentially impact the reliability and validity of these findings. Because of its open-label design, bias as well as a placebo effect could be factors in our findings of improvement in irritability as well as socialization. The results of the additional evaluation of the effects of TJ-54 have to be taken with caution, as the placebo effect can be significant. In this study, diagnoses were made by child and adolescent psychiatrists and pediatricians experienced in the diagnosis of PDDs using DSM-IV-TR criteria. We examined if there were potential medical comorbidities that could cause pain and discomfort to be ruled out as a potential cause of the irritability. Although the physical inspection of patients was performed by the pediatrician, gastrointestinal disorders are frequent in this population and do not typically present with symptoms easily recognized. As TJ-54 has not been reported to improve alimentary symptoms, this improvement of irritability would suggest that the action by TJ-54 is through the central nervous system. As to limitations, the number of subjects in this study was relatively small and the duration of this study was relatively short. These interventions by nonpharmacologic therapy might have impacted the results of this study. In addition, the absence of a control group limits the conclusions that can be definitively drawn regarding the safety and tolerability of TJ-54 in this population, and our findings may not apply to all autism spectrum disorder (ASD)/PDD children and adolescents. Finally, although these analyses can provide very preliminary data in the short term, a much larger double-blind, crossover, placebo-controlled study over a longer period of time is needed in order to more fully understand the efficacy, safety, and tolerability profile of TJ-54.
Despite these inherent limitations, the preliminary results of this study suggest that TJ-54 has the potential to be an effective and well-tolerated treatment for severe irritability in pediatric patients with PDDs. In addition, the improvement in irritability observed with TJ-54 treatment is intriguing, and deserves further study. Taken together, these favorable initial findings are of particular clinical relevance given the high prevalence of children and adolescents diagnosed with PDDs. PDD-NOS is the most common subtype of PDD and warrants more formal investigation, given the impairment it bestows upon those who have it (Fombonne 2005; Towbin 2005). Controlled research and longitudinal studies are needed to further determine the efficacy and tolerability of TJ-54 for the treatment of irritability in these greatly understudied PDDs.
Conclusions
Although at present TJ-54 has not been proved as a formal clinical treatment, this study has produced data to suggest that TJ-54 may be suitable for reducing irritability and hyperactivity in children with PDDs. However, monitoring blood counts in patients receiving TJ-54 seems to be justified. The present data need to be confirmed in larger, randomized, longer-term trials
Clinical Significance
In the clinic, physicians should consider the patient's treatment history, including previous response to medications and preferences, when choosing treatment strategies for PDD. The data analyzed in this study suggest that TJ-54 may be effective and well tolerated for the treatment of those patients with PDD who have irritability and hyperactivity. However, because TJ-54 has not been assessed in randomized, controlled, long-term clinical trials, special care and close monitoring are required with TJ-54.
Footnotes
Disclosures
No competing financial interests exist.