
Abstract
Objective:
Epidemiological research links aggression to low serum concentrations of omega-3 fatty acids, such as those found in fish oil. However, no studies have specifically examined whether fish oil supplementation can reduce the frequency and severity of impulsive aggression in children with disruptive behavior disorders.
Methods:
Children presenting with impulsive aggression and meeting research criteria for diagnosis of disruptive behavior disorders were randomized to receive either: 1) Fish oil capsules (4 g daily) for 6 weeks followed by placebo (identical-looking capsules) for 6 weeks; or 2) placebo for 6 weeks, followed by fish oil for 6 weeks, in a double-blind, crossover design. Primary outcomes were the Children's Aggression Scale and the Modified Overt Aggression Scale. Secondary outcomes included emotional and behavioral functioning (Strengths and Difficulties Questionnaire [SDQ]), hyperactivity symptoms (Attention-Deficit/Hyperactivity Disorder [ADHD] Rating Scale), family functioning (Family Assessment Device), and cognitive functioning (Stop Signal Task, Trail-Making Task, and Eriksen Flanker Task). Serum concentrations of omega-3 and omega-6 fatty acids were measured at baseline, and at 6 and 12 weeks.
Results:
Twenty-one children participated (81% male; mean age 10.3±2.2 years; range 7–14). Fish oil treatment increased serum concentrations of eicosapentanoic acid (F=14.76, p<0.05) and total omega-3s (F=20.56, p<0.05), but did not influence primary ratings of aggression. In fact, a trend suggested that fish oil worsened a secondary measure of aggression (SDQ Conduct Subscale, F=4.34, p=0.06). Fish oil treatment was associated with an improvement in one rating of hyperactivity (SDQ Hyperactivity Subscale, F=2.22, p<0.05), but did not influence any other outcome measures.
Conclusions:
These findings suggest that fish oil treatment does not improve aggression in children with disruptive behavior disorders.
Introduction
A
Impulsive aggression can respond to treatment (Connor et al. 2006). Generally, best practice for management of aggression within a mental health framework involves psychological approaches such as parenting interventions, anger management, and problem-solving training (Sanders et al. 2000; Spence 2003; Kazdin 2005; Connor et al. 2006; McGuire 2008). However, some families are not able to engage in psychosocial treatments (Eyberg et al. 2008; Jensen 2008). In practice, pharmacological treatments may also be used, especially when aggression is severe or nonresponsive to behavioral interventions (Steiner et al. 2003; Connor et al. 2006). Evidence suggests that rates of medication use for aggression is increasing (Pappadopulos et al. 2003; Dean et al. 2009; Harrison et al. 2012).
Parents and children are increasingly using complementary and alternative medicines (CAM), such as fish oil, for mental health problems and behavioral management (Sinha and Efron 2005; Barnes et al. 2008). A range of epidemiological studies have linked violent behavior with low seafood consumption or low serum concentrations of omega-3 fatty acids (Hibbeln 2001; Iribarren et al. 2004; Gillies et al. 2012). Omega-3 fatty acids, such as those found in fish oil, have been suggested as a potential treatment for aggressive behaviors in children (Vaddadi 2006). Fish oil is a major source of the omega-3 fatty acids docosahexaenoic acid (DHA) and eicosapentanoic acid (EPA). These long-chain polyunsaturated fatty acids are found in the brain, and have a number of essential roles, such as maintaining the structural integrity of neuronal membranes (Hibbeln et al. 2006). However, these cross-sectional studies do not address causality, or identify whether supplementation can reverse problem behaviors.
Experimental studies using healthy volunteers suggest that fish oil may reduce aggression in university students (Hamazaki et al. 1996) and the elderly (Hamazaki et al. 2002), but not children (Itomura et al. 2005; Hamazaki et al. 2008). Fewer studies have examined the effects of fish oil in groups exhibiting aggressive behavior. One small trial reported that omega-3 supplementation led to a reduction in anger ratings in adult substance users, and that change in anger scores correlated with change in serum concentrations of DHA (Buydens-Branchey et al. 2008). A trial examined the effects of a combined supplement (vitamins, minerals, omega-3 and omega-6 fatty acids) on aggressive behaviors in adult prisoners. Compared with placebo, 2 weeks of supplementation were associated with a significant reduction in violent and aggressive incidents (Gesch et al. 2002). It is difficult to draw conclusions about the differential contribution of omega-3 fatty acids to this outcome, and the relevance of these findings to children and adolescents.
Two placebo-controlled studies suggest that fish oil may improve behavior in young people with developmental coordination disorder (Richardson and Montgomery 2005) or autism (Amminger et al. 2007). The majority of clinical trials examining fish oil in clinical populations of children and adolescents have focused on ADHD. The Cochrane meta-analysis examines 13 trials, incorporating 1011 participants (Gillies et al. 2012). Although two trials reported some beneficial effects of combined omega-3 and omega-6 supplementation, overall results indicated limited effect of fatty acid supplementation on parent or teacher ratings of ADHD symptoms. One of these studies reported improvements in teacher ratings of oppositional behaviors in a subgroup with oppositional behavior (Gustafsson et al. 2010). However, this finding was not reported in other studies (Gillies et al. 2012), and no studies have specifically examined fish oil in young people presenting with aggressive behavior.
The primary aim of this study was to assess the efficacy of omega-3 fatty acids in the treatment of impulsive aggression in children and adolescents with a diagnosis of a disruptive behavior disorder. The primary hypothesis was that fish oil treatment would reduce the frequency and severity of aggressive behavior compared with placebo. Secondary outcomes assessed included general emotional and behavioral functioning, hyperactivity symptoms, family functioning, and cognitive functioning.
Methods
Participants
Participants were recruited via advertising or clinical referral between September 2008 and December 2010 (n=21). Inclusion criteria were being 6–17 years of age, exhibiting impulsive aggressive behaviors persisting for at least 6 months, meeting criteria for diagnosis of oppositional defiant disorder or conduct disorder, as determined by structured interview (Kiddie Schedule for Affective Disorders and Schizophrenia for School-Aged Children—Present and Lifetime Version [K-SADS-PL])(Kaufman et al. 1997), and history of at least one unsuccessful attempt at behavioral intervention for aggression. Potential participants were excluded if they had a diagnosis of autism or other developmental disorder, moderate-severe mental retardation, psychotic or bipolar disorder, posttraumatic stress disorder, substance abuse disorder, or an acute unstable medical/psychiatric condition requiring priority intervention. Other exclusion criteria were: Recent (previous 8 weeks) initiation of other psychiatric intervention, coagulation disorder or anticoagulant treatment, seafood allergy, and pregnancy or lactation. An initial semistructured telephone interview asked parents to describe the problem behavior. If the child exhibited behaviors such as verbal abuse, physical attacks on objects, physical attacks on others for at least 6 months, they were then invited to complete a research interview to complete the K-SADS-PL). After telephone screening, potentially eligible participants and caregivers were invited to the research clinic for assessment and provision of oral and written information about the study. Eligible participants and caregivers provided written informed consent. No changes to eligibility criteria or other methods were made after trial commencement. Ethical clearance was provided by Mater Human Research Ethics Committee and The University of Queensland Medical Research Ethics Committee. The trial was preregistered on the Australian and New Zealand Clinical Trials Registry (ACTRN12608000477325).
Trial design
This trial was a prospective, randomized, placebo-controlled, crossover trial comparing fish oil to placebo.
Interventions
Participants were randomly allocated to receive either: 1) Fish oil capsules for 6 weeks (Phase 1) followed by placebo capsules for 6 weeks (Phase II) or 2) placebo capsules for 6 weeks (Phase I) followed by fish oil for 6 weeks (Phase II) (Allocation ratio 1:1). Dose of fish oil was 4 g daily, containing 400 mg EPA and 2000 mg DHA. Placebo capsules looked identical, and contained low polyphenol olive oil and 10 mg standard fish oil to assist in maintaining blinding. Patients were provided with study medication every 2 weeks during the study period.
Implementation of randomization and blinding
Randomization sequence was generated by an external trials site. After provision of written consent, each participant was assigned to the next consecutive participant number. All investigators, outcome assessors, and participants were blinded to treatment allocation procedures and treatment group throughout the study.
Outcome assessment
Clinical assessments were conducted every 2 weeks. Research assessments were conducted at baseline, 6 weeks, and 12 weeks. Primary outcomes were ratings of aggressive behavior, as rated by the following two instruments.
• The Children's Aggression Scale - Parent Version (CAS-parent) is a 33 item parent-rated measure that quantifies the frequency and severity of aggression over five domains: Verbal aggression, aggression against objects and animals, provoked physical aggression, initiated physical aggression, and use of weapons (Halperin et al. 2002). Higher scores indicate higher aggression. It has adequate psychometric properties in children (Halperin et al. 2002).
• The Modified Overt Aggression Scale (MOAS) is a 16 item, parent-rated measure of overt aggressive behavior (Sorgi et al. 1991) that rates frequency of verbal aggression, physical aggression against objects, physical aggression against self, and physical aggression against others. Higher scores indicate higher aggression. It has reasonable reliability in children, and is sensitive to drug-related change (Connor 2002).
Secondary clinical outcomes assessed incorporated the following measures:
• The Strengths and Difficulties Questionnaire (SDQ) (Goodman 1997) rates general emotional and behavioral functioning. In addition to total scores, five subscale scores are generated: Emotional symptoms, conduct problems, hyperactivity symptoms, peer relationship problems, and prosocial behaviors. It has well-established reliability and validity (Stone et al. 2004; Vostanis 2006).
• The Family Assessment Device General Functioning Scale (FAD-GFS) (Byles et al. 1988) is a 12 item, parent-rated assessment of family functioning. It demonstrates adequate reliability and validity.
• ADHD Rating Scale (DuPaul et al. 1998) is a parent-rated, 18 item scale that reflects symptoms of ADHD based on American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria (American Psychiatric Association 1994). It exhibits good psychometric properties. We utilized total scores only; higher total scores reflect more severe ADHD symptoms (Zhang et al. 2005).
Cognitive functioning was assessed using three tasks.
• Executive control–Trail Making Task: Participants are presented with a sheet of paper with 25 circles that they must connect by pencil as quickly as possible. In Part A, target circles are numbered 1–25 and the participant must connect these consecutively (1, 2, 3). In Part B, the target circles include both numbers (1–13) and letters (A–L), and the participant is required to connect these in alternate sequence (1, A, 2, B, 3, C). Instructions were provided according to Delis–Kaplan Executive Function System (Delis et al. 2001). The final score used for this study is the total time for completion of Part B, minus the time taken to complete Part A (seconds) (Sanchez-Cubillo et al. 2009).
• Response inhibition–Stop Signal Task: Response inhibition is a specific executive function which involves suppression of behavioral impulses (Logan and Cowan 1984). The Stop Signal Task requires the cancellation of a pre-potent “go” response upon presentation of an infrequent “stop” signal. Stop signal inhibition can be viewed as a race between two competing “go” and “stop” processes. By introducing a delay between the presentation of the go and any subsequent stop signal, one can bias the outcome of the race. The stop signal reaction time (SSRT) was derived as the mean reaction time (RT) to go stimuli minus the stop signal delay for the 50% inhibition threshold (Verbruggen and Logan 2009). A lower (i.e., faster) SSRT is indicative of better inhibitory control. In this study, there was a 64 trial practice block, followed by two 128 trial blocks with a break scheduled in between each block.
• Cognitive control–Eriksen Flanker Task: Participants are required to identify the direction of a central target arrow (left or right), as quickly as possible, using the arrow keys on a standard keyboard (Eriksen and Eriksen 1974). For congruent conditions, the target arrow is flanked by arrows pointing in the same direction as the target. For incongruent conditions, the target arrow is flanked by arrows pointing in the opposite direction. Improvements in cognitive control are represented by decreases in RT during incongruent, relative to congruent, conditions; that is, the key outcome variable was the difference between RT during incongruent and congruent conditions (Flanker Cost). Participants performed three practice blocks, each consisting of 10 stimuli, and were given oral feedback. The experimental phase of the task comprised two blocks of 240 trials each. Stimuli were presented for 600 ms, followed by an interstimulus interval of 780 ms. Presentation of congruent and incongruent stimuli was randomized. Performance was monitored throughout, and participants received oral encouragement to maintain engagement and fast response times. Simple and choice RT were also recorded to assess low-level speed of information processing.
Adverse effects were measured by the Treatment Emergent Symptom Scale, a 31 item self-report questionnaire widely used in psychopharmacology trials (Guy 1976). A total score was utilized to assess a range of potential adverse effects.
Weight was measured at each follow-up. Participants were also invited to spontaneously report any other potential symptoms occurring during the study.
Biological testing: Quantification of fatty acids
Blood samples (non-fasting) were collected via Mater Pathology Services at baseline, 6 weeks, and 12 weeks. Saturated and unsaturated fatty acids (chain length C8 to C26) were extracted from plasma, and assayed using capillary gas chromatography-electron capture negative ion mass spectrometry (Lagerstedt et al. 2001). This method quantifies absolute concentration data, and is more accurate than methods utilized in older studies, which quantify relative percentage concentrations (Lagerstedt et al. 2001). Fatty acid insufficiency is commonly defined by the triene/tetraene ratio (TT ratio). A range between 0.013 and 0.050 has been suggested as the normal range (Lagerstedt et al. 2001), and serious deficiency has been defined as a TT ratio>0.20 (de Meijer et al. 2010). For this study, we defined insufficiency as a TT ratio>0.05, and deficiency as a TT ratio>0.02.
Sample size and power calculation
Sample size and power calculations were based on the Verbal Aggression Subscale of the CAS-parent. Published psychometric data for the CAS-parent subscales are provided for conduct disorder, oppositional defiant disorder, ADHD, and non-aggressive clinical controls. Estimates of expected effect sizes focused on clinically significant change, and were calculated based on the difference in published mean score on the verbal aggression subscale between groups with oppositional defiant disorder, and non-aggressive clinical controls. This difference corresponds to a moderate-large effect size. Estimating effect sizes using other subscales generated similar expected effect size.
A priori sample size calculations estimated that a sample size of 27 would have a power of 80% to detect moderate-large effect sizes, based on two occasions of response, a moderate within- subject correlation and a two sided significance level of 5%. Based on observed within-subjects standard deviations (mean 2.02; range 0.03–4.83) for the Verbal Aggression Subscale, post-hoc power calculations indicate that 21 participants provide a mean power of 99% (CI 48–100%) to detect a three point difference in means on the Verbal Aggression Subscale.
Statistical analysis
Treatment outcomes were analyzed using mixed-effects modeling. A mixed-effects model was created for each outcome variable. Primary analysis examined the effect of treatment (fish oil vs. placebo) on treatment outcome. Fixed effects used for each model were: Treatment period, group, baseline concentration of omega-3, an interaction between treatment and baseline omega-3s, and the baseline rating of the outcome being assessed. Analysis for primary outcomes of aggressive behavior also included diagnosis of conduct disorder as a fixed effect. Similarly, analysis of secondary outcomes of hyperactivity ratings included diagnosis of ADHD as a fixed effect. The adequacy of each model was assessed by examining residuals for heterogeneity and normality. Analysis included all randomized participants (intention-to-treat analysis). Effect sizes were calculated by methods described by Thalheimer and Cook (2002).
Results
Recruitment and participant flow
Trial recruitment began in September 2008 and follow-up was completed in January 2011. During this period, 153 individuals contacted the recruitment team. From this, 53 children and adolescents were screened for eligibility; 21 met inclusion criteria and, along with their parent, provided consent to participate. Twelve were randomly allocated to receive fish oil in Phase I followed by placebo in Phase II; nine were allocated to receive placebo first, followed by fish oil. Three participants discontinued prior to study completion (Fig. 1). All participants were included in outcome analyses.
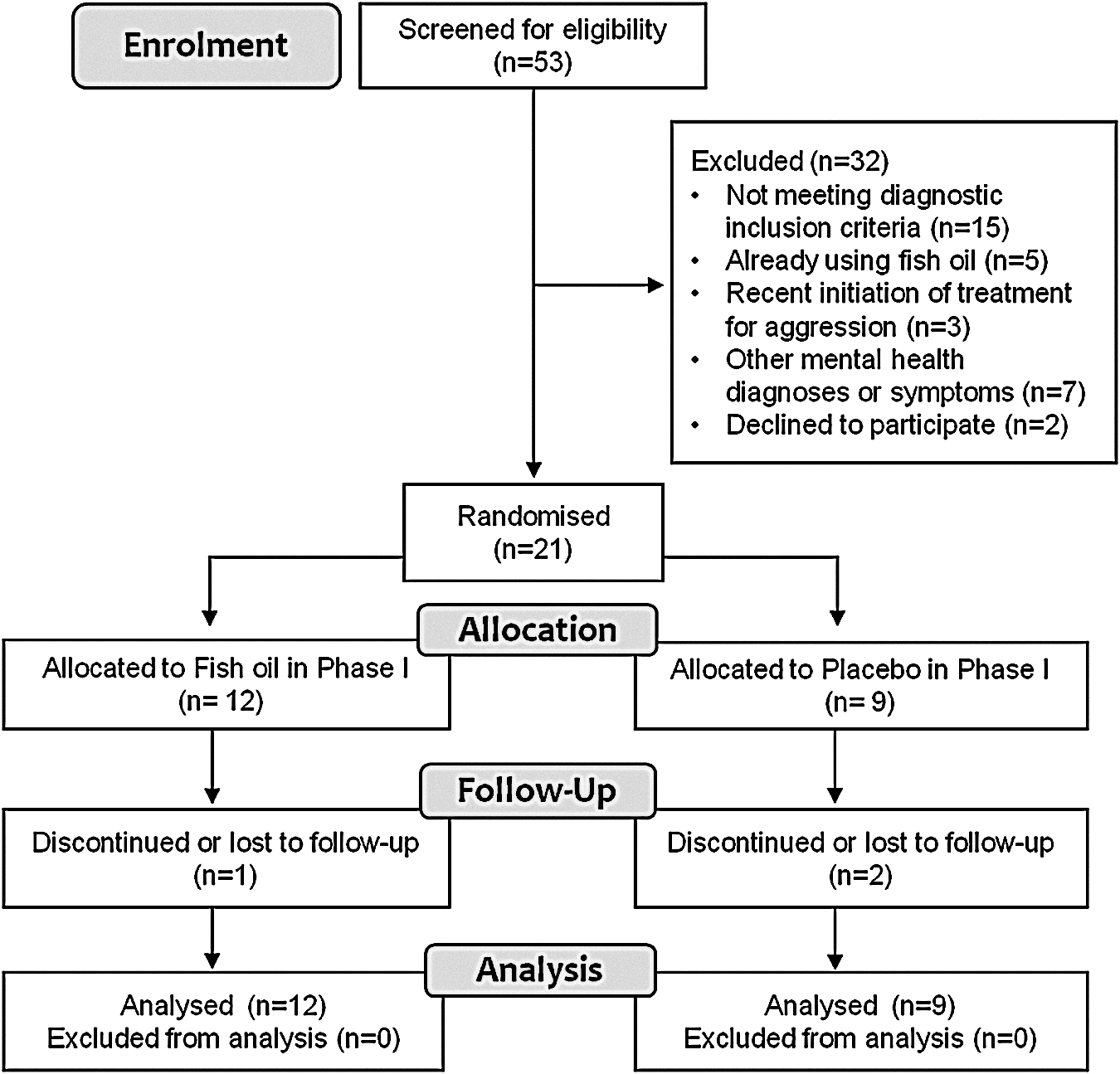
Flow chart of trial participation.
Patient characteristics at baseline
The mean age of participants was 10.3±2.2 years (range 7.1–14.2; median 9.9) and the majority were male (81%; 17/21). Half met diagnostic criteria for conduct disorder (52.4%; 11/21) and 76% met criteria for ADHD (16/21). No significant differences were observed between randomization groups in baseline ratings of clinical symptoms, cognitive function, or serum concentrations (data not shown). Fifteen participants provided at least one blood sample during the study (13 at baseline, 8 at 6 weeks, and 2 at 12 weeks). Correlations between baseline measures of 1) behavior and cognitive function and 2) serum fatty acid concentrations and measures of cognition and behavior are reported in Tables 1 and 2.
p<0.05; ** p<0.01; †trend at p<0.08.
SSRT, stop signal reaction time; CAS, Children's Aggression Scale; MOAS, Modified Overt Aggression Scale; SDQ, Strengths and Difficulties Questionnaire; ADHD, attention-deficit/hyperactivity disorder.
p<0.05; ** p<0.01; †trend at p<0.08.
EPA, eicosapentanoic acid; DHA, docosahexaenoic acid; AA, arachadonic acid; CAS, Children's Aggression Scale; MOAS, Modified Overt Aggression Scale; SDQ, Strengths and Difficulties Questionnaire; ADHD, attention-deficit/hyperactivity disorder; SSRT, stop signal reaction time.
Changes in fatty acid concentrations
Compared with placebo, fish oil supplementation led to a significant increase in serum concentrations of EPA (F=14.76, p<0.05), total omega-3s (F=20.56, p<0.05), and total omega-3s and omega-6s (F=34.72, p<0.01), and a nonsignificant increase in DHA (F=12.30, p=0.09) (Table 3). No change was observed in concentrations of arachidonic acid (F=2.08, p=0.22), total fatty acids (F=0.98, p=0.57) or the triene/tetraene ratio (F=0.87, p=0.40) (Table 3). At study baseline, more than one third of children (5/13, 38.5%) exhibited fatty acid insufficiency as determined by TT ratio. However, no children had a serious deficiency. At completion of the fish oil phase, two out of six participants exhibited insufficiency. At completion of the placebo phase, two out of four children (50.0%) exhibited insufficiency.
p<0.05; ** p<0.01; †trend at p<0.06.
CAS, Children's Aggression Scale; MOAS, Modified Overt Aggression Scale; SDQ, Strengths and Difficulties Questionnaire; ADHD, attention-deficit/hyperactivity disorder; SSRT, stop signal reaction time; EPA, eicosapentanoic acid; DHA, docosahexaenoic acid.
Primary outcomes: Aggressive behavior
No effect of fish oil treatment was observed on change in total scores of the CAS (F=0.05, p=0.82) or any effect of the interaction between treatment and baseline omega-3 concentrations (F=0.32, p=0.58). Similarly, fish oil treatment had no significant effect on the Verbal Aggression Subscale (F=0.38, p=0.55) or any other subscale scores of the CAS, nor was there an interaction between treatment and baseline omega-3 concentration (data not shown). No effect of treatment (F=0.08, p=0.79), or the interaction between treatment and baseline omega-3 concentration (F=0.24, p=0.34) was observed for the MOAS.
Secondary outcomes: Clinical measures
A trend suggested that fish oil supplementation worsened scores on SDQ Conduct Problems Subscale (F=4.34, p=0.056). In contrast, fish oil supplementation was associated with a significant improvement in SDQ hyperactivity scores (F=5.00, p<0.05). No effect of fish oil supplementation was observed for other SDQ subscales or SDQ total score, the ADHD rating scale, or family functioning (FAD) (Table 4).
Secondary outcomes: Cognitive measures
Fish oil supplementation did not lead to any changes on the Stop Signal Task (F=0.06, p=0.81), Trail-Making Task (F=0.00, p=0.96), or Flanker Cost (F=1.07, p=0.34) (Table 4).
Safety outcomes
Based on the Treatment Emergent Symptom Scale, there were no differences in adverse effects reported between fish oil and placebo (F=0.30, p=0.59, data not shown). There was no difference in weight gain between fish oil and placebo (F=0.26, p=0.62). No serious side effects were reported throughout the trial.
Discussion
This trial is the first, to our knowledge, specifically designed to assess the effects of fish oil supplementation on aggression in young people presenting with impulsive aggressive behaviors. Our findings indicate that fish oil supplementation for 6 weeks had no beneficial effects on various ratings of aggressive behavior. In fact, a trend suggested that fish oil supplementation was associated with worsening aggression, on one rating of aggressive behavior. Fish oil led to a minor improvement in one measure of hyperactivity symptoms, but had no effect on any other clinical and cognitive measures. These findings suggest that fish oil is not an effective treatment for aggressive behavior in young people with disruptive behavior disorders.
Our finding, that short-term supplementation of omega-3 fatty acids did not improve aggressive behavior, is in contrast with one trial in aggressive adults, which reported that supplementation of omega-3 and omega-6 fatty acids generated reductions in violent behavior (Gesch et al. 2002). Interestingly, we observed an improvement in one rating of hyperactive symptoms. Although this may reflect a type I error, it is consistent with some trials that report that omega-3 fatty acids can improve ADHD symptoms, although meta-analyses do not support an overall beneficial effect of fatty acids for ADHD (Gillies et al. 2012). Extant clinical studies examining fish oil for behavioral outcomes exhibit substantial heterogeneity with regard to the specific omega-3s utilized, the doses used, and the concomitant use of omega-6 fatty acids. The dose used in our study was higher than that used in many other studies; therefore, our negative findings are unlikely to have resulted from inadequate doses. Despite the large number of studies published, no research has identified a specific fatty acid, minimum dose, or minimum treatment duration required to improve behavioral outcomes. It is possible that the effects of fatty acid deficiency on brain-related outcomes operate over many years, and that long-term supplementation is required to improve behavioral outcomes. However, study in adults reported beneficial effects on behavior after only 2 weeks of supplementation (Gesch et al. 2002). In addition, the trend for fish oil to worsen one aggression rating, while improvements were observed in hyperactivity, reinforces the importance of not assuming that longer treatment periods would generate beneficial effects.
The putative mechanism of omega-3 fatty acids for influencing aggression and related behaviors has not been established. It is unclear whether potential effects should be expected only in individuals who are deficient, or whether omega-3 fatty acids exert specific pharmacological effects in those with adequate serum concentrations. Omega-3 fatty acids may influence monoamine neurotransmission (Hibbeln et al. 1998a,b; Hamazaki et al. 2000, 2005), and emotional regulation via endogenous cannabinoid signaling (Lafourcade et al. 2011) both of which are implicated in the pathophysiology of aggression (Miczek et al. 2007; Siever 2008). Cognitive or executive functions have also been implicated in the etiology of aggression (Morgan and Lilienfeld 2000; Raaijmakers et al. 2008). Interest in the potential procognitive effects of fish oil continue to grow, but little research has demonstrated significant benefits in school-aged children (Karr et al. 2011).
Complementary medicines, such as fish oils, remain popular with families in many developed nations, with one study reporting rates of fish oil use in children of >30% (Barnes et al. 2008). However, given the lack of evidence for aggression, prescribers and practitioners should take a cautious approach to their use. Although generally recognized as safe, fish oil may be associated with a range of side effects, including gastrointestinal disturbances, adverse skin reactions, and increased risk of bleeding (Bays 2007). In addition, unnecessary use of complementary medicine may delay initiation of effective treatments or generate a significant financial burden. Within clinical practice, it remains important to assess use of fish oil and other complementary medicines. Use of complementary medicines in children with mental health disorders may indicate families experiencing dissatisfaction with conventional services, or represent a group at risk of poor adherence to psychotropic medicines (Dean et al. 2011).
Limitations
Our study has a number of limitations. Although our sample was adequately powered for primary analyses, the number of participants with serum concentration data available was too small to conduct potentially interesting secondary analysis, such as examining treatment effects in the subgroup with lower baseline concentrations, or examining how changing serum concentrations of different fatty acids influenced behaviors. Secondary analyses were not adjusted for multiple comparisons; however, this strengthens the likelihood that our negative findings represented a true lack of effect in this group. The absence of a washout period in the design means that treatment effects from Phase I may have influenced outcomes in Phase II. However, the influence of not incorporating a washout period was minimized by only assessing the outcomes at the end of the 6 week period; this ensures that any putative carryover effects from Phase I would have been washed out by the end of Phase II. Although the age range of our participants was narrower than that permitted by the inclusion criteria, it is possible that interventions such as fish oil may exhibit differential efficacy across developmental stages. Future studies may benefit from focusing on a narrow age range, or assessing the role of age in determining outcomes. We were not able to measure history of exposure to trauma or adversity. It is possible that such factors could influence efficacy of interventions for aggression.
Conclusions
In summary, until evidence becomes available to support the use of fish oil or fatty acid supplementation for aggression and related behaviors, clinicians should be cautious about its use. If future research does support the use of complementary therapies for aggression, it is likely that any potential role will be part of a multidimensional approach to interventions, rather than a sole intervention.
Clinical Significance
Omega-3 fatty acids are commonly used to treat externalizing behavior problems. However, little evidence has examined their efficacy for aggressive behavior. These findings suggest that fish oil is not an effective treatment for aggression.
Footnotes
Disclosures
No competing financial interests exist.