
Abstract
Objective:
The purpose of this study was to examine the impact of prior authorization policies on the receipt of antipsychotic medication for Medicaid-enrolled children.
Methods:
Using de-identified administrative Medicaid data from two large, neighboring, mid-Atlantic states from November 2007 through June 2011, we identified subjects <18 years of age using antipsychotics, from the broader group of children and adolescents receiving behavioral health services or any psychotropic medication. Prior authorization for antipsychotics was required for children in State A <6 years of age from September 2008, and for children <13 years of age from August 2009. No such prior authorizations existed in State B during that period. Filled prescriptions were identified in the data using national drug codes. Using a triple-difference strategy (using differences among the states, time periods, and differences in antidepressant prescribing rates among states over the same time periods), we examined the effect of the prior authorization policy on the rate at which antipsychotic prescriptions were filled for Medicaid-enrolled children and adolescents.
Results:
The impact of prior authorization policies on antipsychotic medication use varied by age: Among 6–12 year old children, the impact of the prior authorization policy on antipsychotic medication prescribing was a modest but statistically significant decrease of 0.47% after adjusting for other factors; there was no effect of the prior authorization among children 0–5 years.
Conclusions:
Prior authorization policies had a modest but statistically significant effect on antipsychotic use in 6–12 year old children, but had no impact in younger children. Future research is needed to understand the utilization and clinical effects of prior authorization and other policies and interventions designed to influence antipsychotic use in children.
Introduction
S
Policy makers' concern about the increased use of antipsychotics in children, particularly among children with disorders for which there is limited evidence of efficacy, is driven in part by strong evidence of the adverse effects of antipsychotic use, and by mounting evidence that children may be at even greater risk for adverse effects from these medications than adults (Correll and Carlson 2006; McIntyre and Jerrell 2008; Correll et al. 2009; Crystal et al. 2009), including weight gain (Correll and Carlson 2006) and diabetes (Hammerman et al. 2008). States' concerns about the increased use of antipsychotics and the associated costs (Farley et al. 2008; Jerrell et al. 2012), coupled with the increased risk of adverse effects in individuals for whom there is limited support for the effectiveness of these medications, has led states to begin implementing a range of policies designed to influence the use of antipsychotics (Texas Health and Human Services Commission 2010; Vogt et al. 2011). The most common approach, prior authorization—requiring physicians and patients to obtain approval before using a medication—has now been adopted by more than a third of state Medicaid programs (Soumerai et al. 2008).
The impact of prior authorization policies on adult prescribing has been mixed. A number of studies have raised concerns about prior authorization policies in Medicaid populations, such as the greater treatment discontinuities observed among adults subject to a prior authorization policy for antipsychotic medications (Soumerai et al. 2008). Other studies, however, have not found any such negative effects of prior authorization policies reducing the use of antipsychotics (Cunningham 2005; Soumerai et al. 2008; Adams et al. 2009; Abouzaid et al. 2010; Simeone et al. 2010; Walthour et al. 2010; Vogt et al. 2011). With respect to children, little is known about the impact of prior authorization policies on antipsychotic medication use, despite increasing state attention to Medicaid-enrolled child use of antipsychotic medications, highlighted by the establishment of a Medicaid Medical Directors' Learning Network to address use of antipsychotics among children (Foti, 2010), and two subsequent, multi-state, quality collaboratives developed to support states' efforts to improve psychotropic prescribing practices.
In this article, we begin to address this gap in empirical evidence by examining whether there is an impact of prior authorization policies on physician prescribing of antipsychotic medications for Medicaid-enrolled children, and if so, the magnitude of the impact, using Medicaid data from two large, neighboring, mid-Atlantic states. Children in State A were subject to a prior authorization policy implemented in September 2008, requiring physicians prescribing any antipsychotic medication for a child <6 years of age to obtain a prior authorization to prescribe the medication. Approximately a year later in August 2009, a second prior authorization policy was implemented in State A requiring physicians prescribing any antipsychotic medication for children <13 years of age to receive a prior authorization before prescribing an antipsychotic. Both pre-authorization policies presented a relatively modest burden, requiring physicians only to submit a form indicating their specialty, providing information about the child's diagnosis/diagnoses, symptoms, and history of medication trials, and indicating why prior medication trials were ineffective, with an opportunity to appeal if the authorization was denied. No such prior authorization policies were implemented in State B. We hypothesized that use of antipsychotics among children would decrease in State A following the implementation of the prior authorization policies, compared with use in State B.
Methods
Population and variables
Using de-identified Medicaid claims data for Medicaid-enrolled children <18 years of age, in two large, neighboring, mid-Atlantic states, we identified a cohort of children who had received any behavioral health services or treatment between November 2007 and June 2011 (defined as having received specialty outpatient behavioral health services or filled a prescription for a psychotropic medication). For each month during the study period, we then used National Drug Classification (NDC) codes to identify 22,409 children from State A and 61,566 children from State B who had received an antipsychotic medication between November 2007 and June 2011. Using the same method, we identified 24,378 children from State A and 66,979 from State B who had received an antidepressant medication during the same period. Children were categorized as having received the respective medication in a given month if they had received a prescription or had any days' supply remaining from a previously filled prescription for any days in that month. Children were grouped into age cohorts corresponding to the age groups (0–5 years old and 6–12 years old) affected by the prior authorization policies, and an age group (13–17 years old) unaffected by prior authorization policies. We defined our main outcome measure, the antipsychotic prescription rate (APR), as the fraction of children in the cohort who received an antipsychotic in each month. The study was approved by the University of Pittsburgh's Institutional Review Board (IRB), the New York State Office of Mental Health's IRB, and the New York State Psychiatric Institute's IRB.
Analyses
We first conducted descriptive analyses, calculating the APR and the antidepressant prescription rate (ADR) for each age cohort for each month from November 2007 through June 2011, the mean difference between those rates within a state for each month, and the difference between those means across the states, and describing prescribing trends in both states over time.
Using both the prior authorization for children 0–5 years of age that went into effect in September 2008, and the prior authorization affecting children 6–12 years of age that went into effect in August 2009, we used a difference-in-difference-in-difference approach (i.e., a “triple difference” strategy; an extension of a traditional difference-in-difference analysis) to examine the impact of prior authorization policies on APRs among Medicaid children. A traditional difference-in-difference approach would compare the change in the monthly APR in State A (from the period before the passage of prior authorization policy for that age cohort to the period after the passage of the prior authorization policy for that age cohort), to the change in the monthly APR in state B (where no prior authorization law was in place during that period) over the same time periods. Such an approach would allow us to control for pre-implementation differences in APR between State A and B, and also allow us to control for time trends that might otherwise be confounded with the prior authorization policy. However, it would not control for changes in State A that could be affecting the use of all psychotropic medications, such as a lower Medicaid reimbursement rate for medication checks or increased community concerns about the use of psychotropic medications in children. We therefore used the APR for the same populations and over the same time periods to conduct a triple difference analysis. As antidepressants are not directly targeted by the antipsychotic prior authorization policies, this approach allowed us to control for time-varying, state-specific factors that might affect psychotropic prescribing, which are unrelated to the antipsychotic medication prior authorization policies. We conducted separate regressions for each age cohort (0–5-year-olds, and 6–12-year-olds) aggregating data and clustering standard errors at the state-month level, using month-fixed effects, and weighting the data by the sample size in each state-month cell. As a further attempt to ensure that we were assessing the effects of the prior authorization policies, we also re-ran our analyses for 13–17-year-olds, who would be unaffected by either of the prior authorization policies.
Results
Patterns of antipsychotic and antidepressant medication use prior to the prior authorization policy
Prior to the August 2009 prior authorization policy start in State A, the average monthly rate of antipsychotic use among 6–12-year-old children receiving behavioral health services or treatment was 9.8% (Table 1). In State B, for the same time period and population, the average monthly rate of antipsychotic use was 5.9%. The average monthly rate of antidepressant use among the same cohort over the same time period (4.4% and 1.8% in States A and B, respectively) was lower than the average monthly rate of antipsychotic use in both states (Table 1).
p<0.01
Reference timing is introduction of prior authorization for 6–12-year-old children. When timing of introduction for 0–5-year-old children is used as the reference, the triple difference estimate is −0.203 m.
Similarly, among 0–5-year-old children, before the start of the prior authorization policy in State A in September 2008, the average monthly rate of antipsychotic use was ∼1.7%, (Table 1), whereas for the same time period and population in State B, the average monthly rate of antipsychotic use was ∼0.66%. The average monthly rate of antidepressant use among the same cohort over the same time period was lower than the average monthly rate of antipsychotic use in both State A (0.38%) and State B (0.09%) (Table 1).
Impact of prior authorizations on antipsychotic use
After the August 2009 start of the prior authorization policy affecting 6–12-year- old children in State A, the average monthly rate of antipsychotic use decreased from 9.8% to 9.5%, a decrease of 0.30% (Table 1). In State B, for the same time period and population, there was a very slight decrease in antipsychotic medication use of 0.08%, leaving the average monthly rate of antipsychotic use essentially unchanged at 5.9%.
Among 0–5-year-old children, after the implementation of prior authorization policy in September 2008 in State A, the average monthly rate of antipsychotic use was ∼2.1% (Table 1), an increase of 0.32% from before the implementation of the policy. In State B, for the same time period and population, the average monthly rate of antipsychotic use decreased by 0.009%, to 0.65% from the 0.66% rate prior to the policy (Table 1).
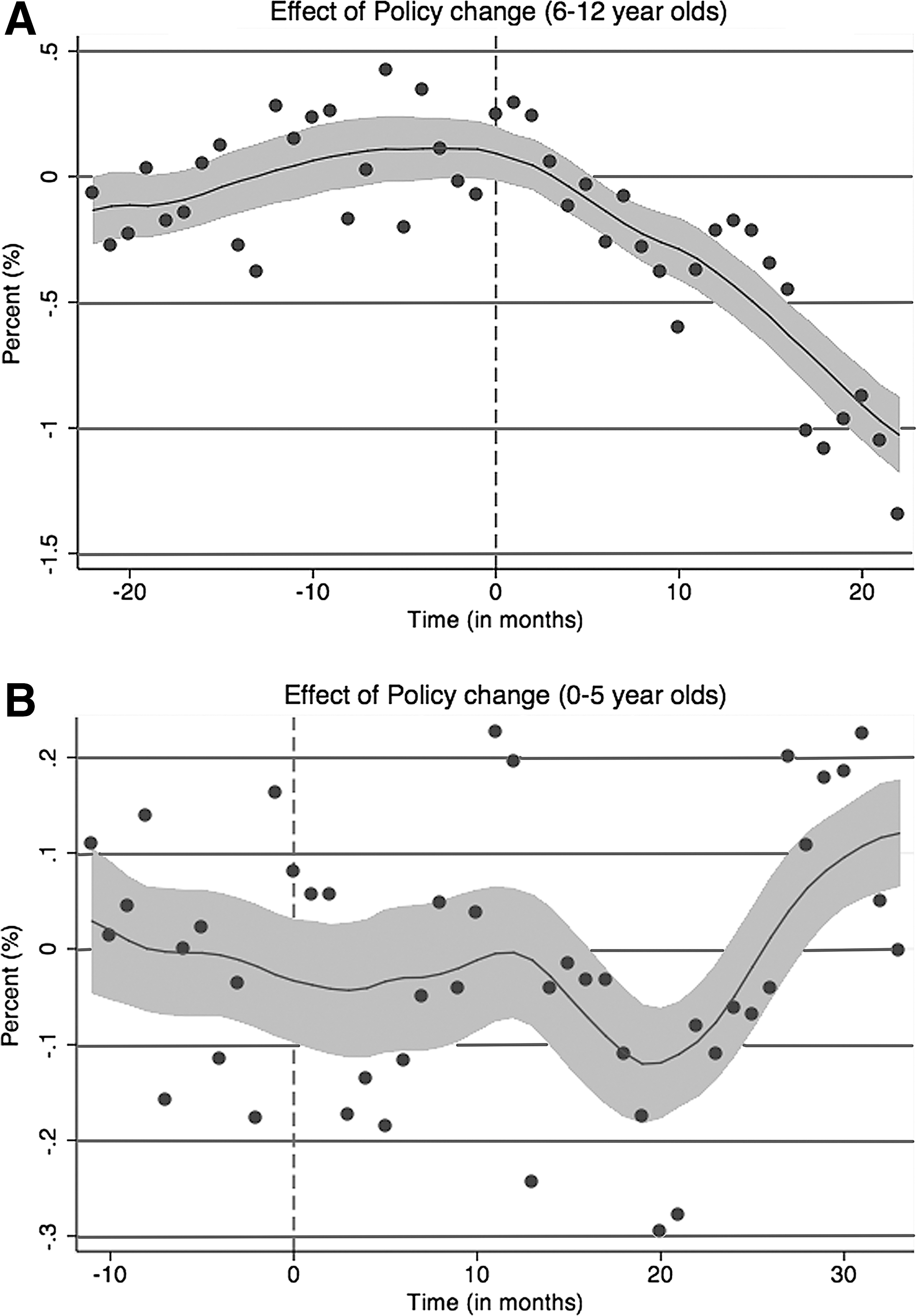
Figures 1A and B illustrate the impact of the prior authorization policies on 6–12- and 0–5-year-olds, respectively, by plotting the difference between the rate of use of antipsychotics and antidepressants in State A minus the same difference in State B for each month, using the mean difference between State A and State B in the pre-authorization period for the respective cohorts as the baseline. The vertical line indicates when the prior authorization was introduced in State A. As the smoothed regression line illustrates, there was a substantial decrease in the use of antipsychotic medications among 6–12-year-olds in State A following the prior authorization policy, but not a comparable change in 0–5-year-olds. When we conduct the triple difference analysis to examine the impact of the prior authorization policies on antipsychotic use, controlling for non-time varying state factors and state-specific trends in psychotropic use, we find that among 6–12-year-olds the prior authorization policy resulted in a 0.4% decrease from the baseline rate in the use of antipsychotic medications (p<0.01; Table 1) in the months after the prior authorization. In contrast, a comparable analysis reveals that the prior authorization policy had a negligible effect (0.02% decrease, ns) on the number of 0–5-year-old children in State A using antipsychotics (Table 1). As expected (given no change in prior authorization policies for this age group), comparable analysis of antipsychotic use among 13–17-year-old children found no significant change in the use of antipsychotic medications among children in State A after either of the prior authorizations was implemented, compared with the rate of use of antipsychotic medications in periods before the prior authorizations.
Discussion
We found that new prior authorization policies for antipsychotic medication resulted in a modest but statistically significant decrease in their use among 6–12-year-olds, but did not have a significant effect on antipsychotic use among 0–5-year-olds. Despite the increasing interest among state Medicaid programs in interventions to influence the use of antipsychotic medication in children (Naylor et al. 2007; Hilt et al. 2009; Foti et al. 2010; Hilt 2012), we are unaware of empirical studies that have examined this issue. The findings from this analysis contribute to filling this important gap in knowledge regarding the impact of prior authorization policies on influencing the use of antipsychotic medication in children.
The magnitude of the effect of the prior authorization policy we found on the use of antipsychotic medications by 6–12-year-olds, although statistically significant, was modest, with an unadjusted decrease in the rate of antipsychotic medication use of only 0.30%. Among 0–5-year-olds there was no significant impact of the antipsychotic prior authorization policy, with the rate of antipsychotic medication use increasing after the prior authorization policy by 0.32%, only slightly less than the 0.36% increase in the use of antidepressants in 0–5-year-olds in the state in the same time frame. Although no comparable data from studies of Medicaid-enrolled children are available, effects of comparable magnitude have been observed in similar studies of adults (Simeone et al. 2010; Vogt et al. 2011). Several factors could contribute to this modest policy effect. First, as others have suggested (Law et al. 2008), prior authorization policies may have a lesser effects on antipsychotic prescribing because, compared with many other medications, children may be more likely to be using antipsychotic medications on an ongoing basis, and the impact of prior authorization policies may be greater when an individual is starting a new medication than when a prescription for a medication refill is being written. It may also be that clinicians (and/or families) may be more willing to seek prior authorization for antipsychotic medications for children because of a perceived lack of available treatment alternatives; this hypothesis is consistent with research showing challenges to families in accessing specialty child mental health treatment (Horwitz et al. 2007; Cunningham 2009) in the context of a limited child mental health specialty workforce (Manderscheid and Henderson 2002; Kim 2003; Thomas and Holzer 2006). We note, however, that in some situations, prior authorization policies have been associated with changes in the use of antipsychotic medications in youth. For example, a prior authorization policy in Illinois decreased the concurrent use of two or more antipsychotic medications among youth <18 years of age in the child welfare system (Naylor 2013), whereas a program in Washington involving elective and mandatory prior authorization telephone consultations with a child psychiatrist decreased antipsychotic use among Medicaid-enrolled children (Hilt et al. 2012). Similar to the substantial variation in state approaches to prior authorizations for the use of antidepressants in Medicaid-enrolled youth (Fischer et al. 2007), there is likely substantial variation across states in the processes and goals of antipsychotic prior authorization policies. As a result, it will be useful for future studies of prior authorization policies to examine such policies at a more granular level with respect to the level of burden, the specific target of the policy, and the context (including other concurrent interventions) in which the policy is being implemented. It will also be useful to examine how such prior authorization policies interact with patient, prescriber, practice, and payer factors.
It is also unclear why the effect of a prior authorization policy we did observe existed among 6–12-year-olds but not among children <6 years of age. Among children 6–12 years old, antipsychotics are commonly used to treat off-label disorders such as attention-deficit/hyperactivity disorder (ADHD), other disruptive behavioral disorders, and depressive disorders (Wolraich 2003; Cooper et al. 2006; Olfson et al. 2006; Patel et al. 2006; Thomas et al. 2006; Aparasu and Bhatara 2007; Findling 2008; Crystal et al. 2009; Olfson et al. 2010; Pathak et al. 2010; Constantine et al. 2011). Younger children, who are less likely to receive these diagnoses, are more likely to be prescribed antipsychotics for autism spectrum disorders and other complex clinical situations. One possibility, therefore, is that prior authorization policies may be more likely to influence prescribing practices for 6–12-year-olds because the disorders for which they are commonly prescribed in this age group, such as ADHD and other disruptive behavior disorders, often have more alternative, evidence-based psychosocial and pharmacological treatment options, which were not subject to prior authorization. In contrast, disorders such as autism spectrum disorder have relatively fewer alternative evidence-based treatments that can substitute for antipsychotics. Unfortunately, the absence of information about children's diagnoses in our data prevents us from examining this issue directly. Further research is needed to better understand the impact of prior authorization policies on the prescribing of antipsychotic medications for populations of children with different diagnoses.
Similar to our findings, other studies have also found substantial variation across states in the use of psychotropic medications (Raghavan et al. 2010; Leslie et al. 2011; Merikangas et al. 2012), including variations in rates of use of antipsychotic medications (Foti et al. 2010; Merikangas et al. 2012), and have shown that a range of factors are likely to influence the rates of use of psychotropic medications, beyond the clinical characteristics of the patients. Such factors may include Medicaid eligibility requirements, shortages of child mental health specialty providers (Koplewicz 2010; Caccavale 2012; Musgrove 2012), differences in services available for vulnerable populations, pharmaceutical promotion (Berndt and Donohue 2008), or quality improvement efforts (Wisdom et al. unpublished data) such as phone consultation programs (Naylor et al. 2007; Hilt et al. 2009; Hilt 2012; Hilt et al. 2013). Further research is needed to better understand the impact of such factors on variations in the use of child antipsychotic medications across states and regions.
Limitations
As with all studies, our results must be considered within the context of its limitations. In our examination of the impact of the prior authorization policies on the use of antipsychotic medications in children, we attempted to control for other factors that may influence their use by using data from both a neighboring state and from the use of another psychotropic medication. This allowed us to control for any unobserved changes that might be influencing the prescribing of antipsychotic medications. Our triple difference strategy has strong internal validity and only requires that there be no unobserved factors that are correlated with the prior authorization policy change but not the prescribing of other psychotropic medications. Our approach also assumes that physicians are not substituting antidepressant medications for antipsychotic medications, an assumption that we believe is reasonable, as the two classes of medications are commonly used to treat different disorders. We note, however, that there was an increase in the use of antidepressants among 6–12-year-old children following the introduction of the prior authorization policy. It is possible that in cases in which physicians were uncertain whether an antipsychotic would offer particular clinical benefits compared with another psychotropic agent, they may have used an antidepressant instead of an antipsychotic medication after the prior authorization, although there was also an increase in antidepressant use among 6–12-year-olds in State B over the same time frame, which would not have been influenced by a prior authorization policy. Such a possibility reinforces the importance of examining not only the rate of use of medication after the introduction of a prior authorization policy, but also, to the extent possible, the appropriateness of observed shifts in prescribing patterns to other related agents. Unfortunately, we did not have access to diagnostic information, making us unable to determine to what extent utilization of antipsychotic medications varied by child clinical status. Similar to other studies of the impact of prior authorization policies in adults (Cunningham 2005; Soumerai et al. 2008; Adams et al. 2009; Abouzaid et al. 2010; Simeone et al. 2010; Walthour et al. 2010; Vogt et al. 2011), we do not have any way to determine the burden on physicians of the prior authorization policies. Physician burden would be important to measure in future studies, as it might explain the variability in prior authorization policy impacts observed in different studies and/or different states. Physician behavior would also be more likely to be influenced in situations in which the rates of authorizations not being approved was higher; unfortunately, we do not know how frequently sought authorizations were not being approved, nor if the rate of not being approved varied significantly for authorizations sought for 6–12-year-old children versus 0–5-year-old children. Finally, we were unable to compare rates of antipsychotic use in our population of Medicaid-enrolled children receiving any psychotropic medication or behavioral health services with studies of antipsychotic use in populations of all Medicaid-enrolled children reported by others.
Conclusions
Despite these limitations, this article contributes to our understanding of the impact of prior authorization policies on the use of antipsychotic medications among children. Our findings suggest that, even when effective, the prior authorization policy impact may be modest, and in some populations it may have little or no impact. Given the range of potential negative health effects of antipsychotics (Correll and Carlson 2006; Correll 2007; Hammerman et al. 2008; McIntyre and Jerrell 2008; Correll et al. 2009; Crystal et al. 2009), and that the cost of such medications now far exceeds that of any other drug class in Medicaid (Crystal et al. 2009), it is reasonable to anticipate that states will continue to make efforts to ensure that antipsychotic medications are appropriately used in children, and are not overused or misused. Our study highlights the limitations of prior authorization policies alone in influencing prescriber behavior, as well as the fact that such policies may not influence prescribing patterns equally for all groups of children. It also suggests the need for evaluations of more targeted and/or clinically nuanced and informed approaches, such as efforts to work with prescribers whose use of antipsychotics are outside the norm (Becker et al. 2013), or telephone consultation programs, second opinion programs, or consultation and feedback systems (Naylor et al. 2007; Hilt et al. 2009; Foti et al. 2010; Hilt 2012; Hilt et al. 2013). Given that the ultimate goal, however, is helping children and families, it is important that evaluations of such efforts move beyond examining the impact of such initiatives on the prescribing of antipsychotic medications, and examine the impact on the clinical and functional outcomes of the children receiving such medications and their families.
Clinical Significance
In recent years, there has been increasing attention and concern regarding the use of antipsychotic medication in children, especially given the increasing off-label use of such medications, their costs, and the increased risk of adverse effects in children. This study of the impact of prior authorization policies for use of antipsychotic medications in children suggests that even when significant, the impact of such policies may be quite modest, and suggests the need for more targeted and clinically nuanced and informed approaches to meaningfully influence the prescribing patterns of antipsychotics in children.
Footnotes
Acknowledgments
The authors thank Mike Naylor and Robert Hilt for information regarding state Medicaid prior authorization programs, and Gina Boyd of the RAND Corporation for research assistance and manuscript preparation.
Disclosures
Qingxian Chen has no disclosures to report. Ka Ho Brian Chor has no disclosures to report. Molly Finnerty is currently supported by the New York State Office of Mental Health. Dr. Finnerty currently receives research support from Agency for Healthcar Research and Quality (AHRQ). Dr. Finnerty also currently serves as principal investigator on a project in which her research staff is supported by a Sunovion contract, and in the past has served as the principal investigator on a project in which her research staff was supported by Bristol Myers Squibb Foundation. Emily Leckman-Westin has no disclosures to report. Edward Okeke has no disclosures to report. Deborah Scharf has no disclosures to report. Mark