
Abstract
Objective:
There is evidence that Korean red ginseng (KRG) can reduce the production of the adrenal corticosteroids, cortisol, and dehydroepiandrosterone (DHEA), and thus may be a viable treatment for attention-deficit/hyperactivity disorder (ADHD). The present randomized double-blind placebo-controlled clinical trial tested the effect of KRG on children with ADHD symptoms.
Methods:
Subjects 6–15 years, who satisfied the inclusion criteria and had ADHD symptoms, were randomized into a KRG group (n=33) or a control group (n=37). The KRG group received one pouch of KRG (1g KRG extract/pouch) twice a day, and the control group received one pouch of placebo twice a day. At the 8 week point, the primary outcomes were the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for inattention and hyperactivity scale scores, which were measured at baseline and 8 weeks after starting treatment. Secondary outcomes were quantitative electroencephalography theta/beta ratio (QEEG TBR) (measured at baseline and week 8) and salivary cortisol and DHEA levels (measured at baseline and at 4 and 8 weeks).
Results:
The baseline characteristics of the KRG and control groups were not statistically different. The mean ages of the KRG and control groups were 10.94±2.26 and 10.86±2.41, respectively. The KRG group had significantly decreased inattention/hyperactivity scores compared with the control group at week 8 (least squared means of the differences in inattention adjusted for baseline scores: −2.25 vs. −1.24, p=0.048; hyperactivity: −1.53 vs. −0.61, p=0.047). The KRG group had significantly decreased QEEG TBR compared with the control group (least squared means of the differences: −0.94 vs. −0.14, p=0.001). However, neither the KRG group nor the control group exhibited significant differences in salivary cortisol or DHEA levels at week 8 compared with the baseline levels. No serious adverse events were reported in either group.
Conclusions:
These results suggest that KRG extract may be an effective and safe alternative treatment for children with inattention and hyperactivity/impulsivity symptoms. Further studies to investigate the efficacy and safety of KRG are warranted.
Introduction
A
Red ginseng is a type of cultivated ginseng. It is one of the most popular herbal medicines worldwide, and has a positive effect on a variety of conditions including glucose metabolism, psychomotor function, and pulmonary disease (Lee and Son 2011). There are two major types of ginseng, namely, Panax ginseng (Korean ginseng) and Panax quinquefolus L. (American Ginseng). P. ginseng contains ginseng saponins called ginsenosides, polyacetylene, acidic polysaccharides, antioxidative aromatic compounds, and insulin-like acid peptides. It has more types of ginsenoside than Panax quinquefolium (38 vs. 19) (Lee and Son 2011). Red ginseng is harvested after 6 years, and then steamed and dried. The steaming process gelatinizes the ginseng starch, and thereby increases the saponin levels (Coon and Ernst 2002). Of the various components of red ginseng, ginsenoside has the most medical promise, as it has been shown to have immunomodulatory, anti-inflammatory, anticarcinogenic, and antistress properties. It has also been shown to act on the central nervous system (Christensen 2009). In particular, two studies have shown that red ginseng may regulate adrenal function by suppressing catecholamine secretion and cortisol production, and by regulating nicotinic acetylcholine receptors in the central nervous systems (Tachikawa and Kudo 2004; Hasegawa et al. 2013). Given that imbalances in adrenal corticosteroids such as cortisol and DHEA may contribute to the mood and attention disorders of adolescents with ADHD (McGee et al. 1992; Goodyer et al. 2000), it is possible that treatment with ginseng may ameliorate these disorders by modulating adrenal function. Supporting this is a trial with postmenopausal women with climacteric syndrome. Treatment with ginseng markedly improved their fatigue, insomnia, and depression, and this was associated with significant decreases in their cortisol/DHEA (C/D) ratios (Tode et al. 1999). However, studies on the effects of ginseng treatment on children or adolescents with chronic psychological disorders have not been performed.
Because ADHD is one of the most significant psychological disorders among children and adolescents, the present randomized, placebo-controlled, double-blind study was performed to determine whether treatment with ginseng can alter the attention levels and adrenal function of children with inattention and hyperactivity/impulsivity symptoms. To determine adrenal function, the levels of cortisol and DHEA in the saliva were measured. Salivary cortisol is a simple noninvasive marker of free-circulating cortisol levels, and has been used previously to measure the stress response system (Vining et al. 1983; Tornhage 2009). Several studies have shown that there is a good correlation between plasma and salivary levels of cortisol (Inder et al. 2012). In the present study, salivary cortisol levels <10 ng/mL were deemed to signify chronic stress (Cetinkaya et al. 2007) on the basis of the documented close relationship between hypocortisolism and chronic stress (Heim et al. 2000).
Methods
Study design and population
This single-center, double-blind, placebo-controlled, randomized clinical trial was performed in a tertiary care academic hospital in Daegu, Korea, to evaluate whether red ginseng treatment improved the attentiveness and adrenal function of children with chronic stress. The safety of red ginseng was also evaluated. The trial started in August 2011 and ended in February 2012. Of the 150 recruited children who were screened, 72 who met the inclusion criteria and consented to participate in the study were randomized. The study was approved by the institutional review board of Yeungnam University Medical Center and Ministry of Food and Drug Safety in Korea (protocol no. KGC-YNU-001). The legal representative of each subject provided written informed consent prior to any procedures. This study followed the Declaration of Helsinki, Good Clinical Practice, and applicable laws and regulations.
Eligibility criteria
Subjects were included if they were 6–15 years of age and had more than six symptoms of inattention or hyperactivity/impulsivity; these symptoms are the diagnostic criteria for ADHD described in the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) (American Psyhciatric Association 1994). Before the study started, the original inclusion criterion was that all subjects should have more than six inattention symptoms or more than six hyperactivity/impulsivity symptoms. However, as many of the patients also met an exclusion criterion (“taking drugs that could affect psychological symptoms”), this inclusion criterion was changed to include patients not only with ADHD but also with ADHD NOS (not otherwise specified). All enrolled patients had had symptoms for >6 months and had morning salivary cortisol levels <10 ng/mL, which is considered to indicate chronic stress (Cetinkaya et al. 2007). Subjects were excluded if they were taking drugs that could affect psychological symptoms, including antipsychotic drugs; common cold drugs such as amphetamine, ephedrine, and ginseng products; or vitamin supplements. Subjects were also excluded if they had adrenal or thyroid disease, or if they had received a psychological diagnosis within the preceding 3 months.
Procedures and data collection
During the 2 week screening period, the demographic data, past medical history, medication use, and vital signs of each subject were analyzed to determine whether they met the eligibility criteria of the study. Thereafter, they were randomly assigned in a double-blind manner to receive one pouch (40 mL) of Korean red ginseng (KRG) extract (1 g of KRG concentrated extract; Korea Ginseng Corporation, Seoul, Korea) twice a day or one pouch (40 mL) of an identically flavored and identically packaged placebo twice a day. All participants, care providers, and those assessing outcomes were blinded after assignment to interventions. The treatment duration was 8 weeks. At baseline (0 weeks) and 4 and 8 weeks after randomization and commencement of treatment, the subjects were asked to visit the clinic, where their vital signs were recorded. One day before the visit to the hospital, saliva samples for hormone assays were taken from the patients at home at four time points during the day. At baseline and the 8 week visit, the parent(s) and/or schoolteacher of each patient were asked to complete a questionnaire to assess the patient's symptoms of inattention or hyperactivity/impulsivity, and quantitative electroencephalography (QEEG) was performed. The subjects were asked to report any adverse events whenever they occurred during the entire study period.
Primary outcome
Inattention and hyperactivity/impulsiveness scale score
To assess the ADHD symptoms, patients answered 18 questions pertaining to the DSM-IV diagnostic criteria (American Psychiatric Association 1994). Nine questions examined inattention and nine questions examined hyperactivity/impulsivity. Each question with a positive answer resulted in a score of one point. The symptoms of inattention are “failure to provide close attention to detail, makes careless mistakes,” “has difficulty maintaining attention in play, school, or home activities,” “seems not to listen, even when addressed directly,” “fails to follow through,” “has difficulty organizing tasks, activities, and belongings,” “avoids tasks that require consistent mental effort,” “loses objects required for tasks or activities,” “is easily distracted by irrelevant stimuli,” and “is forgetful in routine activities.” The symptoms of hyperactivity and impulsivity are “shows excessive fidgetiness,” “has difficulty remaining seated when sitting is required,” “has feelings of restlessness or runs around or climbs inappropriately,” “has difficulty playing quietly,” “is difficult to keep up with, seeming to always be ‘on the go,’” “talks excessively,” “has difficulty waiting their turn,” “blurts out answers too quickly,” and “interrupts or intrudes on others.”
Secondary outcome
Salivary cortisol and DHEA levels
The saliva samples taken at baseline and weeks 4 and 8 were used to measure the cortisol and DHEA levels. At these time points, saliva samples were collected four times at home by using saliva collection tubes according to standardized sampling instructions (Michels et al. 2012): in the morning (8:30 a.m.±1 hour), the afternoon (12:00 noon±1 hour), the evening (6:00 p.m.±1 hour), and at night (10:00 p.m.±1 hour). Collected saliva was refrigerated at −20°C prior to analysis and taken to the hospital the next day. The molar cortisol/DHEA ratio was calculated by dividing the morning cortisol by the DHEA levels at each time point. The saliva sample tubes were centrifuged for 10 minutes, and the cortisol and DHEA concentrations in the supernatants were measured by using a commercially available, enzyme-linked immunosorbent assay (ELISA).
QEEG
Complete EEG data at baseline (week 0) and the week 8 visit were obtained in 41 subjects (KRG group, n=20; control group, n=21). The subjects were not allowed to take either KRG extract or a placebo the night before. QEEG was recorded by using a MITSAR EEG 201 system, PC-controlled 21-channel EEG system. The session lasted from 60 to 90 minutes. The input signals referenced to the linked ears were filtered between 0.5 and 50 Hz, and digitized at a sampling rate of 500 Hz. Impedance was kept <5 kOhm for all electrodes, which were placed according to the international 10–20 system by using an electrode cap with 19 electrodes (Electro-cap International Inc.). Two reference input connectors (A1 and A2) and two ground input connectors were used for successful EEG recording. Quantitative data were obtained by using WIN-EEG software. The band ranges for theta and beta were set in the eyes-opened (EO) condition at 4–8 Hz (theta) and 13–21 Hz (beta) registered at the vertex (Cz), in accordance with previous literature (Monastra et al. 1999). The theta-to-beta power ratio (TBR) was then calculated.
Safety assessment
At each study visit, the subjects were asked an open-ended question regarding adverse events. The investigator recorded all subject-reported adverse events as a case report form and judged each event in terms of its relationship to the trial medication. Adverse events were recorded from the first day of taking a dose of the KRG extract or placebo to 14 days after the last dose.
Statistical analysis
The data were analyzed by using intention-to-treat (ITT) and per-protocol (PP) analyses. For ITT analysis, all data from subjects who had at least one postrandomization assessment were included. For missing or incomplete data, the most recently available data were used (last observation carried forward analysis). For PP analysis, only those subjects with complete data for weeks 0 and 8 data were included. The groups were compared in terms of baseline characteristics by using Pearson's χ2 test or independent t test. Repeated measures ANOVA was used to compare the two groups in terms of changes in salivary hormone levels relative to baseline. Analysis of covariance (ANCOVA) was used to compare the two groups in terms of treatment efficacy on inattention/hyperactivity scale scores and QEEG relative to baseline values. Effect sizes were calculated according to Cohen's d. The values of 0.2, 0.5, and 0.8 are generally assumed to be small, medium, and large effects, respectively (Cohen 1988). To compare the two groups in terms of treatment safety, Fisher's exact test was used. All analyses were conducted by using the IBM SPSS statistics version 20 (SPSS INC., Chicago, IL). P values <0.05 were considered to be statistically significant.
Results
Baseline characteristics of the subjects
In total, 150 participants were recruited during the study period. Of these, 78 subjects were excluded because they did not consent to be in the study or did not meet the inclusion criteria. The remaining 72 patients were assigned randomly to the KRG and control groups at a 1:1 ratio. There were 35 patients in the KRG group and 37 in the control groups. In two KRG group children, saliva was not collected at any time point after randomization. Consequently, they were excluded. Therefore, the final ITT population consisted of 70 patients: 33 in the KRG group and 37 in the control group (Fig. 1). The two groups did not differ significantly in terms of any of the baseline characteristics (Table 1). The mean ages of the KRG and control groups were 10.94 and 10.86 years, respectively; males accounted for 63.6% and 62.2% of the two groups, respectively; their mean inattention scale scores were 6.39 and 5.70, respectively; and their mean hyperactivity scale scores were 3.09 and 3.81, respectively. Their mean baseline morning levels of salivary cortisol were 5.54 and 5.35 ng/mL, respectively. Significant differences between the groups in terms of afternoon, evening, and night levels of cortisol were also not observed. The mean salivary DHEA levels of the KRG and control groups were 3.06 and 2.97 pg/mL, respectively. In addition, their QEEG TBR scores were 3.79 and 3.74, respectively.
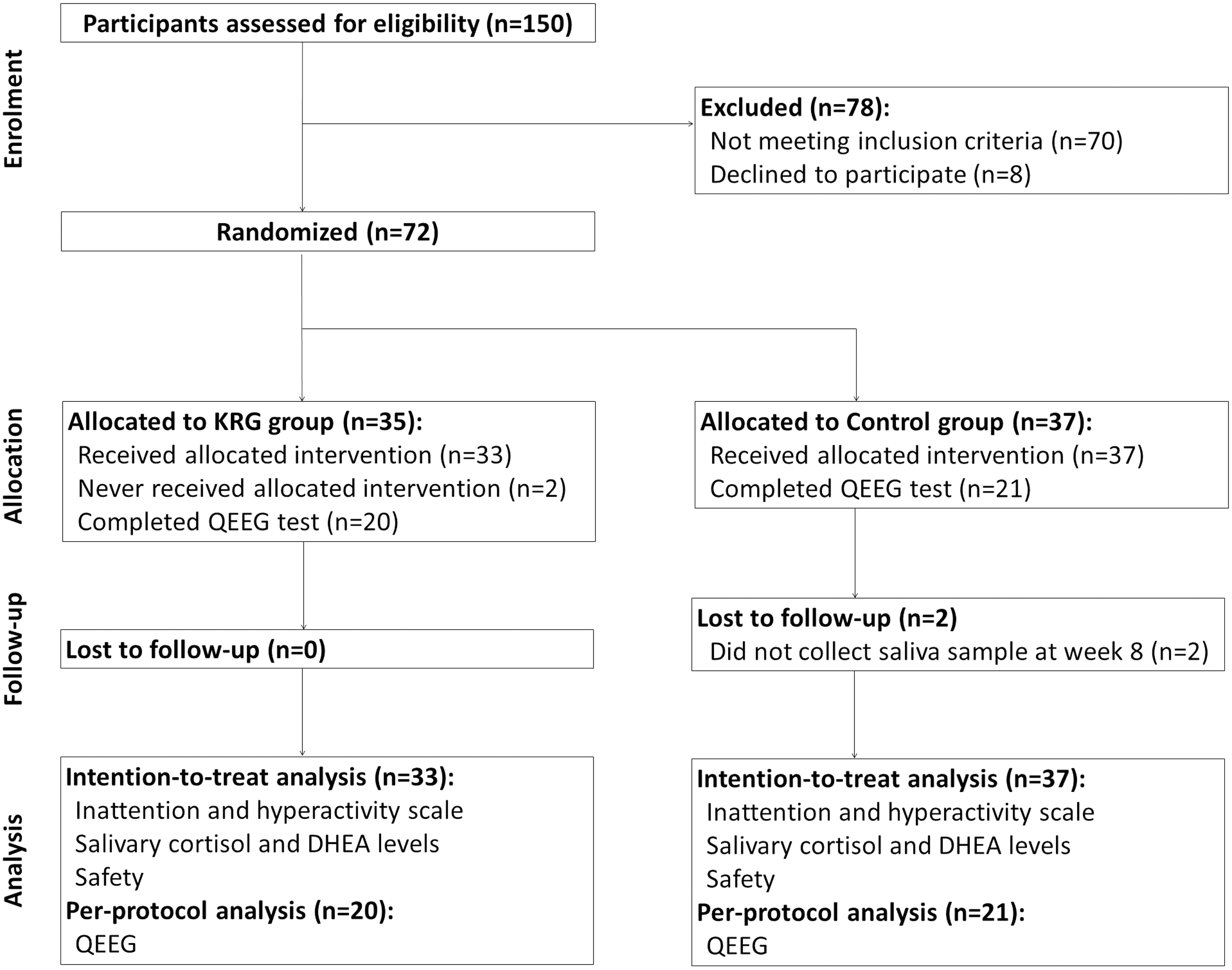
Flow of participants through the study.
The data are presented as mean±standard deviation or number (%).
Independent t test or Pearson's χ2 test.
Per-protocol population, n=20 vs. n=21, respectively.
DHEA, dehydroepiandrosterone; KRG, Korean red ginseng; QEEG TBR, quantitative electroencephalography theta/beta ratio.
Efficacy of ginseng treatment
Inattention and hyperactivity/impulsivity scale scores
The mean inattention scores of the KRG group decreased from 6.39 at baseline to 4.03 at week 8 (p<0.001). Similarly, the control group scores decreased from 5.70 to 4.57 (p=0.002). The difference of inattention scores at week 8 between the two groups was not statistically significant (p=0.391). However, for the KRG and control groups, the least squared means of the differences between baseline and week 8, after adjustment for baseline inattention scores by using the Bonferroni correction, were −2.25 and −1.24, respectively. Therefore, the KRG group exhibited a greater decrease in inattention scores after 8 weeks of treatment than did the control group. This difference was statistically significant with a medium effect size (p=0.048, Cohen's d=0.47). With regard to the mean hyperactivity scores at week 8 relative to baseline, these also decreased from 3.09 to 1.76 (p=0.002) in the KRG group, and from 3.81 to 3.03 (p=0.050) in the control group. The hyperactivity scores at week 8 between the two groups showed statistically significant difference (p=0.019). For the KRG and control groups, the least squared means of the differences between baseline and week 8, after adjustment for baseline hyperactivity scores by using the Bonferroni correction, were −1.53 and −0.61, respectively. Therefore, the KRG group exhibited a significantly greater decrease in hyperactivity scores than did the control group, with a medium effect size (p=0.047, Cohen's d=0.49) (Table 2).
The data are presented as mean±standard deviation.
Independent t test comparing the KRG and control groups in terms of their week 8 results.
Analysis of covariance (ANCOVA) adjusted for baseline inattention/hyperactivity scores.
Bonferroni correction, differences from week 8 to week 0; the data are presented as mean±standard error.
KRG, Korean red ginseng.
Salivary cortisol and DHEA levels
In both groups, the salivary cortisol levels in the morning, evening, and night generally increased steadily during the treatment period. However, the two groups did not differ significantly in terms of changes during treatment relative to baseline (interaction effect: p=0.911, 0.897, 0.214, and 0.448 for the morning, afternoon, evening, and night cortisol levels, respectively). Although the salivary DHEA levels decreased steadily in both groups from baseline to 8 weeks, the two groups did not differ significantly in terms of salivary DHEA levels relative to baseline (p=0.836). Therefore, although the C/D ratio increased dramatically in both groups, significant between-group differences were not observed (Table 3).
The data are presented as mean±standard deviation.
Repeated measures ANOVA.
DHEA, dehydroepiandrosterone; KRG, Korean red ginseng.
QEEG TBR
The QEEG TBR decreased from 3.79 to 2.85 (p=0.001) in the KRG group, and from 3.74 to 3.63 (p=0.126) in the control group, using PP analysis, respectively. A t test on the week 8 data revealed that the KRG had a significantly lower QEEG TBR than the control group (p=0.017). For the KRG and control groups, the least squared means of the differences between baseline and week 8, after adjustment for baseline QEEG TBR by using the Bonferroni correction, were −0.94 and −0.12, respectively. Therefore, the KRG group showed a significantly greater decrease in QEEG TBR with a large effect size (p= 0.001, Cohen's d=1.13) (Table 4).
The data are presented as mean±standard deviation.
Independent t test comparing the KRG and control groups in terms of their week 8 results.
ANCOVA adjusted for baseline QEEG TBR.
Bonferroni correction, differences from week 8 to week 0; the data are presented as mean±standard error.
ANCOVA, analysis of covariance; KRG, Korean red ginseng; QEEG TBR, quantitative electroencephalography theta/beta ratio.
Safety of the treatments
Adverse reactions were monitored during the entire course of the study. Of the 70 subjects, none reported adverse reactions that related directly to the intervention. One subject in the KRG group (3%) had loose stool, whereas two in the control group (5.4%) had gastrointestinal symptoms (nausea) that were unrelated to the placebo product. The two groups did not differ significantly in terms of frequency of adverse events (p=0.494). There were no serious adverse reactions (data not shown).
Discussion
Although medications to treat psychiatric disorders for children and adolescents have been widely researched and several are on the market, natural products may also be effective in these patients while inducing fewer significant adverse effects. The present randomized controlled trial was performed to assess whether KRG, a well-known traditional medicine plant that is used particularly frequently in Eastern Asia, can improve the adrenal function and inattention/hyperactivity symptoms of chronically stressed children with ADHD symptoms. KRG extract significantly improved the inattention and hyperactivity of the subjects and had a good safety profile. However, the KRG extract did not have significant effects on cortisol or DHEA levels.
Ginseng is a natural medicine and health supplement that is widely used worldwide by both healthy people and people with health conditions. Several randomized controlled trials have shown that ginseng has positive effects on psychomotor function in patients with Alzheimer's disease and in healthy populations (Kennedy et al. 2001; Scholey and Kennedy 2002; Heo et al. 2008; Lee et al. 2008). Animal studies have also shown that ginseng and its ginsenoside components have antineurodegeneration properties (Van Kampen et al. 2003), improve maze performance in scopolamine-treated rats (Yamaguchi et al. 1996), and improve spatial learning (Mook-Jung et al. 2001). These results led us to perform the present randomized controlled trial. The subjects were on average about 10 years old and had mild to moderate ADHD symptoms: At baseline, their mean inattention score was 6.03 and their mean hyperactivity score was 3.47. None had clinical histories of psychological interventions or ADHD medications. Compared with placebo, KRG treatment significantly improved the inattention scores and hyperactivity scores with medium effect sizes. Three other studies have also assessed the effect of ginseng treatment on children diagnosed with ADHD. One was a recent observational study performed in Korea that showed that KRG improved the inattentiveness of children with ADHD (Lee et al. 2011). Another was a small observational study in Italy, which showed that P. ginseng may slightly improve some symptoms of ADHD in children (Niederhofer 2009). The third was an open-label pilot study in Canada that showed that 4 weeks of treatment with a herbal extract combination containing P. quinquefolium and Ginkgo biloba may improve the symptoms of ADHD in children (Lyon et al. 2001). These reports are consistent with our results showing that ginseng significantly reduced the inattention and hyperactivity of chronically stressed children compared with placebo. Therefore, ginseng may be an effective alternative medicine for treating ADHD. It should be noted that our study is the first randomized controlled trial to assess the effect of ginseng on the ADHD symptoms of children; all previous studies (Lyon et al. 2001; Niederhofer 2009; Lee et al. 2011) were observational studies that lacked a control group. Their sample sizes were also very small (18, 3, and 36, respectively).
EEG is the oldest way to image human cortical brain activity, and is increasingly being used in psychiatric research applications. The TBR that is measured at the vertex (Cz) during the eyes-open or eyes-closed resting condition has been proposed to capture the relative contributions of two relevant frequency bands for diagnosing and monitoring ADHD (Monastra et al. 1999). In terms of resting EEG, elevated theta and reduced beta, together with TBRs, are reliably associated with ADHD (Barry et al. 2003). A recent meta-analysis reported that TBR increase is a common trait in ADHD, and that the effect size of 3.08 predicts a sensitivity and specificity of 94% (Snyder and Hall 2006). In our study, the mean QEEG TBR at baseline was >3.08, and it dropped <3.08 in the KRG group, whereas it remained >3.08 in the control group at 8 weeks. We also found that our KRG-treated children had significantly lower TBR scores at 8 weeks than the placebo-treated children, after adjusting for baseline levels, which suggested that KRG may improve cognitive performance and hyperactivity symptoms. The effect size for QEEG TBR between the KRG and placebo groups was 1.13, showing that KRG had a large effect. However, the result may not be sufficiently powered to detect differences in QEEG, on account of the small sample size. Because the QEEG takes between 60 and 90 minutes to complete, 13 and 16 KRG and control group children dropped out of the QEEG, respectively.
An in vitro study has suggested that KRG may improve psychomotor impairments, such as inattention and hyperactivity, by suppressing catecholamine secretion and cortisol production, thereby regulating adrenal function (Tachikawa and Kudo 2004). Because hypocortisolism is also closely related to chronic stress, especially psychiatric stress (Heim et al. 2000), we hypothesized that the reported cortisol-elevating effect of KRG might improve the psychomotor function of chronically stressed subjects. However, when we measured the salivary cortisol and DHEA levels of our patients and calculated their C/D ratios on the basis of morning salivary cortisol levels, we did not detect any significant differences between the KRG and control groups after 8 weeks of treatment. In fact, contrary to the results of the in vitro study on the adrenal function-regulating ability of KRG (Tachikawa and Kudo 2004), other studies have also shown that ginseng treatment does not significantly change serum cortisol or DHEA levels in adults (Tode et al. 1999; Youl Kang et al. 2002; Lee and Ji 2014).
Although these studies had relatively small sample sizes, had short treatment durations, and involved quite different subjects, they consistently found, like our study, that ginseng did not appear to have a significant effect on cortisol and DHEA levels. However, the relatively small study populations and the focus on specific conditions of these and our studies mean that it cannot yet be concluded that ginseng truly has no effect on adrenal function. Moreover, in our study, the baseline morning cortisol levels of the subjects were <10 ng/mL, and these levels never exceeded this threshold, even after 8 weeks of administration. Furthermore, salivary cortisol levels differ significantly among individuals, and sampling time and anthropometric characteristics can influence salivary cortisol and cortisol responses to interventions (Konishi et al. 2012) These may lead the changes of cortisol levels to statistically nonsignificant results. Additional clinical trials with larger sample sizes and longer treatment durations and follow-up periods are needed to determine whether ginseng treatment can affect adrenal function.
There are a few limitations in this study. First, there may have been some selection bias, as the subjects were all enrolled in a single center located in Daegu, Korea, and the study sample was relatively small (70 children). Therefore, we cannot generalize the conclusions to the larger population. The second limitation is that our study included not only ADHD patients (75.7%) but ADHD NOS patients (24.3%) who did not meet the full criteria for ADHD diagnosis. This reflects the fact that we had to change our inclusion criteria just before the study started; although we initially sought to enroll patients who had been diagnosed with ADHD (defined according to DSM-IV criteria as having six or more symptoms of hyperactivity or six or more symptoms of inattention), most of such patients were already taking medications (including methylphenidate and atomoxetine), which was an exclusion criterion. Therefore, the inclusion criteria had to be modified to “having more than six symptoms of inattention or hyperactivity for more than 6 months.” The third limitation is that the treatment duration was relatively short. This meant that the long-term effects of ginseng could not be evaluated. The fourth limitation is that the KRG dose was 2000 mg/day, which is two thirds of the recommended dose for adults (3000 mg/day). It remains possible that the pharmacodynamics of KRG may be influenced by weight, age, and sex. Nevertheless, despite these limitations, this study has several strengths. It is the first randomized controlled trial to show that KRG extract effectively reduces the ADHD symptoms of children with chronic stress and ADHD symptoms. It is also the first study to assess the effect of KRG treatment on salivary adrenal hormone levels in such children.
Conclusions
In conclusion, compared with placebo, KRG extract significantly improved the inattention, hyperactivity/impulsivity symptoms, and QEEG TBR, but not the salivary cortisol or DHEA levels, of chronically stressed children with ADHD symptoms. KRG extract also did not have any adverse events. These results suggest that KRG extract may be an effective and safe alternative treatment for children with inattention and hyperactivity/impulsivity symptoms. Large-scale studies that determine the long-term efficacy and safety of KRG treatment in childhood ADHD and its effects on adrenal hormone levels are warranted.
Clinical Significance
To our knowledge, this is the first randomized controlled trial to investigate the efficacy and safety of Korean red ginseng extract for children with ADHD. The stimulant medications for ADHD have demonstrated not only clinical efficacy, but also significant adverse events such as poor growth, tics, and psychosis. Although KRG extract did not affect the salivary cortisol or DHEA, it significantly improved ADHD symptoms and QEEG TBR. And the safety profile of KRG extract was good. The results imply that KRG extract is a possible effective alternative medication for ADHD children.
Disclosures
No competing financial interests exist.