
Abstract
Objective:
Little is known about the pattern of service receipt and outcomes from clinics implementing best practice guidelines in child mental health. This study aimed to determine these variables for a clinic that implemented an attention-deficit/hyperactivity disorder (ADHD) treatment guideline proposed by the Children's Medication Algorithm Project (CMAP).
Methods:
Secondary analyses of medical record extracts were conducted for children who received treatment from 2007 to 2012 in a specialty clinic linked to a public children's hospital in Canada. Patterns of medication selection and dosing were compared with CMAP guidelines. Outcomes were based on parent and teacher ratings on the ADHD portion of the Multimodal Treatment Study for ADHD (MTA)- Swanson, Nolan, and Pelham, Version IV (SNAP-IV).
Results:
Data were available for 132 children (ages 5–14), 81.8% of whom had no previous ADHD medication exposure, and 97.0% of whom had started at least one medication. Methylphenidate was used first for 59.8% of children, whereas 33.3% started with an amphetamine product. Of the 47.0% of children who progressed to a second medication trial, 88.7% tried a stimulant from a second class. In total, 19.7% tried atomoxetine, which was typically used as a third stage choice (i.e., after two different stimulant exposures). Stage four to six medications were rarely used, rather stimulants were retried after atomoxetine and/or medication combinations were tried. Symptomatic remission at the end of treatment was achieved by 70.4% and 82.4%, according to parents and teachers respectively, for those with outcome data and who completed treatment. Outcomes for those further along the treatment algorithm were similar to discharges at the beginning of the algorithm.
Conclusions:
The high rates of symptomatic remission observed within this clinical service may be a function of adherence to CMAP recommendations. However, the lack of a comparison group or experimental design prevents determination of causality. Additional investigations of the impacts of implementing evidence-based guidelines are critically needed, with proposed benchmarks to inform outcome evaluations.
Introduction
Gaps in attention-deficit/hyperactivity disorder (ADHD) Care
M
Best practice guidelines
The implementation of evidence-based practice guidelines provides one strategy that may improve the quality of care and treatment outcomes for children with ADHD. Ideally, practice guidelines should help guide clinical decision making, enable clinicians to deliver treatments that have been demonstrated to be effective, produce positive clinical outcomes, and improve consistency of care (Worrall et al. 1997; Woolf et al. 1999; Hoagwood et al. 2001). Unfortunately, there are few studies examining outcomes from guideline use in child mental health.
One exception in ADHD treatment is a feasibility study examining the implementation of the Texas Children's Medication Algorithm Project (CMAP) ADHD guideline (Pliszka et al. 2003). This study contrasted service patterns and outcomes for a sample of children treated at mental health centers post-guideline training and implementation, compared with a historical cohort treated at the same centers. In comparison with the historic cohort, guideline implementation was associated with fewer combination medications and non-protocol medication exposures, patterns consistent with CMAP (Pliszka et al. 2003). In addition, the guideline group had better scores on the Clinical Global Impressions Scales (Pliszka et al. 2003). Although this was a critical study, there were some limitations including 1) algorithm implementation oversight by CMAP developers, 2) a relatively small sample size for the intervention group (n=50), 3) service patterns examining a relatively short set treatment time period (i.e., 4 months) versus full duration of treatment, and 4) the lack of completeness of additional outcome measures (e.g., only 17 children had complete teacher ratings).
Outcome monitoring and remission
There is a growing interest in trying to attain remission when treating ADHD, rather than accepting any positive treatment response. This has been defined as a loss of diagnostic status, with minimal or no symptoms, and attainment of optimal functioning (Steele et al. 2006). Establishing and implementing remission criteria in clinical practice may provide clinicians with an outcome goal in the long-term management of disorders such as ADHD. Parent and teacher reports of ADHD symptom severity on validated rating scales are proposed as a critical component of determining whether a patient has at least achieved symptomatic remission.
One proposed instrument for the measurement of symptom severity and achievement of symptomatic remission is the Multimodal Treatment Study for ADHD (MTA)- Swanson, Nolan, and Pelham, Version IV (SNAP-IV) (Ramos-Quiroga and Casas 2011). Parent and teacher ratings on this instrument were used as core outcome measures in the MTA. At the 14 month follow-up, 56% of children in the medication management group achieved symptomatic remission (defined as a mean score of ≤1 using a combined parent–teacher measure on the MTA-SNAP-IV) compared with 25% of children who received typical community care (Jensen et al. 2001; Swanson et al. 2001; MTA Cooperative Group 2004). In a study from Taiwan, the Chinese version of the SNAP-IV, completed by the parents only, was used to examine symptomatic remission among children with ADHD switching from methylphenidate-immediate realease (IR) to methylphenidate- osmotic-release oral system (OROS) (Chou et al. 2012). Of the 439 children who completed the study, 290 (66.1%) achieved ADHD symptomatic remission using no symptoms at the “pretty much” and “very much” level as the indicator of remission (Chou et al. 2012). Although informative, both of these examples were clinical trials, which may not reflect outcomes attained within clinical services.
The current study aimed to determine key service patterns and treatment outcomes from an ADHD medication service that implemented a CMAP approach. In contrast to the previous CMAP evaluation (Pliszka et al. 2003), this study included 1) implementation and evaluation independent of CMAP developers, 2) use of a larger sample, 3) examination of a full treatment period, and 4) teacher-rated outcomes. Key research questions included 1) to what extent did medication choice and associated dosages adhere to CMAP protocols, 2) what were the associated service utilization patterns, and 3) to what extent were symptoms reduced and remitted at the end of treatment?
Methods
Setting
All children included in this study were enrolled in the Child Development–Medication Assessment Service (CD-MAS). This is a publically funded service based in the outpatient developmental pediatric services of the Alberta Children's Hospital in Calgary, Alberta, Canada. All physician costs are covered by the province's universal health insurance. Medication may be paid for through a combination of family supplemental private insurance, out-of-pocket payments, government medication coverage for eligible low-income families, and/or through pharmaceutical company supplies.
CD-MAS is a treatment service that systematically evaluates whether a given child's attentional and/or behavioral difficulties are responsive to psychotropic medication and, if so, aims to determine the optimal medication and dose based on a balance of maximal improvement with minimal emergence of adverse effects. CD-MAS is an acute phase specialized treatment service. Once an optimal medication and dose have been identified for a given child, these are designated as their medication and their maintenance dose, and they are discharged from CD-MAS and transferred to their primary care physician for long-term management.
CD-MAS is guided by the parameters of CMAP with respect to medication sequence, dosing, and use of systematically collected parent- and teacher-rated ADHD symptom severity scores throughout treatment, to inform medication titration (Pliszka et al. 2000a,b, 2006). As a clinical service responsive to individual patient needs and parental preferences, there was flexibility in the application of these guidelines; however, the following parameters were followed where possible. First, each dose of a given medication was trialed for a minimum of 1 week, unless adverse effects necessitated earlier discontinuation. Second, dosing titration increases were recommended until teacher ratings suggested minimal to no ADHD symptoms unless 1) the child had unacceptable adverse effects, 2) the parent/guardian refused further increases, or 3) the maximum dose for a given medication was reached. Third, if the child did not demonstrate minimal to no ADHD symptoms associated with a given medication, a trial of the next stage in the CMAP algorithm was recommended to be initiated, subject to parent agreement, under the same titration guidelines. Alternatively, in the event that minimal to no ADHD symptoms were demonstrated at a safe and tolerable dose of medication, a maintenance dose was designated if a minimum 4 further weeks of observation demonstrated this similar response pattern, at which point the child was discharged from CD-MAS. Unacceptable adverse effects were elicited from information derived from clinical interview; measurement of weight, pulse, and blood pressure; and parent and teacher ratings on items derived from the Barkley Symptom Checklist (Barkley et al. 1990), with a final consensus determined between clinician and parent.
The largest referral source for CD-MAS is a separate program called the Community Outreach of Paediatrics and Psychiatry in Education (COPE), a school–health partnership based in the same city. COPE provides child psychiatric and pediatric consultations for children, referred from all elementary schools in the city and an adjacent periurban school district, for whom the schools have concerns about emotional, behavioral and/or developmental problems (McLennan et al. 2008). Referral to CD-MAS requires an ADHD diagnosis by a pediatrician or child psychiatrist, and physician–parent agreement on proceeding to medication treatment.
Sample
An electronic database of patients no longer receiving care at CD-MAS, stripped of identifying information, was provided to the research team. The time period from March 1, 2007 to December 31, 2012 was covered by the database. Eligibility criteria included referral from the COPE program, and admission and discharge (or dropout) from CD-MAS within the time period available from the database. Of the 169 children admitted to CD-MAS from the COPE program during the time period, 37 had not been discharged by December 31, 2012 and were, therefore, excluded.
Measures
Data available included child age and gender, parent and teacher reports of ADHD symptom severity at the start and end of treatment, total number of service contacts, medication exposures and dosages throughout treatment, and final status as either discharged or dropped out.
A modified version of the MTA-SNAP-IV, completed by parents and teachers, was utilized to measure symptom severity, and was termed the “M-SNAP.” The MTA-SNAP-IV is composed of all the symptoms from Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) for ADHD and oppositional defiant disorder (ODD), scored on a four point severity scale (American Psychiatric Association 1994). For this study, only the 18 ADHD items were available. A total mean value across all ADHD items was generated and ≤1 used as an indicator of “symptomatic remission” (Swanson et al. 2001; Steele et al. 2006; Ramos-Quiroga and Casas 2011). Outputs were generated for 1) parent, 2) teacher, and 3) combined parent–teacher ratings with the combined ratings derived from the average of the two respondent ratings. The “baseline” ratings used for this study were those closest to initial medication initiation and the “end-point” ratings were those closest to discharge when on final/discharge dose. The difference in time between a child's discharge date and final available parent rating and teacher rating was a mean of −7.9 (SD 18.2) days and −8.4 (SD 16.7) days, respectively.
Analysis
In order to examine adherence to CMAP, flow charts representing sequence of medication choice were created to portray progression through the CMAP algorithm, similar to one presented in the original CMAP feasibility study (Pliszka et al. 2003). Frequency distributions were utilized to summarize medication class exposures, class combination exposures, and final discharge medications. To provide an index of dosing and titration, initial and final dose and extent of titration were determined for those receiving methylphenidate-based products as their first medication. Finally, service utilization patterns were examined using measures of total service contacts, total duration of time in the treatment program, and status as dropouts or discharges. Dropouts were defined as a child/family who abandoned medication treatment against medical advice. By definition they left the program on no medication. A discharge status was based on a mutual decision between the treating health professional and child/family that an optimal medication and dose for maintenance had been attained such that treatment by CD-MAS was no longer required and provision of this maintenance dose would be under the responsibility of the primary care physician. In a few cases, the mutual decision was that the child did not benefit from medication and the decision was to discharge on no medication.
Several treatment outcomes were generated. First, frequency distributions of M-SNAP scores were produced at discharge for the parent, teacher and combined subsamples. Second, the proportion of children with a mean score ≤1 at the end of treatment was determined for parent, teacher, and combined ratings for the M-SNAP, with the combined rating being a mean of parent and teacher ratings. Third, the McNemar test of paired proportions was conducted to compare children classified as having symptoms resolved at the end of treatment by each rater. Fourth, means of pre-post scores were determined, and their differences compared using two tailed paired t tests at the 0.05 significance level. Fifth, mean M-SNAP outcomes contrasting those with one, two, and three or more medication exposures were determined using ANOVAs using a significance level of 0.05.
This study was approved by the Conjoint Health Research Ethics Board (CHREB) at the University of Calgary.
Results
Characteristics of participant sample
The overall sample was composed of 132 children with 76.5% (n=101) having at least some outcome data. Table 1 provides details on the full sample and outcome subsample.
Sex differences between subsamples not significant (χ2=0.56, p=0.46).
Age differences between subsamples not significant (t[130]=−1.38, p=0.17).
Difference in parent baseline ratings not significant (t[105]=1.16, p=0.25).
Difference in teacher baseline ratings not significant (t[117]=−1.11, p=0.27).
n=81 (20 children did not have parent data at baseline and discharge).
n=91 (10 children did not have teacher data at baseline and discharge).
Includes dropouts (n=26).
n=26 (5 children did not have parent data at baseline).
n=24 (7 children did not have teacher data at baseline).
SD, standard deviation; ADHD, attention-deficit/hyperactivity disorder.
Adherence to CMAP
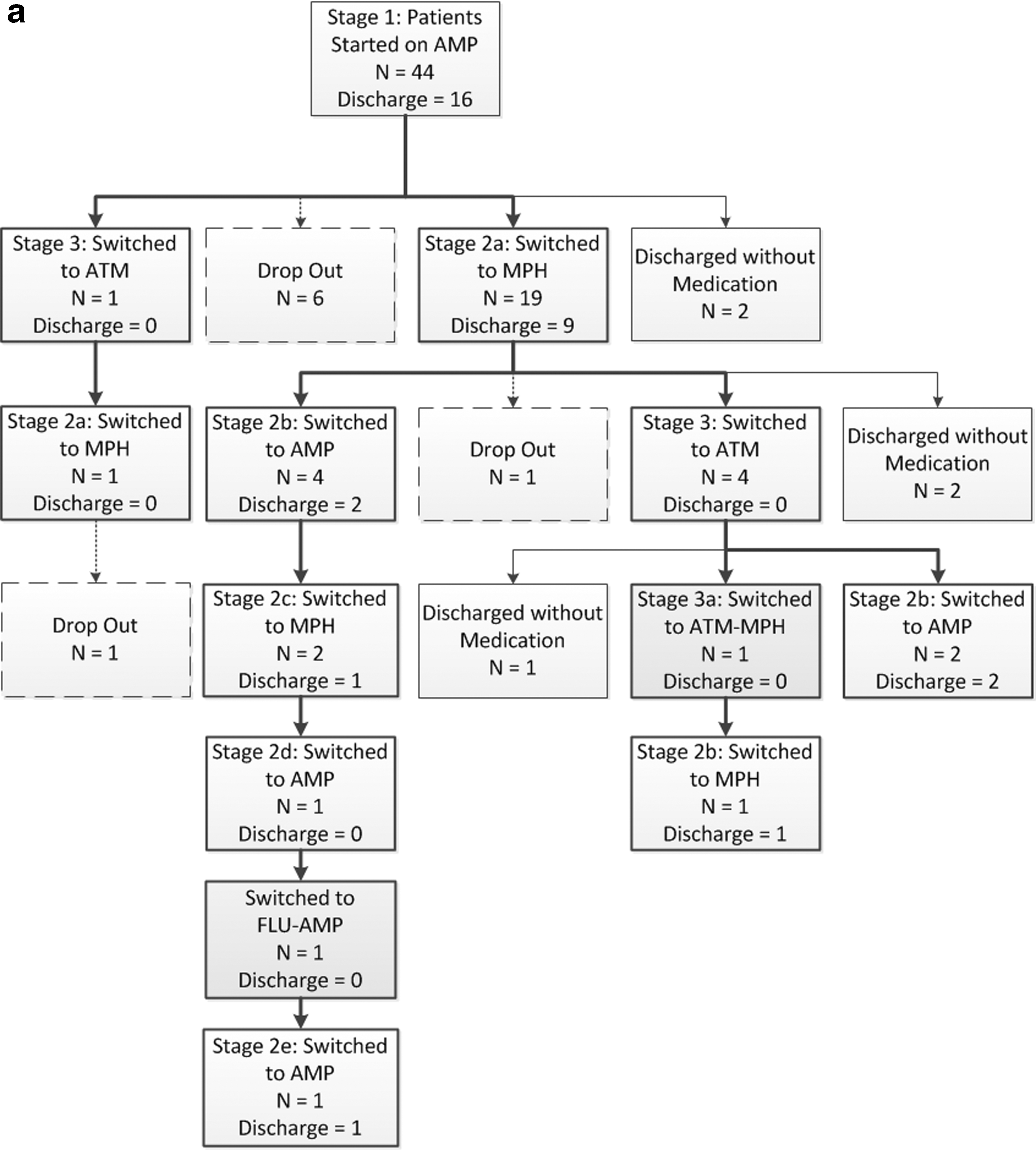
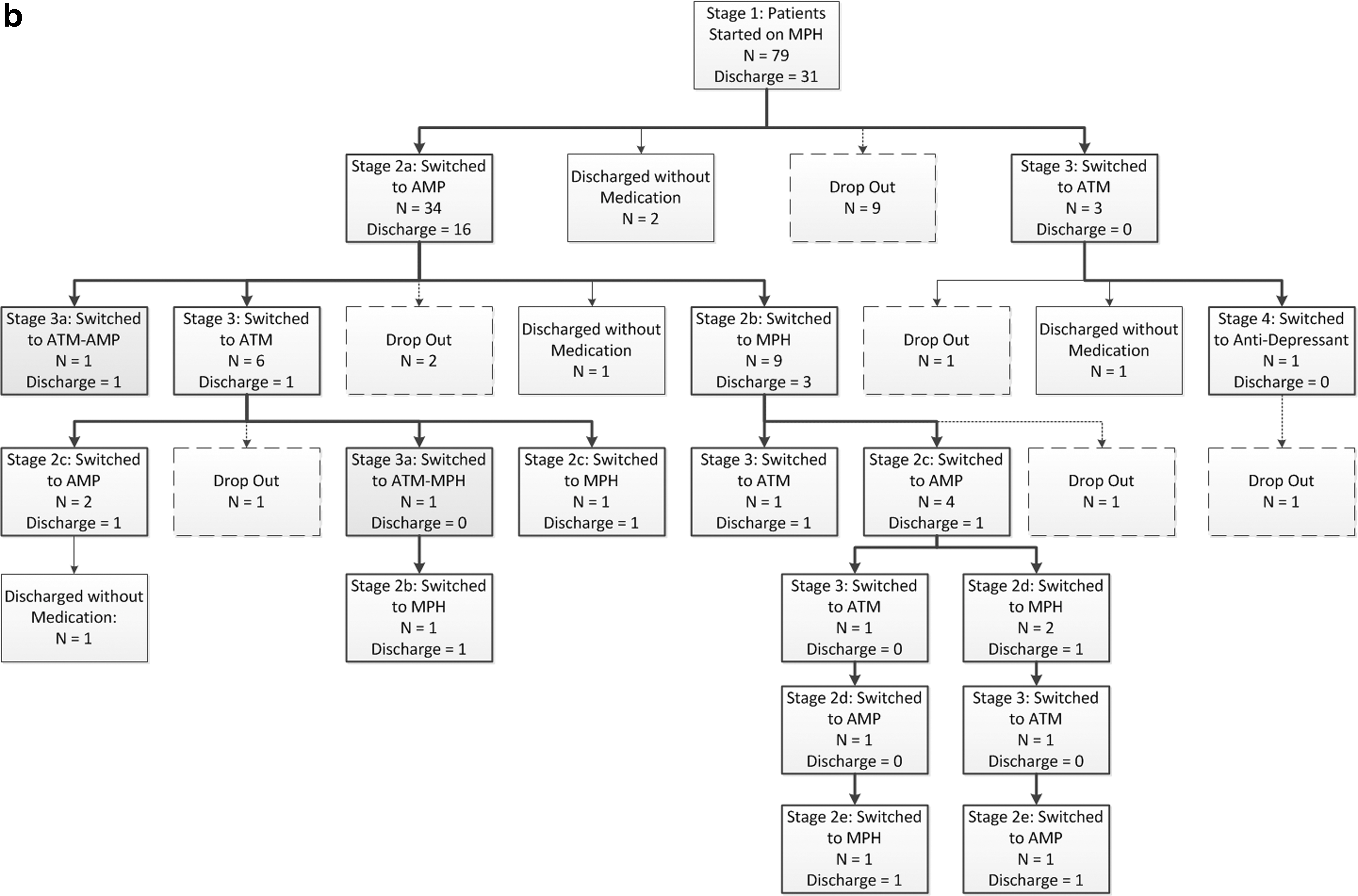
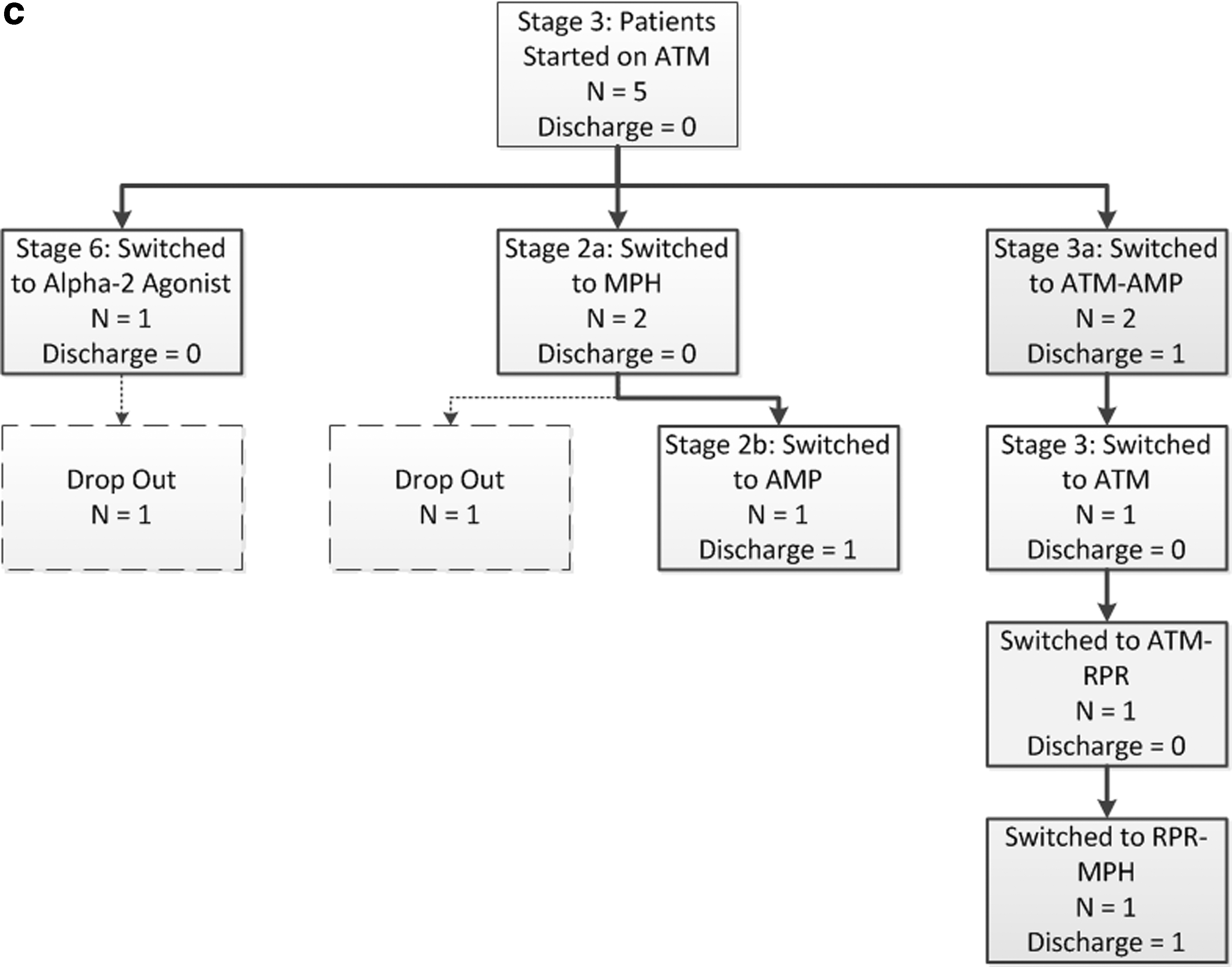
Figure 1 presents information on admission to CD-MAS and first medication exposures. Four (3.0%) children did not start medication treatment, as two dropped out from the service prior to medication initiation, and medication treatment was not recommended for the other two. Details on medication use for those progressing beyond an initial medication trial are presented in Figures 2a–c. A key difference from the CMAP algorithm in these latter stages is the tendency of repeating trials of stimulants after completing stage 2 or 3, rather than moving on to trials of antidepressants or α-2 agonists.
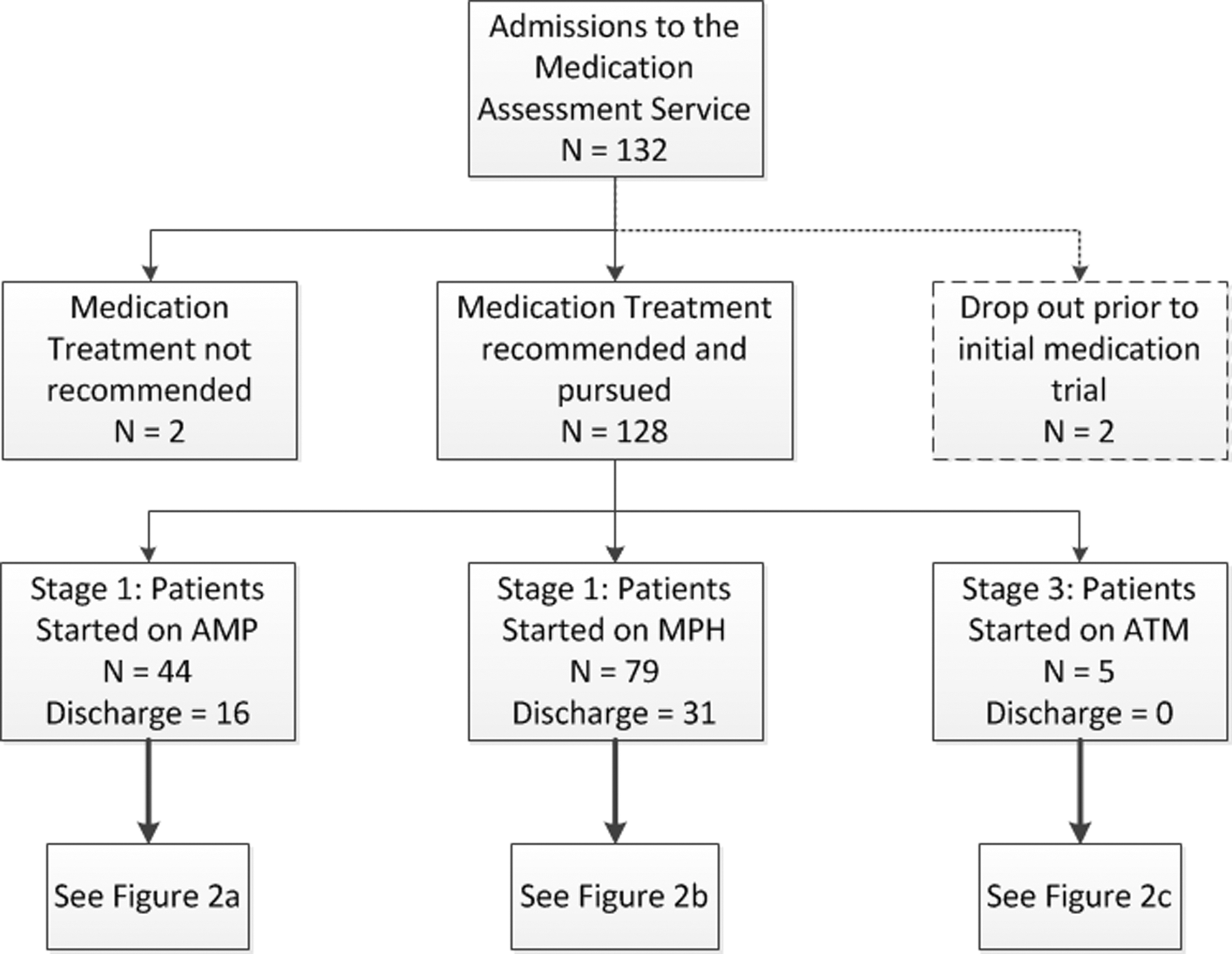
Admission and initial medication exposures. AMP, any amphetamine product; ATM, atomoxetine; MPH, any methylphenidate product.
In all cases, initial medication choice within CD-MAS was consistent with the CMAP algorithm when prior medication exposure was considered (Table 2). Of the 62 children (47.0% of total) progressing to a second medication, 7 received treatment differing from the algorithm. Whereas 4.5% of children were exposed to combination medication at some point during their treatment, only 2.3% (n=3) were actually discharged on combination medications.
All 5 had previous exposure to both classes of stimulants.
All four had only one previous stimulant class exposure each (either prior to or within the service).
One had previous exposure of MPH and AMP prior to intake. Another child had previous exposure to MPH and was on ATM at intake. ATM was continued as first medication prior to ATM-AMP exposure.
Child had been previously exposed to MPH and AMP, and was on ATM at intake but had not been tried on one of the suggested antidepressants.
Mean service contacts: 11.6 (SD 9.5). Includes combination of on-site and documented phone reviews.
Most children whose first trial was a methylphenidate-based product were initiated on the recommended starting doses, although some started at higher ones (Table 3). A few children were exposed to higher than recommended maximum methylphenidate doses, although very few were discharged on such doses. The majority of children were titrated through multiple doses.
Information on child's weight at each dosing point is not available to calculate mg/kg.
Children's Medication Algorithm Project (CMAP) recommendation is 5 mg b.i.d. (or t.i.d. at clinician's discretion); however, the lowest dose available for methylphenidate OROS is 18 mg.
Only 2 children were discharged on MPH equivalents >60 mg.
This was based on the number of different daily total MPH dose exposures for each child during the first medication trial.
Service utilization
Service contacts (on-site and/or documented phone reviews) ranged from 1 to 60 with a mean of 11.6 (S.D. 9.5) (Table 2). A total of 19.7% of the total sample dropped out at some point during treatment. Reasons for dropping out were not available. For those who were discharged, the mean total duration of time in the service was 270 (SD 243) days, with a median of 188 days.
Treatment outcomes
Table 4 summarizes the proportion of children who achieved symptomatic remission at the end of treatment. Although there are slight proportional differences between each of the subsamples, the majority achieved symptomatic remission. The reduction in ADHD symptoms from baseline to discharge was determined to be significant for the parent, teacher, and combined subsamples. Pre-post effect size changes ranged from 1.4 for the parent subsample to 2.4 for the combined parent/teacher subsample. Mean final M-SNAP scores of those discharged after the first, second, and third or more medication trials were not significantly different.
Based on a mean of combined parent and teacher scores.
Symptomatic remission considered as a mean score ≤1 on ADHD symptoms on the M-SNAP.
McNemar test revealed no significant differences in proportions classified as symptomatic remission. p=0.26.
There was a greater symptom reduction reported by teachers than by parents (t[70]=2.65, p=0.01).
Difference in Teacher Outcome ratings not significant: F=0.11, p=0.90.
Difference in Parent Outcome ratings not significant: F=0.95, p=0.39.
Difference in Combined Outcome ratings not significant: F=1.10, p=0.34.
ADHD, attention-deficit/hyperactivity disorder; MTA-SNAP-IV, Multimodal Treatment Study for ADHD - Swanson, Nolan, and Pelham, Version IV; M-SNAP, Modified MTA-SNAP-IV rating scale; SD, standard deviation.
As there is a risk for overestimating positive treatment outcomes by excluding patients without outcome data, M-SNAP summary scores were recalculated by assuming no change for those who were excluded from the initial analyses (dropouts or discharges), but who had sufficient baseline data. In other words, baseline scores were used as their outcome scores. With this recalculation, mean M-SNAP parent outcome scores (n=107) were 1.0 (SD 0.7) with 55.1% in symptomatic remission, whereas the equivalent based on teacher scores (n=119) were 1.0 (SD 0.8) with 64.7% in symptomatic remission. Combined parent and teacher mean M-SNAP scores (n=95) were 1.0 (SD 0.6) with 63.2% in symptomatic remission.
Discussion
Adherence to CMAP
This clinic generally adhered to the CMAP guidelines with respect to first and second stage medication choice, and minimizing simultaneous multiple medication use. Less consistent with CMAP was the tendency of retrialing stimulants after a trial of atomoxetine was found to be inadequate, rather than moving on to an antidepressant or α-2 agonist trial. This is similar to a pattern found in the original feasibility study with CMAP (Pliszka et al. 2003) and may be typical practice given the common situation of a partial, rather than no, response to stimulants for some children. Whereas a partial response does not result in symptomatic remission, it may be judged as better than no medication and potentially superior to, or safer than, a trial of antidepressants.
With regard to dosing parameters, only a few children started on higher than recommended initial methylphenidate doses. This may be attributable to treatment of children who were larger, older, or had previous trials in which low doses were ineffective. Second, some children were trialed on doses that exceeded recommended maximums. This may have been an attempt to attain symptomatic remission in children who demonstrated partial responses, without significant adverse effects, on maximum recommended doses. Nevertheless, only 1.5% (n=2) of children were discharged on a dose greater than the recommended maximum.
Service utilization
The commitment to implementing CMAP at CD-MAS may have resulted in greater frequency of service contacts than is seen in more typical practice. Unfortunately, there are few published service data to which these findings can be compared. In a United States medical claims analysis, dose titration was associated with children with three or more visits in their first 90 days of treatment (Olfson et al. 2009). In another study, it was found that children receiving medication treatment had an average of one to two follow-up visits per year in primary care (Zima et al. 2010). That this current study was conducted in Canada may also limit comparisons, given that physician services are free to the consumer, and there are no limits per child on the number of outpatient treatment sessions, in contrast to some United States settings.
Treatment outcomes
This represents one of the few outcome reports based on the implementation of an ADHD treatment guideline in an ongoing clinical service, in contrast to the many reported outcomes from controlled clinical research studies of ADHD. Results suggest that a substantial proportion of children can attain symptomatic remission in practice, and that this may be a function of implementation of treatment guidelines.
It is difficult to contrast the outcomes from this study with others, given the lack of explicit outcome reports from clinical practices and differences in outcome measures. However, despite methodological and sampling differences, a similar percentage of children achieved symptomatic remission in the study by Chou et al. (2012).
Although there are also important sampling, treatment, and measurement differences between this study and the MTA-study, some outcome comparisons may be of interest. At 14 months into the MTA study, 56% of children in the medication only group were rated as having symptoms resolved by combined parent–teacher ratings, in contrast with the 83.1% finding in this study (or 63.2%, using the conservative adjustment as reported in the final paragraph of the Results section) (Jensen et al. 2001). This may be a function of several factors. For example, unlike the protocols of the MTA study, there were no restrictions on medication type, dosing ranges, or duration of treatment in this study. Also, the proportion in remission from the MTA study was based on a combination of ADHD and ODD scores, whereas in this study, only the ADHD scores were available.
It is well documented that agreement between parent and teacher ratings of ADHD symptom severity are low (Wolraich et al. 2004); however, there are few reports of this relationship during medication management for ADHD. An important exception was a clinical trial that found that agreement between parent and teacher ratings of ADHD symptoms were not high enough for clinicians to rely on parent reports alone during treatment (Lavigne et al. 2012). Given these findings, we explicitly disaggregated parent and teacher ratings. In this sample, teachers tended to rate ADHD symptoms as more severe, which may be consistent with symptom manifestation in ADHD, as well as the fact that this sample is derived from school referrals. Whereas teachers reported slightly greater improvements, parents reported most children as being symptom remitted.
Limitations
There are a number of limitations to this study. First, data utilized for this study were obtained from a single clinic, and generalizability to other specialty clinics in Canada and elsewhere is unknown. Generalizability to primary care may also be challenging, unless adequate support and infrastructure for the treatment of ADHD is extended such as was attempted with the San Diego ADHD Project (Leslie et al. 2004). Second, this study was conducted without the use of a comparison group of children receiving treatment without explicit commitment to a best-practice guideline. Also, as this was not a controlled study, causality cannot be determined. Third, as our measure was restricted to symptom severity, we cannot comment on the attainment of “optimal functioning” within our sample. In contrast, the Pliszka et al. (2003) study included a functional measure, the Clinical Global Impressions–Severity score, in their assessment of the algorithm. Fourth, there was a fair amount of missing outcome data and a substantial number of dropouts in this study, although this is partly addressed by the additional offered conservative analysis. Fifth, the CMAP guidelines were developed prior to findings from randomized controlled trials (RCTs) of long-acting α-2 adrenergic agonists. From this class of medication, only short-acting clonidine was available in Canada as an off-label option at the time of this study. Sixth, CMAP does not meet all the current expected criteria for a clinical practice guideline (CPG) (Institute of Medicine 2011). However, CMAP development did include several of the Institute of Medicine (IOM) recommended CPG elements, and a number of CMAP recommendations are consistent with those given in other evidence-informed practice guidelines such as the American Academy of Child and Adolescent Psychiatry (AACAP) guidelines (Pliszka and AACAP Work Group on Quality Issues 2007).
Conclusions
Findings from this clinic's experience suggest that it is feasible to implement a best-practice guideline, although this may have driven the relatively high resource use as reflected by the large volume of appointments. The encouraging outcomes identified in this analysis also suggest that further examinations of the impact of best-practice guideline implementation may be useful, both using controlled research designs that manipulate various service components, as well as process and outcomes of real-world services.
Clinical Significance
This study indicates that it may be feasible to implement, with a high degree of fidelity, an evidence-informed, best-practice guideline into a clinical service. This may help address some of the substantial gaps identified and suspected in routine child mental health services. Furthermore, the encouraging outcomes found in this study suggest that high rates of symptomatic remission may be achieved, in clinical practice, for children with ADHD. Ideally, reporting treatment outcomes should be a routine part of clinical services, with the development of benchmark outcomes to aid in evaluating effectiveness of different clinical services and fostering continuous quality improvement with the aim of improving the effectiveness of clinical practices for children with ADHD, as well as informing refinement of current best-practice guidelines.
Footnotes
Disclosures
No competing financial interests exist.