
Abstract
Objective:
Little is known about the effectiveness of pharmacological interventions on autism spectrum disorder (ASD). This is a systematic review of the randomized controlled trials (RCTs) of oxytocin interventions in autism, made from January 1990 to September 2013.
Method:
A search of computerized databases was supplemented by manual search in the bibliographies of key publications. The methodological quality of the studies included in the review was evaluated independently by two researchers, according to a set of formal criteria. Discrepancies in scoring were resolved through discussion.
Results:
The review yielded seven RCTs, including 101 subjects with ASD (males=95) and 8 males with Fragile X syndrome. The main categories of target symptoms tested in the studies were repetitive behaviors, eye gaze, and emotion recognition. The studies had a medium to high risk of bias. Most studies had small samples (median=15). All the studies but one reported statistically significant between-group differences on at least one outcome variable. Most findings were characterized by medium effect size. Only one study had evidence that the improvement in emotion recognition was maintained after 6 weeks of treatment with intranasal oxytocin. Overall, oxytocin was well tolerated and side effects, when present, were generally rated as mild; however, restlessness, increased irritability, and increased energy occurred more often under oxytocin.
Conclusions:
RCTs of oxytocin interventions in autism yielded potentially promising findings in measures of emotion recognition and eye gaze, which are impaired early in the course of the ASD condition and might disrupt social skills learning in developing children. There is a need for larger, more methodologically rigorous RCTs in this area. Future studies should be better powered to estimate outcomes with medium to low effect size, and should try to enroll female participants, who were rarely considered in previous studies. Risk of bias should be minimized. Human long-term administration studies are necessary before clinical recommendations can be made.
Introduction
A
ASD shows a marked male bias in prevalence, with approximately four affected males for every affected female (Werling and Geschwind 2013). Males tend to be over-represented among high-functioning cases, whereas males and females are more equally represented among cases with severe intellectual disability (Fombonne 1999).
Twin studies have long led to the recognition of the high heritability of ASD (Smalley et al. 1988; Mendelsohn and Schaefer 2008). The most consistently reported single-gene disorders associated with ASD (∼5% of cases) are Fragile X syndrome, Rett syndrome, tuberous sclerosis, and phosphatase and tensin homolog (PTEN) mutations (Carter and Scherer 2013). Rare genetic variants, and copy number variants in particular, have been shown to play a major role in ASD (Heil and Schaaf 2013). In addition to autism-related genes, various environmental events are thought to act as triggering factors in the development of ASD, including obstetric complications (Arndt et al. 2005; Libbey et al. 2005; Patterson 2009); prenatal influenza, rubella, and cytomegalovirus infections (Pardo et al. 2005); maternal stress during pregnancy (Beversdorf et al. 2005; but also see Rai et al. 2012); and maternal use of thalidomide (Strömland et al. 1994), misoprostol, and especially valproic acid during pregnancy (Landrigan 2010; Christensen et al. 2013).
People with ASD typically show disrupted social motivation (Chevallier et al. 2012; Stavropoulos and Carver 2013). They express abnormal social orienting through diminished eye contact and social aloofness (Osterling et al. 2002; Nakano et al. 2010); reduced reward in social relationships through diminished friendship seeking and liking (Baron-Cohen and Wheelwright 2003; Howlin et al. 2004); and scarce efforts in maintaining social relationships because of scarce interest in initiating social exchanges, and lack of tact or indifference to reputation (Hobson and Lee 1998; Izuma et al. 2011). It was suggested that early impairment in children's social attention would reduce their interest in social relationships. This would result in deprivation of social learning experiences, with further imbalance in attending to social stimuli and social cognitive development, and disrupted social skills (Chevallier et al. 2012).
The complexity and the considerable variability of the severity and appearance of ASD symptoms are particularly challenging. A comprehensive and detailed assessment of symptoms variation in time is crucial to decide on the effects of treatment (Johnson and Myers 2007; Falkmer et al. 2013).
Pharmacotherapy for the core symptoms in ASD
Nowadays, there is no approved pharmacological therapy for the social symptoms of ASD. The antipsychotic risperidone was approved for the treatment of behavioral symptoms of ASD grouped under the general heading of irritability, which included aggression, deliberate self-injury, and temper tantrums (Jesner et al. 2007). The antipsychotic aripiprazole, also, was approved for the treatment of irritability in ASD in the United States (Farmer et al. 2013). Drugs are generally used to control the most dysfunctional behaviors in the social sphere (Dove et al. 2012), whereas the treatment of the social symptoms is based on social skills training aimed at improving social and communicative skills (Maglione et al. 2012), in combination with other psychosocial and educational treatments aimed at addressing sensory processing disorders, language impairment, and atypical information processing (Suarez 2012; Oono et al. 2013).
Evidence that polymorphisms and haplotypes in the oxytocin receptor gene are related to ASD (Jacob et al. 2007; Lerer et al. 2008; Liu et al. 2010; Li et al. 2012), and the demonstration that oxytocin administration can influence social behavior in humans (Kosfeld et al. 2005; Domes et al. 2007b; Guastella et al. 2008; Declerck et al. 2010), prompted the investigation of the effectiveness of oxytocin in ASD (Andari et al. 2010; Guastella et al. 2010; Anagnostou et al. 2012).
Oxytocin, a multipurpose compound
Oxytocin is a nonapeptide (i.e., it has nine aminoacids); it is synthesized in magnocellular neurons in the paraventricular nucleus and the supraoptic nucleus of the hypothalamus, and is released into the bloodstream by axon terminals in the posterior pituitary (du Vigneaud et al. 1953; du Vigneaud 1955; Insel 1992). There is one single oxytocin receptor, a 389 aminoacid polypeptide with seven transmembrane domains, which belongs to class I of the G protein-coupled receptor family (Kimura et al. 1992). This oxytocin receptor is expressed in peripheral tissues, such as the uterus, the mammary gland, the ovary, the kidneys, the heart, the bones, and the endothelial cells (Gimpl and Fahrenholz 2001), and in the mammalian central nervous system. The olfactory bulb and tubercle, the neocortex, the endopiriform cortex, the hippocampus, the central and lateral amygdala, the bed nucleus of the stria terminalis, the nucleus accumbens, and the ventromedial hypothalamus were reported to express the oxytocin receptor in rodents (Yoshimura et al. 1993; Vaccari et al. 1998). In humans, an autoradiographic study detected oxytocin-binding sites in the basal nucleus of Meynert, in the diagonal band of Broca, the lateral septal nucleus, the preoptic/anterior hypothalamus, the ventral pallidum, and the lateral septum, but not in the striatum or the amygdala (Loup et al. 1991).
By acting on its receptor, oxytocin triggers its own further release from the magnocellular neurons in the paraventricular nucleus and the supraoptic nucleus (Landgraf and Neumann 2004). This positive feedback loop is likely to be involved in the therapeutic action of the compound (Carson et al. 2013). The oxytocinergic system shows high plasticity (Theodosis et al. 2006; Veenema 2012), and is likely to reflect sensitivity to adaptive physiological conditions (pregnancy, lactation) and environmental ones (bond formation and cleavage).
The main peripheral actions of oxytocin are induction of milk letdown and the facilitation of uterine contractions (Ivell et al. 2001). In addition to pregnancy, oxytocin is involved in a wide range of peripheral actions in the male and female reproductive tract, the pancreas, the cardiovascular system, and the kidneys (Lippert et al. 2003). Oxytocin and the related nonapeptide arginine vasopressin are also involved in social behavior, and, in particular, in the formation of mother–infant and adult–adult pair bonds, separation distress, social memory, and recognition, as well as stress response and regulation of feeding and grooming (Donaldson and Young 2008; MacDonald and MacDonald 2010). Peripheral indicators such as levels of salivary and plasma oxytocin, were related to parenting behaviors in child–parent attachment relationships (Levine et al. 2007; Feldman et al. 2011). Studies in animals proved that oxytocin antagonizes avoidance of proximity and inhibits defensive behavior, thereby facilitating approach behavior (Heinrichs et al. 2009). Oxytocin is also involved in sexual arousal and in orgasm, with its actions being principally expressed in the periphery (Borrow and Cameron 2012). Some actions of oxytocin might be peripheral initially (stimulating central actions) rather than primary central (Borrow and Cameron 2012; Churchland and Winkielman 2012).
In humans, oxytocin has become the treatment of choice for managing postpartum hemorrhage (Su et al. 2007), and is widely used to induce labor (Alfirevic et al. 2009). Peripherally administered oxytocin does not cross the blood–brain barrier. A scant 0.002% of the peripheral dose can be found in cerebrospinal fluid (CSF) after intravenous injection (Mens et al. 1983), although peptides can enter the CSF through the nasal pathway as it bypasses the blood–brain barrier (Born et al. 2002). The administered peptides last in the CSF up to 80 minutes after intranasal administration, but some of their effects have a shorter duration (Thompson et al. 2006). Replicable changes in brain functioning – as inspected with functional magnetic resonance or electroencephalography – after intranasal administration of oxytocin were considered a further proof of this route of administration, allowing the compound to pass the blood–brain barrier (Perry et al. 2010; Riem et al. 2011; Bethlehem et al. 2013). Intranasal administration is simple, and is likely to cause minimal discomfort to the patient, therefore resulting in high compliance (Guastella et al. 2013).
Oxytocin and social cognition
In healthy humans, intranasal oxytocin was reported to increase trust (Kosfeld et al. 2005; Baumgartner et al. 2008; Andari et al. 2010), and to foster cooperation among unrelated persons (De Dreu et al. 2010; Rilling et al. 2012). Administration of oxytocin was also found to improve recognition of emotional facial expressions (Kirsch et al., 2005; Bartz et al. 2010; Hurlemann et al. 2010; Marsh et al., 2010), which is thought to support greater empathic concern for conspecifics (MacDonald and MacDonald 2010). Cumulative effect sizes were small (Cohen's d=0.21) for emotion recognition, and medium (d=0.43) for in-group trust (Van Ijzendoorn and Bakermans-Kranenburg 2012). Studies were not always consistent, and negative findings were reported, as well (Bartz et al. 2011). Situational and/or individual difference moderators were suggested to impact on the effects of oxytocin on social cognition and behavior. Different mechanisms were hypothesized to explain the situational dependence of oxytocin social effects in humans. Oxytocin might reduce anxiety toward social stimuli by favoring prosocial approaches (e.g., increased trust). Evidence that oxytocin modulates anxiety and fear in animals (McCarthy et al. 1996), and shows anti-stress effects in humans (Ditzen et al. 2009) is compatible with this hypothesis. Oxytocin might also influence the perceptual salience and/or processing of social cues (Bartz et al. 2011). Oxytocin promotes gaze in the eye region (Guastella et al. 2008; Andari et al. 2010); this effect might depend on increased salience attributed to social stimuli, or greater reward from attending to socially relevant stimuli after oxytocin.
Potential effects of oxytocin in people with ASD
People with ASD refrain from social interactions, show gaze aversion, and attend to social stimuli with lower interest than people without ASD. Reducing social anxiety, and increasing salience to social stimuli or their rewarding properties might improve some of the core features of ASD. Moreover, it might decrease repetitive behavior as a positive side effect of reducing anxiety and/or increasing attention toward social stimuli.
Why this review is important
Despite limited scientific evidence, there is a growing interest in the effectiveness of oxytocin in ASD. A growing number of claims about the potential effectiveness of oxytocin in ASD have recently spread in the media, particularly on web sites (e.g., Yale University, 2012). Some parents report that they decided to administer the compound themselves to their children affected by ASD (Munesue et al. 2010; Kosaka et al. 2012). These were not controlled studies, and the consistency of these results requires confirmation. A considerable amount of public and private funds is being invested to evaluate the therapeutic benefit of oxytocin in ASD (Miller 2013). Considering the relevance of the topic for healthcare policies and the community at large, a systematic review of randomized controlled trials (RCTs) assessing the effectiveness of oxytocin treatment of ASD and providing adequate evaluation of the risk of possible bias in the results and a detailed grading of evidence, might be useful to guide new studies and spread scientific knowledge. Past reviews on this topic merely listed the main results of the studies without evaluating their quality or the possibility to generalize evidence (Stavropoulos and Carver 2013).
Aims of the study
This study aimed at presenting a systematic review of all randomized, placebo-controlled trials of oxytocin administration in people with ASD, with particular focus on the possible bias in the results, and with a grading of empirical evidence.
Methods
A literature search was conducted for RCTs evaluating treatments of ASD with oxytocin. Studies were considered relevant if they: • were published in peer-reviewed journals; • included a sample of individuals diagnosed with ASD; • included a placebo-controlled group; • included at least one outcome measure related to an ASD core symptom, in the domain of either communication and socialization, or of restricted and repetitive patterns of interests and activities.
PubMed/MEDLINE® was searched from January 1990 to March 2013 using the key words
Two authors (M.M., S.S.) assessed all the retrieved articles for inclusion, on the basis of their titles and abstracts. A third author (A.P.) assessed the selected records again, and inspected the full article for inclusion criteria. The selection flow chart is shown in Figure 1.
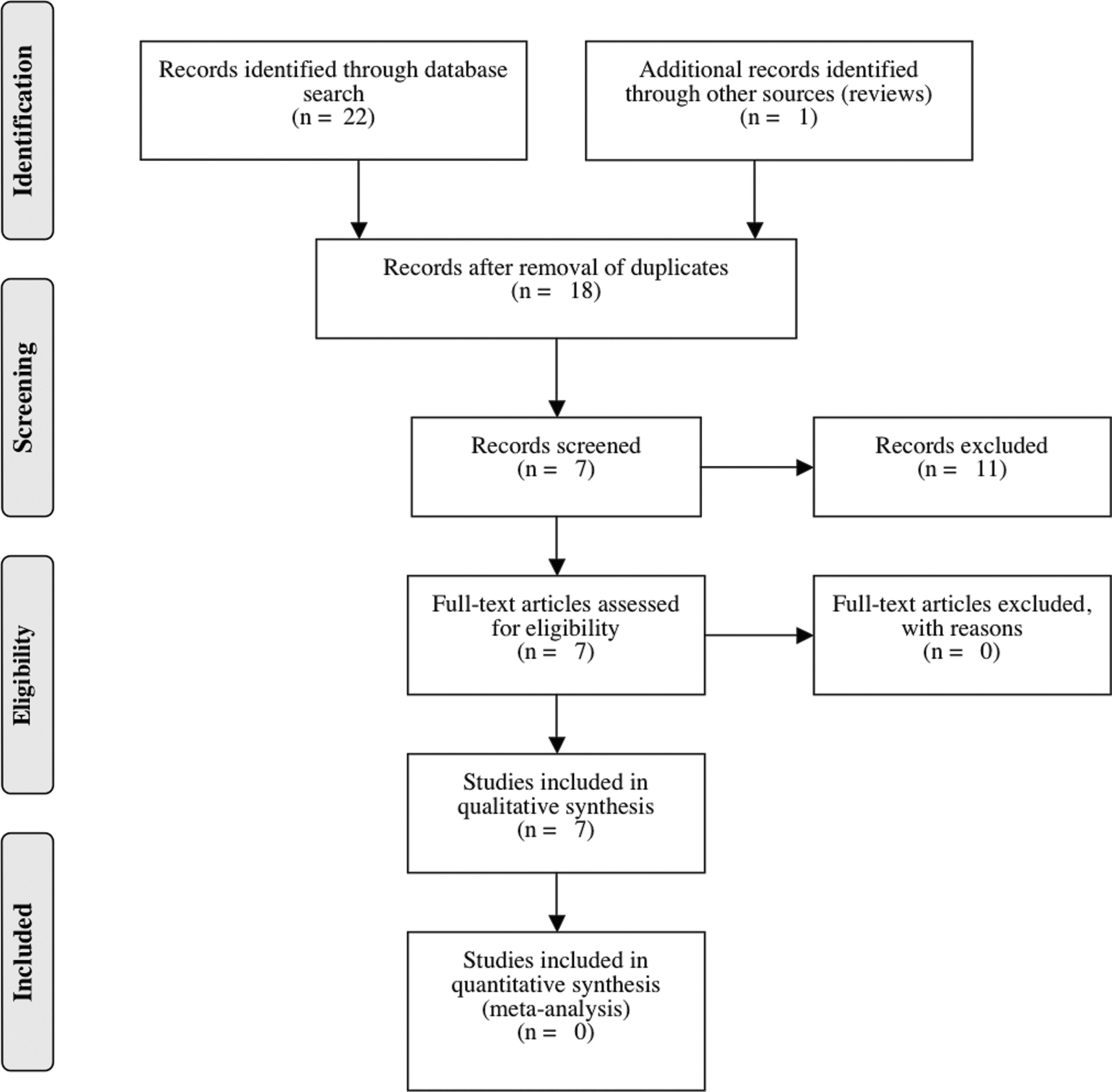
Flow diagram.
Two authors (M.M., S.S.) extracted the data, and disagreements were solved by discussion.
Two researchers assessed the quality of the studies independently using the Cochrane risk of bias tool (Higgins et al. 2011). Six specific methodological domains were assessed: Sequence generation in the randomization, allocation concealment, blinding of participants and assessors, incomplete outcome data, selective outcome reporting, and a residual category for other issues (see subsequent discussion). The “sequence generation in the randomization” is any description of the procedure that was adopted to generate an unpredictable sequence of allocations; “allocation concealment” refers to the description of the precautions taken to prevent patients becoming aware of the group they will be assigned to before their final allocation to their respective groups; the “blinding of participants and assessors” refers to the description of the procedures that prevent study participants, caregivers, or outcome assessors from knowing which intervention was received (Wood et al. 2008); “incomplete outcome data” refers to data missing because of attrition or exclusion from the analysis; “selective outcome reporting” is any evidence of the selection for publication of a subset of study findings or analyses based on the significance and direction of the results (Sterne et al. 2008), and it is inferred by some outcome measures' being recorded in the methods but not reported; and the “other issues” are specified subsequently.
The risk of bias of each domain was judged low, high, or unclear. Two authors performed this evaluation (A.P., M.V.). Discrepancies in scoring were resolved through discussion. Further consideration was given to the following factors (other issues): Whether diagnostic criteria were specified, how the diagnosis was achieved, whether psychometric characteristics of the tool used to assess the main outcome were reported, whether an a priori power analysis was performed, whether dropouts were reported or not, and whether side effects and adverse events were reported. The lowest sample size necessary to achieve ≥80% power, with a 5% one tailed test to detect the minimum large effect (d=0.80), is 20 (Kraemer and Kupfer 2006); in crossover trials, when participants serve as their own controls, this corresponds to 10 subjects. With the same parameters, the lowest sample size to detect the minimum medium effect size (d=0.50) is 60 (i.e., 30 subjects in crossover trials).
Key findings were summarized in a narrative form, as few studies were finally included, and only one study was retrieved for each comparison, precluding meta-analyses. When calculable, effect sizes were reported as Cohen's d, η2 or Pearson's r (Cohen 1988). To calculate r from Mann–Whitney U test's z, the following formula was applied: r=z /(square root of n), with n=sample size.
Grading of evidence was estimated according to the recommendations of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, which takes into account how the evidence was achieved (RCTs versus observational trials or case reports), inconsistency of results (which is inferred by significant heterogeneity of the study results), indirectness of evidence (which is inferred by the use of approximated population level measures), imprecision (which pertains to wide confidence intervals [CI], continuous data with CI>0.5, and binary and correlation data with CI>0.25 in either direction), and the risk of bias in the trials (Guyatt et al. 2008, 2011). Five factors (study limitations, imprecision, inconsistency of results, indirectness of evidence, likely publication bias) may lead to rating down the quality of evidence, whereas three factors (large magnitude of effect, dose-response, and confounders) may rate it up (Guyatt et al. 2008, 2011).
Results
The search strategy identified 18 abstracts, 7 of which related to potentially eligible studies. The main characteristics of the included studies are reported in Table 1.
IQ, intelligence quotient; DSM-IV, American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; DISCAP-ASD,
Six studies included subjects diagnosed with high functioning ASD (intelligence quotient [IQ]>70); two out of these six studies were on the same subjects (Hollander et al. 2003, 2007). One study was on eight males diagnosed with Fragile X syndrome, an inherited condition causing intellectual disability that is assimilated into ASD because of its symptoms: Disturbance in language/communication, social deficits with peers, social avoidance, gaze aversion, unusual responses to sensory stimuli, and stereotypic behavior (Hall et al. 2012).
Duration of the trials
Five studies were crossover trials with a short interval (1–3 weeks) between the first administration (oxytocin or placebo) and the second (the reverse). One study was a short-term, 4 day treatment trial (Dadds et al. 2013), with administration of oxytocin once a day. The participants were involved in parent–child interaction training, including an emotion recognition training based on the Mindreading program developed by Baron-Cohen (2007), and the study was aimed at assessing pre-post changes in parent–child social interaction, repetitive behaviors, and emotion recognition. Changes in parent–child social interaction and repetitive behaviors were assessed by the microanalysis of the family observation videos, whereas emotion recognition was tested with the University of New South Wales (UNSW) Facial Emotion task (Dadds et al. 2004). Diagnostic severity at post-treatment (day 5) was assessed with the Childhood Autism Rating Scale (CARS) (Schopler et al. 1988) and the Ohio State University (OSU) Autism Rating Scale-DSM IV (OSU Research Unit 2005). Another study was a 6 week treatment study where administration of intranasal oxytocin was twice a day (Anagnostou et al., 2012). Participants were tested every 2 weeks on the Clinical Global Impressions (CGI) (Guy 1976), and received additional testing on the Yale Brown Obsessive Compulsive Scale (YBOCS) – Compulsion Subscale (Goodman et al. 1989), the Repetitive Behavior Scale – Revised (Bodfish et al. 2000), and the Social Responsiveness Scale (Constantino 2002). At baseline and after the 6 weeks of treatment, participants were also tested on the Reading the Mind in the Eyes (Baron-Cohen et al. 2001), the Diagnostic Analysis of Nonverbal Accuracy (DANVA) (Baum and Nowicki 1989), and on a measure of quality of life, the World Health Organization Quality of Life Questionnaire (WHOQOL) – Emotional/Social Subscales (Skevington et al. 2004). Primary outcome measures of the study included the CGI – Improvement, the DANVA Paralanguage Test, and the Repetitive Behavior Scale – Revised. The other measures were considered secondary.
Location of the trials
Four studies were conducted in the United States, two in Australia, and one in France.
Administration methods and doses of oxytocin
Two studies were based on continuous intravenous administration of oxytocin (10 IU/mL; total dose unspecified); the other five studies were based on intranasal administration of oxytocin, with doses ranging from 12 to 48 IU. The youngest participants received the lowest doses.
Comparisons
In all studies oxytocin was compared with placebo. In the two studies based on continuous intravenous administration of oxytocin, saline was used as a placebo. In the five studies based on intranasal administration of oxytocin, saline was used as a placebo in one study, whereas three studies used an identical placebo containing all the ingredients except oxytocin; in one study the composition of the placebo was not specified.
Outcomes
Outcomes were either dichotomous or continuous. Five studies provided effect sizes for the primary outcome, but they were too dissimilar to allow for any meaningful comparison.
Scales
Validated scales were used to make the diagnosis and estimate IQ. Some of the outcome measures were created ad hoc.
Excluded studies
Eleven studies did not meet the criteria for inclusion in this review, because they, too, were reviews (n=2); they were mentioned in an abstract for a congress, with not enough details to evaluate the outcome of the study (n=1); RCTs were not on oxytocin (n=5); they assessed oxytocin effects in healthy subjects (n=2), or dealt with the genetics of oxytocin (n=1).
Risk of bias in the included studies
Overall, the studies had a medium to high risk of bias (Table 2). The randomization procedure was rarely described. Two studies only provided details on allocation concealment. The blinding of participants and assessors was claimed but never tested, except in Guastella et al. (2010), for participants only, and in Dadds et al. (2013), who also tested the experimenter. All studies reported data by group according to the randomization, but it was unclear whether there were missing outcome data. In many cases, outcomes were presented in graphic form, or the authors only provided statistical tests and p values, which prevented the numerical summarization of the outcomes.
The risk of bias has been expressed as the number of bias items presented by each study and as a percentage across all the included studies.
Other biases
No study provided an a priori power analysis. No study had a sample size large enough to detect a priori medium effect sizes, which might be detected still by chance in small sample studies. All the studies reported details on the diagnostic criteria and how the diagnosis was achieved. None reported information on the psychometric properties of the tool used to assess the outcomes. The occurrence of drop outs was specified in two studies. Five out of seven studies reported side effects that occurred during the administration of the drug (Table 3).
Effect of interventions
Sometimes studies had multiple outcomes, which, unfortunately, were too disparate to allow a meta-analysis of the findings.
Three studies evaluated the effects of oxytocin on restricted and repetitive patterns of interests and activities. Hollander et al. (2003) found a statistically significant reduction in repetitive behaviors following oxytocin infusion in comparison with placebo infusion over 240 minutes in 15 subjects with ASD. Overall, 13 patients (86%) showed a decrease in repetitive behavior after oxytocin as against 6 (40%) with placebo. Anagnostou et al. (2012) found only a trend reduction in repetitive behaviors such as stereotypy and self-injury, measured with the Repetitive Behavior Scale – Revised, after 6 weeks of oxytocin versus placebo in 19 adults with ASD, with medium effect size (d=0.64). Dadds et al. (2013) found no statistically significant change in repetitive behavior or in children's autistic mannerisms.
Five studies evaluated the effects of oxytocin on communication and socialization deficits.
Three studies evaluated the effects of oxytocin on eye gaze. Andari et al., (2010) found statistically increased eye gaze, measured with a computerized apparatus, after acute intranasal administration of oxytocin in 13 subjects with ASD, with medium effect size (d=0.57). Hall et al. (2012) found significantly increased eye gaze, measured with a paper and pencil method, after acute intranasal administration of oxytocin in eight males with Fragile X syndrome, with large effect size (η2=0.49). Dadds et al. (2013) evaluated child eye contact during parent–child interaction by means of video microcoding and the global coding of observations. They found an increase by time (from day 1 to day 5) in the child eye contact in both the placebo group and the oxytocin group, with no effect of treatment.
Four studies investigated emotion recognition. Hollander et al. (2007) found improved affective speech recognition, measured with a paper and pencil method, following oxytocin infusion in comparison with placebo infusion over 240 minutes in 15 subjects with ASD. Guastella et al. (2010) found a statistically improved performance on the Reading the Mind in the Eyes Test (Baron-Cohen et al. 2001) after acute intranasal administration of oxytocin, with low effect size (d=0.24) and with greater improvement in the “easier” than in the “harder” items (distinction based on the probability of correctly identifying the target item). Anagnostou et al. (2012) found significant improvements on the Reading the Mind in the Eyes Test after 6 weeks of oxytocin versus placebo in 19 adults with ASD, with high effect size (d=1.2). Dadds et al. (2013) found increased accuracy by time (from day 1 to day 5) on the emotion recognition task (UNSW Facial Emotion task) in both the placebo group and the oxytocin group, with no major effect of treatment.
One study measured cooperative behavior. Andari et al. (2010) found increased discrimination in cooperative behavior, as measured with a computerized apparatus, after acute intranasal administration of oxytocin in 13 subjects with ASD, with large effect size (Mann–Whitney U test: z=1.99, equal to r=0.55).
Two studies evaluated the global effects of oxytocin on the clinical status of subjects with ASD. Dadds et al. (2013) found a decrease by time in diagnostic severity in both the oxytocin and the placebo groups after 4 days of treatment administered once a day, with no main effect of treatment. Anagnostou et al. (2012) found no significant improvement on the CGI or the DANVA, a measure of expressive and receptive ability to use and decode facial expressions and other aspects of nonverbal communication in a testing situation, after 6 weeks of oxytocin versus placebo in 19 adults with ASD.
Completion of treatment
Information on treatment completion was not available in the acute administration studies. In the 4 day treatment study, there were four dropouts, equally represented by group. In the 6 week treatment study there were two dropouts, with no indication as to whether these were in the oxytocin or in the placebo group.
Side effects
Five studies reported details on the occurrence of side effects. Overall, oxytocin was well tolerated and no adverse events requiring medical intervention or hospitalization were reported. When present, side effects were generally rated as mild (see Table 1 for details).
The administration method or the duration of treatment did not impact on safety. In the Hollander et al. (2003) study based on continuous intravenous administration of oxytocin, infusion had no significant effects on blood pressure, pulse, or temperature. In the 4 day treatment study based on intranasal administration of oxytocin, no effects were found on systolic and diastolic blood pressure or heart rate (Dadds et al. 2013). In the 6 week treatment study, based on intranasal administration of oxytocin, an electrocardiogram and weight measurements were done at baseline and at the week 6 visit (Anagnostou et al. 2012) to check the blood test including blood count, electrolytes, liver and renal function, and osmolality. No clinically important differences were reported between oxytocin and placebo in blood count, electrolytes, liver/renal function, and osmolality, and no abnormal electrocardiograms emerged.
Discussion
RCTs of oxytocin interventions in patients with ASD yielded potentially promising findings in neuropsychological measures of emotion recognition and eye gaze. Compared with placebo, the effectiveness of oxytocin varied from low to large effect size. Most findings were of medium effect size. Most reproducible findings were on eye gaze and emotion recognition, two core features of social cognition that were found impaired in people with ASD (Elsabbagh et al. 2012; Sucksmith et al. 2013). The effects of oxytocin on repetitive behaviors were positive after acute administration, but only a trend toward reduction was found in the 6 week treatment study. Only one study found an increase in discrimination in cooperative behavior after acute administration of oxytocin, and the finding needs replication (Andari et al. 2010). Only one study reported negative findings on repetitive behaviors, eye contact, emotion recognition, and global severity of symptoms, and this was a 4 day treatment trial based on once-daily intranasal administration of oxytocin (Dadds et al. 2013). This study looked at pre-post changes in outcome measures following multiple exposures to oxytocin combined with social interaction intervention, whereas prior studies had tested the effects of the drug while participants were still under the influence of oxytocin.
To date, the only RCT assessing the effectiveness of oxytocin on the global clinical status of subjects with ASD after a short-term (6 weeks) treatment was largely negative (Anagnostou et al. 2012). The results of the 6 week treatment study were congruent with the results of an open label 7 month treatment study on eight males with ASD (age range: 10–14 years; IQ range: 20–101), who were scheduled to receive intranasal oxytocin (up to 24 IU/dose, six puffs/dose twice a day) and showed no statistically significant improvement on the Aberrant Behavior Checklist (Aman et al. 1985) or the Child Behavior Checklist (Achenbach 1991), despite marginal improvement on the Autism Diagnostic Observation Schedule – Generic (Tachibana et al. 2013). No statistically significant effect of oxytocin on diagnostic severity measured with the CARS and the OSU Autism Rating Scale-DSM IV was found in 38 males with high functioning ASD after a 4 day RCT with once-a-day intranasal administration (Dadds et al. 2013). As intranasally administered oxytocin has a short half-life (<2 hours), the once-daily administration may be not adequate to produce meaningful clinical effects.
Overall completeness and applicability of evidence
The positive findings in this review are from small-sample pilot studies, designed to test a proof-of-concept hypothesis based on animal and healthy human studies (Bartz et al. 2011; Modi and Young 2012). All studies but two were crossover trials testing the effects of acute administration of oxytocin. No firm conclusion can be drawn about the stability of these findings after medium- to long-term administration. To date there is evidence from only one study that the improvement in emotion recognition is maintained, and even increased, after a 6 week treatment with intranasal oxytocin (Anagnostou et al. 2012). The decrease of repetitive behaviors observed after acute administration of oxytocin was not maintained, with the exception of a trend observed after the 6 week treatment with the compound. The extent to which the subjects included in these studies can be considered representative of the population of people with high functioning ASD is unknown, as only one study included a consecutive sample of patients, and it was on males with Fragile X syndrome (Hall et al. 2012). Heterogeneity of ASD samples, both among and within studies, is a major problem in ASD research, hampering the generalization of the findings.
The risk of bias was medium to high in many studies. No study had a sample large enough to detect medium or small effect sizes. Some of the reported findings could be chance findings that favored the publication of the study because of the well-known prejudice in favor of positive results (Rosenthal 1979; Easterbrook et al. 1991). Another important limitation to the generalization of the evidence is the impossibility of cumulating results, because of their heterogeneity.
Quality of the evidence
The quality of evidence, assessed according to the GRADE method, may be judged moderate at the most. All studies were RCTs, but the risk of bias was medium to high (i.e., serious to very serious, according to the GRADE method), results were inconsistent, there was some indication of imprecision in the findings (no effect size could be calculated for some outcomes), and publication bias was possible. Effect sizes were rarely large, and confounding factors (sex, age, IQ) were rarely taken into account. There is a general need for further investigation on the topic, but the findings are promising so far.
Implications for practice
The results of these seven RCTs indicate that the acute administration of oxytocin may produce potentially promising effects in neuropsychological measures that are related to the core dysfunctional symptoms of ASD, in particular repetitive behaviors and some indicators of dysfunctional social cognition (eye gaze and emotion recognition). The improvement in social cognition was maintained after short-term (6 weeks) administration of oxytocin, but the global clinical status of the patients was not affected (Anagnostou et al. 2012).
Overall, oxytocin was well tolerated and the side effects, when present, were generally rated as mild. Drowsiness and headache occurred under oxytocin and placebo with the same frequency; restlessness, increased irritability, and increased energy occurred more often under oxytocin. Overall, safety after medium- to long-term use cannot be extrapolated by short-term studies. In studies based on intravenous infusion of oxytocin in women to induce labor, for postpartum care, or to enhance lactation, cardiovascular changes (tachycardia or bradycardia), nausea, vomiting, and headaches, and, sometimes, water intoxication were reported to be common (MacDonald et al. 2011). Less evidence is available on intranasal oxytocin. A systematic review of 38 research studies investigating the central effects of intranasal oxytocin conducted between 1990 and 2010 on 1529 subjects (males: 79%) found that 18% of the participants reported mild side effects, which did not differ between oxytocin and placebo (MacDonald et al. 2011). Side effects specifically related to the route of administration (e.g., nasal irritation and/or dry mouth/throat) were reported by 3% of participants; typical oxytocin side effects, such as light-headedness, drowsiness, and/or headache, were reported by 6%; some pharmacological, potentially therapeutic actions of oxytocin, such as increased calmness/euphoria, feeling more comfortable, or having more energy, were reported by 5% of the sample (MacDonald et al. 2011). Interestingly, participants were in general unable to state accurately whether they had received oxytocin or placebo. This evidence was largely drawn from studies conducted on healthy samples, and based on acute challenge. Generalization of this evidence to medium- or long-term treatment of people with ASD is premature. An open-label study on eight males with ASD (age range: 10–14 years; IQ range: 20–101) who were scheduled to receive intranasal oxytocin (up to 24 IU/dose, six puffs/dose twice a day) reported no remarkable side effect in the sample or changes in serum or urine osmolarity over 7 months of treatment (Tachibana et al. 2013). Further studies are necessary to carefully estimate the safety of long-term administration of intranasal oxytocin in people with ASD.
Based on the available evidence, heart and cardiovascular conditions and neurological disorders such as epilepsy should be considered in the exclusion criteria of future trials, given the known effects of oxytocin on the heart rate and its water-retention and antidiuretic effects. Screening for allergies is also advisable, and for pregnancy of female participants as well.
There is evidence that nasal delivery methods do not always produce consistent responses across individuals and contexts (Guastella and MacLeod 2012). Individual differences in nasal cavity structure and in the environment, and the administration methods can greatly influence transmucosal absorption (Guastella et al. 2013). The ingredients of nasal sprays and the bottle design are also likely to influence potential for absorption (Guastella et al., 2013). Patients with cognitive deficits might have some difficulty in understanding the instructions for use of a spray. The use of practice spray before randomization was suggested in RCTs testing the repeated administration of the drug (Guastella et al. 2013).
Implications for research
The mechanisms by which oxytocin produces its effects on human behavior are still unknown. Most behavioral effects of oxytocin are believed to depend on its release from centrally projecting neurons, which are located in the paraventricular nuclei and in the supraoptic nuclei of the hypothalamus, where oxytocin is synthesized (Meyer-Lindenberg et al. 2011). In rodents, centrally administered oxytocin favors attachment bond development, contact-seeking, and social memory (Popik et al. 1992; Witt et al. 1992; Ferguson et al. 2000). In animals, centrally administered oxytocin also possesses anti-stress effects, and diminishes stress-induced adrenocorticotropic hormone (ACTH) and corticosterone release (Windle et al. 2004). Oxytocin was also found to increase levels of serotonin in the brain (Pfister and Muir 1989), a mechanism that is likely involved in its anxiolytic effects (Guastella et al. 2009; Yoshida et al. 2009).
Oxytocin sets the rewarding properties of sexual behavior and sexual preferences by interacting with the mesolimbic dopaminergic pathways (Melis and Argiolas 2011), and it might increase the rewarding properties of social stimuli in people with ASD, as well. The oxytocin system is known to interact with the dopaminergic system (Liu and Wang 2003). There is some overlap in the distribution of oxytocin and dopamine receptor binding sites (Smeltzer et al. 2006). The kind of affiliative behavior that is modulated by oxytocin is related to changes in the dopaminergic reward pathways (Skuse and Gallagher 2009), and oxytocin was found to modulate activity in brain areas related to the dopaminergic reward system (Strathearn et al. 2009).
Overall, oxytocin might produce its effects in humans by either increasing the rewarding properties of social stimuli (Burkett and Young 2012; Sanna et al. 2012), or decreasing anxiety about social cues (a thorough discussion on this topic can be found in Churchland and Winkielman 2012).
In people with generalized social anxiety disorder, acute intranasal oxytocin (24 IU) reduced amygdala hyperactivity caused by the presentation of threatening stimuli (fearful face), and also decreased medial prefrontal hyperactivity caused by negative stimuli (sad faces) (Labuschagne et al. 2010, 2011). Reduced amygdala activation in response to facial expressions (regardless of the emotion displayed) was reported among healthy men after oxytocin administration compared with placebo administration (Domes et al. 2007a). This was paralleled by a functional decoupling of the amygdala from brain stem regions involved in fearful arousal and behavior (Kirsch et al. 2005). The amygdala is involved in the elaboration of social information conveyed by eyes, faces, or biological motion (Adolphs and Spezio 2006), and in calculating and updating social orienting values (Klein et al. 2009). Decreased anxiety about social stimuli might partially explain some of the purported “social effects” of oxytocin.
However, oxytocin might also increase the salience of the stimuli by interacting with dopaminergic pathways (Skuse and Gallagher 2009; Sanna et al. 2012). Such effects might be gender sensitive, as estrogens facilitate social recognition, possibly by acting on oxytocin and the synthesis and release of its receptor (Gabor et al. 2012). In women, increased amygdala reactivity to threatening or fearful scenes was found after oxytocin administration, compared with placebo (Domes et al. 2010; Lischke et al. 2012). The extreme male brain theory of autism posits that people with ASD are impaired in empathy and related functions because of excess exposure to fetal testosterone (Baron-Cohen 2010). Excess fetal testosterone would result in an imbalance of sex hormones, with impairment of sex-hormone-dependent functions. If oxytocin-related salience to social stimuli is impaired in ASD, amygdala reactivity to oxytocin is expected to be abnormal in ASD. In a randomized, placebo-controlled study on 14 adults with Asperger syndrome, decreased activity in the right amygdala, fusiform gyrus, and inferior occipital gyrus during face processing was found after placebo, but activity in the right amygdala increased after oxytocin (Domes et al. 2013).
It should be borne in mind that many findings from studies conducted in healthy humans on social tasks have medium effect sizes (e.g., Van Ijzendoorn and Bakermans-Kranenburg 2012). Oxytocin is likely to produce effects related to a defective system (altered polimorphisms in the oxytocin receptor), or indirect effects (modulation of anxiety or of the salience/rewarding properties of the stimuli). The effectiveness of oxytocin in ASD is expected to have medium to low effect sizes. Future studies should be powerful enough to detect medium effect sizes, which rarely occurred in the studies conducted so far.
Another caveat is the fact that oxytocin is expressed and synthesized in both central (brain) and peripheral sites, including the heart, the thymus, the gastrointestinal tract, the uterus, the placenta, the amnion, the corpus luteum, and the testes (Kiss and Mikkelsen 2005; Gordon et al. 2011). The interactions of intranasal administration of oxytocin with these peripheral sites are still unknown. Some concern was raised about generalization from short-term studies to long-term effects. A recent long-term study of intranasal oxytocin in the prairie vole, a socially monogamous rodent that is often used as an animal model to screen drugs that might have therapeutic potential for social disorders, found that long-term developmental treatment with oxytocin may be detrimental (Bales et al. 2013). Albeit very preliminary and in need of replication, these results challenge short-term effects documented by previous studies. Therefore, human long-term studies about the impact of oxytocin on behavior are needed before clinical recommendations can be made.
Conclusions
RCTs of oxytocin interventions in autism yielded potentially promising findings in measures of emotion recognition and eye gaze, which are impaired early in the course of the condition and might disrupt social skills learning in developing children. Both the acute and short-term challenges indicate that oxytocin is well tolerated in people with ASD, but evidence comes from samples with an excess of male participants. Future studies should be better powered to estimate outcomes with medium to low effect sizes, and should attempt to enroll female participants as well. The risk of bias should be minimized, with better attention paid to allocation concealment and blinding of assessors and participants. Whatever the results of future studies on oxytocin, it is unlikely to prove a “cure” for autism. Future studies should, rather, focus on the use of oxytocin as an adjunct to psychosocial interventions, which can improve social and other skills as well as the quality of life of the people affected by ASD and their families.
Clinical Significance
This is the first systematic review of randomized, placebo-controlled trials of oxytocin interventions in ASDs. Seven randomized, placebo-controlled trials have been conducted so far, and included 101 subjects with ASDs (males=95) and 8 males with Fragile X syndrome. Most reproducible findings were improvements in eye gaze and emotion recognition, two core features of social cognition that were found impaired in people with ASDs. Effects of oxytocin on repetitive behaviors were positive after acute administration, but only a trend toward reduction was found in a 6 week treatment study. Overall, oxytocin was well tolerated and when present, side effects were generally rated as mild. Future studies should address the mechanism by which oxytocin produces its effects, to tailor the treatment to the patients' needs. Future studies should be also better powered to estimate outcomes with medium to low effect size and they should try to enroll female participants, who were rarely considered in previous studies. Risk of bias should be minimized. Human long-term administration studies are necessary before clinical recommendations can be made.
Footnotes
Disclosures
No competing financial interests exist.