
Abstract
Objective:
Little is known regarding demographic and/or clinical characteristics associated with the use of lithium among adolescents with bipolar disorder (BP) in naturalistic clinical settings. We therefore examined factors associated with lithium among adolescents with BP presenting to a tertiary outpatient clinic.
Methods:
Participants were 100 adolescents 13–19 years of age, with BP-I, BP-II, or BP not otherwise specified (BP-NOS). Diagnoses and lifetime medication exposure were determined using the Schedule for Affective Disorders and Schizophrenia for School Age Children, Present and Lifetime Version (KSADS-PL). Analyses examined for demographic and clinical correlates of lifetime lithium exposure.
Results:
Twenty percent of participants reported lifetime lithium use. Participants with, versus those without, lifetime lithium use were significantly older and significantly more likely to have BP-I, lifetime history of psychiatric hospitalization, and psychosis. Lithium-treated participants were significantly more likely to report use of second-generation antipsychotics (SGAs) and antimanic anticonvulsants. In contrast, participants with lithium exposure were significantly less likely to have BP-II, self-injurious behavior, and a family history of depression. Adolescents with lithium exposure had significantly less parent-reported family conflict and mood lability, and significantly less self-reported impulsivity, emotional dysregulation, identity confusion, and interpersonal problems. In multivariable analyses, lithium use was associated with greater lifetime SGA use, lower parent-reported family conflict, and lower adolescent-reported interpersonal problems.
Conclusions:
Lithium was infrequently used among adolescents with BP in this sample. Although constrained by retrospective methodology and a single site, our findings suggest that clinicians may be deferring lithium use until late in treatment. The fact that there are lower rates of lithium use among adolescents with suicidal ideation, impulsivity, mood lability, and family history of depression suggests potential missed opportunities for use of lithium among high-risk adolescents with BP.
Introduction
B
Nonetheless, the existing literature, including naturalistic, open-label, and active comparator randomized control trials (RCTs) of lithium among youth with BP, suggests that there may be an important role for lithium in acute mania, acute bipolar depression, continuation, and maintenance, and in the treatment and possibly prevention of comorbid substance use disorders (SUD) (Strober et al. 1990; Geller et al. 1998; Kafantaris et al. 2003; Findling et al. 2005; Patel et al. 2006a; Geller et al. 2010; Goldstein et al. 2013). For example, greater lithium exposure and/or early response to lithium may predict better prospective course of BP among youth (Strober et al. 1990; Geller et al. 2010). Furthermore, lithium exposure has been associated with greater amygdalar gray matter volume in youth with BP (Chang et al. 2005); putatively beneficial effects of lithium on neural chemistry have also been demonstrated (Patel et al. 2006b, 2008). Despite the recognition that lithium continues to have an important role in the treatment of adolescents with BP (Singh and Zarate 2006; Pfeiffer et al. 2010; Goldstein et al. 2012), little is known regarding demographic and/or clinical characteristics associated with the use of lithium among adolescents with BP in naturalistic clinical settings.
Findings from adults with BP suggest that lithium use is more likely among those with suicidal ideation (SI), suicide attempts (SA) (Goldberg et al. 2005), and psychiatric hospitalizations (Frangou et al. 2002) and of Caucasian race (Kilbourne and Pincus 2006; Depp et al. 2008). In one adolescent sample, patients treated with lithium were older and had later BP onset than those taking valproate or SGAs (Masi et al. 2010). There is a paucity of data that would inform about which youth are most likely to benefit from lithium, although the TEAM study found that youth enrolled following clinical referral and those who have experienced greater maternal warmth may be more likely to respond to lithium (Geller et al. 2012; Vitiello et al. 2012).
We expect that information on who is treated with lithium could potentially inform treatment planning and selection. Therefore, in the present study, we set out to examine the correlates of lifetime exposure to lithium in a clinical sample of adolescents with BP, as this may help inform treatment decisions and identify subgroups of youth with BP for whom lithium may be underutilized. Based on the current literature (Frangou et al. 2002; Goldberg et al. 2005; Kilbourne and Pincus 2006; Depp et al. 2008; Masi et al. 2010), we predicted that older age, Caucasian race, psychiatric hospitalization, SI, and SA would be positively associated with lithium treatment.
Methods
Participants
Participants were recruited consecutively from new clinical referrals to a tertiary subspecialty clinic for adolescent BP at an academic health sciences center, drawn from across the province of Ontario. The vast majority of participants (>90%) were referred by external physicians (psychiatrists, pediatricians, primary care physicians); the remainder were referred by attending adolescent psychiatrists in the general youth psychiatry division of the academic health sciences center. At least one parent/guardian for each adolescent was also interviewed. Participants with BP (n=100; 67 females, 33 males) were 13–19 years of age (mean=16.18, SD=1.47). There were 26 participants with BP-I, 40 with BP-II, and 34 with BP not otherwise specified (BP-NOS), as determined by the Schedule for Affective Disorders and Schizophrenia for School-Age Children, Present and Lifetime Version (KSADS-PL) (Kaufman et al. 1997). Lifetime psychotropic medication exposure was obtained during the KSADS-PL interview with the adolescent and his/her parent/s during the intake assessment, reflecting treatment obtained prior to involvement with the tertiary subspecialty clinic. Psychotropic medication exposure was not systematically confirmed with the participants' medical records.
Procedure and measures
Information reported here was gathered through a clinical research registry. This study was approved by the local research ethics board. Participants and their parents provided written informed consent prior to participation. After hearing a description of the study from research staff, and having the opportunity to review the informed consent form, adolescent and parent participants had the opportunity to ask questions about the study procedures and potential risks and benefits. For the final part of the informed consent process, a quiz was administered to the adolescents to confirm their understanding of the study. Data collection began after participants and their parents provided written informed consent.
Current and lifetime diagnoses were determined with the KSADS-PL, which incorporates information from both adolescents and their parents or guardians. The KSADS Depression Rating Scale (DRS) (Chambers et al. 1985) and KSADS Mania Rating Scale (MRS) (Axelson et al. 2003) were used in place of the mood sections of the KSADS-PL. All interviewers had completed a bachelor's or master's degree in a health science field and had undergone KSADS training under the supervision of the senior author (B.G.).
The age of BP onset was defined as the age at which the individual first met Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria for a manic, hypomanic, or major depressive episode, or when the participant first met study criteria for BP-NOS (American Psychiatric Association 1994). The Course and Outcome of Bipolar Youth (COBY) study criteria were used to operationally define BP-NOS, as DSM-IV does not specify such criteria (Birmaher et al. 2006). The criteria are as follows: 1) Two DSM-IV manic symptoms (three if only irritable mood is reported), 2) change in functioning, 3) mood and symptom duration of at least 4 hours during a 24 h period, and 4) at least four cumulative 24 hour periods of episodes that meet the mood, symptom, and functional change criteria over the participant's lifetime.
Lifetime history of physical and/or sexual abuse was determined via the screening questions for posttraumatic stress disorder (PTSD) within the KSADS-PL and the Safety Assessment Form. Information regarding SAs was acquired via the interviewer-administered DRS and Safety Assessment Form, which outlines lifetime aggression and suicidality that may not have occurred in the context of a depressive episode. Interviewers also administered the Children's Global Assessment Scale (CGAS), which indicates participants' level of general functioning (Shaffer et al. 1983), and the Family History Screen (with parents and adolescents) to identify the psychiatric status of first- and second-degree relatives (Weissman et al. 2000). Participants completed the Life Problems Inventory (LPI; self-report only), Conflict Behavior Questionnaire (CBQ; parent-report only) and Children's Affective Lability Scale (CALS; self-report and parent-report) to identify family conflict and dimensional traits often associated with BP and SUD (Robin and Foster 1989; Gerson et al. 1996; Birmaher et al. 2000). After the interview was completed using the aforementioned measures, data were presented to a child psychiatrist (B.G.) for diagnostic confirmation.
Statistical analysis
Univariate analyses comprised two tailed Pearson χ2 analyses for categorical variables and two tailed t tests for continuous variables. The self-reports (CALS, CBQ, and LPI) were continuous variables; for the purposes of this study, they were dichotomized as high versus low on the basis of median split. Variables associated with lithium at p<0.20 from the univariate analyses were analyzed via logistic regression models conducted in each of four domains: Clinical characteristics and comorbid diagnoses, self-report measures, lifetime medications, and family history. Each domain was also controlled for age. Finally, in order to determine the strength of the relationships among these variables and lithium treatment, an omnibus logistic regression analysis was performed on the variables found significant at p<0.05 in each of the four domain analyses.
Results
Lifetime lithium exposure was reported for 20% (20/100) of the sample. Results from the univariate analyses are summarized in Table 1. Subjects with, versus without, lifetime lithium exposure reported significantly greater psychiatric hospitalization (χ2=12.75, df=1, p<0.001) and psychosis (χ2=13.17, df=1, p<0.001), and significantly less self-injurious behavior (SIB) (χ2=4.86, df=1, p=0.028) and family history of depression (χ2=4.72, df=1, p=0.030). A trend toward significance was observed for SI and family history of SA, with both being more prevalent among adolescents without lithium exposure. Participants with lithium exposure were significantly more likely to have been exposed to antimanic anticonvulsants (χ2=10.70, df=1, p=0.001) and SGAs (χ2=13.74, df=1, p<0.001). As compared with adolescents without lithium treatment, those with lithium exposure were older (t=−3.07, df=98, p=0.003), more likely to have BP-I (χ2=15.17, df=2, p<0.001), and less likely to have BP-II (χ2=9.95, df=2, p=0.007). Regarding self-reports, participants with lithium exposure reported significantly less impulsivity (χ2=6.72, df=1, p=0.010), fewer interpersonal problems (χ2=8.67, df=1, p=0.003), less emotional dysregulation (χ2=6.72, df=1, p=0.010), and less identity confusion (χ2=4.17, df=1, p=0.041). Lithium use was also significantly associated with lower mood lability (CALS) as reported by the parent (χ2=8.41, df=1, p=0.004), and less family conflict (CBQ) as reported by the parent (χ2=5.68, df=1, p=0.017).
Two-tailed Pearson χ2 analyses were performed for categorical variables, and two tailed t tests were conducted for continuous variables.
Dimensional variables are depicted as mean (standard deviation) and categorical variables are depicted as number (percent).
The timeframe for CALS, CBQ, and LPI is current; the timeframe for other clinical characteristics is lifetime.
Any anxiety comorbid diagnosis included agoraphobia, generalized anxiety disorder, obsessive compulsive disorder, posttraumatic stress disorder, separation anxiety, social phobia and/or anxiety not otherwise specified.
Antimanic anticonvulsants=valproic acid, divalproex, carbamazepine.
Second generation antipsychotics=risperidone, olanzipine, aripiprazole, ziprasidone,quetiapine.
SSRI antidepressants=sertraline, paroxetine, fluoxetine, fluvozamine, citalopram, escitalopram.
Non-SSRI antidepressants=bupropion, mirtazapine, venlafaxine, duloxetine.
Stimulants=methylphenidate, amphetamine mixed salts; dextroamphetamine.
BP-I, bipolar I; BP-II, bipolar II; BP-NOS, bipolar not otherwise specified; CALS, Children's Affective Lability Scale; CBQ, Conflict Behavior Questionnaire; LPI, Life Problems Inventory; ADHD, attention-deficit/hyperactivity disorder; SUD, substance use disorder; ODD, oppositional defiant disorder; CD, conduct disorder; SSRI, serotonin reuptake inhibitor.
Logistic regression analyses
The clinical characteristics and comorbidities associated with lithium treatment (p<0.20) in the univariate analyses were included in the regression analyses. These variables included BP-I, BP-II, and the lifetime variables of psychiatric hospitalization, SIB, SI, psychosis, and oppositional defiant disorder (ODD) in the clinical characteristics and comorbid diagnoses domain; total scores for CALS (adolescent), CALS (parent), CBQ (parent), LPI impulsivity, emotional dysregulation, identity confusion, and interpersonal problems in the self-reports domain; antimanic anticonvulsant, SGA, and lamotrigine treatment in the lifetime medications domain; and family histories of depression, anxiety, and SA in the family history domain. Age was included as a covariate in each of the four domain analyses.
From the clinical characteristics and comorbid diagnoses domain, lifetime psychiatric hospitalization and BP-II were significant. From the self-reports domain, parent-reported family conflict (CBQ) and interpersonal problems (LPI) were significant. From the lifetime medications domain, antimanic anticonvulsant and SGA use were significant. No variables in the family history domain were significant after controlling for age. The significant variables were analyzed in the simultaneous logistic regression, where lifetime lithium was included as the dependent variable. Logistic regression analyses indicated that lithium exposure was associated with greater lifetime SGA use (OR=9.12, 95% CI: 1.62-51.51, p=0.012), lower parent-reported family conflict (OR=0.13, 95% CI: 0.03-0.67, p=0.014), and lower adolescent-reported interpersonal problems (OR=0.11, 95% CI: 0.02-0.56, p=0.008). The other variables were no longer significantly associated with lithium exposure. Please refer to Figure 1 for a summary of the multivariable analytic approach and results.
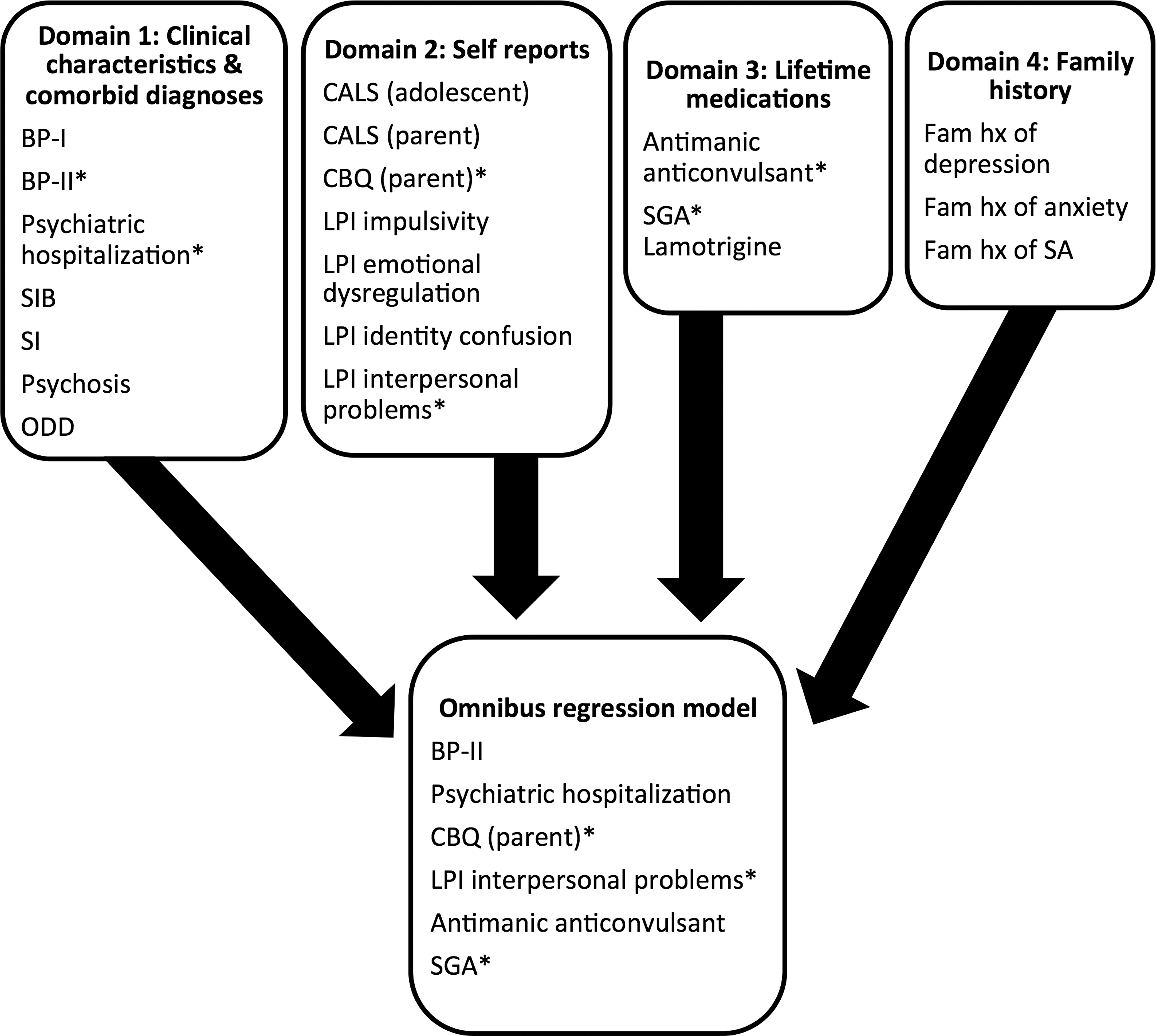
Logistic regression flow chart. BP, bipolar disorder; SIB, self-injurious behavior; SI, suicidal ideation; ODD, oppositional defiant disorder; CALS, Children's Affective Lability Scale; LPI, Life Problems Inventory; SGA, second-generation antipsychotics; SA, suicide attempts; CBQ, Conflict Behavior Questionnaire. *p<0.05.
Discussion
Twenty percent of participants reported lifetime lithium use. Participants with, versus without, lifetime lithium use were significantly older and significantly more likely to have BP-I, psychiatric hospitalization, and psychosis. Lithium-treated participants were more likely to report use of SGAs and antimanic anticonvulsants. In contrast, participants with lithium exposure were less likely to have BP-II, self-injurious behavior, suicidal ideation, or oppositional defiant disorder, and were less likely to have family histories of depression, anxiety, or suicide attempts. Participants with lithium exposure also reported less family conflict, mood lability, impulsivity, emotional dysregulation, and identity confusion, and fewer interpersonal problems. In multivariable analyses, lithium use was associated with greater lifetime SGA use, and lower parent-reported family conflict and adolescent-reported interpersonal problems.
Recent estimates from adults with BP suggest that rates of lithium use are in the range of 25–40% (Ghaemi et al. 2006; Kilbourne and Pincus 2006; Collins and McFarland 2008; Depp et al. 2008). In studies of youth with BP, rates of lithium use reported range widely, from 15% (Potter et al. 2009) to 51% (Bhangoo et al. 2003). This broad range could be explained by differences across study samples. For example, Bhangoo and colleagues' study is based on youth enrolled in research protocols in the intramural program of the National Institute of Mental Health, representing a highly selected sample. Furthermore, Geller and coworkers (2010) found a 32.2% rate of lithium use in a sample that enrolled only children and early adolescents with BP-I. This is consistent with our finding of a higher rate of lithium exposure in youth with BP-I (46.2%), versus a lower overall rate of lithium treatment in the current sample (20%).
Present findings suggest that use of lithium among adolescents with BP is associated with multiple proxies for greater illness severity, including BP-I subtype, psychosis, hospitalization, and polypharmacy. Although more research regarding the relationship between BP subtype and lithium is needed, a study by Ghaemi et al. (2006) revealed that more adults with BP-I, as compared with BP-II, were treated with lithium. Our finding that psychosis is significantly associated with lithium treatment is supported by previous research among both adolescents (Consoli et al. 2009) and adults (Ghaemi et al. 2006) with BP.
Findings related to suicidality warrant comment, given the role of lithium in preventing suicide and suicide attempts (Baldessarini and Tondo 2003; Goodwin et al. 2003; Dunner 2004; Collins and McFarland 2008). Findings from adults suggest that lithium use is more common among BP adults with SI (Goldberg et al. 2005) and perhaps more effective among those with a family history of suicide (Svestka and Nahumek 1975). In the present study, SIB was significantly less prevalent among adolescents with lifetime lithium exposure. Although SI was not significantly associated with lithium exposure, a trend in the opposite direction of our hypothesis was observed; prevalence of SI was lower for those with, versus those without, lifetime lithium. The retrospective methodology of the current study does not allow for examination of temporal patterns of these associations. Perhaps the lower rate of SIB and SI among lithium-treated participants was a direct effect of lithium treatment; however, one can also speculate that prescribers may have been reluctant to prescribe lithium to adolescents with suicidality because of its lethality in overdose. Nonetheless, taken together with the trend toward higher prevalence of family history of suicide attempts among adolescents without lithium exposure, these findings suggest the overall conclusion that lithium appears to be underutilized among BP adolescents at clinical and/or familial risk for suicide.
Our findings that lithium is correlated with age and psychiatric hospitalization are supported by previous research (Frangou et al. 2002; Depp et al. 2008; Masi et al. 2010). The lack of significant relationship between lithium and Caucasian race may be attributed to sample differences (e.g., adolescent vs. adult, Canadian vs. United States) between the present study and previous studies, suggesting higher rates of lithium use among Caucasian participants (Kilbourne and Pincus 2006; Depp et al. 2008).
There is evidence that lithium may work best in patients with a family history of lithium response (Duffy 2007; Grof et al. 2009). The present study did not ascertain familial lithium responsiveness, such that further studies are needed in order to determine the role and use of lithium among adolescents with lithium-responsive relatives.
The present study found a trend toward lower SUD among those with, versus those without, lifetime lithium exposure. Preliminary findings suggest that lithium may reduce substance use and improve functioning among youth with BP and SUD (Geller et al. 1998). Similarly, recent preliminary findings from the COBY study found that greater naturalistic lithium exposure was predictive of lower incidence of first-onset SUD (Goldstein et al. 2013). Therefore, future studies are warranted to determine whether BP youth with, or at risk for, SUD comprise a subgroup in whom lithium may be especially beneficial.
Finally, more research is needed regarding the relationship between variables reported in the self-report measures and lithium exposure. Specifically, the associations of lithium with family conflict, mood regulation, impulsivity, identity confusion, interpersonal problems, and emotional dysregulation have not been well established in the literature. Our finding that the lack of lithium treatment is robustly related to family conflict is interesting, and warrants further research, as there is currently no literature on the association between family conflict and lithium exposure. However, there is some preliminary evidence that impulsivity and mood lability significantly decrease during lithium therapy, which may support the lower prevalence of impulsivity and mood lability we found among those with, versus without, lithium exposure (Hollander et al. 2005; Ohmura et al. 2012; Halcomb et al. 2013). Alternatively, this may reveal possible underutilization of lithium among patients in these subgroups. Future research examining the temporal relationship of lithium treatment to impulsivity and mood lability is needed to determine which explanation best reflects the relationship between lithium and those clinical characteristics.
Limitations
Several limitations of the present study warrant comment. First, although the sample size is relatively large, only 20 participants had lithium exposure, therefore limiting the power of between-group comparisons. The multivariable analyses in particular could have benefited from a larger sample size. Second, we examined lithium exposure dichotomously. Information regarding dosage, levels, adherence, and duration of treatment was not available, and would have been valuable. Third, medication exposure was determined via clinical interview with the adolescents and their parents, and confirmatory prescription records were not obtained. Fourth, the study was based at a single site. Although findings were based on intake assessment, and treatment decisions were naturalistically previously made by multiple clinicians, these findings nonetheless only reflect the prescribing practices for patients referred to a single site. These findings may or may not reflect prescribing practices for patients referred to other sites. Finally, the study employed a cross-sectional and retrospective methodology. As such, the direction of the observed associations is uncertain. Future studies employing larger samples, prospective methodology, and detailed information regarding lithium use are warranted.
Conclusions
This study suggests that relatively few (20%) adolescents with BP have been treated with lithium. Moreover, most adolescents with BP who have been treated with lithium have also been treated with other antimanic medications and/or been hospitalized. It appears that prescribers may be reserving lithium for severe cases and/or prescribing lithium as a later treatment strategy. Pharmacoepidemiologic data confirm that there has been a shift in prescription from lithium to SGAs in the United States (Patten et al. 2012). One factor that may contribute to this shift is the superior efficacy of SGAs (Correll et al. 2010; Liu et al. 2011; Geller et al. 2012) for mania among youth, albeit that this discrepancy appears to be in part setting dependent (Vitiello et al. 2012). Another factor may be the lack of need for serial monitoring of blood levels of SGAs. However, it is important to note that metabolic monitoring of SGAs is required, and that adherence with monitoring guidelines is poor, and worse than what is observed among adults (Haupt et al. 2009; Morrato et al. 2010). Similar to other medications, lithium is not a panacea, and may not be appealing to or appropriate for all adolescents with BP. However, past research suggests that certain subgroups may especially benefit from lithium, such as youth with family history of lithium response (Grof et al. 2009), youth with clinical and/or familial risk for suicide, and youth with or at risk for diabetes and dyslipidemia for whom the risk-benefit balance of SGAs may be suboptimal (DelBello et al. 2007). Youth with or at risk for SUD may also benefit particularly from lithium treatment (Geller et al. 1998; Goldstein et al. 2013). Taken together with the increasing knowledge base regarding pharmacokinetics and dosing of lithium among youth (Findling et al. 2008, 2010, 2011), these subgroups suggest opportunities for greater use of lithium among adolescents with BP. Lithium remains an important and relevant treatment option for adolescents with BP. Continued research regarding the characteristics of BP youth who are, and who are not, treated with lithium could potentially inform treatment planning and selection and generate traction toward personalized treatment approaches for these youth.
Clinical Significance
The present study has substantial clinical significance given the lack of published data on the clinical characteristics associated with lithium exposure in adolescents with BP. Our findings suggest possible underutilization of lithium treatment, an important field without a substantial body of research. Further developing this field could inform prescription of lithium in clinical settings, especially to certain subgroups for whom it may be particularly useful, such as adolescents with suicide risk, impulsivity, or mood lability.
Footnotes
Acknowledgments
The authors thank the participants of this study.
Disclosures
Dr. Goldstein has served as a consultant for Bristol Myers Squibb and has received honoraria from Purdue Pharma. The other authors have no financial, corporate, or commercial relationships to disclose that may pose a conflict of interest.