
Abstract
Objective:
The purpose of this study was to investigate the preliminary effectiveness and safety of lamotrigine for the treatment of depressive episodes in adolescents.
Methods:
This was a 12 week retrospective chart review of lamotrigine treatment among 37 adolescents (mean age 16.3±1.3 years) with depressive episodes (15 with bipolar disorder and 22 with major depressive disorder). Illness severity at the 4th, 8th, and 12th weeks were retrospectively scored using Clinical Global Impressions - Severity (CGI-S) and Clinical Global Impressions - Improvement (CGI-I).
Results:
The mean dose of lamotrigine was 65.4±37.5 mg/day (range 12.5–181.7 mg/day) for a mean duration of 199.9±217.4 days (range 14–879 days). The CGI-S scores were significantly decreased over 12 weeks (F=39.611, p<0.001, partial η2=0.531). Seventeen subjects (45.9%) showed a treatment response at 12 week follow up (defined by a CGI-I score ≤2). There were no differences in treatment effectiveness between the bipolar and unipolar groups. Overall, lamotrigine was well tolerated. The most common adverse event was skin rash (n=5, 13.5%), which resolved spontaneously after drug discontinuation.
Conclusion:
Our results provide preliminary evidence of the effectiveness and safety of lamotrigine in adolescents with bipolar and depressive disorders. Large, prospective, placebo-controlled studies are needed to confirm these findings.
Introduction
A
Lamotrigine is an anticonvulsant that has been approved by the United States FDA for the maintenance treatment of bipolar I disorder in adults. Recent meta-analysis has found that lamotrigine significantly improves depressive symptoms in adults with BD, particularly in more severely depressed subjects (Geddes et al. 2009). However, the studies that have examined the effectiveness of lamotrigine in unipolar depression in adult cohorts have produced inconsistent results.
In adolescent depression, the effectiveness and safety of lamotrigine has not been adequately studied. Two open label studies of lamotrigine have been conducted in youth with BD during depressive (Chang et al. 2006), and manic (Biederman et al. 2010) episodes, and have shown that lamotrigine may have benefits in younger BD patients. One retrospective chart review in adolescents with mood disorders has illustrated that lamotrigine may be effective, but may also be related to a significant risk of benign rash (Carandang et al. 2007). To our knowledge, however, no previous study has been performed in an Asian population. Therefore, we aimed in our present study to investigate the effectiveness and safety of lamotrigine in an adolescent cohort of unipolar and bipolar depression cases.
Methods
Subjects
This study was approved by the Institutional Review Board of Asan Medical Center. We retrospectively reviewed the medical records of 37 children and adolescents who were treated from March 2010 to February 2013 at the Department of Psychiatry of Asan Medical Center, Seoul, Korea. For inclusion in our analyses, all subjects had to meet the following criteria: 1) being between 6 and 18 years of age; 2) satisfying the diagnostic criteria for episodes of bipolar or depressive disorders in accordance with the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) (American Psychiatric Association 2000); and 3) having undergone lamotrigine treatment for >1 week.
Subjects were excluded by any of the following criteria: 1) an intelligence quotient (IQ) <80 on the Korean Educational Developmental Institute's Wechsler Intelligence Scale for Children (KEDI-WISC) (Park et al. 2002); 2) a past and/or current history of schizophrenia or other psychotic, organic mental, or pervasive developmental disorder; 3) the presence of seizure or other neurological disorders; 4) sensory impairments; 5) poor compliance with treatment; and 6) concomitant use of mood stabilizer or antipsychotics (doses >100 mg of chlorpromazine or equivalent [Andreasen et al. 2010]) for minimizing the their effects on mood symptoms and adverse events.
Diagnosis and clinical characteristics
Two independent psychiatrists (H.W.K. and S.H.S) retrospectively obtained the data for each subject. Diagnoses were assessed according to the DSM-IV-TR (American Psychiatric Association 2000) criteria. Bipolar disorder not otherwise specified (BDNOS) was defined using the criteria from the Course and Outcome of Bipolar Youth (COBY) study (Birmaher et al. 2009) (κ=0.75). We classified our subjects into two subgroups: 1) Major depressive disorder (MDD) group; 2) BD group. We obtained information on sex, age at which lamotrigine treatment was begun, IQ, and socioeconomic status (high, middle, and low). Comorbid psychiatric disorders were determined using the DSM-IV-TR (American Psychiatric Association 2000) (κ=0.63–0.77).
Effectiveness and safety of lamotrigine
To assess the effectiveness of lamotrigine during depressive episodes, the Clinical Global Impressions - Severity (CGI-S) and Clinical Global Impressions - Improvement (CGI-I) scores (Spearing et al. 1997) were retrospectively determined based on the patient medical records. CGI-S values were obtained at baseline, and CGI-S and CGI–I scores were obtained at the 4th, 8th, and 12th week (κ=0.89). Treatment response was defined as a CGI-I score of ≤2 by the 12th week of follow-up. Safety was assessed at each visit based on spontaneous reports from the patients or from their parents/guardians.
Statistical analyses
Statistical analyses were performed using PASW (version 18.0, SPSS Inc., Chicago, IL), and all comparisons were two tailed. A significance level of 0.05 was used. Demographic characteristics and psychiatric comorbidities were compared using the χ2/Fisher's exact tests (categorical variables), Student t test (dimensional variables), and Kruskal–Wallis test (ordinal variables). The repeated measures analysis of variance (ANOVA) was used to analyze the time (4th, 8th, and 12th week) and group (bipolar vs. unipolar depression) effects, and the time by group interaction. The last observation carried forward (LOCF) imputation was used for patients who did not complete the treatment period.
Results
A cohort of 37 adolescent subjects was enrolled and analyzed in this study with a mean age of 16.3±1.3 years (range: 13.1–18.4), and a predominance of females (n=27, 73%). Four subjects were diagnosed with BD I and II, 11 with BDNOS, and 22 with MDD. The mean dose of lamotrigine administered in this series was 65.4±37.5mg/day (range, 12.5–181.7 mg/day) for a mean duration of 199.9±217.4 days (range, 14–879 days). Twenty-five (67.6%) subjects had psychiatric comorbidities. The most frequent comorbid diagnoses were oppositional defiant or conduct disorders (n=11, 29.7%), followed by attention-deficit/hyperactivity disorder (n=5, 13.5%), and dysthymic disorder (n=5, 13.5%). There were no differences found in the demographic characteristics and psychiatric comorbidities of the bipolar and unipolar groups.
Figure 1 shows the mean scores and standard errors obtained from a repeated measures ANOVA of the CGI-S scores at baseline and at each follow-up point. The CGI-S scores were significantly decreased during the 12 week trial (F=39.611, p<0.001, partial η2=0.531), but the main effect of group (F=1.232, p=0.275, partial η2=0.034) and the trial by group interaction effects (F=0.071, p=0.911, partial η2=0.002) were not statistically significant. Seventeen subjects (45.9%) showed a treatment response at the 12th week follow-up. There was no significant difference found between the subjects with BD and those with MDD in relation to the proportion of responders.
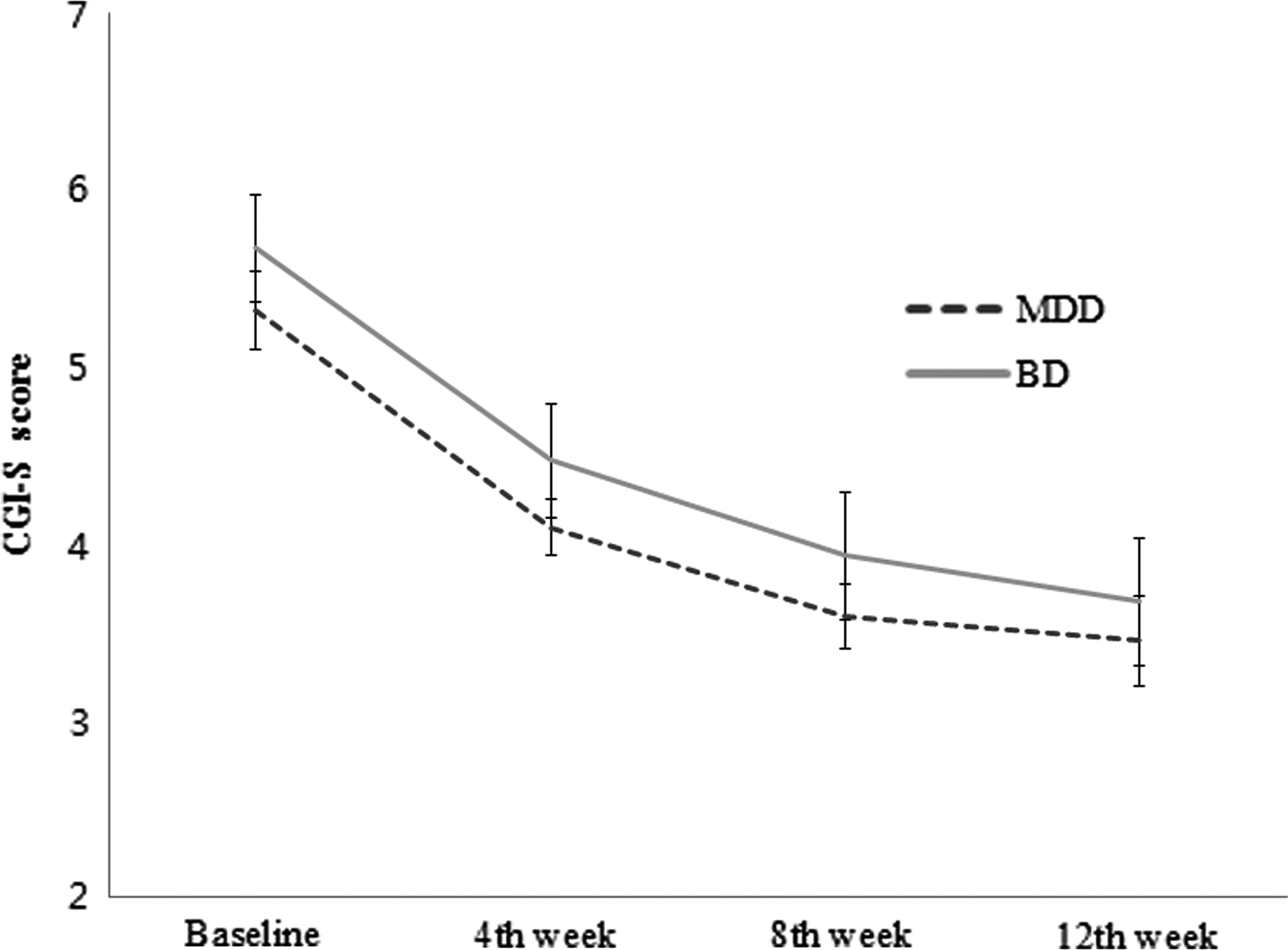
Mean and confidence intervals of the Clinical Global Impressions - Severity (CGI-S) scores. BD, bipolar disorder; MDD, major depressive disorder.
Nine (24.3%) subjects reported adverse events, most commonly skin rash (n=5, 13.5%). In the five skin rash cases, the rashes were mild to moderate in severity and resolved after a discontinuation of lamotrigine. No serious rash, such as Stevens–Johnson syndrome or toxic epidermal necrosis, was reported. The second most common adverse event was sedation (n=2, 5.4%). One subject (2.7%) showed irritability and aggressive behavior without any psychotic features. Five subjects (13.5%) discontinued the lamotrigine treatment because of adverse events; three because of rashes, one because of irritability, and one because of sedation.
Discussion
In this retrospective chart review, lamotrigine was found to be effective and generally tolerable in adolescents with depressive episodes. To the best of our knowledge, this is the only study to evaluate the effectiveness of lamotrigine in an Asian cohort of adolescents with depressive symptoms. Improvement was evident in 45.9% of our subjects, consistent with previous open label studies of lamotrigine, which reported 46–84% response rates for adolescent bipolar depression (Chang et al. 2006; Biederman et al. 2010). There was no significant difference in effectiveness among our groups, suggesting that lamotrigine is beneficial for BD and MDD.
We showed from our current analyses that 13.5 % of the adolescent subjects developed a benign rash, which remitted spontaneously after the discontinuation of lamotrigine. This is consistent with previous reports. Rash is a known common side effect of lamotrigine. In a previous retrospective analysis of adults with unipolar depression or BD from a 12 center series, the rates of benign rash were 6.4–13.1% (Calabrese et al. 2002). In another retrospective study of psychiatric and non-psychiatric adolescents in Korea, 21.6% of these subjects developed benign rash (Tak et al. 2012). Children have been reported to have a higher risk (threefold) of serious rash (Seo et al. 2011). Previous reports have suggested, however, that the risk of rash is decreased by initiating lamotrigine at a low dose, and titrating out this dosage slowly over several weeks (Carandang et al. 2007), as was seen in our study subjects.
One of our subjects (2.7%) showed irritability and aggressive behaviors. The effect of lamotrigine on mood change has not been established yet. In an earlier summary of 12 placebo-controlled trials for BD, serious adverse events such as mania, hypomania, and mixed mania occurred in 2.5% of 1,256 patients on a lamotrigine regimen (Seo et al. 2011).
Limitations
Our current study findings should be interpreted in the context of some notable limitations. First, we conducted a retrospective chart review and, therefore, could not control for the effect of concomitant medications or psychiatric comorbidities. Second, we did not have a control group. Third, diagnoses of mood disorder and comorbid psychiatric disorders were not based on structured interviews. Fourth, adverse events were likely to have been underestimated, because they were based on self-reporting. Our sample size was also relatively small, and this limited our ability to properly generalize our findings.
Conclusions
Our result provides preliminary evidence of the effectiveness and safety of lamotrigine in adolescents with bipolar and depressive disorders. Large, prospective, placebo-controlled studies are needed to support these findings.
Disclosures
No competing financial interests exist.