
Abstract
Objective:
Stimulants are recommended as a first-line treatment for attention- deficit/hyperactivity disorder (ADHD); however, a subset of the patient population augments their stimulant treatment with other medications. The objective of this study was to estimate the 1 year period prevalence of concomitant psychotropic medication use among children and adolescents with ADHD during 2009.
Methods:
Patients 6–17 years of age with one or more primary ADHD diagnoses between July 1, 2008 and December 31, 2009 and one or more stimulant prescription fills during 2009 were identified from a large United States commercial claims database. Concomitant psychotropic medication use, defined as 30 days of continuous medication supply overlap between the augmenting agent and stimulant, was evaluated for 14 distinct psychotropic medication categories (6 with a United States Food and Drug Administration (FDA) approved indication for ADHD, 8 without an indication for ADHD). The 1 year period prevalence of concomitant psychotropic medication use (both overall and within each medication category) was calculated and compared between patients with and without psychiatric or neurologic comorbidities. Children (6–12 years) and adolescents (13–17 years) were evaluated separately.
Results:
A total of 71,201 children and 49,959 adolescents met the inclusion criteria. The 1 year period prevalence of concomitant psychotropic medication use among children and adolescents was 20.3% and 23.4%, with 5.7% and 6.7% augmenting with two or more medication categories, respectively. The most common concomitant medication categories were selective serotonin reuptake inhibitors (SSRIs) (children: 6.2%; adolescents: 11.4%), atypical antipsychotics (5.8%; 6.8%) and clonidine immediate release (5.4%; 2.9%). Children and adolescents with psychiatric or neurologic comorbidities had higher rates of augmentation than did those without comorbidities (all p<0.001).
Conclusions:
This epidemiologic study found that the prevalence of concomitant psychotropic medication use in children and adolescents ranged from 12.6% for noncomorbid ADHD to 41.7% for comorbid ADHD, in 2009. Future research is warranted to evaluate the rationale for, and clinical benefit of, concomitant psychotropic medication usage in patients with ADHD.
Introduction
A
Medication management has been shown to be cost effective for the treatment of ADHD (Wu et al. 2012). Psychostimulants are typically the first-line pharmacologic therapy, with ∼70% of patients responding to this treatment in short-term studies (6–10 weeks) (May and Kratochvil 2010; Wolraich et al. 2011). However, for a variety of reasons, including inadequate or partial response and dose-limiting side effects, there is evidence that some ADHD patients augment their existing stimulant regimen with additional medications (Pliszka 2003; Banaschewski et al. 2004). Currently, the only therapies approved by the United States Food and Drug Administration (FDA) for adjunctive treatment of ADHD in children and adolescents are guanfacine extended release (XR) and clonidine XR (Ming et al. 2011; Childress 2012). In practice, however, other medications are prescribed off label for the treatment of ADHD alongside stimulants, including antipsychotics, antidepressants, nonstimulants, and other stimulants (as adjunctive therapy) (Pappadopulos et al. 2002; Spencer and Biederman 2002; Cooper et al. 2004, 2006; Zito et al. 2008; Czaja and Valuck 2012).
Despite a recommendation by the American Academy of Pediatrics against off-label, adjunctive drug therapy for the treatment of ADHD, concomitant psychotropic medication use in practice is substantial and has been increasing (Martin et al. 2003; Safer 2003; Bhatara et al. 2004; dosReis et al. 2005; Duffy et al. 2005; Jensen et al. 2005; Chen et al. 2009; Comer et al. 2010; Elbe 2011; Wolraich et al. 2011). Between 1996 and 2007, the proportion of children's outpatient visits in which psychotropic medications from two or more medication classes were prescribed increased from one in seven visits to one in five visits (Comer et al. 2010). Unfortunately, the growth in concomitant psychotropic medication has not been sufficiently supported by safety/efficacy data to inform the practice (Bhatara et al. 2004; Comer et al. 2010).
Although the practice of concomitant psychotropic medication usage is well documented, there is little evidence to describe the overall rates of such usage among commercially insured children and adolescents with ADHD, and the evidence to guide patients, clinicians, and payers on this subject is sparse (Bussing and Winterstein 2012). Such practice-based information about concomitant psychotropic medication usage is particularly important, given that the use of off-label therapies for ADHD is controversial (Pappadopulos et al. 2002; Cooper et al. 2004, 2006; Zito et al. 2008; Weiss et al. 2009; Wilens 2009; Alexander et al. 2011; Pathak et al. 2010a; Matone et al. 2012; Sikirica et al. 2012b). Furthermore, recent studies have also questioned the possible negative effects of polypharmacy on ADHD patients, citing concerns of potentially opposing effects on dopamine regulation and potential risks, including inducing metabolic syndrome and its sequelae (Findling et al. 2005; Penzner et al. 2009; Weiss et al. 2009; Wilens 2009; Yanofski 2010; Maglione et al. 2011; Bussing and Winterstein 2012).
Accordingly, this study examines the prevalence of concomitant psychotropic medication use (including medications used off label) among commerically insured children and adolescents with ADHD during 2009. Furthermore, as patients may have common psychiatric or neurologic comorbidities that may be treated with these supplemental medications, the 1 year period prevalence of concomitant psychotropic medication use is also compared between children and adolescents with psychiatric or neurologic comorbidities and those without.
Methods
Data
This study was conducted using data from the Truven Health MarketScan Commercial Claims & Encounters database (MarketScan) from the period of July 1, 2008 to December 31, 2009. These data include commercial health insurance claims and enrollment information from large United States employers and health insurance plans. Such plans provide private healthcare coverage for >45,000,000 employees, their spouses, and dependents, and reflect a variety of fee-for-service, preferred provider organization, and capitated health plans.
Sample selection
Patients with at least one primary ADHD diagnosis (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] codes 314.00 or 314.01) between July 1, 2008 and December 31, 2009 were identified. Patients were required to be 6–17 years of age as of January 1, 2009, have continuous health plan enrollment eligibility during the baseline (July 1, 2008 to December 31, 2008) and study (January 1, 2009 to December 31, 2009) periods, and have at least one filled prescription for a stimulant (identified using generic product identifier [GPI] codes) during the study period. The first stimulant filled in 2009 was defined as the index stimulant. Both the rates of ADHD diagnosis and ADHD treatment vary by age; therefore children (age 6–12) and adolescents (13–17) were analyzed separately (Cooper et al. 2004; Constantine and Tandon 2008).
Patients were then stratified by whether or not they had any psychiatric or neurologic comorbidities during the study period. Specifically, patients with any primary diagnoses of bipolar disorder, dementia, mania, schizophrenia, tics, adjustment disorder, anxiety disorder, conduct disorder, depression, insomnia, learning disability, obsessive compulsive disorder, oppositional defiant disorder, substance abuse, pervasive developmental disorder, epilepsy, and other psychiatric or neurologic disorders (as identified by ICD-9-CM codes; see Appendix A) between July 1, 2008 and December 31, 2009 were considered comorbid ADHD patients. Patients with the absence of these diagnoses were considered noncomorbid ADHD patients.
Measures
Concomitant psychotropic medication usage during the 2009 calendar year was evaluated for 14 distinct categories, which either had an FDA-approved indication for ADHD or could be used off label to treat ADHD in practice (Spencer and Biederman 2002; Cooper et al. 2004, 2006; Zito et al. 2008). These psychotropic medication categories included two classes of short duration of action stimulants (amphetamine [AMPH] short acting [SA], and methylphenidate (MPH) SA), two classes of long duration of action stimulants (AMPH long acting [LA] and MPH LA), two nonstimulants approved for ADHD (atomoxetine and guanfacine XR), two nonstimulants not approved for ADHD (clonidine immediate release [IR] and guanfacine IR), two classes of antipsychotics (atypical antipsychotics [AAPs] and typical antipsychotics [TAPs]), and four classes of antidepressants (bupropion, selective serotonin reuptake inhibitors [SSRIs], serotonin-norepinephrine reuptake inhibitors [SNRIs], and tricyclic antidepressants [TCAs]).
For a medication fill to qualify as concomitant usage, the medication had to have been filled in 2009 and have at least 30 days of supply overlap with the index stimulant, and there had to be at least one primary diagnosis of ADHD recorded prior to the end of medication overlap. For two stimulants to qualify as concomitant usage, the new stimulant had to be a different class than the index stimulant. Patients were classified into multiple categories if they used more than one medication category concomitantly (patients using multiple medication categories concomitantly would be counted multiple times, once for each concomitant medication). Patients who had separate periods of concomitant medication use with the same medications were only counted once. When evaluating multiple augmentations, the periods of overlap between the index stimulant and differing augmenting medications were not required to be mutually exclusive.
The 1 year period prevalence of concomitant psychotropic medication use overall and within each of the 14 distinct medication categories was calculated within 2009. The overall 1 year prevalence of concomitant psychotropic medication use was calculated as the percentage of patients experiencing at least one instance of concomitant usage with any of the 14 distinct psychotropic medication classes during 2009. The 1 year period prevalence of concomitant psychotropic medication use for each medication category was calculated as the proportion of patients experiencing at least one instance of concomitant usage with the given medication category within the 2009 calendar year.
Statistical analysis
Separate analyses were performed for the child and adolescent cohorts. Among these groups, baseline demographic characteristics were compared between patients who augmented stimulant treatment and those who did not augment, using Wilcoxon rank sum tests for continuous variables and χ2 tests for categorical characteristics. The period prevalence of concomitant psychotropic medication use for each medication category was compared between comorbid and noncomorbid patients using χ2 tests. No multivariate adjustments were made for comparisons of comorbid and noncomorbid patients. All analyses were performed using SAS Version 9.2 (SAS Institute, Cary, NC), and statistical significance was evaluated at the 0.05 significance level (two sided).
Results
Children
A total of 71,201 children met the inclusion criteria (Fig. 1). Among this sample of children, 22,796 (32.0%) had at least one diagnosed psychiatric or neurologic comorbidity, and the remaining 48,405 were noncomorbid ADHD patients. Among all children, 14,455 (20.3%) patients had at least one instance of concomitant psychotropic medication usage during the study period, and 4,071 (5.7%) had two or more instances with different psychotropic medications (Table 1). Compared with patients who did not have concomitant medication use, children with ADHD who had concomitant medication use were slightly older (9.5 vs. 9.3 years old; p<0.001), had more psychiatric and neurologic comorbidities (55.6% vs. 26.0%; p<0.001), or a greater proportion were male (75.6% vs. 71.9%; p<0.001).
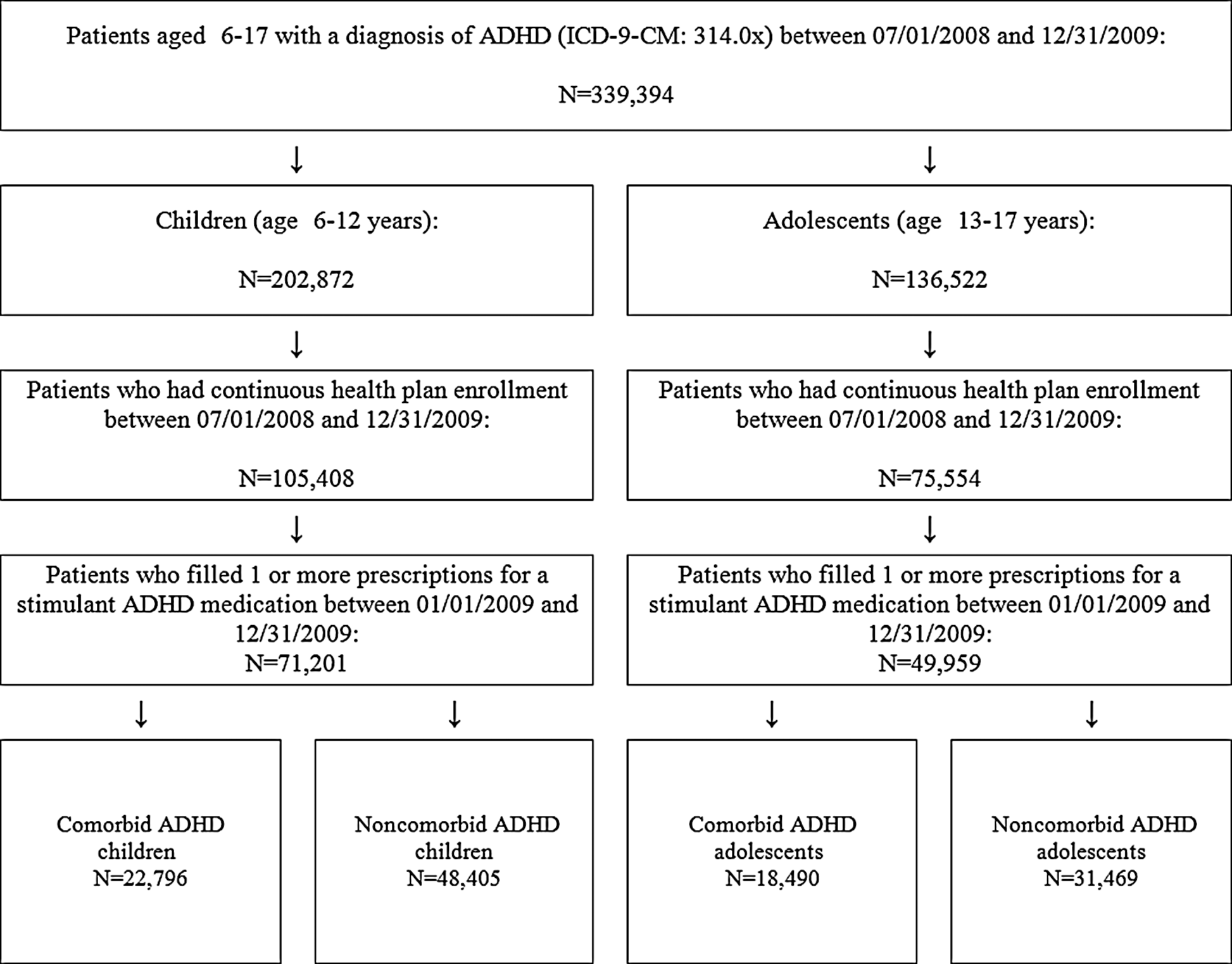
Sample selection flowchart.
Number (n) and frequency (%) are given for each category. Number of concomitantly used medications refers to the number of different medication categories the patient used concomitantly with a stimulant at any time during 2009.
Patients are counted only once per column, and, therefore, rows are mutually exclusive of each other.
Among all children, the 1 year period prevalence of concomitant psychotropic medication use for each medication category (ordered from most to least prevalent) was SSRIs (6.2%), AAPs (5.8%), clonidine IR (5.4%), atomoxetine (2.2%), guanfacine IR (1.9%), MPH SA (1.4%), AMPH LA (1.4%), MPH LA (1.1%), AMPH SA (1.0%), TCAs (0.5%), bupropion (0.5%), guanfacine XR (0.3%), SNRIs (0.1%) and TAPs (0.1%) (Table 2).
AAPs, atypical antipsychotics; ADHD, attention-deficit/hyperactivity disorder; AMPH, amphetamine; IR, immediate release; LA, long acting; MPH, methylphenidate; SA, short acting; SNRIs, serotonin-norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; TAPs, typical antipsychotics; TCAs, tricyclic antidepressants; XR, extended release.
In the noncomorbid ADHD cohort, 6,412 (13.2%) children had at least one instance of concomitant psychotropic medication use. The 1 year period prevalence of concomitant psychotropic medication use for each medication category in the noncomorbid cohort was clonidine IR (4.1%), AAPs (2.6%), SSRIs (2.3%), atomoxetine (1.7%), MPH SA (1.2%), guanfacine IR (1.2%), AMPH LA (1.1%), MPH LA (0.9%), AMPH SA (0.8%), TCAs (0.3%), bupropion (0.3%), guanfacine XR (0.2%), SNRIs (0.03%), and TAPs (<0.01%) (Table 2).
In the comorbid cohort, 8,043 (35.3%) children had at least one instance of concomitant psychotropic medication use. The 1 year period prevalence of concomitant psychotropic medication use was significantly higher (p<0.001) for each of the 14 medication categories among comorbid ADHD patients, compared with noncomorbid ADHD patients.
Adolescents
A total of 49,959 adolescents met the inclusion criteria (Table 1). In the adolescent sample, 18,490 (37.0%) were comorbid ADHD patients, and 31,469 were noncomorbid. Among all adolescents, 11,680 (23.4%) patients had at least one instance of concomitant psychotropic medication usage during the study period, and 3,327 (6.7%) patients had two or more instances (Table 1). When compared with patients who did not have concomitant psychotropic medication usage, adolescents who had concomitant psychotropic medication usage were significantly older (14.92 vs. 14.86; p<0.001), had more psychiatric and neurologic comorbidities (66.0% vs. 28.2%; p<0.001), or a greater proportion were female (33.3% vs. 29.9%; p<0.001).
In the adolescent cohort, the 1 year period prevalence of concomitant psychotropic medication use for each medication category (ordered from most to least prevalent) was SSRIs (11.4%), AAPs (6.8%), clonidine IR (2.9%), bupropion (2.3%), atomoxetine (1.8%), AMPH LA (1.2%), guanfacine IR (1.1%), AMPH SA (1.1%), MPH SA (1.0%), SNRIs (0.8%), MPH LA (0.6%), TCAs (0.5%), guanfacine XR (0.1%), and TAPs (0.1%) (Table 2).
In the noncomorbid ADHD cohort, 3,974 (12.6%) adolescents had at least one instance of concomitant psychotropic medication use. The 1 year period prevalence of concomitant psychotropic medication use in the noncomorbid sample was SSRIs (4.2%), AAPs (2.4%), clonidine IR (1.9%), atomoxetine (1.6%), bupropion (1.0%), AMPH LA (0.9%), MPH SA (0.9%), AMPH SA (0.9%), guanfacine IR (0.7%), MPH LA (0.5%), TCAs (0.3%), SNRIs (0.2%), guanfacine XR (0.1%), and TAPs (0.03%) (Table 2).
In the comorbid ADHD cohort, 7,706 (41.7%) adolescents had at least one instance of psychotropic medication usage. Similar to the result for children, the 1 year period prevalence of concomitant psychotropic medication use was significantly higher (p<0.05) for each of the 14 medication categories among comorbid ADHD patients, than among noncomorbid ADHD patients.
Discussion
To our knowledge, this is the first study to assess the prevalence of concomitant psychotropic medication use with antipsychotics, antidepressants, nonstimulants, or other stimulants among commercially insured children and adolescents with ADHD in the United States. This study found that overall, 20.3% of children and 23.4% of adolescents had at least one instance of concomitant psychotropic medication use during 2009. Furthermore, the study observed that 5.7% of children and 6.7% of adolescents had two or more instances of concomitant medication use (with different psychotropic medication categories) during the study period. These results are qualitatively similar to a study in adult ADHD which found that in 2003–2004, combination therapy was present in roughly 21.0–27.4% of the patient therapy months (Pohl and Brunt 2009).
Potential differences in concomitant medication utilization could be attributable to a number of factors, including age and gender (Biederman et al. 2002; Safer 2003). In the current study, 18.2% of female children and 25.4% of female adolescents had at least one instance of concomitant psychotropic medication use, compared with 21.1% of male children and 22.5% of male adolescents having similar usage patterns. Future demographic analyses may provide more insight regarding the mechanisms underlying concomitant medication use.
In the analyses of both children and adolescents, patients with psychiatric or neurologic comorbidities had a higher prevalence of concomitant psychotropic medication usage (among all studied medication categories) than noncomorbid patients. However, the prevalence of concomitant psychotropic medication use remained high in patients without comorbidities. In the noncomorbid population, 13.2% of children and 12.6% of adolescents had at least one instance of concomitant use, and 2.7% of children and 2.4% of adolescents had two or more instances. Although the adolescent and child cohort were analyzed separately, it is interesting to note that for adolescents, the rates of concomitant psychotropic medication use were higher in the overall population and lower in the noncomorbid population. Further research is needed to evaluate the reasons for these differences.
The prevalence of concomitant psychotropic medication use among the noncomorbid children and adolescents is especially relevant, as such events are likely to be related to ADHD treatment, rather than on-label uses for other comorbid conditions. Furthermore, high prevalence of concomitant psychotropic medication use is noteworthy, given that during 2009, there were no medications approved by the FDA for use as adjunctive therapy with psychostimulants.
Although none of the medication categories studied were approved to be used adjunctively with stimulants during the study period, the most commonly used concomitant psychotropic medications were not approved by the FDA as monotherapy for the treatment of ADHD. SSRIs were the most commonly used concomitant agent in both children (6.2%) and adolescents (11.4%). The majority of this concomitant use (74.7% in children and 76.9% in adolescents) occurred in patients with psychiatric and neurologic comorbidities (e.g., anxiety disorder or depression). However, SSRIs were also used concomitantly for noncomorbid children and adolescents as well (in 2.3% of children and 4.2% of adolescents). These results are noteworthy, particularly given the sparse clinical evidence regarding the efficacy and safety of SSRIs for the treatment of ADHD. AAPs were the second most commonly used concomitant agents in both children (5.8%) and adolescents (6.8%). They were also the second most commonly used concomitant agents among noncomorbid children (2.6%) and adolescents (2.4%). This prevalence rate is potentially concerning, given the lack of demonstrated efficacy for this purpose and the unknown safety profile, including the potential risk of serious adverse events with AAPs (Penzner et al. 2009; Yanofski 2010; Bussing and Winterstein 2012). A detailed breakdown of the psychiatric and neurologic comorbidities of patients who concomitantly used SSRIs and those who concomitantly used AAPs is provided in Appendix B.
The nonstimulants clonidine IR and guanfacine IR were also commonly used concomitantly with simulants (5.4% and 1.9% of children and 2.9% and 1.1% of adolescents with clonidine IR and guanfacine IR, respectively). These medications have the same active ingredient as clonidine XR and guanfacine XR, respectively. Since the completion of the study period, clonidine XR and guanfacine XR were approved by the FDA for monotherapy or adjunctive therapy with stimulants in the treatment of ADHD in children and adolescents. They also have different pharmacokinetic profiles than their IR counterparts (Strange 2008). In contrast, the efficacy and safety profiles of clonidine IR and guanfacine IR for the treatment of ADHD have not been well established in adequate and well-controlled studies. Additionally, there is evidence from retrospective claims database studies that ADHD patients using guanfacine IR may experience greater medical resource utilization and higher medical costs than guanfacine XR patients in practice (Sikirica et al. 2013).
Especially among noncomorbid ADHD patients, the off-label use of medications observed in this study, although controversial, is, perhaps, explained by the relative paucity of clinical evidence regarding the efficacy and safety for concomitant therapy (Pappadopulos et al. 2002; Cooper et al. 2004, 2006; Weiss et al. 2009; Pathak et al. 2010a; Alexander et al. 2011; Bussing and Winterstein 2012). The American Academy of Pediatrics notes that only guanfacine XR and clonidine XR have clinical evidence to support their use as adjunctive therapy in children and adolescents who partially respond to stimulants (Wolraich et al. 2011). Guanfacine XR has also been demonstrated to be a cost-effective alternative to stimulant monotherapy among children and adolescents with suboptimal response to stimulants (Sikirica et al. 2012a). The availability of these newer FDA-approved stimulant adjunctive therapies may help address the potential need for augmenting medications for the treatment of ADHD.
Limitations
This study was conducted using administrative claims data, which is associated with certain limitations. Concomitant psychotropic medication use was defined based on a period of overlapping prescription fills rather than clinician intent to treat concomitantly. This approach allowed real utilization to be captured (e.g., whether the patients actually filled the prescriptions), but did not provide insight into the exact reasons the medications were prescribed, or the intended frequency of concomitant therapy in ADHD. Consequently, there may be difficulties in determining whether the concomitant psychotropic medication was actually used in the treatment of ADHD, and not for other mental health indications. In fact, patients with comorbid ADHD who were labeled as having concomitant psychotropic medication use may have been using the concomitant medication for its on-label indication and the stimulant for ADHD (e.g., ADHD patients with comorbid depression who concomitantly used SSRIs). To address these concerns, an additional subpopulation of patients who did not have any psychiatric or neurologic comorbidities was investigated, and, as expected, the prevalence of concomitant medication use was lower than in the comorbid patients. However, it is possible that some of the noncomorbid ADHD patients may have had mental health conditions that were not recorded in the Truven database (possibly because of stigmas attached to psychiatric diagnoses, lack of clarity in patient presentation, or patients not fulfilling the full diagnostic criteria at the time of visit). Furthermore, this noncomorbid subpopulation will not be generalizable to the entire ADHD population, many of whom are characterized as having a heavy comorbidity burden (Larson et al. 2011).
Previous studies have suggested that psychiatrists are more likely to prescribe concomitant psychotropic medications for youth than are primary care physicians (Bussing et al. 1998; Epstein et al. 1991; Safer 2003). However, the lack of detail regarding prescriber specialty found in this administrative claims database prohibits this hypothesis from being formally evaluated in the current study.
Finally, these results are only generalizable to the commercially insured population in the United States, which may not be representative of all children and adolescents in the United States, particularly those using public insurance programs. Recent studies conducted in state Medicaid and Children's Health Insurance Programs (CHIP) suggest that children and adolescents with public insurance have higher rates of concomitant medication use than those with private insurance (Martin et al. 2003; dosReis et al. 2005; Chen et al. 2009). For example, a retrospective analysis of the Connecticut Medicaid managed care database found that 28–30% of youth with psychotropic medication use received multiple medications (Martin et al. 2003), which exceeds the rates described in the present study. Additional studies have found the source of funding for services to be significantly associated with concomitant pharmacotherapy, with the highest rates observed among patients with public insurance (Duffy et al. 2005; Chen et al. 2009; Comer et al. 2010). Children and adolescents on public insurance have also been shown to have higher than expected rates of AAP utilization (Constantine and Tandon 2008; Crystal et al. 2009; Pathak et al. 2010b; Matone et al. 2012). This is an important consideration, given that more than one in every three children are covered through Medicaid and CHIP (The Kaiser Commission on Medicaid and the Uninsured 2013).
Conclusions
This study quantifies the prevalence of concomitant psychotropic medication use among children and adolescents in the United States during 2009. Despite the fact that none of the 14 psychotropic medication classes studied were approved by the FDA for adjunctive use with psychostimulants, concomitant use was observed in both children and adolescents, ranging from 12.6% for noncomorbid ADHD to 41.7% for comorbid ADHD. Future research is warranted to evaluate the rationale for, and clinical benefit of, concomitant psychotropic medication use in patients with ADHD.
Clinical Significance
In the management of ADHD among children and adolescents, clinicians should evaluate patients on a case-by-case basis, taking into account their unique characteristics and the defined risk–benefit profile for different treatment options. However, the risk–benefit profile of many medications used concomitantly with stimulants in practice is largely unknown. Given that there are currently FDA-approved nonstimulants that have been demonstrated to be safe and effective for adjunctive use alongside stimulants in children and adolescents, further research is required to evaluate the efficacy, safety, and economic impact of using psychotropic medications concomitantly to treat ADHD.
Footnotes
Acknowledgments
The authors thank Julia Dibello, who was an employee of Shire Development LLC at the time of this work, for her contributions in the conceptual design and data interpretation, and Andrew Kageleiry, who is employed by Analysis Group, for his contributions in drafting and editing the manuscript.
Disclosures
Drs. Sikirica, Hodgkins, and Erder are employees of Shire Development LLC and hold stock or stock options with Shire; Dr. DeLeon was an employee of Shire Development LLC at the time of this work. Drs. Betts, Xie, and Wu and Mr. Zhou are employees of Analysis Group, Inc., which received funding from Shire for this study.
Shire Pharmaceuticals LLC is a manufacturer of several products for the treatment of attention-deficit/hyperactivity disorder (ADHD), including guanfacine extended release.
| Comorbidity | ICD-9 Code |
|---|---|
| Psychiatric disorders associated with atypical antipsychotics: | |
| Bipolar disorder | 296.4, 296.5, 296.6, 296.7, 296.8 |
| Dementia | 290, 294.1 |
| Mania | 296.0, 296.1 |
| Other psychotic disorders | 293.81, 293.82, 297.1, 297.3, 298.8, 298.9 |
| Schizophrenia | 295 |
| Tics | 307.2 |
| Psychiatric comorbidities associated with ADHD: | |
| Adjustment reaction | 309.xx |
| Anxiety disorder | 293.84, 300.0x, 300.2x, 313.0x |
| Conduct disorder | 312.xx |
| Depression | 296.2x, 296.3x, 311.xx, 300.4x |
| Epilepsy | 345.xx |
| Insomnia | 307.41, 307.42, 327.0x, 780.51, 780.52 |
| Learning disability | 315.xx |
| Obsessive-compulsive disorder | 300.3x |
| Oppositional defiant disorder | 313.81 |
| Substance abuse | 291.xx, 292.xx, 303.xx, 304.xx, 305.xx |
| Pervasive developmental disorder | 299.x |
| Other neurological disorders | 320.xx-337.xx, 340.xx-349.xx excludes 345.xx |
ADHD, attention-deficit/hyperactivity disorder; ICD-9, The International Classification of Diseases, Ninth Revision
| Children | Adolescents | |||
|---|---|---|---|---|
| Comorbidities n (%) | SSRIs n=4,393 | AAPs n=4,161 | SSRIs n=5,712 | AAPs n=3,411 |
| Adjustment disorder | 399 (9.1%) | 326 (7.8%) | 559 (9.8%) | 266 (7.8%) |
| Anxiety disorder | 773 (17.6%) | 338 (8.1%) | 773 (13.5%) | 300 (8.8%) |
| Bipolar disorder | 137 (3.1%) | 402 (9.7%) | 281 (4.9%) | 586 (17.2%) |
| Conduct disorder | 165 (3.8%) | 255 (6.1%) | 135 (2.4%) | 178 (5.2%) |
| Dementia | 0 (0%) | 0 (0%) | 0 (0.0%) | 2 (0.1%) |
| Depression | 423 (9.6%) | 287 (6.9%) | 1,228 (21.5%) | 568 (16.7%) |
| Epilepsy | 55 (1.3%) | 69 (1.7%) | 53 (0.9%) | 55 (1.6%) |
| Insomnia | 22 (0.5%) | 24 (0.6%) | 51 (0.9%) | 32 (0.9%) |
| Learning disability | 89 (2.0%) | 92 (2.2%) | 46 (0.8%) | 34 (1.0%) |
| Mania | 4 (0.1%) | 11 (0.3%) | 13 (0.2%) | 23 (0.7%) |
| Obsessive compulsive disorder | 137 (3.1%) | 68 (1.6%) | 180 (3.2%) | 79 (2.3%) |
| Oppositional defiant disorder | 219 (5.0%) | 329 (7.9%) | 217 (3.8%) | 272 (8.0%) |
| Other neurologic disorders | 194 (4.4%) | 158 (3.8%) | 224 (3.9%) | 135 (4.0%) |
| Other psychotic disorders | 14 (0.3%) | 23 (0.6%) | 34 (0.6%) | 46 (1.3%) |
| Pervasive developmental disorder | 317 (7.2%) | 374 (9.0%) | 250 (4.4%) | 247 (7.2%) |
| Substance abuse | 4 (0.1%) | 7 (0.2%) | 156 (2.7%) | 123 (3.6%) |
| Schizophrenia | 3 (0.1%) | 6 (0.1%) | 12 (0.2%) | 15 (0.4%) |
| Tics | 59 (1.3%) | 59 (1.4%) | 52 (0.9%) | 53 (1.6%) |
| No comorbidities | 1,110 (25.3%) | 1,271 (30.5%) | 1,318 (23.1%) | 745 (21.8%) |
AAPs, atypical antipsychotics; ADHD, attention-deficit/hyperactivity disorder; SSRIs, selective serotonin reuptake inhibitors.