
Abstract
Objective:
The purpose of this study was to determine if tetrahydrobiopterin (BH4) reduced core symptoms of autism spectrum disorder (ASD).
Method:
In this study, 46 children, 3–7 years of age diagnosed with an ASD were randomly assigned to double-blind treatment with 20 mg/kg/day BH4 or placebo for 16 weeks. The primary outcome measure was the Clinical Global Impressions Improvement and Severity Scales (CGI-I and CGI-S); secondary outcomes were the Preschool Language Scale-4 (PLS-4), Social Responsiveness Scale (SRS), Aberrant Behavior Checklist (ABC), and Vineland Adaptive Behavior Scales (Vineland).
Results:
Overall, no differences were found on global improvement as measured with the CGI-I or CGI-S. Secondary measures indicated significant improvements for BH4 relative to placebo with regard to social awareness, autism mannerisms, hyperactivity, and inappropriate speech. Side effects were minimal and similar between both active medication and placebo.
Conclusions:
These results indicate that BH4 offers promise in reducing symptoms of ASD.
Introduction
Tetrahydrobiopterin (BH4) has shown promise in improving some of the core symptoms of autism. BH4 is a naturally occurring substance that serves as an essential cofactor for several metabolic pathways, including those responsible for the production of monoamine neurotransmitters, the breakdown of phenylalanine, and the production of nitric oxide. Abnormalities in several of these pathways have been implicated in autism spectrum disorder (ASD) (Frye et al. 2010), and reduced central nervous system (CNS) concentrations of BH4 have been reported in individuals with ASD (Frye et al. 2010).
Studies examining the effectiveness of BH4 in individuals with ASD started in the mid 1980s in Japan. Overall, 41–64% of subjects receiving 1–3 mg/kg per day of BH4 over 4–24 weeks showed a moderate or larger improvement in symptoms of autism as measured by the Rating Scale for Abnormal Behavior in Children (Naruse et al. 1987, 1989; Nakane et al. 1990; Naruse et al. 1990). However, all but one of these studies was open label. More recently, Danfors et al. (2005), conducted a double-blind, placebo-controlled crossover study of a group of children with ASD between the ages of 3 and 7 years who had low BH4 concentrations in their cerebrospinal fluid (CSF) (Danfors et al. 2005). Twelve children participated in the study, which consisted of 6 months of one treatment of either 6 mg/kg/day of BH4 or placebo, followed by 6 months of the other. There was a borderline significant correlation between CSF BH4 concentration before treatment and improvement in social interactions on the Childhood Autism Rating Scale (CARS) with BH4 treatment.
Although the clinical trials performed to date suggest that BH4 may ameliorate some of the core symptoms of an ASD, the findings have limitations. Most of the studies are open label, leading to inherent biases. Only two double-blind, placebo-controlled studies have thus far been conducted, and one was limited in sample size (Danfors et al. 2005). Larger, double-blind, placebo-controlled studies are, therefore, needed to assess efficacy.
This proof-of-concept study was designed to test the whether BH4 can improve core symptoms of ASD over a 16 week period. We utilized a placebo-controlled design, randomly assigning participants to either the BH4 (active medication) or placebo. Primary outcome measures were the Clinical Global Impressions Improvement and Severity scale scores, but we also used secondary measures to assess core features of an ASD relating to social skills, language, and restricted and repetitive behaviors.
Method
Design overview
This study was a prospective 16 week double-blind randomized outpatient medication treatment trial of tetrahydrobiopterin dihydrochloride (BH4) versus placebo (resembling a tetrahydrobiopterin tablet) for autism core and associated symptoms in young children with ASD. This study was approved by the Western Institutional Review Board (Olympia, Washington); we also had a Data and Safety Management Board that monitored side effects throughout the study.
Sample
Study participants were recruited from patients of Children's Health Council (CHC) clinicians, local advertisements, radio advertisements, e-mail news blasts, and flyers posted in various autism treatment centers around the greater San Francisco Bay Area. All child participants had to meet American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) diagnostic criteria for an ASD (American Psychiatric Association 2000). Diagnoses were made with the Autism Diagnostic Inventory – Revised (ADI-R; Lord et al. 1994), the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2000), and clinical agreement by two expert clinicians. Other enrollment criteria included being at least 3 but less than 7 years of age at the start of the study, having a developmental quotient >50 as assessed with the Vineland Adaptive Behavior Scale, 2nd Edition (Vineland-2), Interview Edition, Survey Form (Sparrow et al. 2005), and not having taken any psychoactive medications other than supplements, anticonvulsants, melatonin, or diphenhydramine for sleep or seizures within the 6 months prior to enrolling in the study. Further, parents had to agree to not start or change any treatments over the duration of the study period.
The aim and procedures of the study were fully explained to the families before written consent was obtained. To achieve 90% power to detect a significant group difference in the primary outcome measure, the Clinical Global Impressions – Improvement (CGI-I), using a p value of 0.05, we a priori calculated that a minimal sample size of 28 participants was needed per group. Of the 107 subjects who showed initial interest in participating, 46 did not meet inclusion criteria or were unwilling to give final consent. The remaining participants (n=61) were randomly assigned, using a blocked assignment, to either BH4 or placebo groups. Fifteen of these participants changed their minds before starting on medication, secondary to concerns regarding potential side-effects, time commitment to the study, or a decision to try another treatment course. As a result, 46 participants started the study. Group assignment was generated by a randomization program on Microsoft Excel. One member of the research team (LH) was responsible for all randomization; randomization records were kept on a password-protected computer in a locked office. When consent was given for a child to be in the study, a prescription written for both placebo and BH4 was brought to LH, who included a note to the pharmacist indicating which prescription to fill. This was placed in a sealed envelope and transported to the pharmacy at Lucile Packard Children's Hospital at Stanford University. BH4 and placebo were supplied by the pharmacist as matching pills in identical packaging. Participants, parents, and evaluators (GRE and CK) responsible for assessing the children all were blind to assignment; they remained blind until the final participant completed the trial.
Study medications
Individual doses of BH4 were prescribed in tablet form at 20mg/kg of body weight and taken once daily. The form of BH4 prescribed was given as tetrahydrobiopterin dihydrochloride. BH4 is trademarked as Kuvan and has been United States Food and Drug Administration (FDA) approved for use with individuals with phenylketonuria (PKU) as young as 2 years of age. Pills are easily crushed, and parents were encouraged to mix the pill into a small amount of a substance the child liked and would take easily. A few of the children were able to swallow the pills whole. The weight of each child was measured on inclusion, and children remained on the same dose throughout the duration of the study. No child's weight increased significantly over the course of the study. At each study visit, parents returned unused pills and were provided enough to get them to the next study visit. Compliance was thus assessed at each time point by confirming with the parents and counting the pills. No child missed a significant number of doses, although an occasional miss happened because a child refused to take the medicine on a particular day, was sick and parents skipped a dose, or parents forgot.
Participants were all started on doses of 20mg/kg, the highest dosage that the FDA endorsed for use of BH4 in children with a diagnosis of PKU. If side effects were noted, parents were given the option of decreasing the dose to 10mg/kg or discontinuing in the trial.
Procedures and measures
All patients underwent a standard diagnostic evaluation to screen for inclusion in the study and to collect baseline measures. Each child and the parent or legal guardian were interviewed using the ADOS (Lord et al. 2010) and the ADI-R (Lord et al. 1994). All diagnostic interviews, including the administration of the ADOS, were completed by trained child psychologists, and expert clinical agreement was made with the child psychologist and child psychiatrist. Both raters had to agree that the child met criteria for an ASD.
Baseline assessments included measures of child adaptive functioning, language abilities, and obsessive-compulsive behaviors. Parents completed rating scales that assessed symptoms of maladaptive behaviors, attentional difficulties, and social reciprocity skills as well as a demographic questionnaire. Initial height, weight, blood pressure, and pulse were obtained.
Once participants started the trial, they were seen at weeks 1, 2, 3, 4, 8, 12, and 16. Visits at weeks 1, 2, 3, 4, and 12 were brief, to assess side effects; measure weight, blood pressure, and pulse; and assess global improvement. Appointments at weeks 8 and 16 were lengthier; in addition to the above-listed activities, children were reassessed with ASD symptom-targeted measures including the Preschool Language Scale, 4th Edition, Vineland Adaptive Behavior Scales, 2nd Edition, Survey Interview Form, and questionnaires including the Aberrant Behavior Checklist (ABC) and Social Responsiveness Scale (SRS). At each visit, investigators inquired about health, symptom changes, bowel habits, sleep habits, and irritability. Pills and bottles were also returned and counted to ensure compliance with taking the medication. A semistructured review was completed to assess for adverse effects.
Primary outcome
The CGI-I (Guy, 1976), was considered the primary outcome measure for this study. The CGI-I is a seven point scale that assesses how much the patient's illness has improved or worsened relative to the baseline state at the beginning of the intervention. Categorical responses range from 1 (very much improved) to 7 (very much worse) with a 4 being no change. There is also an efficacy index, which is a four by four matrix that assesses the therapeutic effect by severity of adverse effects. The CGI-I was used by the evaluators, blind to treatment status. For each visit, the child was rated by at least one of the independent evaluators. At weeks 8 and 16, both evaluators rated response to treatment, and these scores were compared for reliability purposes. Participants who received CGI-I scores of 1 (very much improved) or 2 (much improved) at week 16 were considered to be positive responders to the medication.
Secondary outcomes
Several secondary measures were chosen based on their ability to examine core symptoms and important associated symptoms of an ASD. Measures included those to assess language abilities, social skills, repetitive behaviors, irritability, attentional difficulties and adaptive behaviors.
The ABC (Aman et al. 1985) is a 58 item informant-based, factor-analyzed scale composed of a total scale and five subscales that generate raw scores. Subscales include: Irritability (tantrums, aggression, self-injury), Social Withdrawal (lack of responding to others, lack of initiation of interaction), Stereotypic Behaviors (mannerisms, repetitive movements), Hyperactivity, and Inappropriate Speech (excessive talking, repeating phrases). Higher subscale scores indicate more symptoms. The ABC has normative data on individuals with developmental disabilities (Brown et al. 2002) and is sensitive to change with treatment (Research Units on Pediatric Psychopharmacology Autism Network 2002, 2005).
Social skills were assessed with the SRS (Constantino 2002), a 65 item scale used to measure the severity of symptoms in ASDs as they occur in natural social settings. The SRS is composed of one total scale and five subscales that generate raw scores that can be converted to standard T scores (with mean of 50 and standard deviation of 10) for gender and rater type. Standard scores were selected for use in this study. Subscales include Social Awareness, Social Cognition, Social Communication, Social Motivation, and Autism Mannerisms. A total T score of ≥76 is considered severe, and strongly associated with a clinical diagnosis of autistic disorder. A T score of 60–75 is in the mild to moderate range, and considered typical for children with mild or “high functioning” ASD, whereas a T score of ≤59 suggests an absence of ASD symptoms. A total raw score of >75 was associated with a sensitivity value of 0.85 and specificity value of 0.75 for ASD (autistic disorder, Asperger's syndrome, or pervasive developmental disorder – not otherwise specified [PDD-NOS]).
Language skills were assessed using the Preschool Language Scale, 4th Edition (PLS-4; Zimmerman et al. 2002). The PLS-4 is a direct assessment of total, receptive, and expressive language abilities in children up to 6 years, 11 months of age. The PLS-4 is composed of a total scale and two subscales: Receptive Communication and Expressive Communication. The scales generate raw, standard, and age-equivalent scores; raw scores were selected for use in this study. Higher subscale scores indicate more skills.
Adaptive behavior was assessed using the Vineland-2 (Sparrow et al. 2005). The Vineland-2 is a semistructured interview designed to assess communication, daily living, socialization, and motor skills. The Vineland-2 is composed of a total Adaptive Composite scale. We chose to use 10 subscales that specifically address functional domains relevant for a young ASD sample: Receptive Communication, Expressive Communication, Personal Daily Living Skills, Domestic Daily Living Skills, Community Daily Living Skills, Interpersonal Relations, Play Skills, Coping Skills, Gross Motor Skills, and Fine Motor Skills. The scales generate raw or sum, V-, and age-equivalent scores; raw scores were selected for use in this study. Higher subscale scores indicate more skills.
Analytic approach
Chi-square analyses were used to assess change in Clinical Global Impressions – Severity (CGI-S) scores (by group, pre- to posttest) and differences in CGI-I scores (by group, posttest). Mixed-effects regression models (Laird and Ware, 1982) via SPSS MIXED determined the main effects attributed to differences by group (BH4 and placebo), time (treated as categorical at levels baseline, 8 weeks, and 16 weeks), and the group-by-time interaction. Data were not transformed for analysis. All available data were used. There was no imputation of missing values, and the participants were analyzed in their allocated randomization group, consistent with an intent-to-treat analysis, and such that data from all randomized subjects with at least one assessment after baseline (n=46) were analyzed (Fisher et al., 1990). The mixed-effects models accounted for each participant's outcome data at each time point. The mixed-effects regression model is well suited for the analysis of longitudinal data; these models are robust to the data dependency that occurs with the repeated assessments of individuals over time, and can handle missing data. The direct likelihood estimation used for linear mixed models provides unbiased estimates of the means for each group and time combination (under the assumption of missing at random). We used random intercept and trend modeling that accounts for each individual's distinct initial level of symptom severity/functioning and rate of change over time.
Separate models were used for the predictor variable (group) on each secondary outcome measure. Each model included the intercept, time, group, and the time–group interaction to examine differences in treatment response trajectories for children as a function of medication group. In all tests, p values <0.05 were used to indicate statistical significance.
Results
Dosing of tetrahydrobiopterin (BH4)
The mean dose for tetrahydrobiopterin at end-point was 385 mg/day (SD=89) or 19 mg/kg/day (SD=4). Over the 16 week study period, three participants had decreased medication doses (by 50–75%) secondary to side effects of sleep disturbance or irritability. Two participants were in the BH4 group; one was in the placebo group. In all cases, side effect symptoms resolved with the decreased medication dose.
Preliminary analyses
Table 1 summarizes demographic and clinical characteristics, as well as descriptive statistics for all study measures at baseline and end treatment for the total sample and by treatment group, with BH4 (n=23) and placebo (n=23). Chi-square and t test analyses of group differences in the demographic and clinical characteristics revealed that the two groups did not differ significantly in age, gender, racial background, and maternal education. They also were similar for baseline CGI-S and SRS Total. There were group differences at baseline for PLS-4 Total, ABC Social Withdrawal, and Vineland-2 Adaptive Behavior Composite with significantly better baseline PLS-4 Total, ABC Social Withdrawal, and Vineland-2 Adaptive Behavior Composite scores in the BH4 group (see Table 2). In the whole sample, four children had either Asperger's syndrome or PDD-NOS; all four were randomly assigned to the BH4 group. The diagnostic category divergence may explain the baseline group differences with regard to baseline social communication and adaptive skills.
ASD, autism spectrum disorder; CGI, Clinical Global Impressions; PDD-NOS, pervasive developmental disorder, not otherwise specified.
CGI, Clinical Global Impressions; ABC, Aberrant Behavior Checklist; SRS, Social Responsiveness Scale; PLS, Preschool Language Scale.
Forty-two participants completed the study. Four subjects stopped early because of an impression of lack of efficacy, desire to try a different treatment approach, or adverse medication effects. The two groups did not differ in terms of treatment completion: 22 were in the placebo group, and 20 were in the BH4 group. The CONSORT diagram (Fig. 1) displays the flow of participants through the study.
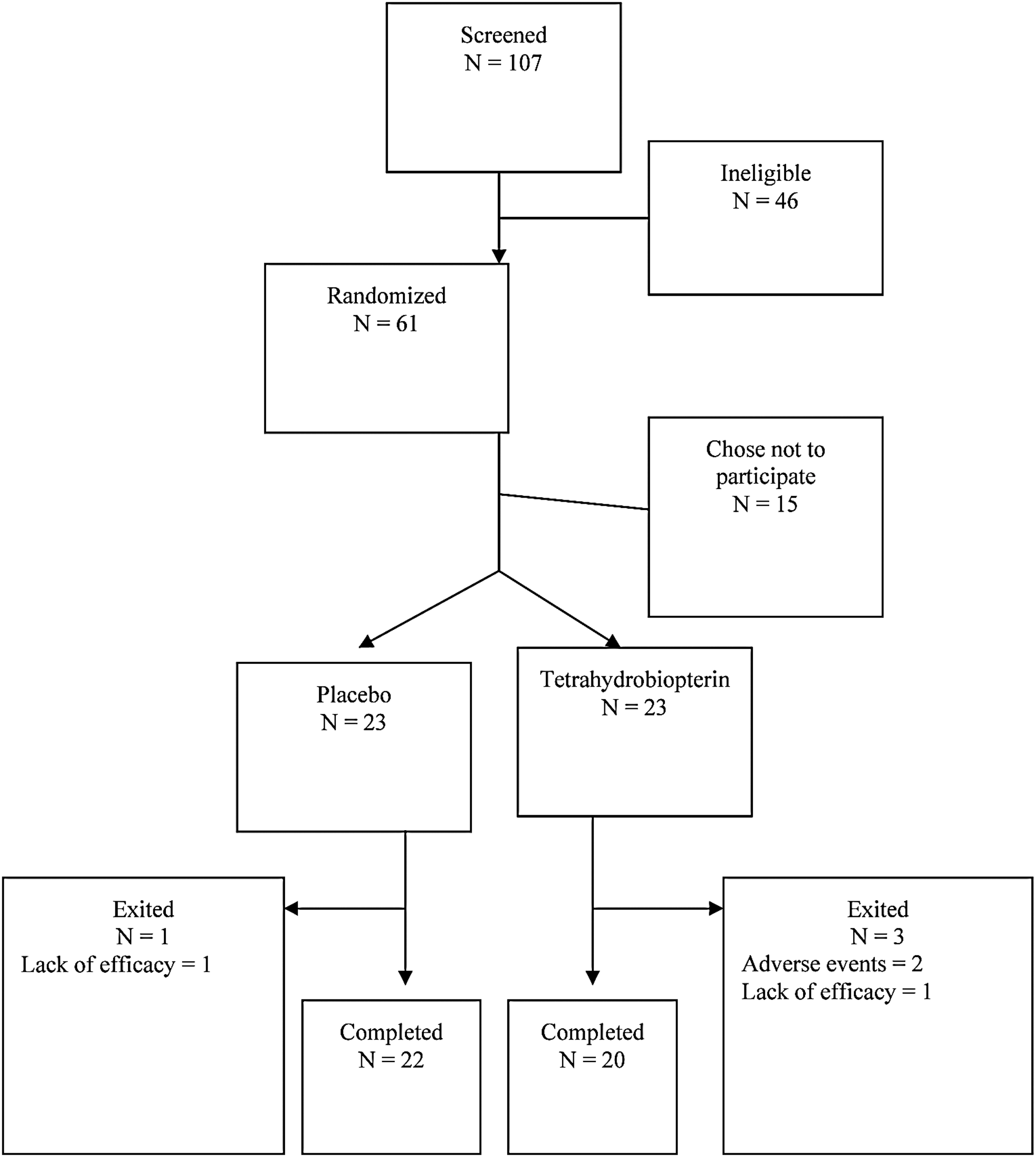
Flow diagram (CONSORT) of a trial of BH4 versus placebo in children with autism spectrum disorder (ASD).
Treatment response
A chi-square analysis was conducted for the primary outcome measure (CGI-I) (see Table 2). Mixed-effects regression models were conducted separately for secondary outcome measure subscale scores (Vineland-2, SRS, PLS, ABC). Given baseline differences on the PLS, ABC, and Vineland-2 measures, the models do not assume successful randomization. Baseline and end-point values for CGI-I, ABC, SRS, PLS, and Vineland-2 are reported in Table 2. Results of the mixed-effects regression models, including parameter estimates, SEs, t values, and p values, are presented in Tables 3 –6.
Does not assume successful randomization. Included additional control variables, including a quadratic term for time; only theoretically relevant effects are reported.
ASD, autism spectrum disorder; ABC, Aberrant Behavior Checklist.
Does not assume successful randomization. Included additional control variables, including a quadratic term for time; only theoretically relevant effects are reported.
ASD, autism spectrum disorder.
Does not assume successful randomization. Included additional control variables, including a quadratic term for time; only theoretically relevant effects are reported.
ASD, autism spectrum disorder.
Does not assume successful randomization. Included additional control variables, including a quadratic term for time; only theoretically relevant effects are reported.
ASD, autism spectrum disorder.
Primary outcome, CGI-I
Overall, there were no significant differences in CGI-I scale scores after 16 weeks of treatment (see Table 2). In the BH4 group, 25% of children showed much or very much improvement, compared with 14% of children in the placebo group (χ2=0.88, p=0.35) (Fig. 2). The CGI-S did not change over the course of the study for either group (χ2=3.44, p=0.06). For both groups, no child showed worsening of symptoms. It is important to note that all children were enrolled in other treatment programs, which were unchanged in intensity or number over the course of the study.
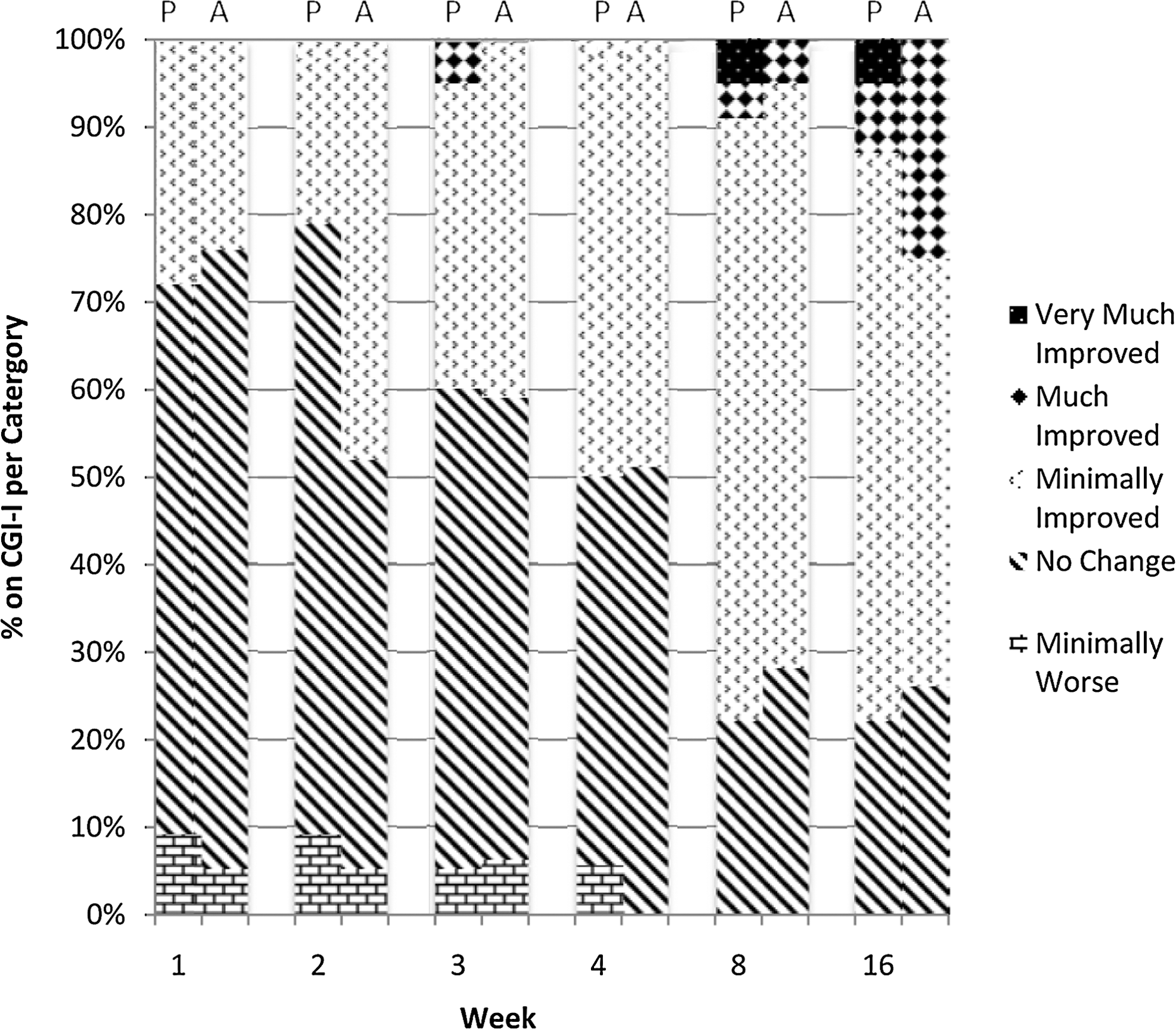
Graphic representation of Clinical Global Impressions-Improvement (CGI-I) scores, over the course of intervention, per placebo (P) and active (A) treatment groups respectively.
Secondary outcomes
Significant differences between groups were noted in several of the secondary measures. Tables 3 –6 summarize the individual models for each outcome measure.
Table 3 addresses the ABC, the measure of abnormal behavior including ASD core symptoms. For all five subscales (Irritability, Lethargy/Social withdrawal, Stereotypy, Hyperactivity, Inappropriate speech), there was a significant group effect: Compared with scores for the placebo group, BH4 group scores were lower (less problematic). For the Stereotypy scale, there was a significant time effect, indicating a decrease in stereotypic behavior over the course of the study. Finally, the group×time interaction analyses generated significant findings for the Hyperactivity scale (T=−2.34 p=0.03) and Inappropriate speech scale (T=−2.19, p=0.03): Compared with children in the placebo group, those in the BH4 group had a greater reduction in hyperactivity and inappropriate use of language. There was a similar trend for the Stereotypy scale (T=−1.93, p=0.06): Compared with children in the placebo group, those in the BH4 group tended to have a greater decrease in stereotypic behaviors.
Table 4 addresses the SRS. For each subscale (Total, Social Awareness, Social Cognition, Social Communication, Social Motivation, Autism Mannerisms), there was a significant group effect, indicating lower SRS subscale scores (i.e., better skills) for BH4 compared with placebo. There was no significant time effect. Finally, the group×time interaction analyses indicated that, compared with children in the placebo group, those in the BH4 group had greater decreases in social awareness problems (T=−2.24, p=0.03) and autism mannerisms (T=−2.01, p=0.05).
Table 5 reports findings for the PLS-4. For all scales and subscales (Total, Expressive Communication, Auditory Comprehension), there was a group effect, indicating higher PLS-4 scores (i.e., better skills) for BH4 compared with placebo. In addition, there was a significant time effect, meaning that all children experienced an improvement in language skills over the 16 week study period. Further, there were no significant group×time interactions.
For the Vineland-2 analyses (Table 6), there was a group effect, indicating higher Vineland-2 scores (i.e., better adaptive behavior) for BH4 compared with placebo. Further, there was a significant time effect with scores improving over time. Finally, there were group×time interactions that were statistically significant for the Play subscale, and a trend for the Community subscale. With regard to social play skills, both groups showed improvement; however, the children in the placebo group showed greater improvement over time (T=−2.62, p=0.02). In addition, compared with children in the placebo group, those in the BH4 group tended to have greater increases in skills necessary to succeed in one's community (T=1.77, p=0.08).
Side effects
At the 16-week visit, 39% of participants reported no adverse events (35% in the placebo group and 43% in the BH4 group). The most common adverse events on the side effects review were (placebo and BH4, respectively): Irritability (17% and 22%), difficulty sleeping (17% and 9%), change in bowel habits (17% and 0%), repetitive behavior (9% and 4%), hyperactivity (4% and 9%), and transient viral rash (0% and 9%). One participant, who was in the placebo-control group, developed new-onset seizures on the last day of the 16 week study; this was the only unanticipated adverse event in the study.
Discussion
This study did not detect an overall effect of BH4 in young children with ASD as measured by the primary outcome instrument, the CGI scale. Nonetheless, significant beneficial effects were detected on several secondary outcome measures, particularly those addressing maladaptive behaviors and social communication skills.
Analysis of the secondary measures reflecting parent reports (ABC, SRS) and clinician interviews (Vineland-2) indicated that there were noteworthy changes that distinguished the BH4 group, particularly with regard to reduced aberrant behaviors, including inappropriate speech, stereotypies, autism mannerisms, social awareness deficits, and hyperactivity, and with regard to improved adaptive skills, including community daily living skills.
With regard to core symptoms, children treated with BH4, compared with placebo, showed greater reductions in the inappropriate use of language (on the ABC), improved social awareness (on the SRS), and larger decreases in autism mannerisms (on the SRS and ABC). Inappropriate use of language includes unusual intonation, echolalia, literal interpretations, and idiosyncratic phrases, and may extend to bizarre or limited expression, reducing the potential for two-way communication. Social awareness focuses on the consistency between facial expressions and feelings, the awareness of the state of mind of others, focus of attention, and self-awareness. Autism mannerisms are the stereotypical behaviors or restricted interests typical in individuals with an ASD. These also can limit expressive or creative peer activities. The reduction in these core ASD symptoms is consistent with the findings of previous uncontrolled nonrandomized studies (Fernell et al. 1997; Naruse et al. 1987, 1989; Nakane et al. 1990; Naruse et al. 1990). The trend for a BH4-related decrease in a particular maladaptive behavior – hyperactivity – has not been reported in previous studies of BH4. This finding deserves further exploration using direct observation measures and reports from multiple observers.
In addition to the measurement of symptom reduction, findings from this study add to the growing scientific literature that concerns the use of medication to support skill improvement and adaptive behavior increases in children with ASD. Children in the BH4 group tended to have improved community-based daily living skills (as assessed with the Vineland-2). Social awareness – the ability to notice social cues (measured by the SRS scale) – also tended to increase. Skills in these areas allow children with ASD to better interact with others, to share, to imitate, and to follow community rules.
Symptom reduction and skill improvement go hand-in-hand: As children with ASD decrease their tendencies to use idiosyncratic phrases and be echolalic, they have more opportunity to use language in a functional manner, such as engaging in conversations with others, answering a range of questions, responding appropriately to questions, and increasing their mean length of utterance. In the same way, when children with ASD are less engaged in perseverative, stereotypic, and hyperactive behavior, they are more likely to notice and respond appropriately to social cues. The demonstration of BH4-related symptom reduction and skill increase in both language and social domains is encouraging, as it increases the likelihood of positive change that is clinically significant.
It is possible that only a subgroup of individuals with ASDs is responsive to treatment with BH4. We did not obtain any physiological measures that could be used to distinguish among possible subtypes of autism with respect to BH4. However, recent work by Frye et al. (2013) examined biomarkers found in CSF. The authors noted that biomarkers related to nitric oxide and pterin metabolism were associated with positive language and behavioral outcomes in children with autism who were treated with BH4. Frye's small, open-label study suggests that use of biomarkers might be one approach to identifying individuals with autism who are likely to respond to BH4.
Strengths of this study include that it was a randomized placebo-controlled trial, that the dosage of medication used was higher than that in past studies, and that the study was maximized to achieve results based on findings from past research (use of younger participants, using a 16 week design, and enrolling children with developmental quotients of at least 50). As with all studies, there are limitations, one of which is sample size. Although this is the largest double-blind placebo-controlled trial to date using BH4, recruitment proved difficult and, therefore, the initial sample size was not obtained, affecting power. Further, secondary to recruitment difficulties, part way through the study, the sample was broadened to include all children on the autism spectrum rather than just those with autistic disorder proper. As a result, four children with an ASD were included; and, purely by chance, all four were assigned to the BH4 group. This likely resulted in the reported baseline differences by group. We addressed those differences statistically, using a robust analytic approach (i.e., linear mixed models) that does not assume successful randomization. However, subsequent study designs could incorporate a recruitment and randomization approach that increases the likelihood of groups with similar ASD symptom range and severity at baseline. Our decision to use the PLS-4 as our clinic-based test of language also was a limitation. Several children made significant improvements in their language capabilities and the ceiling of the PLS-4 did not extend high enough to capture these changes. This may have contributed to the lack of end-of-study group differences on the PLS-4 scales.
As noted, earlier treatment studies with BH4 mainly performed in Japan and Sweden showed similar results to those of the present study. Four of those studies performed between 1985 and 1990 were open label. The double-blind study by Naruse et al. (1989) showed that 54% of the children in the BH4 group and 31% of children in the placebo group responded to treatment. This difference was significant, with the best response observed in children <5 years of age. In the study by Danfors et al. (2005), no significant effect was found between treatment and control group on the CARS; however, post-hoc analyses showed a statistically significant improvement of the ability to interact socially, and a correlation between improvement of social interaction and intelligence quotient (IQ). As in past studies, the treatment was considered safe and well tolerated.
Conclusions
Although results were limited in this study, some promising findings emerged. Most studies of pharmacological agents in autism have focused on treating secondary symptoms; none currently available have been shown to alter core symptoms of ASD such as social, communication, and behavioral difficulties. This study, confirming the results of Danfors et al. (2005), indicates that BH4 may produce some improvement in core symptoms. Also, further research is needed to determine if BH4 may be more beneficial to a specific subgroup of individuals with ASD. Further, specific measures are needed that specifically address change in the core symptoms of autism, especially at the interface of social interaction and language use. The CGI, although a robust measure of change, was developed as a means of addressing psychiatric symptoms, and not necessarily developmental disorders such as autism.
Clinical Significance
Most studies of pharmacological agents in ASD have focused on treating secondary symptoms; none currently available have been shown to alter core symptoms of ASD such as social, communication and behavioral difficulties. This study, confirming the results of Danfors et al. (2005), indicates that BH4 may produce some improvement in core symptoms.
Footnotes
Acknowledgments
The study was conducted at Children's Health Council in Palo Alto, California.
Disclosures
No competing financial interests exist.
Study drugs and matching placebo were provided by BioMarin Pharmaceutical, Inc.