
Abstract
Objective:
The purpose of this study was to assess the risk of manic switch associated with antidepressants in Medicaid-enrolled pediatric patients with bipolar depression.
Methods:
This retrospective cohort study involved 2003–2007 Medicaid Analytic eXtract (MAX) data from four geographically diverse states. The study sample included children and adolescents (ages 6–18 years) who had received a diagnosis of bipolar disorder on two or more separate occasions or during a hospital discharge, followed by a diagnosis of depression. According to the pharmacotherapy received by these patients in the 30 days around the index bipolar depression diagnosis, patients were categorized into five mutually exclusive groups. Manic switch was defined as having received a diagnosis of mania within 6 weeks after the initiation of bipolar depression treatment. Relative risks of manic switch between antidepressant monotherapy/polytherapy and their alternatives were assessed using Cox proportional hazards model. The robustness of the conventional Cox proportional hazards model toward possible bias caused by unobserved confounders was tested using instrumental variable analysis, and the uncertainty regarding manic switch definition was tested by altering the duration of follow-up.
Results:
After applying all the selection criteria, 179 antidepressant monotherapy, 1047 second-generation antipsychotic (SGA) monotherapy, 570 mood stabilizer monotherapy, 445 antidepressant polytherapy, and 1906 SGA–mood stabilizer polytherapy users were identified. In Cox proportional hazard analyses, both antidepressant monotherapy and polytherapy exhibited higher risk of manic switch than their alternatives (antidepressant monotherapy vs. SGA monotherapy, hazard ratio [HR]=2.87 [95% CI: 1.10–7.49]; antidepressant monotherapy vs. mood stabilizer monotherapy, HR=1.41 [95% CI: 0.52–3.80); antidepressant polytherapy vs. SGA-mood stabilizer polytherapy, HR=1.61 [95% CI: 0.90–2.89]). However, only the comparison between antidepressant monotherapy and SGA monotherapy was statistically significant. The instrumental variable analysis did not detect endogeneity of the treatment variables. Extending the follow-up period from 6 weeks to 8 and 12 weeks generated findings consistent with the main analysis.
Conclusions:
Study findings indicated a higher risk of manic switch associated with antidepressant monotherapy than with SGA monotherapy in pediatric patients with bipolar depression. The finding supported the clinical practice of cautious prescribing of antidepressants for brief periods.
Introduction
B
Until 2002, antidepressant monotherapy had been recommended as the first-line treatment for bipolar depression in all treatment guidelines for adults (Baldessarini et al. 2007; Amit and Weizman 2012). That year, the American Psychiatric Association (APA) treatment guidelines relegated antidepressants to second-line use after initial treatment with mood stabilizer monotherapy (Hirschfeld et al. 2002). However, there has been debate over whether antidepressants are safe and effective medications for the condition, both before and after the APA revision. Multiple observational studies including patients' self-reports and naturalistic studies reported a higher risk of manic switch associated with the use of antidepressants in adults with bipolar depression (Peet 1994; Altshuler et al. 1995; Boerlin et al. 1998; Henry et al. 2001; Ghaemi et al. 2003; Truman et al. 2007). However, most of the clinical trials included in the review by Licht et al. (2008) and in the meta-analysis by Gijsman et al. (2004) did not find statistically significant differences between antidepressants and placebo regarding the risk of manic switch.
Critical evaluation of these clinical trials suggested that it is difficult to make a confirmatory conclusion based on available evidence, because of the presence of biases in the existing trials (Licht et al. 2008). For example, in some of the randomized controlled trials (RCTs) that compared the risk of manic switch between antidepressants and placebo, 75% of the patients were concomitantly treated with mood stabilizers or second-generation antipsychotics (SGAs). Also, these trials captured manic switch during various follow-up times, and did not report whether the switch occurred during acute treatment for depression or after remission, thereby drawing inconclusive evidence for manic switch risk with antidepressants (Licht et al. 2008).
Bipolar disorder with childhood onset seems to be more severe than the form that first appears in adults (Perlis et al. 2004; Birmaher et al. 2006). Although there are no empirical data available to clarify the association between antidepressant monotherapy and the risk of manic switch in this subgroup, some indirect evidence suggests that children and adolescents with bipolar disorder may have symptoms more often and switch moods more frequently than adults with the illness. In a recent study conducted among a cohort of youth (9–20 years) with depressive and anxiety disorders, and with at least one parent with bipolar I disorder, 21% had been treated with antidepressants. Among these antidepressant recipients, 57% had had an adverse reaction in the form of manic symptoms (irritability, aggression, impulsivity, or hyperactivity), leading to antidepressant discontinuation (Strawn et al. 2014). Therefore, the existing pediatric guidelines for bipolar disorder tend to be more conservative in recommending the use of antidepressants. Antidepressant monotherapy was never recommended, and the use of antidepressants as an adjunct treatment was mentioned as “may not be necessary unless the depressed phase persists or becomes severe” (McClellan et al. 1997) and “caution must be taken because antidepressants may destabilize the patient`s mood or incite a manic episode” (McClellan et al. 2007). However, our previous research using Medicaid data revealed that antidepressants were used in nearly half (48.17%) of children and adolescents with bipolar depression, of whom 42.40% received it as an adjunct treatment and 5.77% received is as a monotherapy (Bhowmik et al. 2013).
Almost all existing clinical trials assessing manic switch associated with the use of antidepressants compared them to placebo (Mendlewicz and Youdim 1980; Himmelhoch et al. 1982; Cohn et al. 1989; Nemeroff et al. 2001; Tohen et al. 2003). However, in practice, the more clinically relevant issue is the risk from antidepressants versus their alternatives. Head-to-head comparison data between antidepressant monotherapy and SGA/mood stabilizer monotherapy, or between antidepressant polytherapy and SGA/mood stabilizer polytherapy, are needed. Therefore, the objectives of this study were to evaluate the comparative risk of manic switch associated with 1) antidepressant monotherapy versus SGA monotherapy, 2) antidepressant monotherapy versus mood stabilizer monotherapy, and 3) antidepressant polytherapy (with SGA or mood stabilizer) versus SGA-mood stabilizer polytherapy in Medicaid-enrolled children and adolescents with bipolar depression. We hypothesized that an antidepressant, when used alone or in combination with a mood stabilizer/SGA in children with bipolar depression, was associated with increased risk of manic switch compared with corresponding SGA and mood stabilizer monotherapies or combination.
Methods
Data source
In this retrospective cohort study, 2003–2007 Medicaid Analytic eXtract (MAX) files from the Center for Medicare and Medicaid Services (CMS) were used to achieve the study objectives. The MAX is a set of person-level claims data files containing information on Medicaid eligibility, demographics, service utilization, and payments. We used data from four geographically diverse states with large Medicaid enrolments of children and adolescents (CA, TX, IL, and NY).
Pharmacotherapy for bipolar depression
The pharmacotherapies for bipolar depression assessed in this study were mood stabilizers (lithium, sodium divalproex/valproate, oxcarbazepine, topiramate, lamotrigine, and gabapentin); SGA (risperidone, aripiprazole, olanzapine, quetiapine, clozapine, and ziprasidone); newer antidepressants (serotonin reuptake inhibitor [SSRI] antidepressants and others, citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, venlafaxine, and bupropion); and other antidepressants (amitriptyline, clomipramine, desipramine, doxepin, imipramine, nortriptyline, mirtazapine, nefazodone, and trazodone) (Bhowmik et al. 2013).
Study population
The study design and cohort identification process are presented in Figure 1. Children and adolescents with bipolar depression were identified based on the following algorithm (Bhowmik et al. 2013): 1) 6–18 years of age (children and adolescents), 2) having received a minimum of two diagnoses of bipolar disorder other than bipolar depression (International Classification of Diseases, 9th version, Clinical Modification [ICD-9-CM]: 296.0, 296.1, 296.4-296.8, 301.11, 301.13) on different service dates, or only one diagnosis of bipolar disorder that came from hospital discharge, followed by a diagnosis of depression (ICD-9-CM: 296.5, 296.2, 296.3) (Busch et al. 2008) any time between January 2003 and December 2007; and 3) having received antidepressants, SGA, or mood stabilizers within 30 days of the depression diagnosis. The date on which the first prescription of these medications was filled was defined as the index date.
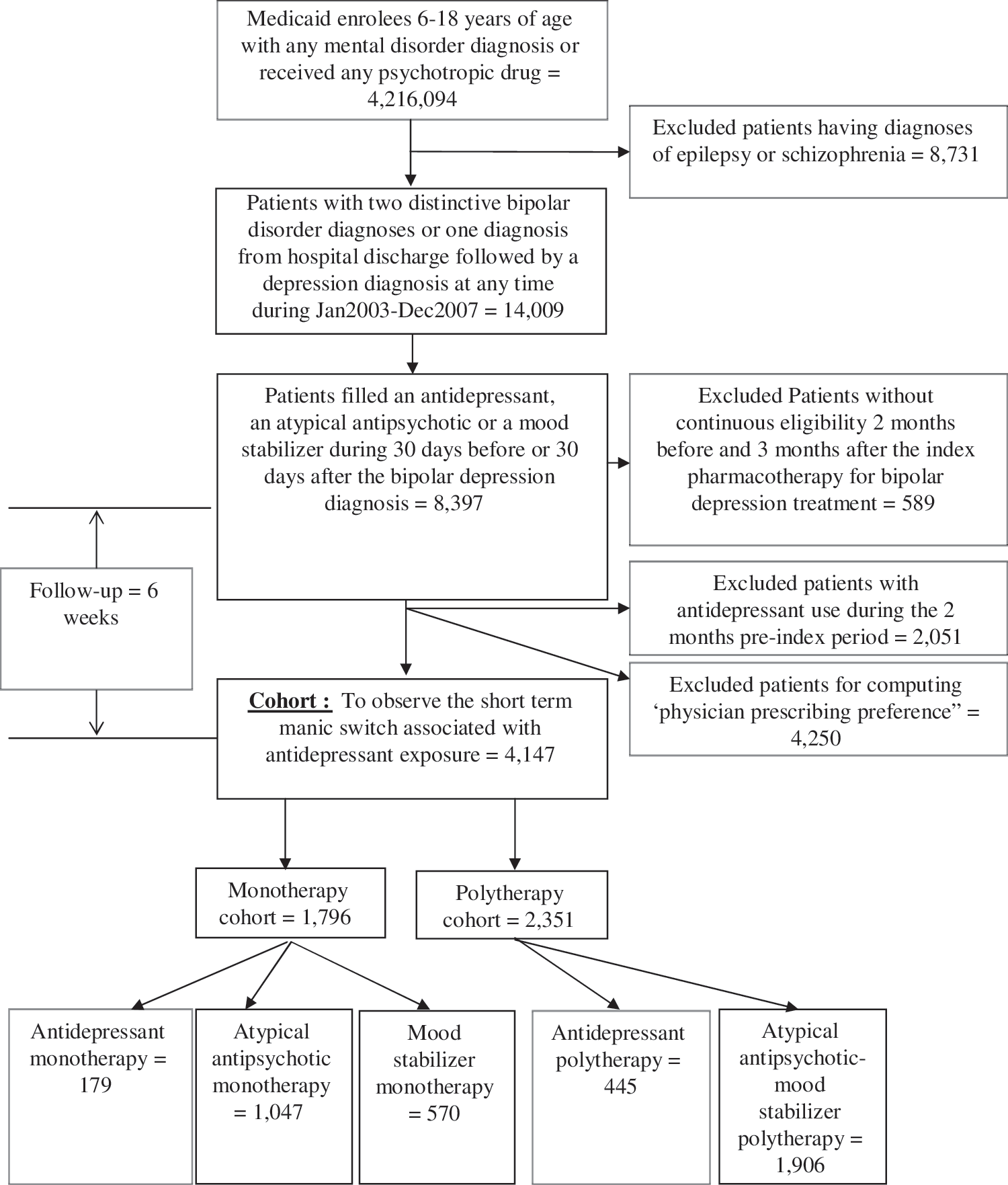
Consort diagram.
Exclusion criteria
Patients who received diagnoses of schizophrenia (ICD-9-CM: 295.0-295.9) or epilepsy (ICD-9-CM: 345.xx) were excluded from the cohort, to increase the likelihood that the prescriptions were used for the treatment of bipolar disorder. Patients without continuous Medicaid eligibility 2 months prior to and 3 months after the index date were also excluded. Finally, for identification of new users of antidepressants, patients who had received antidepressant prescriptions during the 2 month pre-index period were excluded.
The bipolar depression patients identified were then divided into five mutually exclusive groups based on their medication use during 30 days around the index bipolar depression diagnosis: 1) Antidepressant monotherapy, 2) SGA monotherapy, 3) mood stabilizer monotherapy, 4) antidepressant–SGA or antidepressant–mood stabilizer polytherapy, and 5) SGA–mood stabilizer polytherapy. Monotherapy was defined as receiving medications from a single therapeutic class only, whereas polytherapy was defined as receiving medications from different therapeutic classes within 30 days of the depression diagnosis and with a minimum of 14 day overlap between the prescriptions.
Manic switch
Manic switch events were identified from the combined inpatient and other therapy MAX files, using the ICD-9-CM codes of mania (296.0, 296.1, 296.4, 296.81) during the 6 week follow-up period after the index date. The follow-up window was restricted to 6 weeks to differentiate manic events as being treatment emergent rather than the natural progression of bipolar disorder itself (Salvadore et al. 2010).
Statistical analyses
Descriptive analysis was conducted to describe the demographics, treatment utilization, comedications, and comorbidities during the 2 month pre-index period for the monotherapy and polytherapy users, respectively. Time to manic switch was analyzed using a multivariable Cox proportional hazards regression model to assess the risk of manic switch associated with bipolar depression treatment. The analyses evaluated antidepressant monotherapy versus mood stabilizer or SGA monotherapy and antidepressant polytherapy versus SGA–mood stabilizer polytherapy. Kaplan–Meier plot, log-minus-log survival plot, and Schoenfeld residual test were performed to test the proportionality of hazard assumption. Patients were censored in the model upon: 1) Discontinuation of the index treatment regimen, 2) augmentation with a newer medication other than the index regimen, or 3) end of follow- up. SAS 9.3 was used for the entire analyses and p<0.05 was considered to be statistically significant.
Covariates included in the Cox model were patient demographics, comedications, and comorbidities that were measured at 2 months pre-index date. Comorbidities included previous manic episodes identified by diagnosis codes of mania, substance abuse disorder (SUD), attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), anxiety, adjustment disorder, and psychotic disorder at baseline. Comedications included stimulants, sedatives, hypnotics, anticholinergics, SGAs, or mood stabilizers at baseline. Uses of psychotherapy and hospital admissions at baseline were identified as measures of disease severity. Patient demographic characteristics included were age (categorized as children if <13 years of age and adolescent if ≥13 years of age), gender, race (white, black, or other) and state of residence (TX, NY, CA, or IL). Medicaid eligibility categories such as Temporary Assistance for Needy Families (TANF) and foster children were also identified, as these variables may indicate socioeconomic characteristics of patients. Duration of disease was computed as days between the first bipolar disorder diagnosis identified in the data and the index bipolar depression diagnosis date, as longer duration of disease may influence the future symptomatic outcomes, such as mood destabilization. Finally, number of physicians available in each zip code was measured to adjust for psychiatric care availability for patients.
Sensitivity analysis on unobserved confounding
The robustness of the conventional Cox proportional hazards model toward possible bias caused by unobserved confounders such as the responsiveness to previous treatment for bipolar disorders was tested using instrumental variable (IV) analysis. In this study, “physicians' preference,” “misdiagnosis of index bipolar depression as unipolar depression (ICD-9-CM code: 296.2, 296.3),” and “year of cohort entry” were identified as instruments. Among these IVs, the “physician prescribing preference” has been established as a valid instrument for explaining psychotropic treatment variation in the literature (Brookhart et al. 2006, 2007; Rassen et al. 2009).
Physician prescribing preference was operationalized as the treatment prescribed to the previous eligible patient of the same physician (Brookhart et al. 2006). According to this approach, if the last prescription written by a physician for a child with bipolar depression was for an antidepressant, then for the next patient the physician was classified as an “antidepressant prescriber.” Otherwise, that physician was classified as a “non-antidepressant prescriber.” Confirmed bipolar disorder patients (those with two consecutive bipolar disorder diagnoses) experiencing a depressive episode and given a major depressive disorder (unipolar depression) diagnosis instead of a bipolar depression diagnosis (ICD-9-CM: 296.5) suggested a misdiagnosis (Stensland et al. 2008). The year patients entered into the cohort, computed based on their index date, explains secular changes in Medicaid policy and formularies, which may predict treatment selection between antidepressant and its alternates.
Conceptually, physician's preference for a drug is a strong predictor for treatment selection. A prior history of treating bipolar depression with antidepressants over mood stabilizers or SGAs may predict future use of antidepressants by those physicians while treating subsequent patients. Similarly, misdiagnosing bipolar depression as major depression leads to a higher likelihood of prescribing antidepressants. The availability and coverage of medications at different years also predicts the utilization. However, these factors do not directly result in a manic switch or affect a patient's clinical profile or sociodemographic characteristics; hence, they cannot predict the risk of manic switch, except through its influence on the type of treatment administered.
Apart from these conceptual justifications, we also performed specification tests to validate the instruments. Strength of association between the instruments and the binary treatment variables were assessed by computing a partial F test and partial R2 (Rassen et al. 2009; Hadley et al. 2010). Change in observed covariate imbalance was determined by comparing the covariate distribution across the treatment groups and the instruments. Fractional change in distribution (Rassen et al. 2009) of each covariate between the treatment groups and the instruments was computed. Test to detect the presence of endogeneity was also performed by testing the statistical significance of the coefficient on the residual computed from the first stage and included in the second stage of the regression.
The IV analysis that was used in this study is called the “two-stage residual inclusion” (2SRI) estimation (Terza et al. 2008). In the first-stage model, binary continuous treatment variables were regressed on all the covariates and the instruments using a linear probability model (Humphreys et al. 2011). Residual (r) for each patient was computed as the difference between the binary treatment variable and the predicted treatment variable from the linear probability model.
In the second-stage model, time to manic switch associated with the treatment variables was assessed using a conventional Cox proportional hazards regression model adjusting for all the previously measured covariates and r computed from the first stage. The standard errors in the second stage were bootstrapped to avoid using the ones generated from the manual computation of the 2SRI. Association between the outcome and the treatment variable and all other covariates were reported as hazard ratios (HRs) with 95% CIs. Statistical insignificance of r in the second stage regression might be the result of the exogeneity of the treatment variable, thereby making the IV analysis unnecessary.
Sensitivity analysis on the duration of follow-up
Although 6 weeks is a commonly used follow-up period for assessing short-term manic switch, the medical community has not yet reached a consensus on the duration of follow-up. According to the nomenclature of the course and outcome of bipolar disorder defined by the International Society for Bipolar Disorders (ISBD) task force (Tohen et al. 2009), a manic event ≤8 weeks after treatment is a “definite” measure of manic switch, whereas one during the ≤12 week window is a “likely” or “possible.” To test the robustness of our findings toward the variations in the follow-up period, sensitivity analyses were conducted by extending the follow-up to 8 weeks and 12 weeks, respectively.
Results
As presented in Figure 1, 4147 children and adolescents with bipolar depression were identified after imposing all inclusion and exclusion criteria. Most of these patients were adolescents (≥13 years), white, and male. Approximately 25% of these patients were foster children. The most common comorbid conditions were ADHD, ODD, anxiety, and adjustment disorder, and common comedications were stimulants and sedatives. More than 50% of the monotherapy and polytherapy users received psychotherapy, and 16–30% had been hospitalized during the pre-index period. The average duration between the first bipolar disorder diagnosis presented in the data and the index bipolar depression was 300 days.
Of 4147 patients identified, 1796 received monotherapy and 2351 received polytherapy. These patients were further categorized as recipients of antidepressant monotherapy (n=179), SGA monotherapy (n=1047), mood stabilizer monotherapy (n=570), antidepressant–mood stabilizer or antidepressant–SGA polytherapy (n=445), or SGA–mood stabilizer polytherapy (n=1906).
Descriptive statistics
As presented in Tables 1 and 2, antidepressant (both monotherapy and polytherapy) recipients were older, more likely to be female, less likely to be foster children, and less likely to have comorbid ADHD or to receive stimulants than SGA and mood stabilizer recipients. During the 6 week follow-up period, the highest incidence of manic switch was observed in children and adolescents receiving SGA–mood stabilizer polytherapy (n=218, 11.44%), followed by mood stabilizer monotherapy (n=62, 10.88%), antidepressant monotherapy (n=17, 9.50%), SGA monotherapy (n=95, 9.07%) and antidepressant polytherapy (n=136, 8.09%). Using antidepressant monotherapy as the reference, log rank tests found that there were no statistically significant differences in the risk of manic switch between antidepressant monotherapy recipients and the recipients of all other regimens.
SGA, second-generation antipsychotic; ADHD, attention-deficit/hyperactivity disorder; TANF, Temporary Assistance for Needy Families.
SGA, second-generation antipsychotic; ADHD, attention-deficit/hyperactivity disorder; TANF, Temporary Assistance for Needy Families.
Multivariable Cox proportional hazards regression analysis
Tables 3 –5 present the findings of three traditional Cox proportional hazard analysis models that compared the risk of manic switch between antidepressant monotherapy and SGA monotherapy, antidepressant monotherapy and mood stabilizer monotherapy, and antidepressant polytherapy and SGA–mood stabilizer polytherapy after controlling for all observable confounders. Antidepressant monotherapy was associated with a higher risk of manic switch than SGA monotherapy (HR=2.87 [95% CI: 1.10–7.49]). However, similar results were not found when antidepressant monotherapy was compared with mood stabilizer monotherapy (HR=1.41 [95% CI: 0.52–3.80]), and when antidepressant polytherapy was compared with SGA–mood stabilizer polytherapy (HR=1.61 [95% CI: 0.90–2.89]).
Only statistically significant variables at p<0.05 are included in the table. Complete list of variables included in the models was as follows: demographics (age category, gender, race, state, number of physicians in the ZIP codes), proxy measurements of severity (duration of disease, prior hospitalization), Medicaid eligibility groups (foster care, Temporary Assistance to Needy Families), comorbidity (substance abuse disorder, attention-deficit/hyperactivity disorder, oppositional defiant disorder, anxiety, adjustment disorder, psychotic disorder, prior mania), comedications (stimulant, sedative, hypnotic, anticholinergic, psychotherapy, SGA, mood stabilizer).
Only statistically significant variables at p<0.05 are included in the table. Complete list of variables included in the models was as follows: demographics (age category, gender, race, state, number of physicians in the ZIP codes), proxy measurements of severity (duration of disease, prior hospitalization), Medicaid eligibility groups (foster care, Temporary Assistance to Needy Families), comorbidity (substance abuse disorder, attention-deficit/hyperactivity disorder, oppositional defiant disorder, anxiety, adjustment disorder, psychotic disorder, prior mania), comedications (stimulant, sedative, hypnotic, anticholinergic, psychotherapy, history of second generation antipsychotics, history of mood stabilizers).
Only statistically significant variables at p<0.05 are included in the table. Complete list of variables included in the models was as follows: demographics (age category, gender, race, state, number of physicians in the ZIP codes), proxy measurements of severity (duration of disease, prior hospitalization), Medicaid eligibility groups (foster care, Temporary Assistance to Needy Families), comorbidity (substance abuse disorder, attention-deficit/hyperactivity disorder, oppositional defiant disorder, anxiety, adjustment disorder, psychotic disorder, prior mania), comedications (stimulant, sedative, hypnotic, anticholinergic, psychotherapy, SGA, mood stabilizer).
SGA, second-generation antipsychotic.
Among all three models, a prior manic episode was a very strong predictor of short-term manic switch with an HR of 14.00 (95% CI: 8.99–21.78) for the comparison between antidepressant monotherapy and SGA monotherapy, 17.80 (95% CI: 10.29–30.81) for the comparison between antidepressant monotherapy and mood stabilizer monotherapy, and 10.96 (95% CI: 8.36–14.37) when antidepressant polytherapy was compared with SGA–mood stabilizer polytherapy.
IV analysis
Table 6 presents the statistical validation of instrumental variables. The F statistic for all three comparisons ranged from 149 to 285, and the partial R2 ranged from 0.27 to 0.40 which were well above the widely used rule of thumb (i.e., 10 for F statistic) indicated by Staiger and Stock (1997). These measures implied that the instrumental variables selected for the study were strong predictors of treatment selection.
SGA, second-generation antipsychotic.
Tables 3 –5 present the findings of IV analysis using 2SRI models. It was found that the residuals (r) generated from the first stage regressions were not statistically significant in the second stage model in all three comparisons, which might imply exogeneity of the treatment selection for bipolar depression.
Sensitivity analysis on duration of follow-up
As presented in Tables 3 –5, the associations between the treatment regimens and the risk of short-term manic switch remained consistent when the follow-up period was extended from 6 weeks to 8 and 12 weeks.
Discussion
Consistent with existing adult data (Yatham et al. 2005; Bond et al. 2008; Frye et al. 2009; Perlis et al. 2010), previous manic episode was identified in our study as the most important predictor (HR ranged from 11 to 18 for the three comparisons) for short-term manic switch in children and adolescents with bipolar depression. The finding is consistent with the general belief that polarity switch may be a part of the natural course of bipolar disorder itself. Irrespective of antidepressant treatment status, subjects who had had a manic episode prior to the treatment initiation were more likely to transition to a manic phase than were those without the previous episode. Consequently, previous manic history should be an important consideration in treatment decisions.
After adjusting for previous manic episode and other covariates, the Cox proportional hazard analysis suggested that antidepressant monotherapy was associated with increased risk of manic switch compared with SGA monotherapy (HR=2.63). The higher risk of manic switch associated with antidepressants versus SGA could be explained by the psychotropics' mechanism of action, as described in previous literature. Previous animal and genetic studies have explored the potential role of many neurotransmitters in manic switch, including serotonin, noradrenergic, dopamine, and catecholaminergic activity (Salvadore et al. 2010). The mechanism that helps to explain the different effects of antidepressants and SGA on manic switch is the effect of these medications on regulating synaptic plasticity and α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA) receptor trafficking in the hippocampus region of brain that is associated with SGA. The exposure to antidepressants (such as imipramine) known for triggering manic switch has been reported earlier to increase AMPA synaptic expression in the hippocampus (Du et al. 2003; Gray et al. 2003). Other research suggests that treatment of rodents with antipsychotics can reduce the expression of some AMPA receptor subunit mRNA and protein expression (Fitzgerald et al. 1995; Healy and Meador-Woodruff 1997; Fumagalli et al. 2008). Given the opposing effect of SGA and antidepressant drugs on the AMPA GluR1 receptor, AMPA receptor trafficking has been strongly suggested to play a key role in the mechanism of manic switching.
Existing research suggests that mood stabilizers such as lithium and valproate have similar effects as SGA on reducing glutamate AMPA receptor (GluR1) synaptic expression in the hippocampus (Du et al. 2004). However, statistically significant differences in the risk of manic switch were not observed when antidepressant monotherapy was compared with mood stabilizer monotherapy (HR=1.41 [95% CI: 0.52–3.80]) in our study. The finding could be explained by the slower and weaker antimanic effect of mood stabilizers compared with SGA (Delbello et al. 2006; Macmillan et al. 2008; Pavuluri et al. 2010; Geller et al. 2012), and also by the relatively small sample available for the comparison between MS and antidepressant monotherapy recipients.
Both mood stabilizers and SGA are recommended for acute and prophylactic treatment of the manic phase. Therefore, antimanic medications (mood stabilizers and SGA) are believed to treat or prevent an antidepressant-induced manic switch when antidepressant–SGA/mood stabilizer combination therapy is used. Literature suggests that concomitant therapy with a mood stabilizer may reduce antidepressant-induced manic switch (Ghaemi et al. 2003). Our analysis confirmed that the combination of antidepressant and SGA/mood stabilizer has a comparable risk of manic switch as SGA and mood stabilizer.
Our study is the first that assessed the risk of manic switch in children and adolescents with bipolar depression, and it is also the first head-to-head comparison study between antidepressant monotherapy and polytherapy and their alternatives. Given that making such comparisons in children using an experimental design is highly unlikely because of ethical concerns, an observational study such as this can provide valuable data for clinical practice.
Despite these advantages, existence of unobserved confounders is always a concern in observational studies, regardless of how refined the statistical methods and adjustment of the confounding factors are. Although particular patient characteristics were taken into account by adjusting for clinical and sociodemographic variables, geographic location, comorbidities, and past use of somatic and psychotropic medications, data on some potentially important confounding variables, such as responsiveness to the previous treatment, were unavailable. Literature suggests that responsiveness to previous psychopharmacotherapy is an important predictor of the risk of manic switch associated with an antidepressant (Salvadore et al. 2010). It is likely that there is a severity difference, and that patients who did not respond well to mood stabilizer and SGA were switched to antidepressants. To test the robustness of the conventional Cox proportional hazards model for possible unobserved confounding, the analysis was conducted again using an IV approach. The statistical insignificance of the residual r in the IV analysis probably implies that unobserved confounding was not a concern in the three models. Hence, the conventional Cox proportional hazards model used in the main analysis might provide sufficient statistical justification for the association between psychotropic treatment and the risk of manic switch.
Another concern about the studies of manic switch is the lack of agreement on the duration of follow-up (Salvadore et al. 2010). Ideally, in order for results to be comparable across studies, a single a priori definition of the time frame (e.g., 6 weeks) from the beginning of antidepressant treatment in patients experiencing a depressive episode, is required. Our present lack of consensus regarding temporal criteria may dilute the biological underpinnings of this phenomenon, because subjects who develop affective switch within very different time frames from the start of antidepressant treatments are considered equivalent. This methodological issue has been emphasized by a task force of the ISBD (Grunze 2008). To test the robustness of our findings against the different definitions of switching, and to understand the effect of possible misclassification, we conducted a sensitivity analysis by extending the follow-up period from 6 weeks to 8 and 12 weeks. The sensitivity analysis confirmed the higher risk of manic switch with antidepressant monotherapy versus SGA monotherapy.
In addition to the two main concerns that have been addressed in the sensitivity analysis, our study has other limitations because of the nature of claims data. For example, prescription claims for antidepressants, SGAs, and mood stabilizers were captured and deemed bipolar depression treatment without documented indications from physicians' notes. To ensure that those medications were prescribed to treat bipolar depression, other common indications for prescribing SGA or mood stabilizers (epilepsy, schizophrenia) were removed from the cohort, and a strict rule requiring initiation of the antidepressant within 30 days of depression diagnosis was also applied. Also, bipolar depression cases and manic switch events were identified based on ICD-9 diagnosis codes rather than structured clinical evaluation using depression and mania rating scales. To negate possible misclassification of bipolar cases, a strict algorithm was applied, and only patients who had had a minimum of three bipolar disorder diagnoses were included in the analysis. Manic switch associated with medication use is an emergent, one-time event that cannot be ascertained by repeated coding; therefore, misclassification of outcome caused by misdiagnosis or miscoding cannot be completely ruled out. However, there is no practical reason to believe that misclassification of disease in the claims data would have affected treatment groups differently and, therefore, it should not affect the study's conclusions.
Lastly, subcategories and individual drugs within the broad antidepressant class could have varying degrees of risk of manic switch. Tricyclic antidepressants (TCA) have been reported to have higher risk of manic switch than newer antidepressants, such as SSRIs (Salvadore et al. 2010). However, in our study cohort, ∼90% of children and adolescents in the antidepressant monotherapy group were on an SSRI antidepressant. It would be valuable, in future analysis, to further assess the relative risk between individual SSRI antidepressants in terms of manic switch.
Conclusions
In conclusion, antidepressant monotherapy was associated with an increase in the risk of short-term manic switch compared with SGA monotherapy. However, a similar association was not found between antidepressant monotherapy and mood stabilizer monotherapy, or between antidepressant polytherapy and SGA–mood stabilizer combination. Overall, the study findings support the current guidelines that antidepressant monotherapy should be always avoided, because of its potential for causing manic switch
Clinical Significance
Our study is the first that assessed the risk of manic switch in children and adolescents with bipolar depression, and it is also the first head-to-head comparison study between antidepressant monotherapy, and combinations and their alternatives. Given that making such comparisons in children using an experimental design is highly unlikely because of ethical concerns, observational studies such as this can provide valuable data for clinical practice.
Footnotes
Disclosures
No competing financial interests exist.