
Abstract
Objective:
This article evaluates the additive effects of children's comorbid conditions with attention-deficit/hyperactivity disorder (ADHD) in relation to caregivers' distress, in a clinical trial conducted through telemental health (TMH).
Methods:
The Children's ADHD Telemental Health Treatment Study (CATTS) is examining the effectiveness of treatment delivered via TMH for children with ADHD who are living in underserved communities. The CATTS trial recruited 223 children (μ=9.53±2.06 years) and their caregivers. Diagnoses of ADHD and comorbid oppositional defiant disorder (ODD) and anxiety disorders (ADs) were established with the Child Behavior Checklist and the Computerized Diagnostic Interview Schedule for Children. We took advantage of rich baseline data from the CATTS trial to investigate associations between caregivers' distress and children's comorbid mental health conditions. Caregivers' distress was assessed with the Patient Health Questionnaire-9, Parenting Stress Index, and Caregiver Strain Questionnaire. ANOVAs were used to compare children with ADHD alone with children having one comorbid condition (ODD or ADs) and children having two comorbid conditions (ODD and ADs).
Results:
Three quarters (75.3%) of participants met criteria for ODD and/or AD comorbid with ADHD: 24.7% had neither comorbidity; 47.5% had ODD or AD; and 27.8% had both ODD and AD comorbidities. The parents of children with multiple comorbid conditions experienced the highest levels of depression, stress, and burden of care.
Conclusions:
The CATTS sample that was recruited from underserved communities provided evidence of additive effects of child psychiatric comorbidities with caregivers' distress, echoing earlier findings from the Multi-modal Treatment of ADHD (MTA) study that was conducted with a metropolitan sample of youth. Results indicate that caregivers' distress should be addressed in developing treatment models for children with ADHD.
Clinical Trials Registry:
Introduction
In the MTA study, comorbidity showed a complicated relationship with baseline characteristics including caregivers' distress in parenting a child with ADHD. Parenting stress and difficulties in the parent–child relationship regarding power assertion and positive affection were significantly increased in relation to ADHD comorbidities of ADs or disruptive behavior disorders. As the impact of ADs and ODD/CD was demonstrated primarily by main effects rather than interaction effects, the investigators suggested that comorbidities have an additive effect on some aspects of caregivers' distress (Jensen et al. 2001a). This association between ADHD comorbidities and caregiver distress has been supported in other investigations, none of which has represented children living in underserved non-metropolitan communities and all of which were conducted with traditional recruitment methodologies that seek to enroll youth with a level of clinical symptomatology typically treated in a psychiatry clinic (Baker 1994; Faraone and Biederman 1997; Bussing et al. 2003; Pfiffner et al. 2005; Kepley and Ostrander 2007; Evans et al. 2009).
The Children's ADHD Telemental Health Treatment Study (CATTS) is a randomized clinical trial designed to evaluate the effectiveness of using telemental health (TMH) to treat children with ADHD who live in in distant underserved communities (Myers et al. in press). In this context, TMH refers to the use of videoteleconferencing (VTC) to provide psychiatric and other mental health services that are usually provided in person (Grady et al. 2011). In this report, we use baseline data from the CATTS study to address the question of whether children's ADHD comorbidities are associated with elevations in caregivers' distress. We anchor our findings to the MTA study upon which the CATTS intervention was based.
Methods
Overview
The CATTS trial was modeled on the MTA study's findings of the benefits of combined medication and psychosocial interventions and delivered through TMH in collaboration with primary care providers (PCPs), who increasingly are expected to provide ADHD treatment, but need assistance with more complex cases (American Academy of Pediatrics 2000, 2001; American Academy of Pediatrics and Committee on Psychosocial Aspects of Child Family Health 2001; Jensen et al. 2001b). Participants represented a broad sample of children diagnosed with ADHD living in underserved communities throughout western and central Washington and one site in Oregon (Myers et al. in press). Research activities were conducted at and telepsychiatry services were delivered from Seattle Children's Research Institute (SCRI). A caregiver behavioral intervention was conducted in person at each of the participating sites by a community therapist who was trained and supervised remotely by a clinical psychologist at SCRI.
Subjects, eligibility, randomization and interventions
Subjects
Boys and girls 5.5–12 years old with suspected ADHD were referred to the CATTS trial by their PCPs. Selected common psychiatric disorders comorbid with ADHD were allowed. Ineligibility criteria included intelligence quotient (IQ) <70, being non-English-speaking, not living with a legal guardian, or medical or psychiatric conditions that required other specific interventions not included in the study protocol, that is, seizure disorders, cardiac disease, autism, or bipolar disorder.
Eligibility determination
Eligibility for participation was determined in a two-step process. After referral of suspected cases of ADHD by PCPs, caregivers completed the Child Behavior Checklist (CBCL) to screen for the presence of ADHD symptoms in their children (Achenbach 2001). If the ADHD diagnostic subscale approached the cutoff (T >65), ADHD was considered probable (American Psychiatric Association 2000). The caregiver then completed the Computerized Diagnostic Interview Schedule for Children (CDISC) to confirm an ADHD diagnosis and the presence of comorbid ODD or generalized anxiety disorder (Shaffer et al. 2000).
Obtaining consent for participation
The study therapists in the study sites obtained written consent and assent for participation in the study according to the study protocol approved by the Institutional Review Board at Seattle Children's Research Institute.
Assessment and randomization
After a diagnosis of ADHD was established, participants completed the baseline assessment of participants' mental health and functional status, including caregiver-report measures and child self-report measures (for children ≥10 years old) with established psychometric properties. Caregivers' distress was measured through administration of validated self-report questionnaires. Participants were then randomized by site and age (5.5–9 years and 10–12 years) to an intervention group without consideration of comoribidity status.
Interventions
Participants were randomized to either active intervention or “enhanced treatment as usual.” The active intervention, Group A, received six two-component sessions spaced 4 weeks apart. The first component, provided by a psychiatrist via TMH, was based on an algorithm-driven pharmacological treatment for ADHD (Pliszka et al. 2006). The second component, provided in person by a community therapist, consisted of an abbreviated evidence-based, caregiver behavior training for ADHD (Pelham and Fabiano 2001). Children randomized to the “enhanced treatment as usual” control condition, Group B, received a single consultation session with a telepsychiatrist who then made recommendations to the referring PCPs for implementation at their discretion.
Measurement of child functional impairment, comorbidity and construction of comorbidity groups
Determining impairment
The CDISC generates a caregiver-rated impairment score in each functional domain on a three point Likert-type scale associated with the child's ADHD symptoms that is based on relationships with their caregiver, family, peers, and teacher as well as the impact on school work. An impairment score on any domain of ≥3 suggests clinical impairment associated with ADHD.
Determining comorbidity
We determined that a comorbid AD or ODD was present if it was indicated on the CBCL and/or the CDISC. Similar to procedures used in other studies, an AD diagnosis was considered present if the Diagnostic and Statistical Manual of Mental Disorders (DSM)-oriented anxiety problem subscale on the CBCL showed a T score ≥70, (Achenbach 1990), and ODD was considered present if the DSM-oriented ODD subscale on the CBCL showed a T score ≥70. An AD and/or ODD were also considered present if parent report met criteria for generalized anxiety and ODD modules of the CDISC (Jensen et al. 2001a; Lewczyk et al. 2003).
Construction of comorbidity study groups
Based on the MTA study's findings that ADs and ODD were additive in their association with caregiver distress, we evaluated the effect of the number of comorbid conditions on caregiver distress. 1) The “ADHD alone” group did not meet criteria for AD or ODD on either the CDISC or the CBCL; 2) The “ADHD plus one” group had ADHD and met criteria for either AD or ODD on the CBCL and/or the CDISC; 3) The “ADHD plus two” group had ADHD and met criteria for AD and ODD on the CBCL and/or the CDISC.
Measurement of caregiver distress
Caregiver distress was assessed in three domains that have been associated with difficulties in parenting a child with mental health problems: Depression, stress, and caregiver strain.
The Patient Health Quesionnaire-9 items (PHQ-9)
The PHQ-9 was used to measure the frequency and severity of caregivers' depressive symptoms experienced in the previous 2 weeks. This scale is widely used, and shows good validity for screening, and high sensitivity and specificity in detecting depression (Gilbody et al. 2006; Wittkampf et al. 2009). In this study, the internal consistency (Cronbach's α) was good at 0.82.
The Parenting Stress Index (PSI)
The PSI is a 20 item measure in which items are rated on a five point Likert-type scale, and higher scores indicate greater stress (Abidin 1983).
Three subscales of the PSI that have shown relevance to parenting a child with ADHD were used: role restriction (7 items; assesses caregivers' perception that their children's demands are a source of frustration and controlling or restricting their personal freedoms), isolation (6 items; assesses whether caregivers feel socially isolated from their peers, relatives, and other supports); and spouse (7 items; assesses whether caregivers perceive that they are lacking the emotional and active support of their significant other to manage their children) (Loyd and Abidin 1985; Haskett et al. 2006). Internal consistency coefficients (Cronbach's α) in this sample ranged from 0.77 to 0.87.
The Caregiver Strain Questionnaire (CGSQ)
CGSQ has 21 items rated on a five point Likert scale and assesses “demands, responsibilities, difficulties, and negative psychic consequences of caring for a relative with special needs” (Bickman et al. 1995; Brennan et al. 1997). The CGSQ has two subscales, objective strain (e.g., missing work because of your child's problems) and subjective strain (e.g., feeling sad as a result of your child's problems). In this study, internal consistency coefficients (Cronbach's α) ranged from excellent (0.89) for objective strain to good (0.85) for subjective strain.
Statistical analysis plan
We report the percentages of participants who met diagnostic criteria for the ODD and AD comorbidities, as well as the percentages of participants with ADHD alone, ADHD with one comorbidity, and ADHD with two comorbidities. Caregivers' distress is reported as means and standard deviations for the PHQ-9, PSI subscales, and CGSQ subscales. To assess the level of caregivers' distress across the three comorbidity subgroups, we conducted a one way analysis of variance (ANOVA), with means and standard deviations for the PHQ-9, PSI subscales, and CGSQ subscales reported across the three ADHD comorbidity subgroups. Tukey honestly significant difference (HSD tests) were used to make post hoc two way comparisons.
A one way analysis of covariance (ANCOVA) (between subjects factor: comorbidity group [ADHD alone, ADHD plus one, ADHD plus two]; covariate: ADHD impairment) was used to assess the contribution of ADHD impairment to the association between children's ADHD comorbidity and caregivers' distress. Bonferroni tests were used to make post-hoc two way comparisons between comorbidity groups after controlling for ADHD impairment. All analyses were conducted in SPSS version 19.0.
Results
Description of sample
The final sample by study subgroups is summarized in Table 1. Overall, 223 children with 163 (73%) males and a mean age of 9.53±2.06 were enrolled in the trial. The majority of caregivers (76%) were biological mothers. Demographics did not vary across the three comorbidity groups, as shown in Table 1.
Chi square analyses demonstrated that the percentage of participants with each of the demographic variables above did not differ across comorbidity groups, all ps >0.14, ns.
ADHD, attention-deficit/hyperactivity disorder.
ODD and/or AD comorbidities were common, diagnosed in 75.3% of participants and distributed among the three comorbidity subgroups as follows: 55 (24.7%) children with ADHD alone, 106 (47.5%) children with ADHD plus one comorbidity (ODD or AD), and 62 (27.8%) with ADHD plus two comorbidities (ODD and AD).
ADHD comorbidity and caregiver distress
Caregivers of children diagnosed with ADHD and comorbid disorders (AD and/or ODD) indicated having higher levels of depression, stress, and strain than did caregivers of children diagnosed with ADHD alone, as is shown in Table 2, and depicted graphically in Figure 1. A consistent pattern emerges, with caregivers of children at each successive level of comorbidity showing an increased increment of distress. The magnitude of the incremental increase in caregiver distress varied across measures.
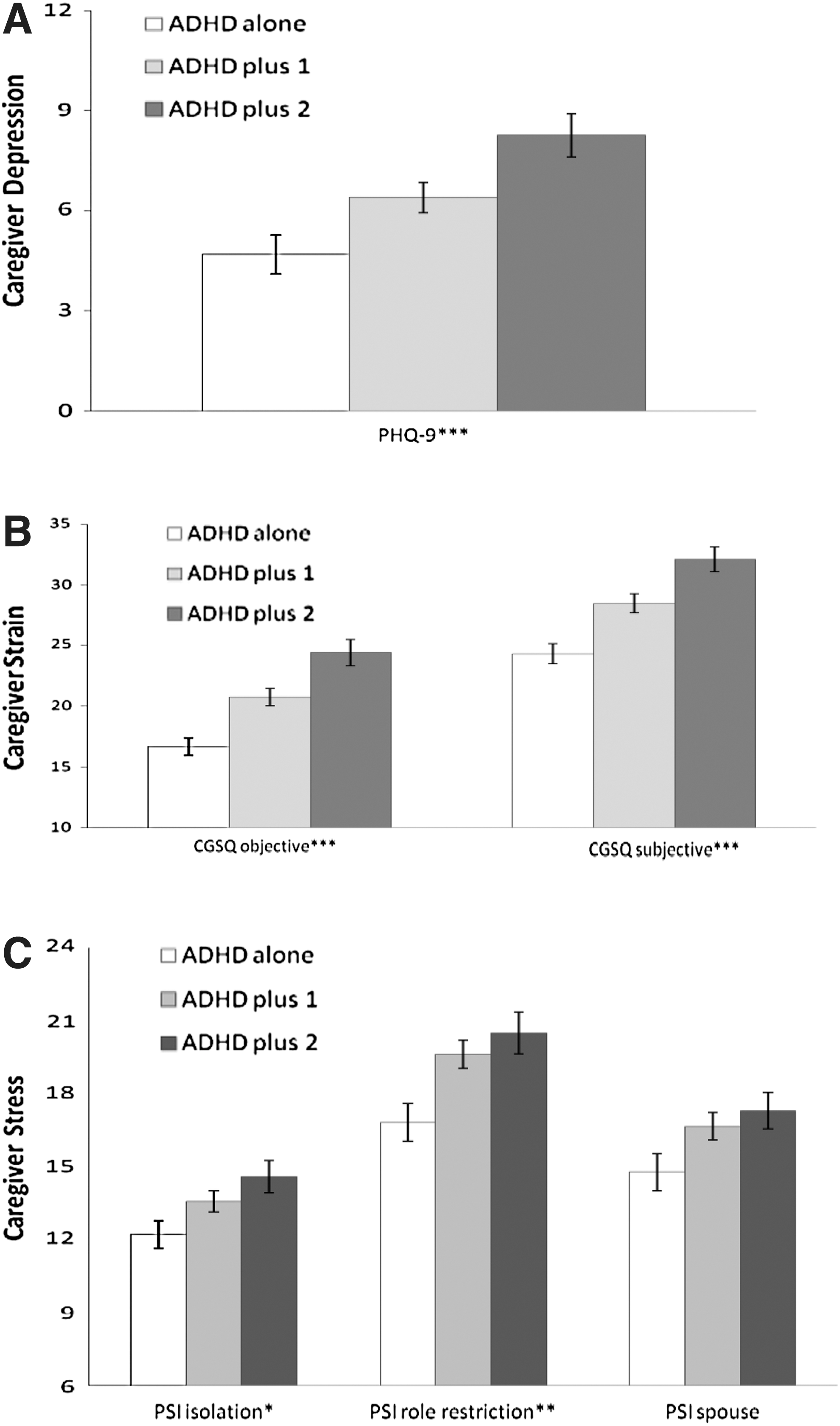
Caregiver distress in relation to attention-deficit/hyperactivitiy disorder (ADHD) comorbidities.
a, ADHD alone different from ADHD plus 1 * p<0.05.
b, ADHD alone different from ADHD plus 2 ** p<0.01.
c, ADHD plus 1 different from ADHD plus 2 *** p<0.001.
ADHD, attention-deficit/hyperactivity disorder; ANOVA, analysis of variance; PHQ-9, Patient Health Quesionnaire-9 items; PSI, Parenting Stress Index; CSQ, caregiver strain questionnaire.
Overall, the mean caregiver depression measured with the PHQ-9 among caregivers in the sample indicated mild depressive symptoms (Gilbody et al. 2006). Depression varied significantly across comorbidity groups with the mean level of caregiver depression increasing with the number of ADHD comorbidities. Having dual comorbidities was associated with higher caregiver depression.
Caregiver stress reported on each of the PSI subscales indicated mild to moderate stress as determined in relation to the established normative data (Abidin, 1983). Caregiver stress varied significantly by comorbidity group for both the role restriction and isolation subscales. Post-hoc comparisons of the PSI role restriction and isolation subscales demonstrated that caregivers of children with ADHD plus one or two comorbidities experienced greater stress than did caregivers of children with ADHD alone. There was no additive effect for dual comorbidities.
The mean level of caregiver strain on the CGSQ for the caregivers in this study indicated a moderately severe level of burden for caregivers. Both the objective strain subscale and the subjective strain subscale, as well as the total score, differed by comorbidity group. Caregivers of children with ADHD alone reported the least and caregivers of children with ADHD plus two comorbidities reported the most objective, subjective, and total strain, or burden, in caring for their children. Post-hoc comparisons showed that there was an additive effect of dual comorbidities for subjective and objective strain, as well as for total score.
Associations of ADHD impairment, comorbidities, and caregiver distress
Caregiver-rated ADHD impairment determined from the CDISC differed across the three comorbidity groups. Post-hoc analyses demonstrated that children with ADHD alone had significantly lower impairment attributable to ADHD than did children with ADHD plus one or ADHD plus two comorbidities. ADHD impairment did not differ between youth with ADHD plus one and ADHD plus two comorbidities.
ANCOVA analysis was performed to evaluate whether child's level of impairment from ADHD accounted for associations between comorbidity and caregiver distress. This analysis showed that caregiver depression and strain remained significantly associated with comorbidity, suggesting that impairment did not account for the association. However, adding the impairment covariate diminished the main effect of comorbidity on caregiver stress as measured by the PSI, such that only the association between child comorbidity status and caregiver stress caused by role restriction was significant. This finding suggests that the child's impairment attributable to ADHD accounted for a substantial portion of the caregivers' reported stress.
Discussion
The CATTS trial was designed to provide an intervention similar to the landmark MTA study, but was delivered via TMH in an abbreviated model relevant to collaboration with PCPs in the care of children and families living in communities that lacked access to expert mental health care (Morley 2010; Lim et al. 2011). The main advantage of delivery of care via TMH is that the patients and families did not have to travel for their care, and PCPs established collaboration with a mental health team.
The analyses presented here are cross sectional and describe the baseline characteristics of the sample prior to intervention. This description of the children and caregivers participating in CATTS paves the way for forthcoming reports of treatment response, outcomes, and moderators and mediators of outcomes. The majority of patients with ADHD who were referred to both the MTA and CATTS studies had high rates of comorbid ODD and/or ADs: 75% of participants in the CATTS trial versus 67% of participants in the MTA study. The somewhat higher occurrence in the CATTS trial may reflect truly higher rates for children living in non-metropolitan communities; or that families with greater comorbidity living in non-metropolitan communities may be more willing to participate in a novel clinical trial that offers expert care that is otherwise unavailable. There is evidence that in the decade since completion of the MTA trial, PCPs have become more skilled in managing routine cases of ADHD; therefore, they may refer more severely affected youth to specialty care such as that offered by the CATTS trial (Pfiffner et al. 2005; Kepley and Ostrander 2007; Ross et al., 2011).
The CATTS trial also echoes the MTA study's findings in several respects regarding caregivers' distress. Overall, caregivers in the CATTS trial rated their level of depression as mild on the PHQ-9 as did caregivers in the MTA study on the Beck Depression Inventory (Owens et al. 2003). In contrast to the MTA study in which comorbid ADs and ODD/CD were not associated with increased caregiver depression, in CATTS, caregivers' depression was significantly higher when youth had ADHD plus two comorbidities. Similar to the MTA study (Jensen et al. 2001a), in the CATTS study, stress caused by both role restriction and isolation were significantly increased when the child had one or two comorbidities. Whereas the MTA study did not assess caregiver strain directly, in the CATTS trial, the total strain score for the highly comorbid group was similar in magnitude to the levels of strain found in past studies of caregivers of youth with severe emotional and behavioral disturbances (Bickman et al. 1995; Brennan et al. 1997; Khanna et al. 2012). The concept of strain, or caregiver burden, is relevant to current efforts in healthcare reform; specifically that rural families carry a disproportionate burden relative to those in urban areas in terms of resources available to optimally address their children's needs (Power 2009).
Limitations
This report is intended to describe the baseline characteristics of the sample enrolled in the CATTS trial with respect to comorbidity and its association with caregivers' distress, which may moderate or mediate outcomes in treatment trials for children with ADHD. As interesting as the findings are in indicating an association between children's ADHD comorbidities and caregivers' distress, the baseline assessment was cross sectional, such that the temporal sequence for the development of childhood psychopathology and caregiver distress could not be determined. At the point of referral, regardless of the temporal sequence, it is important to recognize that children's complex diagnoses are associated with caregivers' distress. The association is likely reciprocal and possibly cascading. The findings regarding prevalence of comorbid conditions and associations between children's ADHD comorbidities and caregivers' distress within a clinical trial of referred participants may not generalize to children with ADHD in the community at large. Furthermore, these findings were based on caregivers' reports alone, which may be affected by caregivers' distress. Patients and families were required to participate in English, which limited the recruitment of Latinos in several of the participating communities. In addition, the use of both the CBCL and the CDISC for eligibility screening is more extensive than is typically achieved in outpatient pediatrics or child and adolescent psychiatry practice. This thoroughness is desirable for thorough evaluation, but may not be feasible in typical practice settings.
Conclusions
This study showed a high prevalence of comorbid conditions, functional impairment, and caregiver distress among children with ADHD living in underserved communities. Each of these features increased the challenges that families of children with ADHD face in navigating and obtaining effective healthcare and educational supports. Comorbidity with ADHD for children living in non-metropolitan communities takes a particularly high toll on the quality of their families' lives because of the limited access to expert mental health services (Thomas and Holzer 2006; Gabel 2009).
Clinical Significance
These findings should encourage policy makers to include caregivers in the development of services for children, and to support the use of TMH as one model to provide such services. A future goal of the CATTS study is to explore in post-hoc analyses how caregivers' level of distress might moderate treatment effectiveness and how reduction in caregivers' distress might mediate the effects of the intervention on treatment outcomes.
We would like to thank Phaedra Pascoe for her work on an earlier version of this article, funded by the American Academy of Child and Adolescent Psychiatry Medical Student Fellowship sponsored by Campaign for Kids. We want to acknowledge the contributions of the CATTS team including Gina Kim and Heather Violette and the children, families, and PCPs who participated in the CATTS project.
Disclosures
No competing financial interests exist.
This research was supported by funding from the National Institute of Mental Health (IR01MH081997 and R01MH081997-04S1); the University of Washington Institute of Translational Health Sciences Small Pilot Project Grant program (5668210); the University of Washington Royalty Research Fund program (65-4020); and the American Academy of Child and Adolescent Psychiatry Abramson Fund (506200020101).