
Abstract
Objective:
This study investigated the trends in neurocognitive function and behavioral symptoms among patients with attention-deficit/hyperactivity disorder (ADHD) during 24 months of treatment with methylphenidate in a clinical setting.
Methods:
Study participants consisted of 181 ADHD patients with a mean age of 13.4±2.5 years (ages ranged from 8 to 18 years; 151 boys and 30 girls) who were prescribed oral short-acting methylphenidate two or three times daily, with each dose ranging between 0.3 and 1.0 mg/kg. At baseline and 6, 12, 18, and 24 months from baseline, neurocognitive function was assessed using the Test of Variables of Attention (TOVA) on the day the patient was off medication, and behavioral symptoms were evaluated using the Swanson, Nolan, and Pelham Version IV Scale for ADHD (SNAP-IV) parent form, the SNAP-IV teacher form, and the ADHD-Rating Scale (completed by a child psychiatrist).
Results:
Of the 181 ADHD patients at the initial visit, 103 (56.9%) completed the study. During the 24-month methylphenidate treatment, only the commission errors in TOVA significantly improved; however, the omission errors, response time, response time variability, response sensitivity, and ADHD score did not. The behavioral symptoms of ADHD, observed by various informants, all declined substantially, and were significantly correlated with each other during the long-term follow-up. The severity of teacher ratings was lower than that of parent and psychiatrist ratings. However, the teacher-rated inattention symptoms showed the strongest correlations with TOVA performance.
Conclusions:
Findings suggest that neurocognitive deficits in ADHD patients, except inhibition ability, might be long lasting in realistic settings. In addition, obtaining behavior profile assessments from multiple informants, especially from teachers, is vital for establishing a complete understanding of ADHD patients.
Introduction
A
Methylphenidate (MPH), a psychostimulant, is the most widely administered drug for the pharmacological management of ADHD patients. Numerous studies have investigated the neurocognitive effects of long-term MPH treatment, but the findings have lacked consensus (Bidwell et al. 2011; Swanson et al. 2011). For example, Aggarwal and Lillystone (2000) indicated that commission errors (but not omission errors, response time, or variability) were significantly ameliorated after stimulant medication therapy for at least 12 months. The Multimodal Treatment study of Children with ADHD (MTA) revealed significant positive effects of the medication across all dimensions of neuropsychological function at the 24 month assessment point (Epstein et al. 2006); however, the improvements in cognitive deficits could lessen after a 2–3-year period (Swanson et al. 2008). Finally, our previous reports indicated that ADHD patients significantly improved in impulsivity and perceptual sensitivity, but not in sluggish or distractive responses, in neuropsychological tests during clinical MPH treatment for 6 months (Wang et al. 2011) and 12 months (Huang et al. 2012). Debate continues regarding whether long-term prescription of MPH enhances neurocognitive performance in ADHD patients.
While ADHD patients receive treatment, their behavioral symptoms might vary across different settings, such as at home, at school, or in a hospital (McConaughy et al. 2010). Such a difference might be related to varying patient performance, observer perceptions, or coverage of medication effects (Breuer et al. 2011). Several researchers have examined the parent–teacher agreement of symptoms associated with ADHD, mostly with a cross-sectional design. They have generally indicated that the concordance of parent and teacher ratings of ADHD symptoms is low (Gomez 2007; Murray et al. 2007; Lavigne et al. 2012). In addition, the teacher reports outperformed the parental reports regarding sensitivity and specificity for the accuracy of ADHD differential diagnoses (Tripp et al. 2006). In our previous longitudinal study (Wang et al. 2013), clinician-rated behavioral symptoms of ADHD patients improved to a greater magnitude than those rated by the parents and teachers during a 12 month treatment period. Nevertheless, few studies have investigated the agreement in ADHD symptoms observed by a patient's parents, teachers, and clinicians in a longitudinal manner.
Neuropsychological functioning might account for significant variability in ADHD symptoms (Healey et al. 2011). However, whether neuropsychological tests could serve as a reliable screening diagnostic tool for ADHD remains controversial (Epstein et al. 2003; Pineda et al. 2007). Moreover, Cho et al. (2011) revealed that teacher-rated symptoms, but not parent-rated symptoms, showed significant correlations with most subscores of neurocognitive performance in children with ADHD. By contrast, Sims and Lonigan (2012) suggested that parent ratings, but not teacher ratings, of both inattention and hyperactivity/impulsivity accounted for the variance of omission errors. Together, the relationships between neuropsychological test performance and behavioral symptoms assessed by various observers, especially in a longitudinal follow-up, are still poorly understood.
Therefore, the purpose of this study was 1) to determine whether neurocognitive function among ADHD patients improves in a sustainable manner over 24 months of treatment with MPH; 2) to examine the concordance and potential discrepancy of assessments of behavioral symptoms among different informants, including patient's parents, teachers, and a psychiatrist; and 3) to elucidate the potential correlation between neurocognitive function and behavioral symptoms during long-term treatment in a clinical setting.
Methods
Study participants
The research protocol was approved by the Institutional Review Board at Chang Gung Hospital in Taiwan. Eligible patients with ADHD treated in the Out-Patient Department of Child Psychiatry at Chang Gung Children's Hospital in Taiwan were recruited for this study if they 1) were between 6 and 18 years of age, and 2) had been clinically diagnosed with ADHD by 2 senior child psychiatrists based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV-TR) (American Psychiatric Association 2000) after structured interviews with the Chinese version of the Schedule for Affective Disorder and Schizophrenia for School-Age Children, epidemiologic version (K-SADS-E) (Kaufman et al. 1997). The Chinese version of K-SADS-E was developed by the Child Psychiatry Research Group in Taiwan (Gau and Soong 1999), and (c) were newly diagnosed with ADHD, or had an existing diagnosis but had not used ADHD medication in the previous 6 months or longer.
Patients were excluded if they 1) had a history of comorbid pervasive developmental disorders, mental retardation, bipolar disorder, psychosis, epilepsy, or brain injury or 2) required additional behavioral or family therapy other than the standard therapy at the Out-Patient Department of Child Psychiatry.
Measurements (Test of Variables of Attention [TOVA])
The TOVA was applied to assess the neurocognitive function of ADHD patients. The TOVA is a computerized, continuous performance test comprising a target stimulus and a nontarget stimulus (Greenberg 1996). The TOVA stimuli are colored squares containing a small black square, which is adjacent to either the top or the bottom edge. The stimuli appear individually and are presented randomly based on a determined ratio. The tested participant was instructed to immediately press a button after seeing a target, but not respond when a nontarget was presented. The test was 22.6 minutes and was preceded by a 2.5 minute practice session. Two visual stimuli appeared 648 times. The TOVA was reported to achieve satisfactory levels of reliability and concurrent validity in Taiwanese children with ADHD (Wu et al. 2007). The indices measured in the TOVA include the following.
Omission errors
This score is evaluated as the failure to respond to the target stimulus. Omission error scores are presented as percentages and are considered to be a measure of sustained attention.
Commission errors
This score is measured as an inappropriate response to the nontarget stimulus. Commission error scores are presented as percentages and are considered to reflect impulsivity or disinhibition.
Response time (in ms)
This score is the average of correct response times, and denotes response latency in information processing and motor response speed.
Response time variability
This score is evaluated as the standard deviation of the mean of correct response times. It is a measure of the patient's inconsistency in response times.
Response sensitivity (d’)
This score is a response sensitivity score reflecting the ratio of the hit rate to the false alarm rate; it refers to the accuracy of target and nontarget discrimination, and is interpreted as a measure of perceptual sensitivity.
ADHD score
This score is calculated by comparing individual performance on the TOVA to those of an ADHD sample collected by the authors of the TOVA. The score indicates how similar the performance of a patient is to the ADHD profile.
Measurements (The Swanson, Nolan, and Pelham Version IV Scale [SNAP-IV])
The SNAP-IV is a 26 item questionnaire that is used to evaluate ADHD symptoms and severity, and is completed by parents or teachers (Bussing et al. 2008). The 26 items include 18 for ADHD symptoms (9 for inattentive and 9 for hyperactive/impulsive) and 8 for oppositional defiant disorder symptoms as defined in the DSM-IV. Each item is scored on a 0-3 Likert scale. The Chinese version of the SNAP-IV parent form (Gau et al. 2008) and the SNAP-IV teacher form (Gau et al. 2009) were reported to have satisfactory levels of reliability and concurrent validity. In this study, only the subscales of inattention and hyperactivity/impulsivity were analyzed.
Measurements (ADHD-Rating Scale ([ADHD-RS])
The ADHD-RS is a validated instrument with which clinicians assign ratings based on information obtained from the parent(s) and child (Reid et al. 1998). The test is an 18 item checklist derived from the criteria outlined in the DSM-IV for diagnosing ADHD. Each of the items has a 4 point Likert scale ranging from 0 to 3 points. The ADHD-RS provides a total score, and can also be divided into inattentiveness and hyperactivity/impulsivity subscales. Higher scores indicate a greater severity of ADHD. The scale was reported to have good interrater reliability (Zhang et al. 2005).
Study procedure
The study was a 24 month, nonrandomized, observational, prospective study. Each patient received the same assessment five times. At Month 0, all patients were drug naïve or had not taken medication for ADHD during the previous 6 months or longer. Each ADHD patient performed the TOVA, and experienced child psychologists conducted the TOVA with individual patients in a room dedicated to reducing variability in testing conditions. The SNAP-IV parent form, SNAP-IV teacher form, and ADHD-RS were completed by the parents, a teacher of the patient, and a child psychiatrist, respectively. These informants were instructed to rate patients' symptoms based on their behaviours in the preceding 7 days.
The ADHD patients were prescribed oral short-acting MPH two or three times daily, with each dose ranging between 0.3 and 1.0 mg/kg, based on the severity of their clinical symptoms, and their age, height, and body weight. Dosage adjustment was performed at biweekly intervals to achieve adequate improvements in ADHD symptoms. The maximum dose of MPH per day was 60 mg, as this was the maximal daily dose approved in Taiwan. The dose was decreased if clinically intolerable adverse events appeared. The final titration dose of MPH with acceptable response was maintained for the subsequent follow-up period. Concomitant medications were prohibited. There was no additional behavioral therapy or family therapy provided during the period of study. Patients were usually reassessed by the child psychiatrist at the outpatient department once a month, and modification of the MPH dose was allowed. Drug compliance was confirmed at each visit based on the reports of the patients' parents and the remaining drug. Patients who started new medication between the different time points of the study were considered as dropouts.
The second, third, fourth, and fifth assessments were performed at the 6th, 12th, 18th, and 24th month after treatment with MPH, respectively. To avoid the bias derived from the time of medication administration, patients were instructed to not take MPH on the day of TOVA assessment. The assessment procedures administered at Month 0 were repeated. ADHD patients performed the TOVA, and ratings for behavioral symptoms were conducted by the same rater at Month 0.
Statistical analysis
Data were analyzed using the statistical software package SPSS, version 16.0 (SPSS Inc., Chicago, IL). Variables are presented as either the mean (standard deviation) or frequency. The TOVA results were reported as standard deviations (Z score), which indicated the extent of deviation from the norm. The χ2 test or t test was used to compare variables at baseline between ADHD patients who completed and ADHD patients who dropped out of the study.
The longitudinal data were analyzed using a linear mixed model or generalized estimating equations (GEE) that used the maximum likelihood estimation method and autoregression covariance matrix as the primary analytic strategy. Compared with traditional approaches (i.e., repeated measure analysis of variance [ANOVA]), these techniques have greater efficacy for handling missing data (Kenward et al. 1994; Zhang and Paik 2009). The linear mixed model was used to examine the trends of neurocognitive function and behavioral symptoms during 24 month follow-up, and to analyze the effects of different informants on the observation of behavioral symptoms. Bonferroni-corrected post-hoc tests were applied for multiple comparisons. We investigated the extent of the age-related and MPH dosage-related differences in changes in neurocognitive function and behavioral symptoms, also using the linear mixed model. GEE were used to explain potential correlations between TOVA performance and behavioral symptoms during the 24 months, and to control the confounding effects of age, sex, ADHD subtypes, and MPH dosage. Two tailed p values of <0.05 were considered statistically significant.
Results
A total of 181 ADHD patients (ages ranged from 8 to 18 years; mean age: 13.4±2.5 years) were recruited in this study. Of these patients, 151 (83.4%) were boys and 30 (16.6%) were girls; 93 of them (51.4%) were classified as inattentive; 10 (5.5%) were classified as hyperactive-impulsive; and 78 (43.1%) were classified as a combined type. Among the 181 ADHD patients at the initial visit, 103 (56.9%) patients completed the study. The mean dose of MPH of the patients remaining at Month 24 was 28.5±11.8 mg. Compared with the 103 patients who completed the study (Table 1), the 78 patients who left the study were significantly older (t=2.94, p=0.004) at the beginning of recruitment. No significant differences were noted in other characteristics at baseline.
TOVA results are reported as standard deviations from the norm; data are expressed as mean±SD or n (%).
Statistical values are expressed as t value or χ2.
p<0.01.
ADHD, attention-deficit/hyperactivity disorder; TOVA, Test of Variables of Attention; SNAP-IV, Swanson, Nolan, and Pelham Version IV; ADHD-RS, ADHD Rating Scale; I, inattention scores; H, hyperactivity/impulsivity scores.
Figure 1 shows the TOVA performance during the 24 month treatment of MPH in a clinical setting. Of the indices in TOVA, commission errors (F=6.52, p<0.001) significantly improved within 24 months. Compared with data at Month 0, commission errors occurred significantly less often during follow-up at Month 6 (t=2.55, p=0.011), Month 12 (t=3.83, p<0.001), Month 18 (t=4.30, p<0.001) and Month 24 (t=4.58, p<0.001). Regarding the other indices of TOVA, the omission errors (F=0.64, p=0.632), response time (F=1.04, p=0.388), response time variability (F=0.87, p=0.484), d’ (F=1.83, p=0.122), and ADHD score (F=1.34, p=0.255) did not significantly change during the 24 month treatment. There were significant age by time interactions on commission errors (F=12.41, p<0.001) and d’ (F=8.82, p=0.003), but no significant MPH dosage by time interaction on any index in TOVA was found.

Trends of neurocognitive performance, using Test of Variables of Attention (TOVA) as the neuropsychological test, in patients with attention-deficit/hyperactivity disorder (ADHD) during the 24 month treatment of methylphenidate. Higher Z scores represent better performance. The error bars represent the standard error of the mean. The commission errors significantly improved during 24 months.
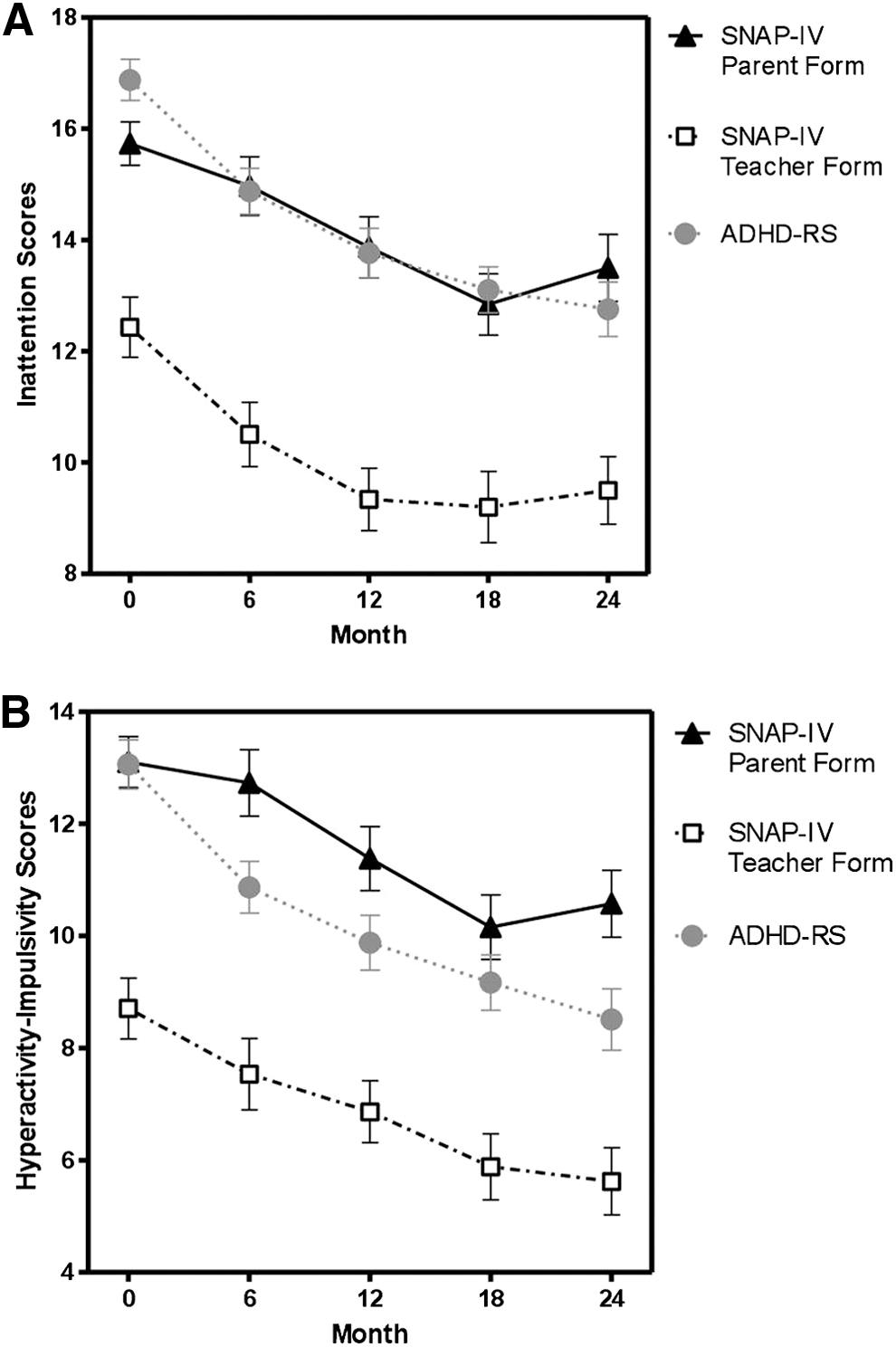
For the behavioral symptoms, the inattention scores measured by parents (F=4.27, p=0.002), teachers (F=5.68, p<0.001), and a psychiatrist (F=19.86, p<0.001) all significantly improved during the 24 month follow-up (Fig. 2A). Hyperactivity/impulsivity scores rated by parents (F=5.42, p<0.001), teachers (F=4.30, p=0.002), and a psychiatrist (F=21.66, p<0.001) also significantly declined (Fig. 2 B). For both the inattention and hyperactivity/impulsivity symptoms, the post-hoc tests (Table 2) indicated that parent and psychiatrist ratings were significantly higher than teacher ratings (p<0.001). In addition, the hyperactivity/impulsivity scores rated by parents were significantly higher than those rated by the psychiatrist (p=0.005). The symptom scores of the inattention and hyperactive/impulsive subscales rated by different observers were all significantly correlated with each other (p<0.001) (Table 3). There were significant age by time interactions on the inattention scores measured by parents (F=7.42, p=0.007), teachers (F=4.14, p=0.043), and a psychiatrist (F=26.51, p<0.001), and on the hyperactivity/impulsivity scores rated by parents (F=7.01, p=0.008) and a psychiatrist (F=29.30, p<0.001). No significant MPH dosage by time interaction on any index in TOVA was found.
Trends in
Data are analyzed using linear mixed model analysis.
p<0.01, *** p<0.001.
ADHD, attention-deficit/hyperactivity disorder; SNAP-IV, Swanson, Nolan, and Pelham Version IV; ADHD-RS, ADHD Rating Scale.
Data are analyzed using generalized estimating equations.
p<0.05, ** p<0.01, *** p<0.001.
ADHD, attention-deficit/hyperactivity disorder; TOVA, Test of Variables of Attention; SNAP-IV, Swanson, Nolan, and Pelham Version IV; ADHD-RS, ADHD Rating Scale; I, inattention scores; H, hyperactivity/impulsivity scores.
Table 3 also presents a summary of the correlation between each index of TOVA and the behavioral symptoms observed by differing informants, which were controlled for age, sex, ADHD subtypes, and dose of MPH. The teacher-rated inattention scores were significantly correlated with omission errors (B=−0.55, p=0.002), d’ (B=−0.75, p=0.010), and ADHD score (B=−0.20, p=0.043) in TOVA. The parent-rated inattention scores were significantly correlated with commission errors (B=−0.43, p=0.012) in TOVA. However, the inattention scores rated by the psychiatrist and the hyperactivity/impulsivity scores rated by parents, teachers, and the psychiatrist were not correlated with any index of TOVA.
Discussion
Trend of neurocognitive function
The findings in this study demonstrated that performance in most indices of TOVA when in a drug-free state did not change during the 24 month follow-up. Commission errors, which represent inhibition ability, was the only index of TOVA that significantly improved. Our previous report revealed that two indices in TOVA, commission errors and d’, progressed during a 12 month follow-up, even when the patient was in a drug-free state (Huang et al. 2012). However, the improved d’ result, which is an indicator of perceptual sensitivity, was not replicated in this study with a larger sample size and longer follow-up period. A previous study (Aggarwal and Lillystone 2000), in which participants were also tested off the drug, reported a comparable finding: Commission errors was the only index showing significant improvement in a 12 month interval with MPH treatment. In the natural course of ADHD, hyperactivity symptoms may remit earlier than distractibility (Spencer et al. 2007). Together with the findings in this study, we suggest that deficits in sustained attention (omission errors) in ADHD patients might be long lasting, while the patients are off medication. Inhibition ability might exhibit a higher rate of improvement than the ability to sustain attention on neuropsychological tests during a naturalistic follow-up.
One possible explanation for the improvement in commission errors is that long-term MPH treatment facilitates the inhibition ability of the patients, even when MPH is absent. However, this study was administered in a noncomparative, nonrandomized and open-label manner. We could not distinguish whether the improvement was derived from normal development of the patients or practice effects. In contrast to the studies using self-selected naturalistic settings, a well-known MTA study was conducted using a randomized-controlled design in the first 14 months. The series reports of the MTA study indicated that all dimensions of neurocognitive performance among medicated patients were superior to those among unmedicated patients at the 24 month assessment point (Epstein et al. 2006); nevertheless, the residual relative benefit of the medication treatment did not remain after 36 months (Swanson et al. 2008). Nevertheless, the participants in the MTA study were tested while they received treatment, as was routine procedure. Further research is warranted to clarify whether sustained use of MPH alters brain functions in neuropsychological assessments over time, even when MPH is withdrawn.
Trend of behavioral symptoms
Severity of ADHD behavioral symptoms for both the inattention and hyperactivity/impulsivity dimensions, as reported by various observers, significantly declined during 24 month treatment, which is generally consistent with findings in relevant literature (Jensen 2002; Huang and Tsai 2011; Buitelaar et al. 2012). However, because of the design of this study, the large improvement effect might be vulnerable and inflated by a placebo effect and the normal development of the patients.
For additional findings that were less affected by the study design, we found that the correlation coefficient between parent ratings and psychiatrist ratings (Table 3) appeared relatively higher than their correlation with teacher ratings. These noteworthy findings might reflect that psychiatrist-rated scores commonly rely on parent reports or on temporary observation in a clinical setting. Similar to the results of previous studies (Gomez 2007; Murray et al. 2007; Lavigne et al. 2012), the agreement between parent and teacher ratings was low to moderate. The ADHD behavioral symptoms rated by teachers, both for inattention and hyperactivity/impulsivity, were less severe than those rated by parents and the psychiatrist. Possible explanations for these trends include actual variation in patient behavior on different occasions, and standard discrepancies used by various observers to judge patient behavior (McConaughy et al. 2010). Furthermore, most patients recruited in this study were school aged, and all of the participating patients received short-acting MPH. Compared with parents and the psychiatrist, teachers might be in the optimal position to observe patient behavior for the duration that patients were affected by the medication (Breuer et al. 2011; Usami et al. 2013). Therefore, teachers might perceive fewer ADHD behavioral symptoms than other informants.
Relationships between neurocognitive function and behavioral symptoms
TOVA was administered at a single point in time, in accordance with the design of the study, and TOVA performance might represent a trait of the brain when functioning without medication effects. However, the ratings for the behavioral symptoms of ADHD patients might be based on global impressions over the previous few days, and the behavioral symptoms were a manifestation of a state under the control of medication effects. We found that the teacher-rated inattention symptoms showed stronger correlations with neurocognitive performance than those reported by other informants during the long-term follow-up. This may suggest that teacher-rated symptoms, which represent first-hand observation of patients' behavior in a learning situation, are particularly close to the ordinary brain functioning of ADHD patients when medication is absent. A possible reason might be that teachers have a clearer opinion of ADHD behavioral symptoms because they are familiar with age-appropriate behaviors, and, therefore, they are able to make comparisons with other pupils (de Nijs et al. 2004). Comparable with the finding in our study, a previous cross-sectional study administered in South Korea reported that teacher-rated symptoms, but not parent-rated ones, showed significant correlations with most subscores of neurocognitive tests (Cho et al. 2011). However, these results differed from those of a study conducted in the United States, which suggested that parental ratings outperformed teacher ratings regarding the correlation with neurocognitive performance (Sims and Lonigan 2012). Further research is warranted to elucidate whether these inconsistencies are attributable to the variety of target populations, cultural differences, or study procedures (i.e., cross-sectional design vs. longitudinal design; neuropsychological testing on medication vs. off medication).
Limitations
This study had certain limitations. First, the study sample was heterogeneous, and a comparison group was absent. Age is an important factor with regard to its impact on neurocognitive performance, and behaviors change (Biederman et al. 2011). In this study, a large percentage of the sample, especially of the dropout patients, likely experienced puberty during the course of investigation. Therefore, how age-related maturation influenced ADHD symptoms and TOVA performance could not be controlled in this study. Second, the severity of ADHD behavioral symptoms was measured using raw scores; however, the TOVA performance was analyzed with a Z score (age adjusted). Therefore, comparisons for the time effect on TOVA performance and behavioral symptoms might not be completely equitable. Third, although we asked that the ratings of behavioral symptoms be performed by the same rater at every visit, during such a long study period, some of the teachers of the patients might have changed because of a patient's ascending grade. Such inevitable variations in interrater reliability could also confound the results. Fourth, no measurements of neuropsychological function and behavioral symptoms were taken after baseline and during the 6th month of treatment. Therefore, in this study, it is difficult to compare the immediate effects of MPH with the long-term effects. Finally, the treatment procedure of MPH was not standardized. Although additional nonpharmacological therapy was not provided, patient treatment-seeking behaviors could not be strictly controlled for such a long study period. These issues might influence the estimation of the extent to which MPH affects TOVA performance and behavioral symptoms.
Conclusions
The results of this study indicate that inhibition ability in ADHD patients improved during the long-term follow-up, but that deficits of sustained attention might be long lasting. Compared with parent and psychiatrist ratings, the severity of teacher ratings for behavioral symptoms was lower; however, the teacher-rated inattention symptoms showed stronger correlations with neurocognitive performance. Therefore, obtaining assessments of behavioral profiles from multiple informants, especially from teachers, is crucial for establishing a more complete picture of patients with ADHD. However, a future study containing a comparison group could confirm whether the trends in cognition and behavior are attributed to long-term effects of MPH or natural alterations from maturation.
Clinical Significance
Although behavioral symptoms of ADHD declined substantially during 24 months of treatment with MPH, neurocognitive deficits in ADHD patients, except inhibition ability, might be long lasting. Gathering behavioral profiles from multiple informants is essential for gaining a complete picture of patients with ADHD. Of the information collected from various informants, teacher-rated symptoms, which represent first-hand observation of patients' behavior in a learning situation, are particularly important, and show the strongest correlations with neurocognitive performance.
Footnotes
Acknowledgments
We thank Wei-Tsun Soong for granting us the use of the Chinese version of the K-SADS, and Shur-Fen Gau for granting us the use of the Chinese version of the SNAP-IV. This study was funded by a grant (CMRPG260181) from Chang Gung Memorial Hospital, Taiwan.
Disclosures
No competing financial interests exist.