
Abstract

To The Editor:
O
It is well known that higher SSRI dosages are needed to obtain positive treatment responses in OCD compared with dosages needed in depression. Furthermore, SSRIs are metabolized more rapidly in young patients than in adults, which can also cause the dosage requirements to be relatively higher, that is, up to 80 mg daily of fluoxetine (Bezchlibnyk-Butler and Virani 2007). When SSRIs are given, the beneficial effects are typically expected to begin only after 4–10 weeks of treatment, and, therefore, the effect should only be judged after 8–12 weeks of treatment have elapsed (Wagner et al. 2003; Findling et al. 2006).
As SSRIs are the most effective medications for OCD treatment, many molecular genetic association studies in OCD have focused on serotonergic genes. The most frequently studied gene is the serotonin transporter (SERT; SCL6A4), with particular focus on its functional polymorphism, 5-HTTLPR, in the upstream region. Comparison between the S-[short] and L-[long] alleles of 5-HTTLPR shows that the L-allele exerts increased transcriptional activity and increased basal reuptake of serotonin in vitro (Heils et al. 1996; Lesch et al. 1996; Murphy et al. 2008). The L-allele is, therefore, referred to as the gain-of-function variant of the serotonin transporter.
Recent findings have led to the subdivision of the 5-HTTLPR L-allele into the high-functioning LA-alleles and low-functioning LG-alleles. When this new classification is used, ∼5–10% of L-alleles (depending on ethnicity) are deemed low functioning and must be grouped with the S-alleles for comparison purposes (Hu et al. 2006). Additional single-nucleotide polymorphisms (SNPs) on the serotonin transporter (SERT) have also recently been reported to influence functionality of the transporter, that is, rs16965628 with C-allele>G-allele (high>low) and rs25532 with C-allele>T-allele (Wendland et al. 2008).
Case Report
The present report describes the case of a 7-year-old boy (henceforth referred to as P.) with rather severe early-onset OCD, who exhibited an extraordinarily fast positive response to sertraline in a low dose of 25 mg. The boy was first registered at our clinic in May 2009, and the referral letter indicated that, 3 months prior, the boy had started to refuse to eat anything “hard.” The symptom increased with such severity that at the time of referral the boy was not swallowing his own sputum, because of fear of choking. In addition, he had developed cleaning compulsions. Somatic examinations were inconspicuous. A 4 week CBT did not reduce the symptomatology substantially; therefore, 25 mg sertraline was introduced. After only 2 days, significant symptom reduction was observed. After 2 weeks, most of the previously described OCD symptoms had disappeared. For several reasons CBT was implemented again: 1) Because of the guidelines of OCD therapy in which a combination of medication with CBT is the first line therapy for children with OCD (Walitza et al. 2011) and 2) in some cases, CBT is only possible or successful if medication precedes the psychological therapy. Therefore, although there was such a good effect, we implemented CBT again after some weeks of good response to medication (for timeline, see Supplementary Fig. 1) (see online supplementary material at
Genotyping results
Genotyping 5-HTTLPR and the SNPs rs25531, rs16965628, and rs25532 showed that the child was homozygous for the LA-allele of 5-HTTLPR (high-functioning transporter), as well as for rs16965628 with GG (lower-functioning transporter) and for rs25532 with CC (high-functioning transporter) (Fig. 1). Thorough genotyping of all known CYP isoform polymorphisms affecting sertraline metabolism revealed that the boy was homozygous wild-type (normal metabolizing) for CYP2C9*2 (CC), CYP2C9*3 (AA), CYP2C19*3 (GG), CYP2D6*4 (GG), and CYP3A4*2 (TT). For CYP2C19*2, he was homozygous for the mutation AA, which is known to cause defective splicing and an inactive enzyme (Ingelman-Sundberg 2001, 2004) (Fig. 1). Analysis of the two copy number variations (CNVs) on CYP2D6*5 showed that both resulted in two normal copies, and not in a deletion of the gene that causes no enzyme expression.
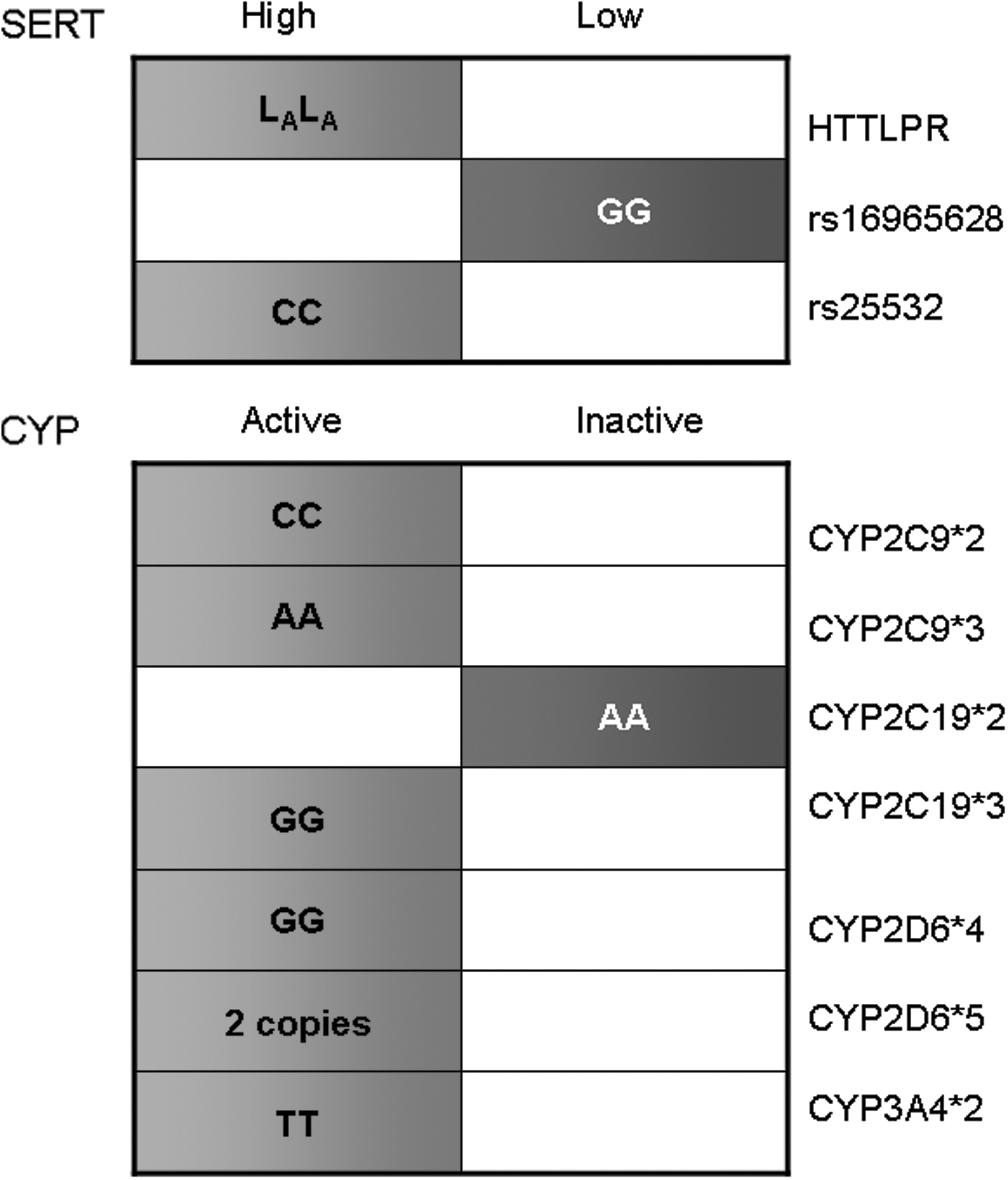
Genotype profile of a 7-year-old boy with early-onset obsessive-compulsive disorder (OCD) for the serotonin transporter (SERT) gene and the cytochrome P450 (CYP) isoforms that are known to metabolize sertraline. Left side, high-functioning SERT or active CYP isoform; Right side, low-functioning SERT or inactive CYP isoform.
Discussion
In this case, we found that a 7-year-old child with early-onset OCD was a carrier of two high-functioning SERT polymorphisms (5-HTTLPR, LALA; rs25532, CC) and one SNP for the low-functioning SERT (rs16965628, GG) (Fig. 1). These results may relate to the patient's very rapid response to a rather low dose of sertraline. Our findings are in accordance with previous observations of SERT genotype effects on SSRI therapy response in depression (Porcelli et al. 2012), and on sertraline therapy response in posttraumatic stress disorder (PTSD) (Mushtaq et al. 2011). The discontinuation syndrome experienced on each occasion after sertraline withdrawal—in which P became restless and anxious and had sleeping disturbances—is also in accordance with previous reports in the literature (Hosenbocus and Chahal 2011).
To rule out possible low drug metabolism through CYP enzymes, we analyzed all major isoforms known to metabolize sertraline, and found that only one isoform was mutated to cause an inactive isoform (and consequently low metabolism), whereas all six gene variants were homozygous for the active enzyme (Fig. 1). Sertraline metabolism occurs through the activity of multiple CYP isoforms rather than by only one isoform; therefore, it has been suggested that no single agent (inhibitor) or single drug-metabolizing enzyme genetic polymorphism could impact the pharmacokinetics of sertraline (Kobayashi et al. 1999; Obach et al. 2005).
One very small study of six poor metabolizers and six extensive metabolizers reported that the polymorphic CYP2C19 might be a major enzyme involved in sertraline N-demethylation (Wang et al. 2001). However, the studies of de Morais et al. (1994) and Obach et al. (2005) show that sertraline metabolism is highly complex, and involves many CYP isoforms, indicating that a series of mutations would be required to definitely cause poor sertraline metabolism. Moreover, a recent study of the therapy response and side effects following treatment of a large OCD cohort with antidepressants investigated associations with the metabolizer status of CYP2D6 and CYP2C19, and found a nonsignificant trend for association of CYP2C19 metabolizer status with response to sertraline (Brandl et al. 2013). In the case reported here, only one isoform was mutated, and all other isoforms were normal, indicating that sertraline metabolism was likely normal in this child, and that the main effect probably came from the SERT genotype. This is also supported by the normal levels of plasma sertraline that were detected in this patient after 2 weeks of therapy.
Limitations
The genotype is certainly not the only etiological factor that could be responsible for the patient's OCD symptomatology. It must be considered that children and adolescents often show a flat dose-response curve, meaning that initial dosages can lead to a positive response (Walitza et al. 2011). However, previous findings in early-onset OCD support the idea that the gain-of-function alleles of 5-HTTLPR are risk factors for OCD (Personal data not yet published). It should also be noted that it is impossible to completely rule out the possibility of a placebo effect in this case report. However, as it was repeatedly observed during a period of >3 years that when P. discontinued his medication, his symptoms returned, we can assume that the beneficial effects were at least partly the result of the sertraline therapy.
Clinical Significance
The results of this case could assist with making the decision whether or not to continue treatment of a child for a longer time if side effects are not observed. The observed repeated discontinuation syndrome indicates that in a highly sensitive patient, such as this case, cessation of sertraline medication should be done with caution. Pharmacogenetic studies of single cases could be helpful in understanding therapeutic effects and, in the best case, could improve efficacy and safety of medication in children and adolescents.
Footnotes
Acknowledgments
We thank our patient and his family. We also thank Miryame Hofmann for her excellent technical assistance.
Disclosures
The patient and his parents gave their consent for this report. The details about the patient have been sufficiently changed such that the patient is unrecognizable. Drs. Grünblatt, Dr. Brezinka, and Tschakarjan have no conflicts of interest or financial ties to disclose. Prof. Dr. Walitza has received lecture honoraria from AstraZeneca, Eli Lilly, and Janssen Cilag in the past 5 years.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.