
Abstract
Objective:
The purpose of this study was to investigate factors for pharmacotherapy adherence in patients with attention-deficit/hyperactivity disorder (ADHD), with an emphasis on medication possession ratio (MPR).
Methods:
The medical records of 300 clinic-treated youth diagnosed with ADHD were retrospectively reviewed. Patients from March 2005 through January 2009 were diagnosed using the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) and psychological tests. Patients were classified based on the time period from the initial visit to the last visit. We selectively compared the early dropout group within 6 months and the long-term medication group over 36 months (LMed) to identify long-term follow-up characteristics. The short-term follow-up group was divided into an early dropout group without pharmacotherapy commencement (EDO) and a short-term medication group (SMed). Sociodemographic data, psychological test scores, and average MPR of the EDO, SMed, and LMed groups were compared.
Results:
The number of EDO patients was 69 (23.0%) out of the 300 total patients who were studied, and there were 59 SMed patients (19.3%), and 60 LMed patients (20.0%). Compared with other groups, the EDO group included significantly more younger patients, younger parents, higher maternal education level, lower Short Form Korean-Conners' Parent Rating Scale (K-CPRS) score, and higher full scale and performance intelligence quotient (IQ). There was no significant correlation between the average MPR and the treatment duration.
Conclusions:
Within the first 6 months of visiting the hospital, >40% of the patients dropped out of treatment regardless of methylphenidate (MPH) use. Twenty percent of the subjects showed adherence to MPH medication after 36 months.
Introduction
A
However, adherence rates in long-term medication groups are vastly different, depending upon the study; Corkum et al. (1999) reported 73.4% at 12 months, Thiruchelvam et al. (2001) reported 52% at 3 years, and Charach et al. (2004) reported 36% at 5 years. In spite of the differences in these reports, previous studies consistently reported that drug compliance remains suboptimal among ADHD patients (Perwien et al. 2004; Molina et al. 2009; Zuvekas and Vitiello 2012).
It is difficult to determine why treatment compliance varies among studies, especially with ADHD, a condition that continues throughout adulthood. A previous study (Kim et al. 2010), determined that the first 6 months after starting medication could be a critical period for adherence to treatment. Recent long-term studies showed that the highest dropout percentage occurred over the first 6 months of treatment (Kim et al. 2008; Garbe et al. 2012; Lawson et al. 2012). In addition to the medication period, several factors such as adolescence (McCarthy et al. 2012), short-acting methylphenidate (MPH) (Marcus et al. 2005), and multiple daily dosing of MPH (Gau et al. 2006) were factors for poor compliance. The authors also considered the medication possession rate (MPR) as contributing factors. Previously, MPR was used as the most representative standard to determine long-term treatment in treatment compliance studies; a MPR>0.8 was identified as good adherence. Based on our clinical experience, variables such as drug holidays, winter and summer vacation, or brief breaks, followed by a uniform application of an MPR>0.8 could result as bias in data analysis.
Therefore, the objective of this study was to explore the critical period defined as good adherence, to investigate whether MPR application is appropriate in clinical trials. In addition, the study sought to determine factors that affect long-term adherence.
Methods
Subjects
We retrospectively investigated the medical records of outpatient clinic visitors from a single medical university hospital from March 2005 to January 2009. The records were sorted according to the diagnostic codes (F90.0) in the International Classification of Disease, Version 10 (ICD-10), and the study included 338 children with a Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) (American Psychiatric Association 2000) diagnosis of ADHD. The diagnosis was made by board certified child and adolescent psychiatrists. As the approved age range for methylphenidate (MPH) use by Korean Food and Drug Administration (KFDA) is 6–18, 30 patients outside that age range were excluded. Eight patients taking concomitant medication for comorbidities before diagnosis of ADHD were also excluded. Patients with pervasive developmental disorders, schizophrenia and other psychotic disorders, and mental retardation were excluded from the study. The final number of study subjects was 300. This study was approved by the Institutional Review Board of Kyung Hee University Hospital.
Procedures
The date of the first outpatient visit was the index date. There were 300 initial patients (100%) and the cumulative number of adherent patients every 6 months was 173 (57.6%) at the 6th month, 142 (47.3%) at the 12th month, 108 (36.0%) at the 18th month, 88 (29.3%) at the 24th month, 72 (24.0%) at the 30th month, and 60 (20.0%) at the 36th month (Fig. 1). Previous studies that investigated treatment follow-up (Kim et al. 2008; Garbe et al. 2012; Lawson et al. 2012) classified treatment duration within 6 months as “short-term treatment” and determined that the rate of discontinuation was the highest within 6 months of initial treatment. Because the dropout rate was also the highest in the first 6 months at 42.4% (127/300), this study classified the group with <6 months of treatment as the “short-term follow-up” group. This study classified patients receiving medication treatment >36 months as the long-term medication use group (LMed), based on criteria from a multimodal ADHD treatment (MTA) report at 3 years (Jensen et al. 2007), and an article by Langberg and Becker (2012) about long-term medication use. We compared the short term follow-up group with the LMed group to identify factors that affect long-term adherence to medication. The patients in the short-term follow-up group were divided into two groups: 58 patients who were taking medication before they dropped out (SMed), and 69 patients who dropped out early without commencing medication (EDO). Finally, we compared the three groups: the EDO, the SMed, and the LMed.
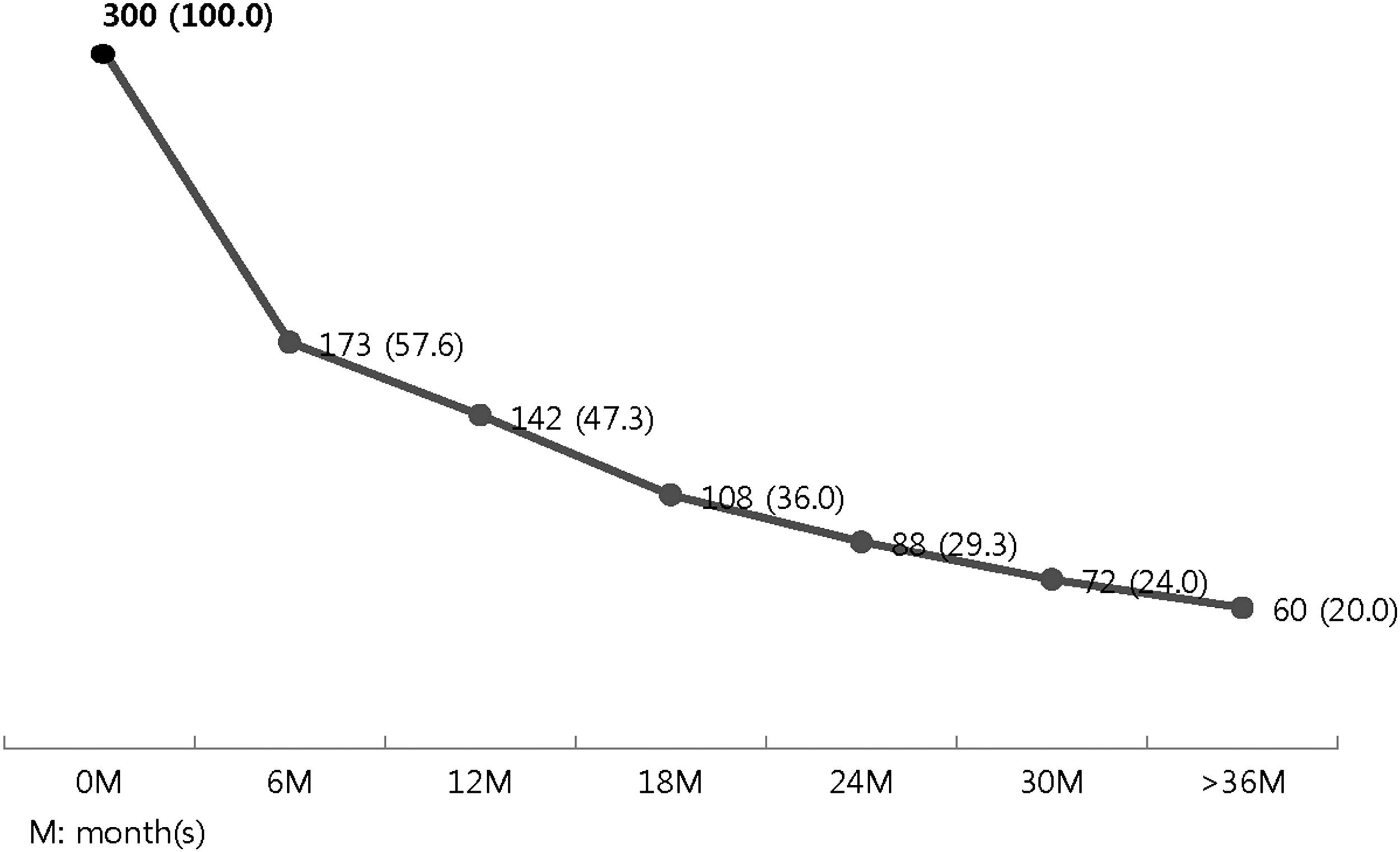
The total number of adherent patients on treatment at every 6 month interval (%).
Psychological tests
Korean-Conners' Parent Rating Scale (K-CPRS), Short Form
The Conners' Parent Rating Scale (Conners 1972) was developed to objectively assess behavioral symptoms related to ADHD. This study used the K-CPRS, short form (Oh and Lee 1989) with 10 items. Each test item uses a four point Likert scale that ranges from “very unlikely (0)” to “very likely (3),” and higher scores indicate more severe symptoms. The cutoff value is >16 points.
Korean-Personality Rating Scale for Children (K-PRC)
The K-PRC (Kim et al. 2005) was developed by partially modifying the Korean Personality Index for Children (KPI-C), and is composed of 10 clinical indices (language development, motor development, anxiety, depression, somatization, delinquency, hyperactivity, family relationships, social relation, and psychosis) and is answered using a four point Likert scale. This test is an instrument that assesses a child's condition based on the parents' report; higher scores indicate more severe symptoms.
Korean Wechsler Intelligence Scale for Children-III (K-WISC-III)
The K-WISC-III, which was based on the Wechsler Intelligence Scale for Children-III (Wechsler 1991) is an individual intelligence test to clinically assess the intelligence of children and adolescents from 6 to 17 years old (Kwack et al. 1991).
MPR
Current studies apply various methods to retrospectively estimate patient compliance, and MPR is one of the most popular assessment methods (Steiner and Prochazka 1997; Peterson et al. 2007; Barner et al. 2011). The MPR of each study subject was calculated by the following method: Number of days of medication supplied within the refill interval/number of days in the refill interval. The authors calculated the average MPR every 6 months, depending upon treatment duration, to assess the correlation between MPR and adherence.
Data analysis
Statistical analysis was performed using the SPSS 12.0® software (SPSS Inc., Chicago, IL) program. The three groups were classified according to the treatment duration and medication usage for intergroup comparisons, and a χ2 test and one way analysis of variance (ANOVA) were used, depending upon the data characteristics. The least significant difference (LSD) post-hoc test was performed to compare aspects among the groups.
Finally, the average MPR during the treatment period was calculated, and a Pearson correlation analysis was performed to test the correlation between MPR and long-term follow-up medication.
Results
Sociodemographic characteristics
Comparison of the three groups (the EDO, the SMed, and the LMed) did not indicate any statistically significant differences in sex (χ2=1.907, p=0.385). There were statistically significant differences in age at treatment initiation (F=5.416, p=0.005) (Table 1).
EDO, the early dropout group without commencement of pharmacotherapy; SMed, the short-term medication group (≤6 months); LMed, the long-term medication group (≥36 months).
After the post-hoc analysis, mean age of the SMed group was significantly higher than that of the EDO and the LMed groups. With the exception of the paternal education level, the analysis indicated that there were significant differences among the three groups with regard to the age of the parents and the education level of the mother (F=3.430, p=0.035; F=4.202, p=0.017; F=5.593, p=0.004) (Table 1). In the post-hoc analysis, the parental age of the LMed group was significantly higher than that of the EDO group. Additionally, the maternal education level was significantly higher in the EDO group than in the LMed and the SMed groups.
Psychological test results
The analysis indicated that there was a significant difference in the total Conners' score for the three groups (F=5.559, p=0.005), even though the average K-CPRS score of the three groups was subthreshold (Table 2). The SMed had a higher score than that of the EDO in the post-hoc analysis.
K-WISC-III, Korean Wechsler Intelligence Scale for Children-III; K-CPRS: Short Form Korean-Conners' Parent Rating Scale; FSIQ, Full scale intelligence quotient; VIQ, Verbal IQ; PIQ, Performance IQ; EDO: the early dropout group without commencement of pharmacotherapy; SMed, the short-term medication group (≤6 months); LMed: the long-term medication group (≥36 months).
The K-PRC determined that there were significant differences among the three groups in the Delinquency (DLQ), Hyperactivity (HPR), and Social dysfunction (SOC) subscales (F=3.551, p=0.031; F=4.034, p=0.020; F=3.186, p=0.044). The EDO had significantly lower scores after the post-hoc analysis than did the LMed group in the DLQ and SOC subscales, and the EDO had a lower score than the SMed group in the HPR subscale.
The full scale intelligence quotient (FSIQ) indicated scores of 107.19±12.88 for the EDO group, 100.05±14.35 for the SMed group, and 99.56±12.28 for the LMed group, and showed that there were significant differences among the groups (F=5.060, p=0.008) (Table 2). Although there was no significant difference in the verbal IQ (VIQ) (F=3.004, p=0.053), there was a significant difference (F=3.661, p=0.028) in the performance IQ (PIQ) of the SMed group (100.41±13.46) and the LMed group (97.58±13.38). The post-hoc analysis indicated that the FSIQ and PIQ of the EDO group were higher than those of the LMed group, and that the FSIQ of the EDO group was significantly higher than that of the other groups.
Treatment duration and MPR correlations
The correlation analysis with MPR data was conducted with 207 of the initial 300 patients, regardless of the patient group. There was no statistically significant difference between the treatment duration and the average MPR (Pearson Correlation=0.032). There was also no significant difference in the average MPR value between the SMed and LMed groups (Pearson Correlation=0.088). The average MPR distributions were 0.6 (2), 0.7 (5), 0.8 (19), 0.9 (10), and 1.0 (24), and the average MPR distributions of the SMed group were <0.3 (10), 0.3 (2), 0.4 (1), 0.5 (1), 0.6 (1), 0.7 (3), 0.8 (8), 0.9 (8), and 1.0 (24).
Discussion
This naturalistic retrospective study showed that the first 6 months after diagnosis was a critical period for ADHD pharmacotherapy. This finding coincided with those of previous studies, which identified a high discontinuation rate within the first 6 months of medication use (Garbe et al. 2012; Lawson et al. 2012). An observational study reported that patients who adhered to treatment over 3 years reported a rate of 38% (Charach et al. 2004). Another study reported an adherence rate of 52% at the 36th month, which was much higher than the 20% revealed in this study (Thiruchelvam et al. 2001). However, unlike this study, the other studies were prospectively designed, and direct and indirect communication was possible during the monitoring period, which may have contributed to the higher rate of adherence.
In this study, the initial treatment age of the SMed group was greater than that of the LMed group. This result is in agreement with previous studies (Thiruchelvam et al. 2001; Gau et al. 2006) that reported that a high initial treatment age was a predictor for treatment noncompliance. According to McCarthy et al. (2012), patients who started ADHD treatment between 6 and 12 years of age had a longer treatment duration, which was an average of 5.9 years, than that of patients who started treatment between 13 and 17 years of age, who had an average of 1.9 years of treatment. The initial treatment age of the SMed group was higher than that of the EDO group. Based on these results, a high initial treatment age may affect medication compliance.
The analysis suggested that parental age increase negatively influenced pharmacotherapy, which was also reported by Gau (2006). According to a study by Rieppi et al. (2002), the education level of parents was generally a positive factor for persistent treatment. However, in this study, the maternal education level of the EDO was higher than that of the medication groups. A Taiwanese study (Gau et al. 2008) reported that compliance was negatively correlated with higher degrees of paternal education. Kim et al. (2010) suggested that parents with higher levels of education were more sensitive to social stigma and were more concerned about ADHD. It was also likely that the parental decision to use nonpharmacological treatment rather than medication was why EDO youth were younger, had higher IQs, and had mothers with more education. Additional research that compares cultural differences is necessary to investigate the conflicting results of studies from Western countries, Taiwan, and Korea.
When the intelligence and symptom severity were compared, the EDO group had higher FSIQ and PIQ values and lower K-CPRS scores. According to Antshel et al. (2007), children with ADHD and a high IQ may be at risk for late identification and treatment. A study by Johnson (2012) suggested that individuals with better executive cognitive function are better able to compensate for the disorder and therefore less likely to receive a diagnosis. The intelligence scores of the SMed and the LMed were compared, and the SMed had higher FSIQ and PIQ scores. However, this result contradicted a study by Hwang et al. (2004). Therefore, there is currently insufficient evidence that compares medication compliance and intelligence, and additional well-designed studies need to be performed to understand these relationships.
MPR
Because MPR is used as a method to assess compliance in both research and clinical practice (Peterson et al. 2007; Cramer et al. 2008), an MPR value of 0.8 is generally accepted as the cutoff value (Cramer et al. 2008). Especially in AIDS/HIV infection, adherence rates of 95–100% are needed for retroviral therapy (Ickovics et al. 2002; Chesney 2003). Gianfrancesco, et al. (2008) reported that a high MPR was related to a reduction in the total patient and outpatient mental health care expenditures for bipolar mood disorders (Gianfrancesco et al. 2008). However, a study that compared the MPR for five chronic disorders showed that with the exception of hypertension, there was no evidence that MPR 0.8 is ideal for other disease comparisons (Karve et al. 2009).
Barner et al. (2011) analyzed adherence differences of different MPR values (0.7, 0.8, and 0.9) in patients with ADHD, and reported that the adherence increased for the 0.7 MPR value and decreased for the 0.9 MPR value. Therefore, the optimal MPR threshold differs depending upon the disease (Cramer et al. 2008; Karve et al. 2009). Because this study did not use MPR as a criterion for group classification or exclusion, the MPR value was calculated by reviewing the chart of each subject. Although there were patients with MPR values <0.8, it was difficult to determine or designate these patients as dropouts because of the possibility of drug holidays or use of different medications, such as Metadate CD®. The results of this study indicated that the correlation between treatment duration and the average MPR of the SMed and the LMed was not statistically significant. This indicates that although the patients were not completely adherent to pharmacotherapy, they generally adhered to it. In addition, the study analysis did not find a correlation between MPR and treatment duration. Based on this result, a compliance MPR value of 0.8 may be overly strict for ADHD patients, and additional discussions are necessary to establish the optimal MPR threshold for ADHD treatment.
Limitations and further directions
There were several limitations to this study. First, because the data were based on records from a single university hospital, it is not representative of treatment characteristics of Korean children and adolescents with ADHD, and, therefore, it is difficult to generalize the findings. Second, the data were based on chart reviews, and may not accurately reflect patient administrations of medication. Third, the patients were not divided into separate child and adolescent groups. Fourth, data regarding the exact courses of the SMed or the EDO groups were not available. Fifth, comorbidities were not considered. However, in spite of these limitations, this is the first study to introduce the concept of MPR in long-term follow-up study of ADHD.
Further studies that include other college and community hospitals, larger sample sizes, and treatment duration based on the Korean Health Insurance Review and Assessment Service (HIRA) data are necessary to accurately determine medication compliance in patients with ADHD. Prospective follow-up studies to improve treatment compliance, based on retrospective study results, are needed, especially considering the importance of long-term treatment for ADHD.
Conclusions
This 36-month retrospective study suggested that the noncompliant group was characterized by younger patients, a higher level of maternal education, younger parental age, higher IQ, and lower K-CPRS. Nonadherence to MPH treatment most frequently occurred within the first 6 months of starting medication. In addition, the results indicated that 20% of the subjects adhered to MPH medication after 36 months.
Clinical Significance
The findings of this study suggest that clinicians should work to determine and obtain better medication adherence for ADHD patients, especially within the first 6 months of diagnosis. In addition, application of the conventional 0.8 MPR cutoff value for adherence may be overly strict for ADHD.
Footnotes
Disclosures
No competing financial interests exist.