
Abstract
Objective:
The purpose of this article was to examine whether injuries in early childhood and gender predict prescriptions of stimulant medication in three groups of children: With attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and other psychiatric disorders (OPD).
Methods:
This was a population-based study with prospective and complete follow-up of children with ADHD (n=11,553), ASD (n=9698), and OPD (n=48,468), of whom 61%, 16%, and 3%, respectively, were treated with stimulants. For all 69,719 individual children data on psychiatric diagnoses, injuries, and drug prescriptions were obtained from national registers and merged.
Results:
Having sustained an injury before 5 years of age increased the likelihood of later stimulant treatment, in children with ADHD (odds ratio [OR]=1.09; 95% confidence interval [CI]=1.01–1.21), ASD (OR=1.19; 95% CI=1.02–1.40), and OPD (OR=1.24; 95% CI=1.08–1.42), with each injury increasing the likelihood by 3%, 10%, and 7%, respectively. Head injury did not increase the likelihood of later stimulant treatment. Within each of the three groups, ADHD, ASD, and OPD boys were more likely than girls to receive stimulant medication, OR=1.17 (95% CI=1.07–1.28); OR=1.71 (95% CI=1.47–2.01), and OR=2.41 (95% CI=2.16–2.71), respectively.
Conclusions:
To our knowledge, this is the first prospective study assessing early life predictors of later ADHD medication in children with a psychiatric disorder, taken from a national cohort with complete follow-up of all cases. We found that the number of injuries prior to diagnosis was associated with initiation of stimulant treatment in all three groups of patients. In addition, male gender predicted treatment with ADHD medications. Our results suggest that the number of injuries early in life prior to diagnosis is associated with stimulant treatment, and may serve as a proxy for the level of later severity of ADHD symptoms, as it is universally associated with pharmacological treatment for ADHD.
Introduction
O
Apart from the actual diagnosis of ADHD itself, very little is known about factors associated with initiation of treatment with ADHD medications in children and adolescents. Few studies have examined factors associated with medication in children with ADHD (Zito et al. 1999; Cox et al. 2003; Romano et al. 2009; Chen et al. 2011) and ASD (Witwer and Lecavalier 2005), and the majority of these were cross-sectional. Cox et al. (2003) found ADHD treatment to be associated with age, male gender, and living in communities with more Caucasians, and higher income (Cox et al. 2003). Chen et al. (2011) found that initiation of stimulant treatment was associated with being male, being older, having lower socioeconomic status (SES), and having had more than one visits to a physician (Chen et al. 2011). Other studies have also examined whether ADHD is correlated with the number of hospital contacts (Miller et al. 2004; Lee et al. 2008).
Follow-up studies of children with ADHD have also indicated an increased risk of injuries compared with controls (DiScala et al. 1998; Brehaut et al. 2003; Miller et al. 2004; Rowe et al. 2004; Xiang et al. 2005; Bruce et al. 2007; Kang et al. 2013; Ban et al. 2014), and they may be more likely to engage in risk- taking behavior (Byrne et al. 2003), anticipate fewer severe consequences of such behavior, have fewer methods of preventing injuries (Farmer and Peterson 1995), and sustain injuries to more body regions (DiScala et al. 1998). Head injuries in early childhood may also be associated with ADHD, although the direction of this association is not completely clear (Levin et al. 2007; Karver et al. 2012).
Hurtig et al. found that hyperactive symptoms before the age of 6 were associated with increased risk of injuries. However, injuries before the age of 6 were not associated with a later diagnosis of ADHD (Hurtig et al. 2013). Maxson et al. (2009) performed a screening of children who were admitted to a hospital for either an injury or for appendicitis, for symptoms of ADHD, and found the injured group to be three times more likely to screen positive for ADHD on parental reports. The authors suggest that screening injured children for ADHD may act as an injury-prevention initiative (Maxson et al. 2009).
Females with ADHD are less likely to be referred and diagnosed (Nøvik et al. 2006; Rucklidge 2010). Two previous studies have found male gender to be an important predictor of stimulant treatment in children with ADHD (Cox et al. 2003; Chen et al. 2011).
Based on these previous studies, we hypothesized that injuries may serve as a proxy for severity of ADHD symptoms and, hence, may predict pharmacological treatment of children treated for ADHD symptoms. In addition, we hypothesized that girls were less likely to be prescribed pharmacological treatment for ADHD than boys.
The objective of the present study was to examine whether gender and injuries in early childhood were associated with later being prescribed ADHD medication, when adjusted for the effect of SES and other potential confounders, in three groups of patients, namely children and adolescents with ADHD, ASD, and OPD ascertained from a population-based sample, using national registry data.
Methods
In this prospective population-based study, we merged register data, using the unique personal identification number as a key identifier to combine data across a number of national registers. The sampling of the study population and the procedures in merging the data set for this study were previously described in more detail (Dalsgaard et al. 2013).
Participants
Data from the Danish Civil Registration System (Pedersen et al. 2006) were used to identify a cohort of all persons born in Denmark between 1990 and 2001 (n=852,711). Within this birth cohort, we identified three mutually exclusive groups of patients who received an International Statistical Classification of Diseases, 10th revision (ICD-10) (World Health Organization 1993) clinical diagnosis of either ADHD (n=11,553), ASD (n=9698) or OPD (n=48,468) in either the Danish Psychiatric Central Register (DPCR) (Mors et al. 2011) or the Danish National Hospital Register (DNHR) (Andersen et al. 1999). The ICD-10 codes for ADHD included F90.0, F90.1, F90.8, and F90.9; for ASD, the codes included F84.0, F84.1, F84.8, and F84.9, and for OPD, they included any other F diagnoses. Data from a total of 69,719 children with a psychiatric disorder were included in this study. Three mutually exclusive groups were defined: 1) ADHD (may have been diagnosed with other psychiatric disorders, but never ASD), 2) ASD (may also have been given a diagnosis of ADHD or other psychiatric disorders at some point), and 3) other psychiatric disorders (never ADHD or ASD).
All children with ADHD seen at a hospital in Denmark have a data record in the registry. However, children assessed by child psychiatrists in private practices are not in the registry, and hence not included in this study. In Denmark,>63% of children and adolescents with ADHD are treated at a hospital, and systematic differences between the two groups were observed (Pottegard et al. 2012).
Children who were diagnosed with a psychiatric disorder before the age of 5 years, were excluded from the analyses (n=419). Among these, one was treated with stimulants before the age of 5.
Data on injuries
Data from DNHR gave information on injuries from birth to end of follow-up for all included individuals. Injuries were defined as ICD-10 codes of S00-T98. Within this group, a subgroup of head injuries were defined as ICD-10 codes S00-09. Only injuries that happened before the child was 5 years of age were included.
Data on prescriptions
Data on prescriptions for all drug purchases recorded in the Danish Register of Medical Product Statistics on all cases were included as the outcome. ADHD pharmacological treatment was defined as purchase of a drug containing dexamphetamine (N06BA02), methylphenidate (N06BA04), or atomoxetine (N06BA09) for a period of at least 6 months. As the vast majority of prescriptions were for methylphenidate (98.2 %), we grouped all three pharmacological agents together. Only prescriptions written after the subject was 5 years of age were included.
Baseline characteristics of study population
Data on baseline variables measured at child birth included early measures of perinatal and child health from the Medical Birth Register (e.g., length of gestation, birth complications, low birth weight, Apgar score). The study also includes data concerning any psychiatric (from DPCR) and somatic (from DNHR) diagnoses in parents, and a number of demographic and socioeconomic background variables for the parents (age, education, income, and occupation) from the Integrated Database for Longitudinal Labour Market Research. All data were collected prospectively, and merged across registers for each individual and parents of each individual.
Statistics
Multivariate logistic regression was applied to model the predictors of treatment with ADHD medication. All children and adolescents were followed prospectively from birth until date of death or December 31, 2010, whichever came first, with a follow-up rate of 100%. In collecting data on the exposure (injuries and other covariates) all children were observed from birth until their 5th birthday. In collecting data on the outcome (stimulant treatment) all children were observed from their 5th birthday until end of study. Adjusted odds ratios (OR) were calculated, with 95 % confidence intervals (CI). The estimated effect was adjusted for maternal and paternal age, income, length of education, employment status, and psychiatric and somatic disease. The statistical package SAS 9.2 was used in the analyses (SAS Institute Inc. 2000). The study was approved by the Danish Psychiatric Central Register (7-505-29-1470/1) and by the Danish Data Protection Agency (2010-41-4766).
Results
Stimulant medication was prescribed to 7021 of 11,553 subjects with ADHD (61%), 1577 of 9698 subjects with ASD (16%), and 1537 of 48,468 cases with OPD (3%). Baseline characteristics of children and adolescents with ADHD, ASD, and OPD treated with ADHD medication are shown in Table 1.
ADHD medications include methylphenidate, dexamphetamine, and atomoxetine for at least 6 months.
Baseline characteristics measured at child's birth.
Any psychiatric diagnosis, but never ADHD or ASD.
Mean and (standard deviation).
ADHD, Attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder.
Within the OPD group, the single most common diagnosis was other behavioral and emotional disorders in childhood (23%). Other common disorders within the OPD group included anxiety disorders (15%), other developmental disorders (12%), and tic disorders (8%).
Injury as a predictor of later treatment
In children with ADHD, having sustained an injury before the age of 5 and before having been diagnosed with the disorder was associated with an increased likelihood of later being prescribed stimulant medication (OR=1.09; 95% CI=1.01–1.21). Having sustained an injury was also predictive of stimulant treatment in children with ASD (OR=1.19; 95% CI=1.02–1.40) and in children with OPD (OR=1.24; 95% CI=1.08–1.42).
Number of injuries before the age of 5 was also associated with later stimulant treatment with an increased likelihood of stimulant treatment of 3% in children with ADHD (OR=1.03; 95% CI=1.01–1.07), of 10% in children with ASD (OR=1.10; 95% CI=1.04–1.17), and of 7% in children with OPD (OR=1.07; 95% CI=1.02–1.11) for every injury sustained.
Having sustained a head injury before the age of 5 was not predictive of later stimulant treatment in children with either ADHD (OR=1.16; 95% CI=0.94–1.42), ASD (OR=0.84; 95% CI=0.62–1.14), or OPD (OR=0.81; 95% CI=0.61–1.08).
Other predictors of later treatment
Birth weight<1500 g increased the likelihood of being prescribed ADHD medication in children with ASD (OR=1.83; 95% CI=1.01–3.34), but not in children with ADHD (OR=0.69; 95% CI=0.47–1.01) or OPD (OR=0.55; 95% CI=0.28–1.09). Mental retardation significantly decreased the likelihood of treatment in children with ASD (OR=0.59; 95% CI=0.49–0.71), but not in children with ADHD (OR=0.90; 95% CI=0.76–1.08), or OPD (OR=0.81; 95% CI=0.63–1.05). Gestational age, birth complications and 5 minute Apgar score did not predict treatment with ADHD medications in any of the groups (see Table 2).
ADHD medications include methylphenidate, dexamphetamine, and atomoxetine treatment for at least 6 months.
Any psychiatric diagnoses, but never ADHD or ASD.
Adjusted for maternal and paternal age, income, length of education, employment status, and psychiatric and somatic disease.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CI, confidence interval; OR, odds ratio.
Gender was a strong predictor of later treatment with ADHD medications across all three diagnostic groups (Fig. 1). Within each of the three groups, boys with ADHD, ASD, and OPD were more likely than girls to receive medications (OR=1.17, 95% CI=1.07–1.28; OR=1.71, 95% CI=1.47–2.01; and OR=2.41, 95% CI=2.16–2.71, respectively).
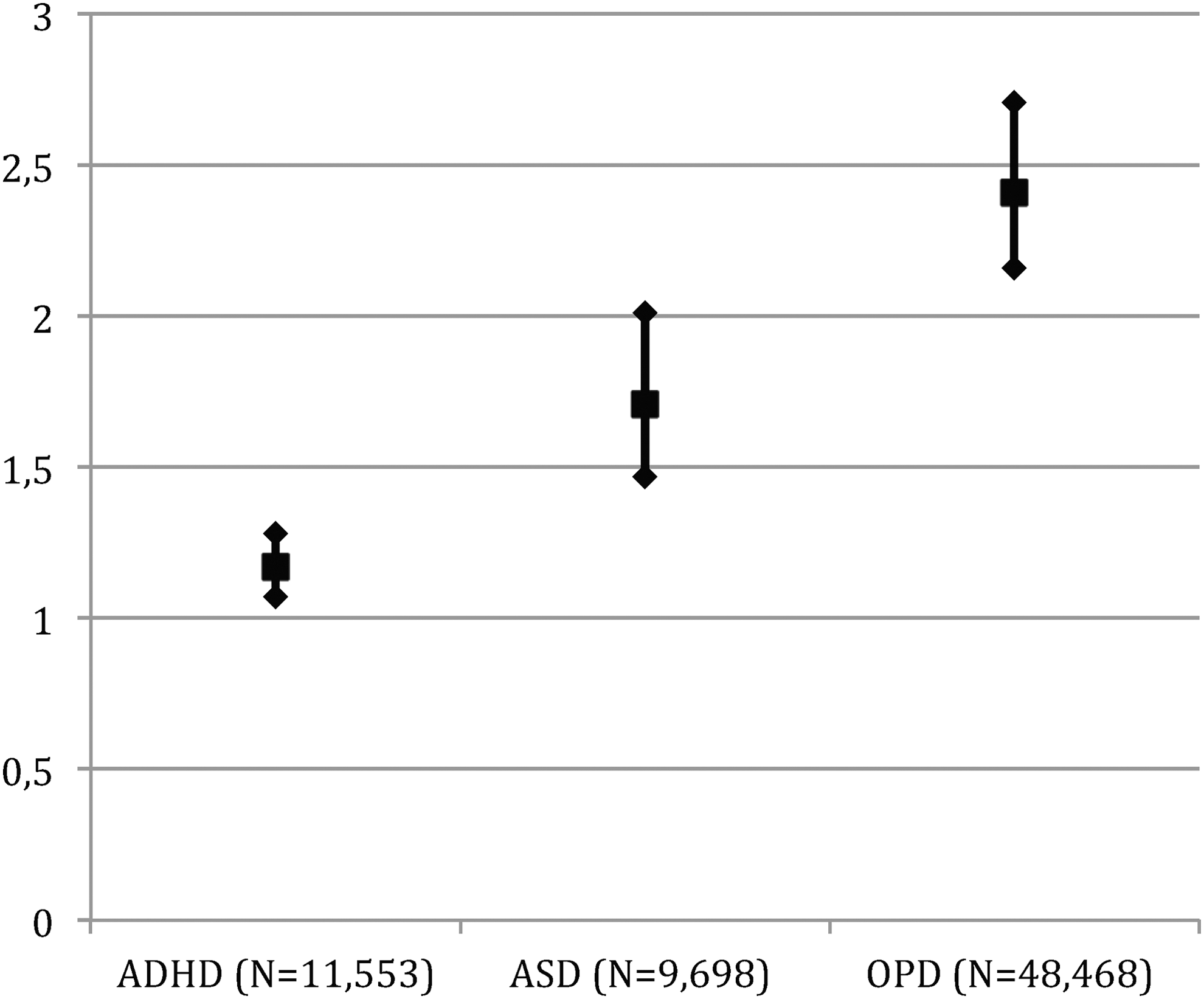
Adjusted odds ratios with 95 % confidence intervals of the predictive effect of gender (males vs. females) in initiation of stimulant medication in three mutually exclusive diagnostic groups of children with attention-deficit/ hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and other psychiatric disorders (OPD).
Sensitivity analyses
Since the prevalence of ADHD medication use increased during the study period, we also performed the analyses adjusted for birth year in an attempt to correct for a possible cohort effect. This did not change the estimated effects of predictors (data not shown). Similarly, stratifying the analyses on the types of medication (stimulant and nonstimulant) did not change the estimated effects, and as very few cases were treated with atomoxetine, we have not included the results from these stratified analyses.
Discussion
Injuries and stimulant treatment
Having sustained an injury before the age of 5 years prior to being diagnosed increased the likelihood of later initiation of ADHD medication in children with ADHD, ASD, and OPD. Additionally, the number of injuries before age 5 was also associated with later treatment, with every injury increasing the probability of later treatment by 3%, 10%, and 7% in children with ADHD, ASD, and OPD, respectively. These results suggest that injuries early in childhood may serve as a proxy for severity of ADHD. Our results are consistent with some the findings in a cross-sectional study comparing 133 children admitted to hospital for injuries and 157 children admitted for appendicitis. Based on parental reports, children admitted for injuries had more symptoms of ADHD than children admitted for appendicitis (Maxson et al. 2009). Similar findings were seen in another cross-sectional study of 72 children (Uslu et al. 2007). Some smaller previous studies have found that children who had sustained a head injury may be more likely to have undiagnosed ADHD, and are also at increased risk of developing symptoms of ADHD post-injury (Gerring et al. 1998; Levin et al. 2007; Karver et al. 2012). Our sample is much larger than those in previous studies, our follow-up prospective rather than retrospective, and we did not find head injuries before the age of 5 to be associated with initiation of stimulant treatment.
Although a number of other previous studies have found that children with ADHD are at increased risk of sustaining an injury (DiScala et al. 1998; Brehaut et al. 2003; Miller et al. 2004; Rowe et al. 2004; Xiang et al. 2005; Bruce et al. 2007; Merrill et al. 2009; Kang et al. 2013; Ban et al. 2014), this is, to our knowledge, the first prospective study to examine the association between injuries early in childhood and later stimulant treatment.
Gender and stimulant treatment
We also found that boys were 1.7–2.4 times more likely than girls to receive ADHD medication. Chen et al. (2011) found that in children with ADHD, boys were 1.4 times more likely than girls to receive stimulant treatment within the 1st year after diagnosis. In children with other psychiatric disorders, boys and girls were equally likely to receive treatment (Chen et al. 2011). Witwer and Lecavalier (2005) performed a smaller cross-sectional study of the treatment patterns of 353 children with ASD as reported by parents, and found that girls and boys with ASD were equally likely to receive any pharmacological treatment (Witwer and Lecavalier 2005). In the present study, gender differences may reflect the fact that clinicians assess hyperactive, impulsive, and inattentive symptoms in boys to be more treatable than in girls. Studies have found that the gender difference in clinical samples of children referred for assessment for ADHD range between 1:4 and 1:8, whereas the gender difference is smaller in population-based studies of the prevalence of the disorder, ranging from 1:4 to 1:2 (Nøvik et al. 2006; Rucklidge 2010). Hence, it is well established that referral bias continues to underidentify ADHD in females. Our results suggest that girls with a clinical diagnosis of ADHD are also undertreated. This is despite the fact that girls with ADHD may at higher risk of significant problems in everyday life as adults, compared with boys with ADHD (Rucklidge and Tannock 2001; Dalsgaard et al. 2002).
This possible undertreatment of girls with ADHD is also concurrent with our additional results, with significant group differences in the effect of gender between children with different psychiatric disorders. Boys were increasingly likely to be prescribed ADHD medication compared with girls, the further away from a specific ADHD diagnosis they actually were. The OR for stimulant treatment in males compared with females were OR=1.17 (in those with ADHD), OR=1.72 (in those with ASD), and OR=2.41 (in those with OPD), with no overlap in confidence intervals.
As some gender differences are seen in the population prevalence of both ADHD and ASD, with higher prevalence in males, studies comparing children treated with stimulants to the background population have naturally found higher gender differences, with boys being 3–4 times more likely to receive stimulants than girls (Zito et al. 1999; Cox et al. 2003; Sclar et al. 2012). These previous results regarding gender differences are, therefore, not comparable to ours and including only children with a psychiatric disorder, as in our study, may offer a more reliable estimate of the gender effect on the likelihood of treatment, and not be as heavily biased by the gender differences in the disorders.
Birth complications and stimulant treatment
We found low birth weight to increase the likelihood of stimulant treatment only in children with ASD, not in children with ADHD or OPD. Low birth weight is associated with ADHD, but whether it is a risk marker of ADHD or a causal effect is unknown (Thapar et al. 2012). Low birth weight has also been thought to be a risk factor for developing ASD, but a recent meta-analysis found that exposure to a range of perinatal problems may increase the risk, but in a complex interaction and not with any of these factors alone being associated with later ASD (Nosarti et al. 2012). Our findings suggest that in children diagnosed with ASD but not in children with ADHD or OPD, low birth weight may be associated with later severity of hyperactive, impulsive, or inattentive symptoms, resulting in the initiation of stimulant treatment. The effect of birth weight by itself was consistent, even after adjusting for gestational age, birth complications, and APGAR score.
Our study has limitations, as do other registry-based studies. First, diagnoses in the registers are clinical diagnoses, not the result of a systematic well-described uniform psychiatric assessment. Second, not all injuries require attending a hospital or an emergency department, and as we have not included data from general practitioners (GP), some children may have sustained an injury and received treatment at the GP without our knowledge.
The registry was not constructed for research, but for administrative purposes, and includes clinical diagnoses. The validity of OPD diagnoses has not been studied. However, the high validity of the diagnoses of ADHD and ASD in the registry has been shown, with agreement percentages of 84–95% (Madsen et al. 2002; Linnet et al. 2009; Lauritsen et al. 2010). The effects of injuries on later stimulant medication are small, but significant and clinically relevant. Absence of pharmacological treatment may reflect less severe symptoms of ADHD, but could also reflect comorbidity, differences in the treatment thresholds, or effects of other interventions. Similar to any other observational studies, we cannot exclude the possibility that children with injuries before the age of 5 may also have fatal injuries before the age of 5. These children were not included, as we only include children who are alive at the age of 5.
Conclusions
To our knowledge, this is the first study to assess early life predictors of later ADHD medication use in children with a psychiatric disorder, from a national cohort with complete follow-up of all cases. We studied predictors in a prospective design, with ascertainment of clinical cases from a population-based sample, and our results suggest that the number of injuries early in life prior to diagnosis and treatment is associated with stimulant treatment, and may serve as a proxy for the level of later severity of ADHD symptoms, as it is universally associated with pharmacological treatment for ADHD.
We also found males to be more likely to be prescribed stimulant medication than females. This is the first study to actually compare the gender differences between diagnostic groups, and the first to show that also among children with other psychiatric disorders, males are more than twice as likely to be treated with ADHD medications as females.
Gestational age, Apgar score, birth complications, and head injuries before the age of 5 were not associated with later treatment in children with either ADHD, ASD, or other psychiatric disorders.
Clinical Significance
Apart from the core symptoms of ADHD, very little is known about premorbid predictors of initiation of ADHD medications in children. Our results shed important new light on and provide insights into this field of pharmacoepidemiology, and point toward new areas in need of more research. Before any recommendations can be made on screening children with multiple injuries for symptoms of ADHD, further studies are needed on the possible association between injuries early in life and later ADHD and initiation of stimulant medication.
Disclosures
Dr. Dalsgaard is a consultant for The Danish Health and Medicines Authority. Drs. Leckman, Nielsen, and Simonsen have no conflicts of interests.
Footnotes
Acknowledgments
The authors thank Niels Gregersen for help with data management.