
Abstract
Objective:
The objective of this study was to investigate the short-term treatment effects of atomoxetine on autism spectrum disorder (ASD) symptoms in children and adolescents with both ASD and attention-deficit/hyperactivity disorder (ADHD).
Methods:
A total of 97 patients 6–17 years of age, with ASD and ADHD, were treated with 1.2 mg/kg/day of atomoxetine during an 8 week double-blind placebo-controlled period. Here, we investigated effects on two parent-based secondary outcome measures, the Aberrant Behavior Checklist (ABC) and the Children's Social Behavior Questionnaire (CSBQ).
Results:
After 8 weeks of double-blind treatment, atomoxetine administration was associated with significant treatment effects on the ABC subscales Hyperactivity, Inappropriate Speech, and Stereotypic Behavior, and on the CSBQ subscale Fear for Changes.
Conclusions:
Our study results indicate no beneficial effects of atomoxetine on social functioning. However, atomoxetine may ameliorate restricted and stereotyped behaviors and communication.
This study has been registered in ClinicalTrials.gov (
Introduction
A
There is currently no curative treatment for ASD. The overall treatment goal is to improve the child's functioning, ideally by reducing impairments in social interaction and communication, and repetitive behaviors. Behavioral interventions can improve children's language abilities, play and cognitive skills, and social functioning, and may reduce maladaptive behavior (Dawson and Burner 2011). Psychotropic medication may also improve children's functioning and allow children with ASD to benefit more optimally from educational interventions (Anagnostou and Hansen 2011; Huffman et al. 2011).
The three classes of medication most extensively studied in ASD clinical trials are atypical neuroleptics, psychostimulants, and selective serotonin reuptake inhibitors (SSRIs). Current evidence indicates efficacy of atypical neuroleptics for ameliorating irritability and repetitive behaviors in ASD, with the strongest level of empirical support for risperidone and aripiprazole (McDougle et al. 2005; Marcus et al. 2009, 2011). Further, positive effects of methylphenidate on social communication and self-regulation in children with ASD and hyperactivity have been observed (Jahromi et al. 2009). Finally, a well-designed and powered study indicated ineffectiveness of citalopram, suggesting no clear place for SSRIs in the treatment of children with ASD (King et al. 2009).
Atomoxetine, a noradrenergic reuptake inhibitor registered for the treatment of ADHD, may be effective in ameliorating ADHD symptoms in children with ASD, as indicated by a number of small-scale studies (Jou et al. 2005; Arnold et al. 2006; Posey et al. 2006; Troost et al. 2006) and by our placebo-controlled trial involving almost 100 subjects (Harfterkamp et al. 2012). Some of the smaller studies had also suggested improvements in core ASD symptoms and social functioning (Arnold et al. 2006; Posey et al. 2006).
Our study in children and adolescents with combined ASD and ADHD consisted of a first 8 week double-blind period of atomoxetine versus placebo followed by a 20 week open label continued treatment period,and used the ADHD rating scale (ADHD-RS) as a primary outcome measure (Faries et al. 2001). Here, we present the possible effects of atomoxetine on ASD symptoms as investigated in the placebo-controlled part of the study, measured by two parent-based secondary outcome measures, the Aberrant Behavior Checklist (ABC) (Aman et al. 1985) and the Children's Social Behavior Questionnaire (CSBQ) (Hartman et al. 2006).
Methods
Study participants
We provided detailed inclusion criteria previously (Harfterkamp et al. 2012). In brief, subjects had to be between 6 and 17 years of age, have an intelligence quotient of at least 60, and have a dual diagnosis of ASD and ADHD. ASD diagnosis was based on clinical assessment, and had to be corroborated by at least two subscale scores on the Autism Diagnostic Interview Revised (ADI-R) above the cutoff (Rutter et al. 2003); ADHD diagnoses had to meet Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) criteria A through D for ADHD any type (American Psychiatric Association 2000). Nine Dutch child and adolescent psychiatry centers, six university centers (Amsterdam, Groningen, Leiden, Maastricht, Nijmegen, and Utrecht), and three non-university centers (The Hague, Hoorn, and Oosterhout) could recruit patients for the study. Exclusion criteria included a weight of <20 kg; presence of psychosis, bipolar disorder, or substance abuse; a serious medical illness; history of seizures; ongoing use of psychoactive medications other than the study drug; and intended start of a structured psychotherapy or inpatient treatment.
Both parents and subjects≥12 years of age had to give written informed consent, and younger children had to assent. The study had been approved by the national and local institutional review board committees. Participants were enrolled in the placebo-controlled study from October 2006 to March 2008.
Study interventions
Patients were randomized in a 1:1 ratio to receive either placebo or atomoxetine capsules titrated to a fixed once-daily dose of 1.2 mg/kg/day (1st week: 0.5 mg/kg/day; 2nd week: 0.8 mg/kg/day; then 1.2 mg/kg/day for 6 weeks).
Outcome measures
To rate changes in ASD symptoms, we used two parent-based questionnaires, the ABC and the CSBQ, which were obtained at baseline and at the end of the study, that is, after 8 weeks. The ABC is a 58 item scale that consists of five subscales, labeled Irritability (includes agitation, crying, and self-injurious behaviors, and contains 15 items, e.g., screams inappropriately; is aggressive to other children or adults; depressed mood); Lethargy/Social Withdrawal (includes social withdrawal, has 16 items, e.g., seeks isolation from others; does not try to communicate with words or gestures; fixed facial expression); Stereotypic Behavior (7 items, e.g., moves or rolls head repetitively; repetitive hand, body, or head movements); Hyperactivity (includes noncompliance, 16 items, e.g., impulsive [acts without thinking]; restless, unable to sit still; disobedient, difficult to control), and Inappropriate Speech (4 items, e.g., talks excessively; repetitive speech). The ABC was developed as a measure of treatment effects in patients with developmental disabilities. It has been used in drug research and other forms of clinical research and has been shown to be sensitive to the effects of psychotropic drugs (Aman et al. 1985; Troost et al. 2006; Karabekiroglu and Aman 2009).
The CSBQ consists of 49 items covering a broad range of features typical for ASD, from subtle social, communication, and repetitive behavioral impairments seen in children with milder forms of ASD, to more severe autistic-like features, with an emphasis on the former (Hartman et al. 2006). Items are rated in a three point Likert-type fashion (i.e., 0=does not apply at all; 1=applies slightly or infrequently; 2=applies clearly or often). The CSBQ consists of a total scale and six subscales: Subscale 1, Behavior/emotions not optimally tuned to the social situation (11 items, e.g., does not know when to stop; goes on and on about things; makes a fuss over little things; makes a mountain of a mole hill); Subscale 2, Reduced contact and social interest (12 items, e.g., has little or no need for contact with others; does not seek comfort when he/she is hurt or upset; lives in a world of his/her own); Subscale 3, Orientation problems in time, place, or activity (8 items, e.g., does things without realizing what stage of the activity he/she is; has no sense of time); Subscale 4, Difficulties in understanding social information (7 items, e.g., takes things literally; is exceptionally naïve); Subscale 5, Stereotyped behavior (8 items, e.g., is extremely pleased by certain movements and keeps doing them; is fascinated by certain colors, forms, or moving objects); and Subscale 6, Fear of and resistance to changes (3 items, e.g., panics in new situations or if change occurs). Multiple estimates of reliability and validity of the CSBQ were found to be good (Luteijn et al. 2000; Hartman et al. 2006; de Bildt et al. 2009).
Data analysis
Analyses were conducted on the full data set which, following the intent-to-treat principle, included all randomized patients receiving at least one dose of the study drug. Changes from baseline to 8 weeks on the ABC subscales and the CSBQ total scale and subscales were analyzed using analysis of covariance (ANCOVA), imputing missing values based on last observation carried forward (LOCF). ANCOVA included fixed effects for treatment group and baseline score. We used a p value <0.05 to indicate statistical significance. In light of the relatively small sample size, we did not adjust the α level for multiple comparisons, to avoid false negative findings.
Results
Participants
Figure 1 shows the flow of the 97 participants through the study. The baseline demographic and clinical characteristics of participants were similar between the treatment groups in the double-blind treatment phase (Table 1). As stated in the flow diagram, 5 of 48 subjects randomized to atomoxetine and 3 of 49 subjects randomized to placebo discontinued for a variety of reasons.
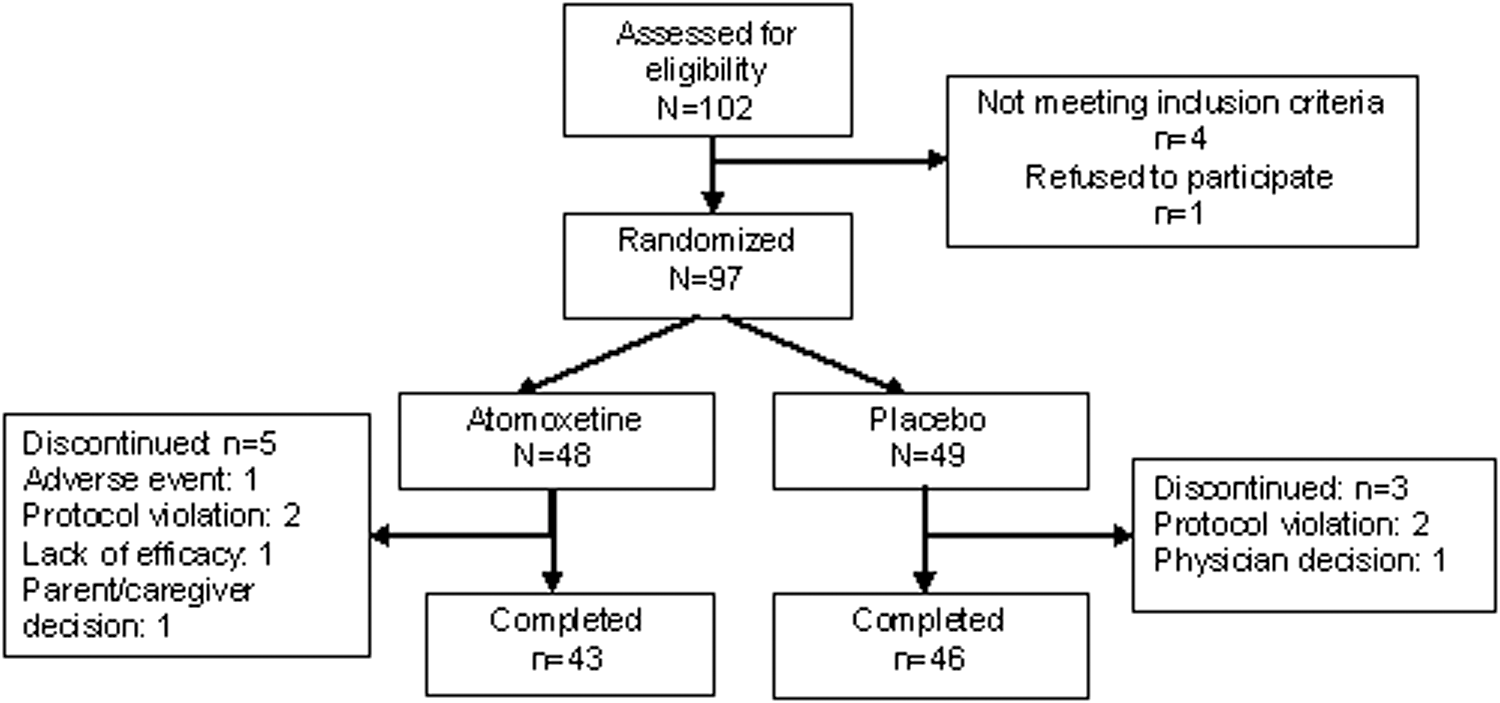
Flow diagram of a trial of atomoxetine versus placebo in children and adolescents with autism spectrum disorder and attention-deficit/hyperactivity disorder symptoms.
Based on clinical diagnosis, corroborated by ADI-R.
Based on clinical diagnosis, corroborated by ADI-R, but two participants (one in each treatment group) had a clinical diagnosis of ASD that was (in deviance with the protocol) not corroborated by ADI-R scores.
ADHD, attention-deficit/hyperactivity disorder; ADI-R, Autism Diagnostic Interview-Revised; ASD, autism spectrum disorder; IQ, intelligence quotient.
Outcomes
After 8 weeks of double-blind treatment, the scores on the ABC subscales Hyperactivity, Inappropriate Speech, and Stereotypic Behavior, and the CSBQ subscale Fear for Changes were significantly more lowered from baseline in the atomoxetine than in the placebo group. None of the other ABC subscales or the CSBQ total scale or subscales showed statistically significant different change scores from baseline to 8 weeks of treatment between the atomoxetine and placebo groups (Table 2).
Based on last observation carried forward analysis of covariance (ANCOVA)
ABC, Aberrant Behavior Checklist; CSBQ, Children's Social Behavior Questionnaire; LS, Least Squares.
Discussion
The present study investigated possible effects of atomoxetine on ASD symptoms in children with ASD and ADHD symptoms. We used parent-based secondary outcome measures (ABC and CSBQ) in an 8 week double-blind placebo-controlled trial. Overall, no treatment effects were observed on the hallmark ASD symptom domain of impairments in social interaction, as indicated by lack of improvements on the CSBQ subscales Not Tuned, Reduced Contact, and Social Information.
Still, we observed some modest improvements in other ASD symptom domains. We found superior effects of atomoxetine on the ABC subscales Hyperactivity, Inappropriate Speech, and Stereotypic Behavior. Obviously, the effect on the ABC Hyperactivity subscale is directly related to improvements in ADHD symptoms, in line with our previously reported findings of superior effects of atomoxetine compared with placebo on the clinician-based ADHD-RS (Harfterkamp et al. 2012). The other two ABC subscales contain items referring to communication and stereotyped behaviors. These ABC findings are largely in line with two earlier, small-scale studies with atomoxetine in children with ASD. A small-scale double-blind placebo-controlled crossover study of clinically titrated atomoxetine and placebo, 6 weeks each, separated by a 1 week washout, in 16 children and adolescents with ASD, reported effects on the ABC subscales Hyperactivity and Lethargy/Social Withdrawal (Arnold et al. 2006). Another 8 week open-label prospective study in 16 children with ASD showed effects of atomoxetine on the ABC subscales Hyperactivity, Stereotypic Behavior, Lethargy/Social Withdrawal, and Inappropriate Speech (Posey et al. 2006). It should be noted, however, that our finding of an overall change of ∼ 20% on the four item ABC Inappropriate Speech subscale, although statistically significant, may not necessarily point to improvement in Inappropriate Speech per se, but could rather be related to changes in ADHD symptoms (e.g., the ABC Inappropriate Speech item “talks excessively” could have improved because of decreased ADHD symptoms rather than a change in core features of ASD).
Fear of changes was the only CSBQ subscale on which atomoxetine had better effects than placebo. This is in line with previous studies that had suggested possible effects of atomoxetine on anxiety, as found in children and adults with ADHD and an anxiety disorder (Geller et al. 2007; Adler et al. 2009). However, better handling of changes may also indicate an effect of atomoxetine on ameliorating restrictive behavior, in line with the positive effects of atomoxetine on the ABC Stereotypic Behavior subscale. It must be noted, however, that the CSBQ Fear of Changes subscale has only three items; with a decrease of ∼ 20%, the improvement may not be clinically meaningful. Also, the lack of improvement in the Stereotypy CSBQ subscale does not substantiate the possible effects of atomoxetine on ameliorating stereotyped behaviors. Although we have no direct explanation for the differing results on the CSBQ subscale Stereotypy versus the ABC subscale Stereotypic Behavior, the lack of consistency most likely reflects differences in item content between these two subscales.
Limitations
A number of limitations need to be acknowledged. Perhaps the most critical one has been the choice of rating scales to assess improvements in ASD symptoms. For this, we relied entirely on parent ratings, without clinical assessment, observation, or use of teacher ratings. However, the ABC has become something of a gold standard for trials in this area. As a second limitation, it should be noted that the study had not been primarily powered to investigate improvements in ASD symptoms. It cannot be excluded that a larger sample size would still indicate effects of atomoxetine on social behavior, even when adjusting levels of significance for multiple comparisons.
Conclusions
In summary, our study indicates no beneficial effects of atomoxetine on social functioning after 8 weeks of treatment. These results are in line with existing studies showing that social functioning is not very responsive to currently available psychopharmacological treatments that have been tested in ASD to date (Anagnostou and Hansen 2011; Huffman et al. 2011). Still, we did find some indication of beneficial effects of atomoxetine on stereotyped behaviors, inappropriate speech, and fear of change, and on hyperactivity. The latter finding is in line with our previously reported improvements in ADHD symptoms (Harfterkamp et al. 2012, 2013). These benefits may help children and adolescents with ASD to profit more from behavioral interventions, which should be investigated in future studies.
Clinical Significance
ASD are a continuum of developmental disorders characterized by impairments in social interaction and verbal and nonverbal communication skills, and stereotyped behaviors, with various frequently co-occurring problems such as symptoms of ADHD, self-injurious behavior, aggression, mood problems, sensory differences, sleep dysfunction, and intolerance of change. Whereas we previously found effects of atomoxetine on ADHD symptoms in children with ASD and co-occurring symptoms of ADHD, the current analyses suggest no beneficial effects of atomoxetine on social functioning. These results are in line with existing studies showing that social functioning is not very responsive to currently available psychopharmacological treatments that have been tested in ASD patients to date. Still, we did find some indication of beneficial effects of atomoxetine on stereotyped behaviors, inappropriate speech, and fear of change, and on hyperactivity.
Footnotes
Acknowledgments
We thank all participating sites in The Netherlands.
Disclosures
Myriam Harfterkamp has accepted invitations for congress travels from Eli Lilly and Eurocept. Ruud B. Minderaa was advisor for Eli Lilly. Jan K. Buitelaar has been a consultant to/member of advisory board of, and/or speaker for Bristol-Myer Squibb, Eli Lilly, Janssen Cilag BV, Medice, Organon/Shering Plough, Servier, Shire, and Union Chimique Belge (UCB). Gigi van de Loo-Neus has received honoraria for a presentation from Eli Lilly and was member of the advisory board for UCB Pharma B.V. and Shire. Rutger-Jan van der Gaag has no financial disclosures. Pieter J. Hoekstra has received honoraria for presentations or advice from Desitin, Eli Lilly, and Shire.