
Abstract
Objective:
The purpose of this study was to determine if the known side effects of lithium in adults may be generalized to younger patients with psychiatric disorders.
Methods:
A retrospective naturalistic study design was used. Data were collected from the database of a tertiary pediatric medical center covering the years 1994–2010. Included were patients hospitalized for bipolar and non-bipolar disorders and treated with lithium, alone or in combination with other medications. The electronic medical files were reviewed for changes in thyroid and kidney function and for hematological parameters during the course of treatment.
Results:
Sixty-one patients 12.5–20.4 years of age (mean 16.94±1.66) met the study criteria: 33 with bipolar disorder and 28 with a non-bipolar disorder. Mean duration of lithium treatment (mean lithium blood level, 0.73±0.24 mEq/L) was 193.68±254.35 days. Mean levels of thyroid-stimulating hormones (TSH) rose significantly from baseline to last measurement (3.16±2.68 vs. 1.52±0.92 mU/L; paired t=−5.19, df=50, p<0.001); in 25% of patients, TSH levels at the last measurement were above normal (≥4 mU/L). Only one patient developed TSH values >10 mU/L (the threshold considered clinically significant). Positive correlation was found between pre- and posttreatment TSH levels (Pearson's r=0.60; n=51, p<0.05). White blood cell count (WBC) also increased significantly following lithium treatment (7195±2151 vs. 7944±2096 cells/mm3; t=2.83, df=60, p=0.006). No significant changes were noted in serum creatinine levels. There was no difference in these parameters between patients treated with lithium alone or in combination with other medications.
Conclusions:
Lithium treatment in adolescents with bipolar or non-bipolar disorders is associated with a significant increase in blood TSH levels and WBC count. Lithium-treated adolescent inpatients with a high basal TSH level may be at risk of developing pituitary–thyroid axis dysregulation. Therefore, baseline measurement of thyroid functions and serial monitoring throughout treatment are recommended.
Introduction
L
Based on findings in adults, lithium was approved by the United States Food and Drug Administration (FDA) for the treatment of bipolar disorder in adolescents ≥12 years of age (Thomas et al. 2011). Lithium's tolerability and safety for short-term treatment in pediatric populations is well established (Findling et al. 2011); however, data on long-term side effects of lithium remain sparse (Findling et al. 2011, 2013). There are few prospective studies on the adverse effects of long-term lithium treatment in bipolar children and adolescents, and they are generally restricted to combination pharmacotherapy studies (Gracious et al. 2004; Pavuluri et al. 2004, 2006; Findling et al. 2013). Recently, Findling et al. examined the long-term effectiveness of lithium for the treatment of pediatric bipolar disorder (Findling et al. 2013). The authors reported that although some patients experienced altered thyroid-related laboratory values during the follow-up, none of them suffered from a thyroid-related adverse event. Renal function was also closely monitored throughout the study, and no significant changes in creatinine clearance were noted (Findling et al. 2013). Considering that children and adolescents with bipolar disorder frequently require long-term treatment, investigating the long-term safety of lithium in pediatric populations is of great importance.
The purpose of the current study was to investigate the long-term effect of lithium treatment on TSH levels, white blood cell (WBC) count, and serum creatinine levels in adolescent inpatients with bipolar and non-bipolar disorders.
Materials and Methods
A retrospective naturalistic study design was used. The data were retrieved from the database of a university-affiliated mental health center and covered the years 1994–2010. Included in the study were patients hospitalized with bipolar or non-bipolar disorders in the adolescent inpatient unit and treated with lithium, either alone or in combination with other medications. The electronic medical files were reviewed for clinical data and for changes in thyroid and kidney function and in hematological parameters during the course of treatment. Patients with missing data were excluded. All the diagnoses were based on the American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria (American Psychiatric Association 1994), using information collected during extensive clinical interviews performed by certified senior child and adolescent psychiatrists, daily observations by nursing staff, and clinical team discussions led by the department director.
The study was approved by the Institutional Review Board. The need for informed consent was waived by the Board because the study was based entirely upon analysis of retrospective anonymous data.
For purposes of the study, we recorded the laboratory values for TSH levels, WBC count, and serum creatinine levels at baseline; before initiation of lithium treatment. In addition, for most patients in the study (n=40), the final lithium, creatinine, WBC, and TSH blood levels were measured prior to discharge from the ward. However, 21 patients continued the follow-up after discharge. For them, the last available blood tests taken during follow-up were used for the lithium, creatinine, WBC, and TSH analyses. For all patients, the last measure; namely, the one taken when they were on a stable maintenance lithium dose, was defined as the end-point.
Lithium was administered twice daily: Morning and evening. This particular blood sample was taken from all participants, in the morning at ∼8:00 a.m., prior to their receiving the morning dose of lithium. Namely, the measurement was done ∼12 hours after the patients were administered the previous dose of lithium (the evening dose) and, therefore, this measurement was taken during the interdose trough period. It should be noted that all other measurements were done at the same time as the lithium.
TSH was measured using the Advia Centar Immunoassay (Bayer Corp., Pittsburgh, PA) (normal range, 0.4–4 mU/L), WBC count was measured with the Advia 2120/120 Hematology System (Bayer Corp.) and the Beckman Coulter LH750 Analyzer (Beckman Coulter, Inc., Brea, CA) (normal range 4800–10,000/mm3), and creatinine was measured with the Olympus AU2700 Chemistry Analyzer (Olympus, Melville, NY) or Roche-Hitachi 747 Chemistry Analyzer (Roche, Basel, Switzerland) (normal range 0.6–1.2 mU/L).
Statistical analyses
Means and standard deviations were calculated for all laboratory parameters. Values were compared between patients with bipolar and non-bipolar disorder using the Student's paired or independent sample t tests or Mann–Whitney test, as appropriate. Associations between laboratory values and demographic and clinical variables were analyzed using the χ2 test or Pearson's correlation, as appropriate. The level of significance was set at 5%. All analyses were two tailed. The Statistical Package for the Social Sciences was used to create a database and perform the statistical analyses (SPPS, version 17 for Windows Inc., Chicago, IL).
Results
Participants
One hundred and eight consecutively admitted patients 12–24 years of age (77 were <18 years of age) were treated at our center during the study period with lithium for bipolar or non-bipolar disorder. Forty-seven patients were excluded from the study because of missing data at end-point, thus resulting in a final study group of 61 patients (46 of them <18 years of age). WBC count data were available for all participants, data for serum creatinine levels were available for 54, and for TSH levels were available for 51. There were no statistically significant differences between the study group and the patients excluded from the study with regard to gender or age distribution, diagnoses, length of hospitalization, or ethnicity (data not shown).
The mean age of the participants was 16.94±1.66 years (range: 12.5–20.4, with a normal distribution) (Fig. 1). Mean length of hospitalization was 107.69±108.15 days (range, 4–533, no normal distribution) (Fig. 2), whereas the mean interval between the two blood tests (basal and endpoint) was 193.68±254.35 days (range, 5–991, no normal distribution). As for some patients the end-point blood sample was taken after discharge from the ward, the mean length of hospitalization was shorter than the mean duration of treatment with lithium.

Age distribution of the clinical sample.
Distribution of length of admission (days) in the clinical sample.
Demographic, clinical, and baseline laboratory data
Thirty-three patients were diagnosed with bipolar disorder and 28 with a non-bipolar disorder, including schizoaffective disorder, dysthymia, conduct disorder, and personality disorder. The bipolar group was significantly older than the non-bipolar group (17.49±1.25 vs. 16.33±1.89 years, t=2.75, df=59, p=0.008), and had a significantly shorter length of hospitalization (72.73±74.54 vs. 148.89±127.09 days, t=2.90, df=59, p=0.005). There were no significant between-group differences with regard to gender distribution, lithium dosage, lithium blood level, and interval from the first to the last blood tests (Table 1). Baseline (pretreatment) TSH levels were significantly lower in the bipolar group (1.30±0.87 vs. 1.77±0.87 mU/L, unpaired t=2.17, df=42, p=0.03). No significant differences were noted between the two groups in baseline WBC count or creatinine levels (Table 1).
Values are n (%) or mean±SD, as appropriate.
WBC, white blood cells; TSH, thyroid-stimulating hormone.
Treatment
Eleven patients were treated with lithium monotherapy. The remainder received lithium with one (n=34), two (n=14), or three (n=2) additional medications, including typical antipsychotics (levomepromazine, perphenazine, haloperidol, zuclopenthixol, sulpiride, chlorpromazine, thioridazine), atypical antipsychotics (olanzapine, risperidone, quetiapine, ziprasidone), non-lithium mood stabilizers (valproic acid, carbamazepine, lamotrigine), antidepressants (clomipramine), and stimulants (methylphenidate). One patient required treatment with
End-point laboratory values
Mean WBC count increased significantly in all participants (n=61), from 7195±2152 cells/mm3 at the first measurement to 7944±2096 cells/mm3 at the last measurement (t=2.83; df=60; p=0.006) (Table 2). Clinical leukocytosis (WBC count >10000 cells/mm3) developed in seven patient (11%). There was no correlation between lithium blood levels and WBC count (r=0.113; n=61; p=NS).
Values are mean±SD.
WBC, white blood cells; TSH, thyroid-stimulating hormone.
Mean creatinine level (n=54) was 0.84±0.19 mU/L at the first blood test and 0.84±0.18 mU/L at the last blood test; this difference is not statistically significant (t=0.31; df=53; p=NS) (Table 2). Creatinine rose above the normal limit in only one patient (1.2 mU/L). No correlation was found between lithium blood levels and creatinine levels (r=− 0.078; n=54; p=NS).
Mean TSH level (n=51) increased significantly from 1.52±0.92 mU/L at baseline, to 3.16±2.68 mU/L at the last measurement (t=−5.19; df=50; p<0.005) (Table 2).
Thirteen of the 51 patients (25%) had a TSH values above normal (>4 mU/L) at the last measurement. Only one patient developed TSH values >10 mU/L (the threshold considered clinically significant). There was no correlation between lithium and TSH levels (r=0.16; n=51; p=NS), or between duration of lithium treatment and TSH levels (r=0.016; p=NS) (Fig. 3). Also, no correlation was found between TSH and lithium blood levels (r=0.095; p=NS). A positive correlation was found between pre- and posttreatment TSH levels (r=0.60; n=51; p<0.001) (Fig. 4) even when controlling for age, gender, and duration of treatment (partial correlation r=0.69, p<0.0001).
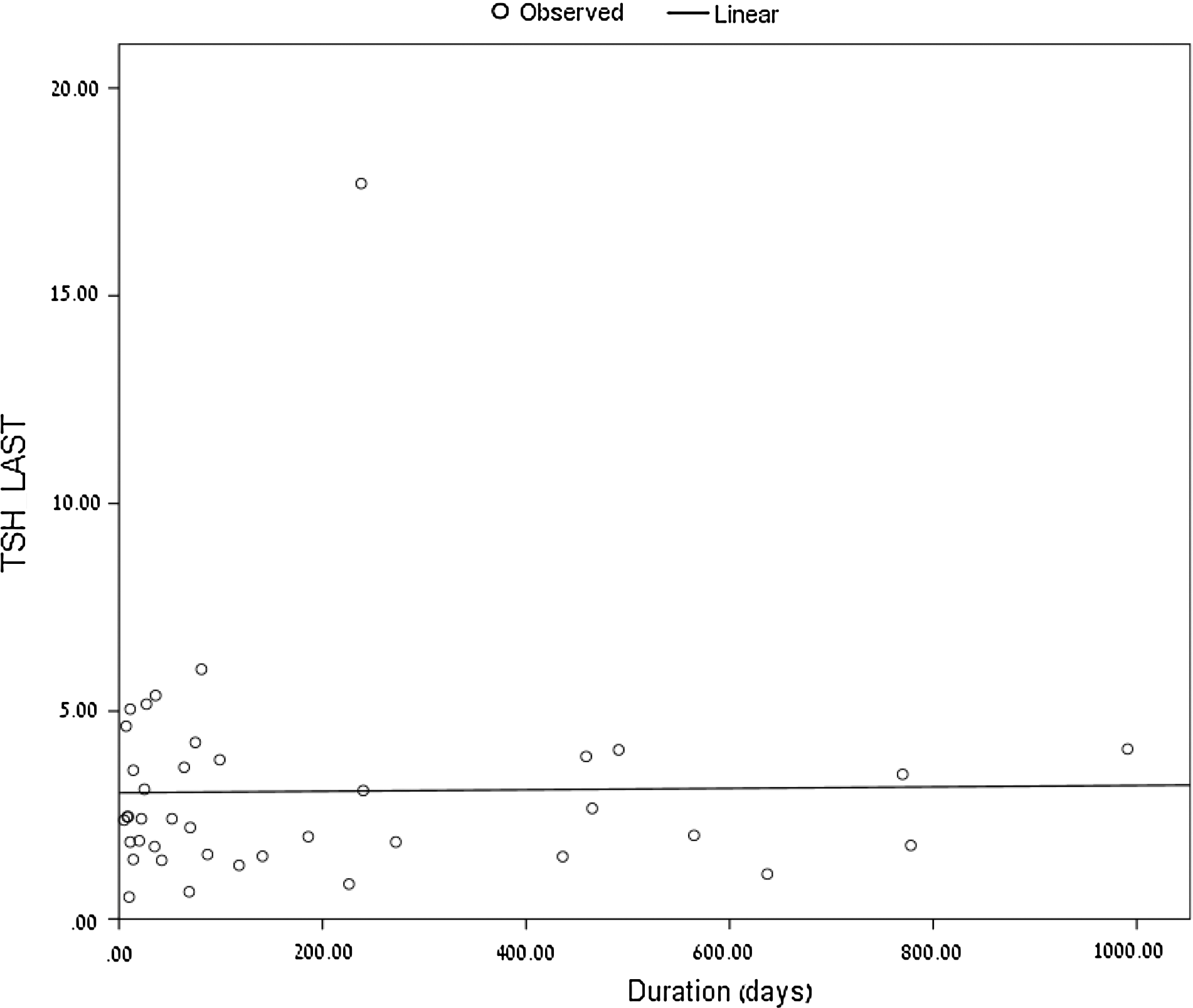
Correlation between duration of treatment (days) and last (end-point) thyroid-stimulating hormone (TSH levels) (TSH_Last; mU/L) (n=40, r=0.0.016, p=NS).
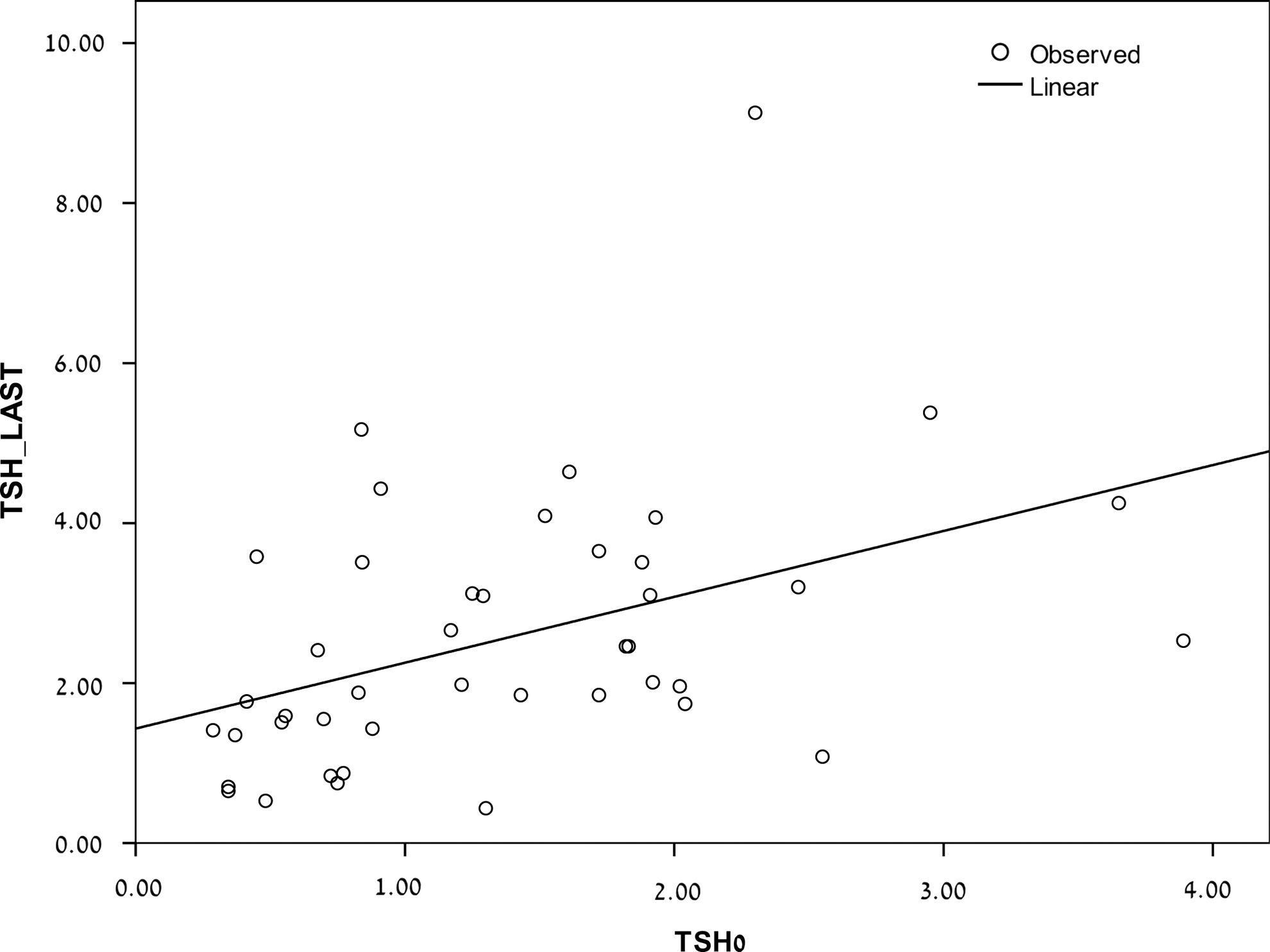
Correlation between first (basal/pretreatment) measurement of baseline thyroid-stimulating hormone (TSH) (mU/L;TSH0) and last (end-point) measurement of TSH (TSH_Last) (n=51, r=0.60, p<0.001).
Multiple linear regression analyses were performed using TSH end-point as the dependent variables, and age, gender, length of treatment, lithium level, and baseline TSH values as the independent variables. The results indicated that two of the variables predicted end-point TSH levels. Namely, end-point TSH levels were predicted by baseline TSH values and gender (F[6, 37]=5.35; p<0.0001; R2 =51%). The standardized coefficients were as follows: gender, β=0.39, p=0.013; baseline TSH values, β=0.68, p<0.001. Therefore, female gender and baseline TSH were positively correlated with end-point TSH, and predicted ∼50% of its value. Other independent variables did not affect the regression.
Dividing the patients into two groups by TSH level at last measurement ([TSH<4 mU/L, n=38] and [TSH ≥4 mU/L, n=13]) yielded a statistically significant difference in mean TSH levels between the two groups at both basal levels and end-point levels. The values obtained in the first measurement were 1.23±0.66 mU/L and 2.38±1.04 mU/L (Z=−3.3; p=0.001), respectively, whereas in the last measurement the values were 2.13±0.97 and 6.16±3.72 mU/L (Z=−5.33; p<0.005), respectively. There were no significant differences between the groups in age or gender distribution, diagnoses, number of medications, lithium blood level, or length of treatment (Table 3).
Values are n or mean±SD, as appropriate.
WBC, white blood cells; TSH, thyroid-stimulating hormone.
Dividing the patients by treatment with lithium monotherapy (n=11) or lithium combined with other medications (n=50), yielded no between-group differences in either TSH levels, WBC count, or creatinine levels (p=NS for all; data not shown).
Discussion
The present study shows that the side effects of lithium, well known in adults, may also occur in adolescents. Speculations that younger children may be more vulnerable to lithium-related side effects than older adolescents have not been confirmed (Thomas et al. 2011).
Thyroid function
According to well-documented evidence in adults, high doses of lithium can interfere with thyroid function and even in low doses inhibit thyroid hormone release from the gland (Kleiner et al. 1999). The reported rate of elevated TSH levels (defined in adults as TSH levels >5 mU/L) in adults treated with lithium is up to 23% as compared with 10.4% in the general population (Kleiner et al. 1999). These effects are often transient or reversible with discontinuation of the drug or initiation of thyroid hormone replacement therapy (Correll and Carlson 2006). Nevertheless, the percentage of lithium-treated patients with high TSH levels increases with time of exposure and does not seem to plateau (Johnston and Eagles 1999; Kleiner et al. 1999). Prevalence studies, largely retrospective, estimated that up to 34% of Western adults with bipolar disorder acquire lithium-induced hypothyroidism (Transbol et al. 1978).
Fewer data on lithium-induced thyroid dysfunction are available for children and adolescents (Gracious et al. 2004; Kafantaris et al. 2004). One 4 week pediatric study reported that lithium treatment induced only minor elevations in serum TSH levels and that those were transient and normalized spontaneously (Kafantaris et al. 2003). However, in a 20 week study in which lithium was administered along with valproic acid, 24% of patients had serum TSH levels of >10 mU/L (Gracious et al. 2004). In a recent randomized controlled trial, mean thyrotropin levels increased significantly, from 2.1 mU/L to 5.2 mU/L in patients treated with lithium (Geller et al. 2012). Findling et al. recently reported that open-label long-term (16 week) lithium treatment was generally safe and well tolerated in their pediatric sample (Findling et al. 2013). Although a few patients experienced clinically significant changes in thyroid-related laboratory values during the 16 week follow-up, none of these patients had from a thyroid-related adverse event. In addition to inhibiting thyroid hormone release, lithium may affect thyroid function by suppressing iodine absorption by the gland, inhibiting tyrosine iodination, and interfering with the action of adenyl cyclase, thereby limiting the production of cyclic adenosine monophosphate (cAMP) (Gracious et al. 2004). Therefore, its use has special implications in the pediatric population. In addition to the physical and mental effects noted in adults, chronic clinical hypothyroidism in younger patients may cause enlargement of the sella turcica and disturbances in sexual maturation and gonadal function, as well as abnormal musculoskeletal structure and function that may result in short stature and muscle hypertrophy (Gracious et al. 2004).
In our sample, TSH levels were significantly higher at the end-point of the lithium treatment course than at baseline. Moreover, they rose at end-point above the normal range, defined in our laboratory as >4 mU/L, in 25% of patients, and that is similar to the rate reported in adults (up to 23%) (Kleiner et al. 1999). Clinical guidelines however, suggest treatment with synthetic thyroid hormone only in cases in which TSH is >10.0 mU/L (Kleiner et al. 1999). In our study, there was only one such patient at end-point, which is a lesser rate than that reported for bipolar children and adolescents treated with both lithium and divalproex sodium (Gracious et al. 2004).
Factors increasing susceptibility to lithium-induced suppression of thyroid gland activity in adults include duration of exposure to lithium, rapid cycling, presence of autoimmune Hashimoto's thyroiditis or circulating anti-thyroid antibodies, cigarette smoking (a risk factor for Hashimoto's thyroiditis), family history of thyroid disease, being female (a risk factor of Hashimoto's thyroiditis), and taking valproic acid in addition to lithium (Correll and Carlson 2006). Gender distribution was similar among the patients with and without elevated thyrotropin, but we did find in the regression analysis that female gender predicted higher TSH end-point values. Therefore, female gender may serve as a risk factor for thyroid abnormalities in lithium-treated young patients, a finding that is inconsistent with some studies (Johnston and Eagles 1999), but that is consistent with others (Gracious et al. 2004). Some researchers suggested that gender may be a risk factor insofar that in the general population, autoimmune thyroid disease occurs more frequently in women (Lazarus 2009). Subsequently, this difference could be expected in a younger population.
Lithium blood levels were also similar in the two groups, although earlier studies reported a dose-dependent effect, with higher lithium levels posing a greater risk of hypothyroidism in young patients. We also found no between-group differences in the use of co-medications or diagnoses, and no correlation of TSH level with age. The mean duration of lithium exposure was similar in the inpatients with thyroid abnormalities and in those without.
Interestingly, we observed significant differences in mean TSH at baseline between patients with and without elevated thyrotropin, and positive correlation between TSH levels at first and last measurements. These findings agree with an earlier pediatric study (Gracious et al. 2004) whereby higher baseline TSH levels were predictive of elevated TSH levels at end-point. The same authors noted that children and adolescents with high baseline TSH levels may be at an increased risk of subclinical hypothyroidism or lithium-induced hypothyroidism. However, this issue should be addressed with caution, given the small size of our sample and the large degree of overlap in individual TSH values.
The significantly lower TSH level in the patients with bipolar disorder than in patients with non-bipolar disorders in our study is in line with the cumulative evidence of the relevance of hypothalamic–pituitary–thyroid (HPT) axis dysfunction to the pathophysiology and clinical course of bipolar affective disorder (Chakrabarti 2011). Children and adolescents with bipolar disorder may have a pretreatment HPT axis dysfunction, and clinicians should bear this in mind when considering lithium treatment.
Hematological abnormalities
Therapeutic doses of lithium lead to fairly reproducible hematopoietic effects, most notably transient leukocytosis (Oyesanmi et al. 1999). This is a true proliferative response, not simply a shift of cell populations to the circulatory pool (Oyesanmi et al. 1999). Possible underlying mechanisms are modulation of granulopoietic cells, elevation of plasma cortisol, and stimulation of leukocyte precursors (Ozdemir et al. 1994). Our finding of a lithium-induced increase in WBC count not exceeding 1.5 times the normal range is in agreement with studies in adults (Ozdemir et al. 1994). The leukocytosis was not related to serum lithium levels. Because of the retrospective study design, we could not determine if the hematological effects of lithium are reversible.
Creatinine
Serum creatinine measurement is a quick, valid, and reliable mean of estimating the glomerular filtration rate (GFR). According to a recent meta-analysis (Paul et al. 2010), adults exhibit a small non-statistically-significant rise in serum creatinine level in the first years of lithium treatment, which becomes statistically significant with increasing duration of treatment. Although lithium-associated increase in serum creatinine is small and of questionable clinical significance, routine monitoring of renal function in patients receiving lithium is essential (Paul et al. 2010). Findling et al. also recently reported that non-significant changes in creatinine clearance were found during their study, but none of the patients discontinued treatment as a result of decreased renal function (Findling et al. 2013). In our study, possibly because of the short duration of treatment, no increase in creatinine levels was found. The difference in creatinine levels between boys and girls can be most probably attributed to the differences in body mass index between the genders (Uemura et al. 2011). It should be noted that according to several reports in adults, women seem to have a poorer concentration capacity, thus increasing their risk for lithium-induced renal toxicity (Gelenberg et al. 1987). We did not detect gender differences regarding vulnerability to lithium.
Limitations
This study has several limitations. Diagnoses were not made using standardized instruments and there was no control group. Because of the study's retrospective nature, we were unable to collect data on several important measures, such as thyroid hormones. In addition, our sample shrank, as we had to exclude some subjects who were missing data critical to this study. Even among those who were included, some were missing data on family history of thyroid disease, including autoimmune thyroid disease, and other parameters. It is possible that we did not find any relationships between lithium concentration and clinical data because of: 1) Not testing at consistent time points (the timing of the last blood tests varied among the subjects as it depended upon length of hospitalization or length of follow-up); 2) having lithium levels being relatively low (Findling et al. 2011); 3) of the range of lithium concentrations in the blood being fairly narrow, thereby making the examination of such relationships difficult; and 4) the study duration being insufficient for true long-term assessment. We were also unable to report how many subjects developed pathological TSH or creatinine levels during our follow-up period, as we collected data at only two time points (i.e., basal and end-point). It is possible that some subjects developed high TSH or creatinine levels during the study period that normalized prior to the final blood test. However, the strength of our study is in the unique age group investigated and the relatively long-term follow-up.
Conclusions
Lithium treatment in adolescents with bipolar or non-bipolar disorders is associated with a significant increase in TSH level and WBC count. Lithium-treated adolescent inpatients with a high basal TSH level may be at risk of pituitary–thyroid axis dysregulation. Therefore, baseline measurement of thyroid functions and serial monitoring throughout treatment are recommended.
Clinical Significance
Clinicians treating adolescents with bipolar or non-bipolar disorder with lithium should be alerted to the relatively high risk of the patients developing TSH abnormalities early in the course of treatment. This is particularly true for patients with high basal levels of TSH. To prevent complications, patients need to undergo comprehensive examination of thyroid function at baseline, with follow-up every 2–3 months after initiation of treatment. If TSH is elevated, blood T4 and T3 levels should be measured and physical examination performed to check for signs and symptoms of clinical hypothyroidism.
Recent years have witnessed a sizeable increase in the use of psychotropic medications in the pediatric population, including the off-label use of the growing number of medications receiving FDA approval (Vitiello 2001). It is essential that they be carefully evaluated for tolerability and safety for the appropriate selection and sequencing of pharmacotherapy and proper counseling of patients and families.
Footnotes
Disclosures
No competing financial interests exist.