
Abstract
Background:
Anxiety disorders typically begin in childhood and adolescence and predict risk for many problems throughout life. Although some neuropsychological correlates have been described, more research is needed, particularly in adolescents. This study compares neurocognitive characteristics of anxious adolescents with and without comorbidity to externalizing disorders to those of typically developing comparison (TDC) adolescents and adolescents with externalizing disorders alone.
Methods:
The study included 57 adolescents 12–18 years of age (TDC, n=23; anxiety, n=16; externalizing, n=11; comorbid, n=7). We used a neuropsychological battery to assess eight domains: Orientation, attention, visual perception, memory, arithmetic, language, praxis, and executive function.
Results:
Multivariate analysis of variance revealed a main effect of group in the neurocognitive domains evaluated (F 8,48=2.32, p=0.034, ηp 2=0.279). Post-hoc analysis revealed that executive functions score differed among groups, specifically in the task of verbal fluency (F[df=3]=5.01, p=0.004, ηp 2=0.221), with both the anxious groups (anxiety and comorbid) presenting a lower score than the TDC and externalizing groups. This effect was independent of age, intelligence, and levels of education.
Conclusions:
Verbal fluency is specifically impaired in adolescents with anxiety disorders. This extends results from neuroimaging research implicating prefrontal areas in pediatric anxiety disorder neurobiology, and has potential implications to new therapeutics.
Introduction
A
Some research has begun to characterize information-processing functions in adolescent anxiety disorders (Shechner et al. 2011; Salum et al. 2012). However, most of this research considers the effects of emotion on cognition, and few studies have characterized adolescents with and without anxiety using the types of measures most frequently employed in research on other adolescent mental disorders, such as externalizing disorders and attention-deficit/hyperactivity disorder (ADHD) in particular (Nichols and Waschbusch 2004; Stefanatos and Baron 2007; Rizzutti et al. 2008).
Previous findings on adolescent anxiety disorders suggested dysfunctions in some aspects of memory and visuomotor integration (Frost et al. 1989; Pine et al. 1999; Toren et al. 2000; Vasa et al. 2007; Micco et al. 2009). Moreover, impairment has also been found in some aspects of executive functions such as inhibitory control (Micco et al. 2009) and cognitive flexibility (Toren et al. 2000). Nevertheless, few findings have been replicated (Gunther et al. 2004), possibly because of methodological differences among these studies, emphasizing the need for further research (Toren et al. 2000; Vasa et al. 2007; Micco et al. 2009).
A few specific deficiences in prior studies could be addressed in such research. First, broad neuropsychological functions such as orientation, visual perception, arithmetic, language, and praxis are rarely examined in the literature, in conjunction with attention, memory, and executive functions. Second, most studies are restricted to referred or currently treated subjects and thereby vulnerable to various sampling biases. Finally, because few studies compare findings in anxiety with other psychiatric disorders, disorder specificity has not been evaluated.
The present study assessed a broad range of neurocognitive functions in a community sample of unmedicated young adolescents with a range of psychiatric problems, as well as in typically developing comparison adolescents. Our aim is to compare adolescents with anxiety disorders and externalizing disorders, and healthy adolescents, using measures of eight neurocognitive functions: Orientation, attention, visual perception, memory, arithmetic, language, praxis, and executive functions. Based on prior work, one would expect to find a unique pattern of dysfunction in anxious and otherwise affected adolescents, although inconsistencies in the prior literature preclude more definitive conclusions on the nature of specific deficits among specific groups of impaired adolescents.
Methods
Sample
Parents provided written informed consent for participating in the study, and the adolescents provided written assent. The study was approved by the Ethics Committee in Research of Hospital de Clínicas de Porto Alegre (HCPA) (number 10-0333). Subjects were drawn from a larger cross-sectional study that initially screened 2457 adolescents. Details of the sampling procedures can be found elsewhere (Salum et al. 2011). Briefly, from this initial sample of 2457 subjects, all 602 who scored above the 75th percentile of Screen for Childhood Anxiety and Related Disorders (SCARED) and a random sample of 10% of the remaining three quartiles (n=240) were invited to undergo a clinical evaluation with a structured psychiatric interview in our outpatient unit. From the subjects who attended the clinical psychiatric evaluation (n=242; 33.3% from the three lower quartiles and 26.6% from the upper quartile), an additional, selected sample of 59 also underwent a detailed neuropsychological assessment. Subjects were classified into four non-overlapping groups: 1. Typically developing comparison adolescents (TDC): Absence of any psychiatric disorder (except for specific phobia) 2. Anxiety: Current social anxiety disorder, generalized anxiety disorder, or separation anxiety disorder 3. Externalizing: Current ADHD or current oppositional defiant disorder (ODD) 4. Comorbid: Both anxiety and externalizing disorders (ADHD and/or ODD).
Comorbid cases of major depression (n=1) and obsessive-compulsive disorder (n=1) were excluded from the sample, because of the small numbers of such cases. No cases of panic disorder and conduct disorder were detected. Subjects with the diagnosis of specific phobia were allowed in all groups, given that specific phobia alone is very common, often minimally impairing, and associated with high spontaneous remission (Klein 2009).
Psychiatric diagnosis
A clinical interview followed by a semistructured diagnostic interview, the Schedule for Affective Disorder and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997), with the participants and their parents, were assessed by six trained psychiatrists. Psychiatrists had to have received at least 2 years of clinical training as well as 36 hours of specific training in the K-SADS-PL to be a part of the diagnostic evaluation team. Interrater reliability for anxiety disorder was evaluated using procedures described elsewhere, which generated acceptably high concordance between evaluators (κ=0.93) (Salum et al. 2011).
Clinicians also rated the Clinical Global Impressions Scale (CGI) - Severity in order to assess global severity caused by psychiatric disorders (Guy 1976), using a score that varied from 1 to 7. On this scale, “1” indicated “normal or not at all ill,” whereas “7” indicated “the most extremely ill patient” Clinicians were asked to rate the severity of each one of the four anxiety disorders, and we calculated a mean of the CGI based on the CGI of the four anxiety disorders. Inconsistencies in diagnosis and symptom severity were discussed with a senior clinician who reviewed the psychiatrists notes (G.G.M.).
Neuropsychological dimensions
Psychologists and speech therapists with formal training in neuropsychology performed the evaluations. The broad neuropsychological dimensions were evaluated using a well-known standardized instrument, the Brazilian Brief Neuropsychological Assessment Battery (NEUPSILIN). The main purpose of this screening instrument is to provide a brief neuropsychological profile of many cognitive functions and cognitive strategies that are used by the subjects (Fonseca et al. 2008, 2009). This measure has the additional advantage of being integrally constructed for Brazilian population, making it culturally appropriate for this sample. As language and culture markedly influence performance, this is an additional important feature of the current study (Fonseca et al. 2008, 2009). Validity and reliability of this instrument has been demonstrated (Pawlowski et al. 2008), as has the appropriateness for use in samples with ages (Zibetti et al. 2010) and overall intellectual skills (Pawlowski 2012) similar to those of our sample.
The instrument was constructed to evaluate eight core abilities described in Table 1: 1) Temporal and spatial orientation, 2) attention, 3) visual perception, 4) arithmetic skills, 5) oral and written language, 6) verbal and visual memory, 7) praxis, and 8) two types of executive functions, verbal fluency and problem solving.
Intelligence
Intelligent quotient (IQ) was calculated using the Wechsler Abbreviated Scale of Intelligence (WASI) (Wechsler 1991; Yates et al. 2006). It is used to assess verbal, nonverbal, and general cognitive functioning (Heck et al. 2009; Strauss et al. 2001). Individuals were excluded if they had an IQ total score <70.
Statistical analysis
Data are presented as mean (SD) and absolute frequency (%). In order to avoid multiple testing, we performed the following stepwise data analysis. First, we performed a multivariate analysis of variance (MANOVA), testing a main effect of group using all domains from the neuropsychological battery as outcome measures. Second, we performed post-hoc analysis of variance (ANOVAs) to detect domains with significant between-group differences. Third, significant between group differences were explored with analysis of covariance (ANCOVAs) controlling for potential confounders (ADHD, gender, school years, IQ) defined as those variables associated with the outcome with a p value <0.2 or of theoretical relevance (Tombaugh et al. 1999; Riva et al. 2000; Sauzeon et al. 2004; Rodriguez-Aranda and Martinussen 2006). Fourth, pairwise contrasts were performed using least significant differences. Finally, domains that were significantly different between groups were further explored with supplemental analysis (described in detail in the Results section), including associations with severity and number of anxiety diagnoses using Spearman correlation coefficients.
Effect sizes were defined in terms of percent of explained variance and 1, 9, and 25% were defined as small, medium, and large effects corresponding to 0.01, 0.06 and 0.14 partial η2 values (Cohen 1988). All analyses were performed using SPSS v. 18.0. All tests were two tailed, assuming a significance level of 5%.
Results
Clinical and demographic characteristics are depicted in Table 2. No significant between-group differences were found regarding gender, socioeconomic status, age, school years, and IQ. As expected, both anxious groups (anxiety and comorbid) presented significantly higher SCARED-C scores than did TDC.
Post-hoc tests using least significant differences (different letters indicate mean differences between groups).
DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; GAD, generalized anxiety disorder; ADHD, attention-deficit/hyperactivity disorder; ODD, oppositional defiant disorder; SES, socioeconomic status; IQ, intelligence quotient; WASI, Wechsler Abbreviated Scale of Intelligence; SCARED-C, Screen for Children Anxiety Related Emotional Disorders, child version.
The MANOVA examining the group effects in the eight neuropsychological domains revealed a significant main effect (F 8,48=2.32, p=0.034, ηp 2=0.279). Post-hoc analysis for the eight domains showed that mean differences were found in the score of executive functions (Fig. 1) and that this difference was independent from potential confounders (Table 3).
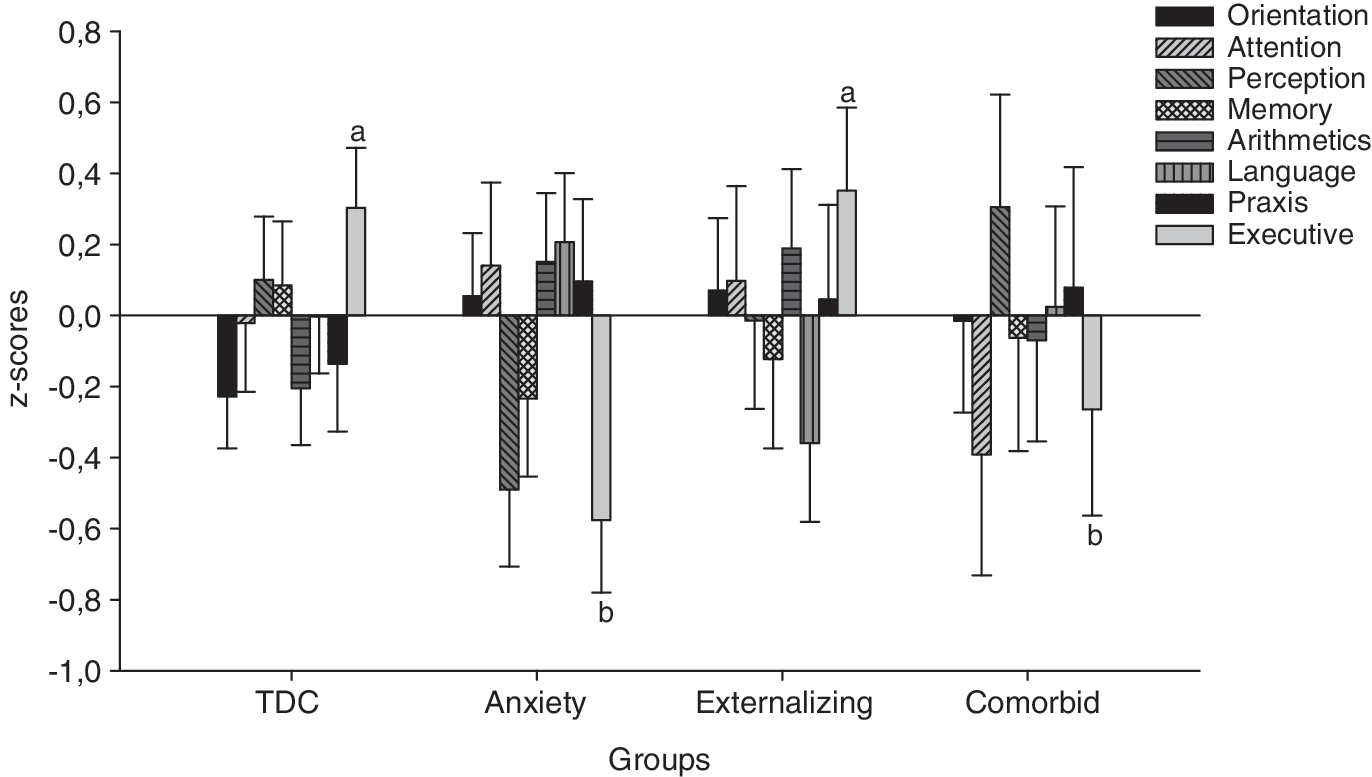
Between-group differences in the eight neurocognitive domains.
All univariate analyses were repeated using nonparametric Kruskal–Wallis test with the same results given by parametric tests.
Adjusted analysis uses gender, school years, and total intelligence quotient (IQ) as covariates. Post-hoc tests use least significant differences (different letters indicate statistically significant differences).
TDC, typically developing-comparison.
Following our analysis strategy, we then performed a MANCOVA with the components of the executive functions score (problem solving and verbal fluency) in order to investigate what component of the executive functions score was contributing to the results. Post-hoc ANCOVAs revealed statistically significant mean differences in the verbal fluency but not in the problem-solving component (Table 4). Contrasts for the verbal fluency score showed that both the anxiety and comorbid groups were significantly different from the TDC and externalizing groups, but not from each other (Table 4, Fig. 2).
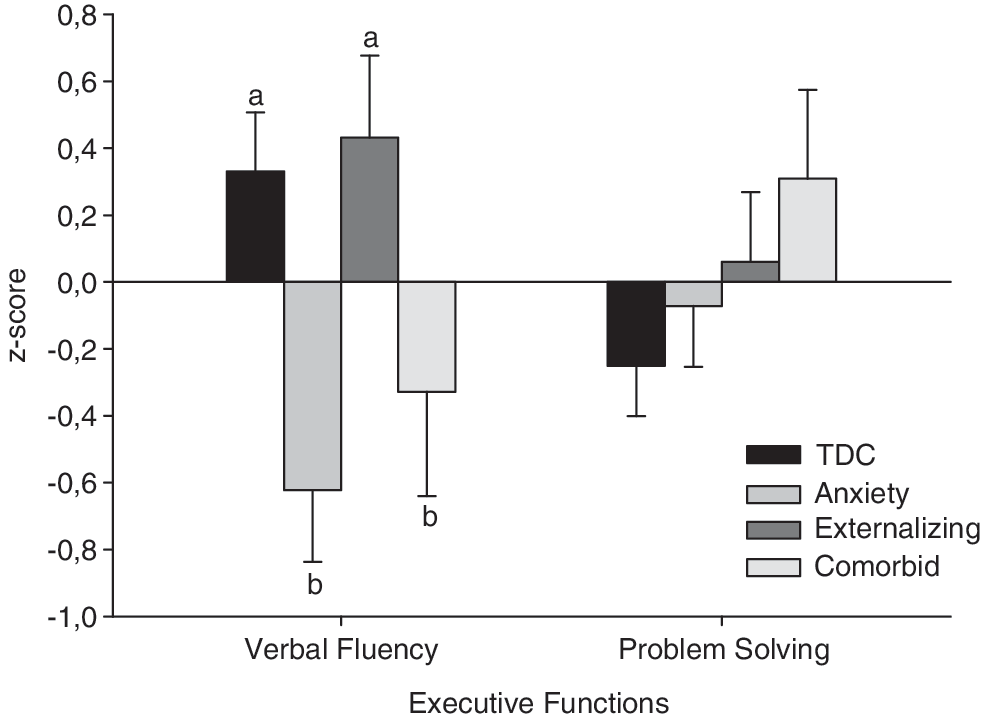
Differences between groups in verbal fluency and problem solving.
All univariate analyses were repeated using nonparametric Kruskal–Wallis test with the same results given by parametric tests.
Adjusted analysis uses gender, school years, and total intelligence quotient (IQ) as covariates. Post-hoc tests use least significant differences (different letters indicate statistically significant differences).
TDC, typically developing comparison.
Supplemental analysis with the verbal fluency score
Dimensional analysis
We found a negative correlation between verbal fluency score in the total sample and the self-rated SCARED total score (r=−0.36, p=0.005), the clinician-rated CGI-Anxiety scores (r=−0.46, p<0.001), and the number of positive anxiety diagnoses in K-SADS-PL (r=−0.45, p<0.001).
Clustering and switching
We further explored the meaning of the lower performance of individuals with anxiety disorders in the verbal fluency task with respect to clustering and switching. Previous investigators (Dell et al. 1997; Troyer et al. 1997; Riva et al. 2000; Troyer 2000; Sauzeon et al. 2004; Tallberg et al. 2011) have observed that words in phonemic-orthographic fluency tasks tend to be produced in phonemic-orthographic clusters, that is, bursts of words over time that are phonemically related. Clusters were defined as groups of successively generated words that began with the same first two letters (e.g., fire and financial), differed only in single vowel sounds (e.g., sit and set), produced rhyme (e.g., strip and ship) or were homonyms (e.g., see and sea). Switches were defined as transitions between clusters and/or between isolated words. We therefore analyzed four variables determined according to previously defined scoring rules (Dell et al. 1997; Troyer et al. 1997): 1) Number of correct words (total words minus repetitions and rule violation), 2) number of clusters, 3) mean cluster size, and 4) number of switches. Following our previous strategy, multivariate analysis found a main effect of group (F 4,51=3.06, p=0.024, ηp 2=0.194), and post-hoc ANOVAs revealed that only the number of switches were different between groups (Table 4), with ANCOVAs approaching significance for the number of switches. Post-hoc tests revealed that both anxious groups (anxiety and comorbid) had a lower number of switches than TDC, but no other significant between-group differences were detected.
Valence analysis
We also performed a valence analysis classifying the words evoked as positive, negative, and neutral, with negative being further subdivided into threatening and nonthreatening. A total of 29 (11%) were classified according to the criteria of an article with Brazilian norms for classification of words for valences (Kristensen et al. 2011). The remaining words (n=234) were classified by two judges independently. When there was no consensus between judges, the words were analyzed again by two new independent judges blind to the first classification. A fifth examiner evaluated nine words that were still discordant. No between-group differences emerged in the percentage of negative, positive, and neutral, and in the percentage of threatening and nonthreatening words between groups (all p values>0.05; Table 4).
Discussion
We found that adolescents with anxiety disorders had a worse performance on a time-dependent verbal fluency task with phonemic-orthographic criteria than did TDC adolescents. Poorer performance in this task was specific to both anxious groups (anxiety and comorbid groups) and did not occur in adolescents with externalizing disorders. Further analysis demonstrated that the poor performance in adolescents with anxiety disorders resulted from a reduced number of switches rather than in the emotional content of these words.
We found a strong association with a large effect size between verbal fluency and anxiety disorder status, one that to our knowledge has not previously been investigated in pediatric samples. With respect to adult population, there are very few empirical studies investigating verbal fluency impairments in anxiety disorders, and results are mixed. Whereas some studies found evidence of verbal fluency deficits in patients with anxiety disorders (Ohta et al., 2008; Nishimura et al. 2009; Nelson et al. 2012), others failed to find such evidence (Airaksinen et al. 2005). Deficits in verbal fluency are also implicated in ADHD (Schuerholz et al. 1998; Dery et al. 1999) and autism (Minshew et al. 1992; Turner 1999), but we were not able to detect such verbal fluency deficits in the subjects with externalizing disorders, unless they were complicated by a co-occurring anxiety disorder. Finally, we found no association between pediatric anxiety and seven other neurocognitive domains, where prior research also generally finds intact function (Frost et al. 1989; Toren et al. 2000; Gunther et al. 2004; Vasa et al., 2007; Micco et al. 2009).
Many studies suggest that executive functions such as inhibitory control and cognitive flexibility are intact in anxiety disorders. Considering this, how might deficits in verbal fluency arise in adolescent anxiety disorders, in terms of the associated brain mechanisms? In our study we measured verbal fluency throughout an individual's ability to generate words beginning with a specific letter (Levelt et al. 1999; Sauzeon et al. 2004; Birn et al. 2010). This places two different demands on the subjects: 1) To produce as many words as possible and 2) to respect task instructions and limit errors. This task can be understood as a complex cognitive problem, taxing at least four different functions: Verbal memory, storage requirements resulting from lexical decisions, executive functions related to organization of performance, and motor output (Rodrigues et al. 2008). Some authors emphasize the executive components of verbal fluency tasks (Toren et al. 2000); others place greater emphasis on verbal abilities and language (Sutin et al. 2011).
Our supplemental analysis linked poor performance in anxiety to deficiencies in switching, but it is associated neither with clustering nor with the mean size of the cluster. According to some authors (Troyer et al., 1997) switching (one of the most important components of phonemic fluency) strongly reflects executive functions associated with frontal lobe function, whereas clustering reflects semantic memory functions and may be associated with temporal lobe area. Nevertheless, as this task involves several other mental functions (verbal memory, storage requirements resulting from lexical-semantic decisions, executive functions related to organization of performance, and motor output), other aspects not directly related to the executive and frontal functions that were not properly measured may be driving the results.
One could also hypothesize that specific findings with the verbal fluency task may be associated with a specific task characteristics – a time-pressure effect (subjects had 1 minute to complete the task) – in a task that involved production of verbal content or with potential deficits in motor function (Ekornas et al. 2010; Pearsall-Jones et al. 2011).
Neuroimaging and lesion studies strictly link verbal fluency to prefrontal function (Baldo et al. 2001; Henry and Crawford 2004; Tupak et al. 2010). Therefore, the present findings reinforce the role of prefrontal regions in the pathophysiology of pediatric anxiety. Studies have shown individual differences related to pediatric anxiety in regions of the prefrontal cortex that are implicated in different aspects of emotion regulation, such as the ventrolateral prefrontal cortex and the ventromedial prefrontal cortex (Pine 2007; Monk et al. 2008a,b; Blackford and Pine 2012; Lissek 2012). We extend the pediatric literature showing that these deficits may be apparent even in tasks with no obvious emotional components. Also, we could extend the literature that has already demonstrated signs of hypofrontality during verbal fluency tasks of adult patients with panic disorder (Ohta et al. 2008; Nishimura et al., 2009; Nelson et al. 2012).
The results of a recent study using a verb-generating task quite similar to the one we used is also in agreement with our findings (Snyder et al. 2010). This study suggested that adults scoring high on an anxiety symptom scale also demonstrated deficient abilities in particular forms of word generation tasks. It is known that this deficient ability was linked specifically to chemical regulation of the ventrolateral prefrontal cortex, the cortical region most consistently implicated in pediatric anxiety disorders (Pine 2007). Taken together, these findings provide indirect evidence that the poorer performance of executive functions in anxious adolescents may reflect specific dysfunction in the ventrolateral prefrontal cortex.
Our study has some limitations. First, the small sample size may limit our ability to detect cognitive differences with lower effect sizes and to detect between-group differences in some tasks, especially regarding the small group of adolescents with externalizing disorders who were solely used in this analysis as a contrast to the comorbid group. However, even with a small sample size, we were able to demonstrate that the two anxious groups (anxiety and comorbid groups) differed from controls and externalizing disorder subjects in a task of verbal fluency not previously reported in the literature. Also, the significant results were reinforced by our dimensional correlational analysis. Second, because of the exploratory nature of this study, the possibility of type I error should also be taken into account. Nevertheless, verbal fluency results remain significant even after controlling for confounders. In addition, we used a stepwise approach in order to avoid spurious associations. Third, between-group differences in IQ might have influenced our results. Nevertheless, IQ was covaried in all our analyses and subjects with intellectual deficiencies were excluded from the sample. Fourth, neurocognitive functions were evaluated by an instrument that focuses on a broad assessment of neurocognitive functions, and fine-grained evaluations of each of the mental functions deserve further evaluations (Pawlowski 2012). Finally, some studies found that a large degree of variety exists among the number of names generated by different letters of the alphabet (Levelt et al. 1999; Tombaugh et al. 1999; Tallberg et al. 2011); therefore, further studies should investigate other letters and other tasks to assess the nature of this specific deficit.
The strengths of our study should also be underscored. First, subjects with anxiety and externalizing disorders were identified in a community sample not previously exposed to medication, increasing our confidence that the findings related to anxiety itself and not to therapeutics. Second, controls were referred from exactly the same community under the same sample selection condition as cases; therefore, they can be seen as ideal in terms of controlling for unmeasured and unknown risk factors for both anxiety and related neuropsychological outcomes. Third, we investigated nonoverlapping groups of psychopathology, including a group with externalizing disorders and group with comorbidities, providing us the ability to assess the specificity of our findings to anxiety and not to other common psychiatric disorders. Fourth, we have used a culturally sensitive instrument validated for Brazilian adolescents (Fonseca et al., 2008) that may bring some important advantages, especially for verbal tasks.
Conclusions
In summary, our results suggest a specific deficit in executive functions represented by verbal fluency deficits and therefore involvement of the prefrontal cortex, even in tasks not directly related to emotional processes in children and adolescents with anxiety. Further studies are needed in order to confirm these findings and to further discriminate those deficits in adolescents with different anxiety disorders.
Clinical Significance
This study compares neurocognitive characteristics of adolescents with an anxiety disorder with and without comorbidity for externalizing disorders, TDC adolescents, and adolescents with externalizing disorders alone. Our results suggest a specific deficit in executive functions represented by verbal fluency deficits and, therefore, involvement of the prefrontal cortex even in tasks not directly related to emotional processes in children and adolescents with anxiety. Such findings underscore the potential role of interventions aiming to improve executive functions in children and adolescents with anxiety disorders.
Footnotes
Acknowledgments
The authors thank the patients and their families for taking part in this study; Andressa Bortoluzzi, Ana Maria Frota Lisboa Pereira de Souza, and Itiana de Castro Menezes for their help in data collection; the Neurocog - UFRGS for their assistance with the database; and Clarissa M. Trentini's research group (UFRGS) for helping with WASI procedures.
Disclosures
No competing financial interests exist.