
Abstract
Objective:
In children and adolescents, the prevalence rate of mental illness is claimed to be as high as 10–20%. Effective pharmacological treatments are available for use in children, adolescents, and adults; however, most of what is known about the effects of these treatments has been confirmed in clinical studies involving adults only. Second generation antipsychotic drugs (SGAs) are the most common class of antipsychotic medication used in pediatric populations, and these drugs are increasingly being used for disorders other than psychosis. Many SGAs are routinely used in pediatric care, and the vast majority of use in this population is off label. Children, adolescents, and adults differ in age, weight, height, and metabolism, which may lead to pharmacokinetic differences in how drugs ultimately affect target tissues. The aim of this review is to summarize and evaluate the literature that investigated blood plasma levels of SGAs in youth.
Methods:
Plasma levels were assessed in relation to their administered dose, indication, and therapeutic range (if known). Studies were limited to those evaluating oral administration only. A systematic electronic database search for peer-reviewed articles published between 2000 and 2013 was conducted. Twenty-one articles were included in the review. Additional articles for discussion were also included throughout the article.
Results:
The only SGA that may require routine therapeutic drug monitoring (TDM) in youth given the current body of research is clozapine. Highly variable results were seen in studies of aripiprazole, olanzapine, and risperidone, indicating that more research is needed on plasma levels with these drugs. Quetiapine maintained a similar profile to that found in adults, with no dosage adjustments or indications of TDM.
Conclusion:
TDM may be indicated in any circumstance in which cytochrome P450 inhibitors or inducers are coprescribed. Further research is required for establishing a sounder safety profile for SGA use in the pediatric population.
Introduction
Second generation antipsychotics (SGAs) in youth
SGAs are currently used for a variety of psychiatric disorders in youth, including schizophrenia spectrum disorders, Tourette's Disorder, bipolar disorder, conduct disorder, attention-deficit/hyperactivity disorder (ADHD), eating disorders, disruptive behavior disorder (DBD), anxiety disorders, sleep disorders, and depression (Linton et al. 2013; Procyshyn et al. 2014). There has recently been a large increase in the use of SGAs in youth (≤18 years of age for the present review) (Patten, et al. 2012; Penfold et al. 2013). Currently, first-line treatment for psychotic disorders in youth is with SGAs (Datta et al. 2014). In many Western countries, only a minority of SGAs, such as risperidone and aripiprazole, are officially indicated for marketing in patients <18 years old (Harrison et al. 2012); furthermore, all SGAs that are used in youth have been predominantly studied in adults. This is not unique to antipsychotic drugs, as other classes of psychotherapeutic medications, such as antidepressants, are commonly prescribed to youth off-label (Czaja and Valuck 2012).
The most commonly recommended SGAs in pediatric populations in Canada are risperidone and quetiapine (Pringsheim et al. 2011). Other drugs used in this population include aripiprazole, clozapine, olanzapine, paliperidone, and ziprasidone (Pringsheim et al. 2011). It is a misconception that SGAs are “safer” than first generation antipsychotic drugs (FGAs) (De Hert et al. 2009). SGAs have a lower propensity for producing extrapyramidal symptoms (EPS) and tardive dyskinesia (TD). Many of the SGAs, however, may cause equally serious adverse events which include the well-known effects in adults on metabolic dysregulation (De Hert et al. 2011; Fredrikson et al. 2014; Tse et al. 2014).
A relative paucity of data exist on the use of SGAs in children (age 6–12) and adolescents (age 13–18) compared with use in adults (Vitiello et al. 2009), both with regard to efficacy and side effects. One particular area requiring further study is therapeutic drug level monitoring for antipsychotic drugs. A number of prior reports have studied the relationship between plasma concentrations of SGAs and clinical response in adults (Mauri et al. 2007). For example, studies in adults have shown that serum plasma levels of risperidone are significantly correlated with clinical response (Riedel et al. 2005). However, there is a lack of similarly published data for the pediatric population. Therapeutic drug levels can be key in controlling psychiatric symptoms, by helping to establish optimal dosing. Youth generally have smaller body masses than adults; therefore, modest fluctuations in plasma drug levels may have larger consequences in terms of side effects and therapeutic effects. Furthermore, youth have been reported to be more sensitive to some of the side effects of SGAs (De Hert et al. 2011). The purpose of this synopsis is, therefore, to systematically review the literature that spans the therapeutic monitoring of SGAs in blood plasma in youth. These plasma levels are evaluated in relation to their administered dose, psychiatric indication, therapeutic range (if known), and relevant pharmacokinetic parameters.
Mechanism of FGAs and SGAs
The principal pharmacological mechanism of action of FGAs is through the antagonism of synaptic dopamine at postsynaptic dopamine D2 receptors primarily located in the ventral striatum (Nord and Farde 2011). SGAs, in addition to blocking D2 receptors, also potently antagonize endogenous serotonin at 5-HT2A receptors. This is believed to modulate the release of dopamine in the four main dopamine pathways of the brain (Stahl 2003). The antagonism of 5-HT2A receptors is likely responsible for the decreased tendency of SGAs to induce the well-known motoric adverse effects, which include the EPS (dystonia, dyskinesias, akathisia, and Parkinsonism) and TD (Casey 2004). In addition, SGAs as a drug class are less likely to induce hyperprolactinemia (Caccia 2013) and neuroleptic malignant syndrome than are the FGAs (Horacek et al. 2006).Unfortunately, many SGAs are associated with significant metabolic side effects, including weight gain, hyperlipidemia, and insulin resistance, which can lead to the development of cardiometabolic diseases such as type 2 diabetes mellitus (Newcomer 2007) and cardiovascular disease (Leung et al. 2012). The individual SGAs vary notably in their propensity to cause specific side effects. For example, olanzapine and clozapine have the highest propensity to induce weight gain, whereas risperidone is more likely to increase prolactin levels (Vitiello et al. 2009). Studies have shown that side effects of antipsychotics may occur with greater severity and with higher frequency in children and adolescents than in adults (Winter et al. 2008), particularly when patients are first exposed to SGAs.
Developmental changes affecting pharmacokinetics in youth
A large number of important physiological developments occur between childhood and adulthood. These developmental changes may affect absorption, distribution, metabolism, and elimination of SGAs. Developmental changes that may affect drug absorption include changes in gastric emptying, intestinal transit time, intestinal pH changes, changes in intestinal transporters, and enzymes involved in first pass metabolism (Barrett et al. 2012). Changes that may affect drug distribution include changes in body fluid compartments and ratios of intracellular and extracellular fluid (Barrett et al. 2012). For example, total body water is 78% in neonates and only 55% in adults. Generally, children have a lower percentage of body fat than adults, and protein binding of drugs occurs to a lesser degree in infants than in children and adults (Barrett et al. 2012). Also, the blood–brain barrier may be more permeable in infants and children than in adults. There are various developmental changes in hepatic metabolism, reflecting factors such as the liver-size/body ratio (the liver size is greater in infants in relation to the rest of the body than in children and adults). Examples of biochemical metabolic differences include glucuronidation and sulfation, which are underdeveloped in infants (Barrett et al. 2012). Developmental changes that may affect the elimination of drugs include a decrease in glomerular filtration rate, which is at its lowest in neonates, and increases gradually through to adulthood. Absorption and secretion is higher in adults than in children and infants (Barrett et al. 2012).
Scope of the present review
A number of previous studies have examined plasma levels and clinical efficacy or side-effects of SGAs in adults (Lane et al. 1999; Spina et al. 2000; Riedel et al. 2005). To our knowledge, however, this is the only review that has summarized specifically therapeutic plasma levels of SGAs in the pediatric population. This review also highlights preclinical pharmacokinetic data that affect plasma levels of commonly used SGAs in youth. Clinical data and conclusions from each study are emphasized. Commonalities and inconsistencies in the research are included in the discussion as well as data synthesis, clinical implications, and directions for future research.
Methods
The articles used in the assembly of this review were obtained through a systematic electronic database search through Embase and MEDLINE® using the following key words:
Results
The results of the present review are compiled and presented for each individual SGA (see Table 1 for a summary). Synopses of study findings, relevant clinical and research implications, and relevant literature from other studies are included. A total of 21 articles met the inclusion criteria for this review (see Fig. 1).
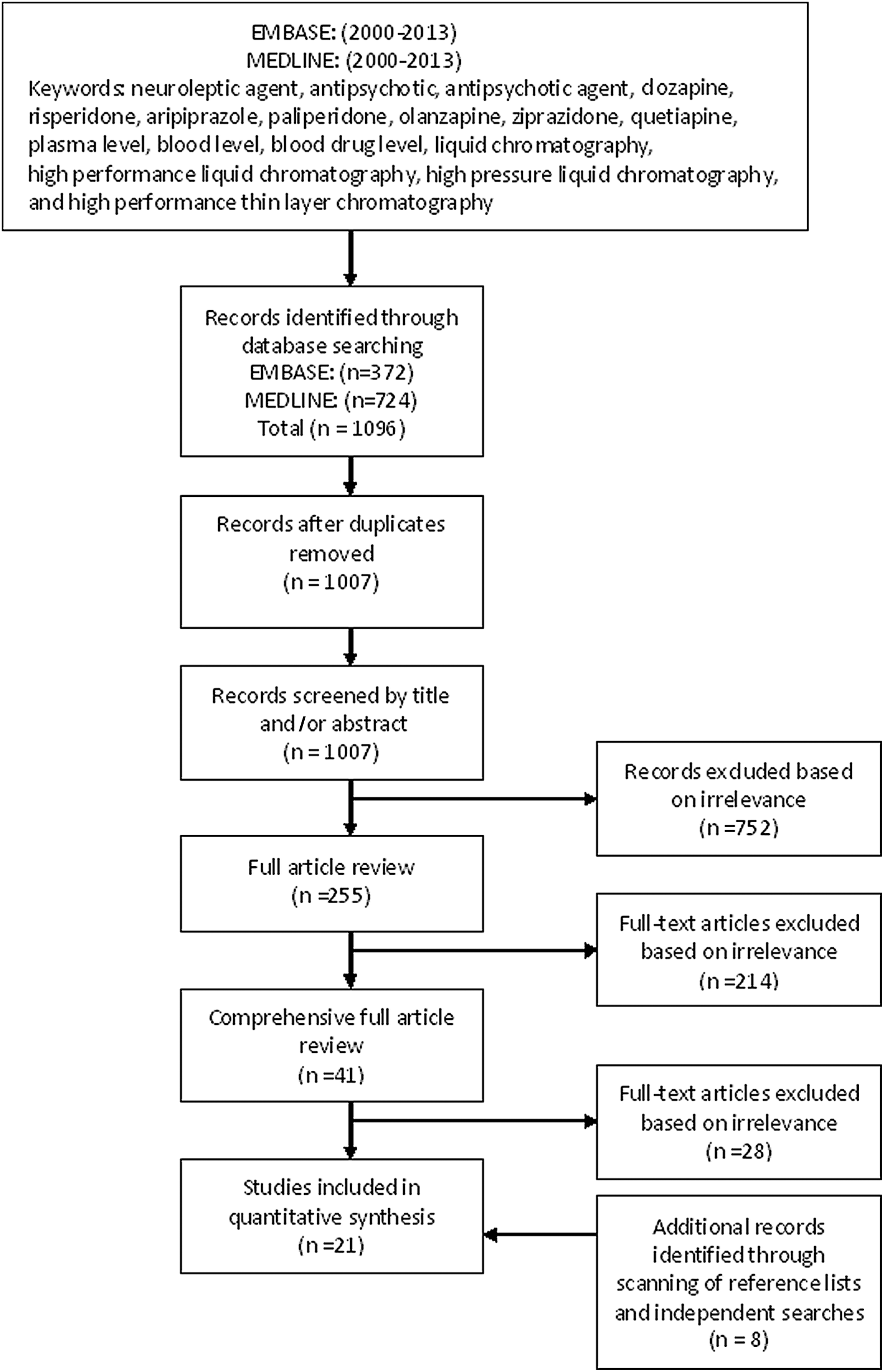
Literature review flow diagram representing the plasma level variability of second generation antipsychotics in youth.
AE, plasma levels correlated with adverse events; age (years), mean age (standard deviation) or range; AUC, area under the curve; AUC0-t, final measured concentration; BID, twice daily; Cmax; maximum plasma concentration; Cssmax, maximum plasma concentration at steady state, dose (milligrams [mg]), E, plasma levels correlated with clinical efficacy; weight, kilograms (kg) as mean (standard deviation) or range (if given); x, data not available.
Aripiprazole
The pharmacological mechanism of action of aripiprazole is somewhat different from all other SGAs in that it provides partial agonism at dopaminergic receptors. This partial agonistic effect decreases neuronal transmission in areas of hyperdopaminergic activity and increases neuronal transmission in areas of hypodopaminergic activity (Mailman and Murthy 2010). Aripiprazole has high affinity for the dopamine D2 and D3 receptors and moderate affinity for D4 receptors. Partial agonism occurs with the D2 receptors.
Published data investigating the pharmacokinetics of aripiprazole in children and adolescents are limited. Three articles to date have met the inclusion criteria for this review and were relevant to include in this review. In the first study of a pediatric population, Findling and colleagues conducted a study in 21 participants 10–17 years of age (Findling et al. 2008). In this study, participants were separated into three groups, receiving either 20, 25, or 30 mg daily doses. Overall, aripiprazole was found to be well tolerated, with a similar safety profile to that found in adults. One dystonic reaction occurring at fixed a dose of 25 mg was reported. The authors suggest that dose titration contributed to the low frequency of adverse events compared with previous work that used fixed dosing (Findling et al. 2003). Maximum plasma concentrations of aripiprazole at steady state (Css) were found to be higher in children and adolescents than was reported in a previous study in adults, with similar dosing (Mallikaarjun et al. 2004). In addition, time to reach maximum steady-state plasma concentrations (Tmax) values was less than had been previously reported in adults (Mallikaarjun et al. 2004). The authors hypothesize that the higher Cmax values seen in children and adolescents were the result of a lower body weight and, consequently, lower volume of distribution compared with adults.
In a separate study, Findling and colleagues investigated the tolerability and effectiveness of aripiprazole in 23 patients 6–17 years of age with a primary psychiatric diagnosis of conduct disorder (Findling et al. 2009). They found that steady state plasma levels were achieved following 14 days of once-daily aripiprazole therapy. Cmax and area under the curve (AUC) values were linearly proportional to administered oral doses. In a study of aripiprazole in adolescent patients with schizophrenia, Bachmann and colleagues found steady state serum concentrations of both aripiprazole and its metabolite dehydroaripiprazole, which correlated with the administered oral dose (Bachmann et al. 2008). This is consistent with the other studies in youth (Findling et al. 2008,\ 2009). No significant effects of age, sex, body mass index (BMI), or cigarette smoking were found on plasma levels of aripiprazole in this study. The effects of the following comedications were assessed: SGAs, anti-Parkinsonian agents, β-blockers, selective serotonin reuptake inhibitors (SSRIs), FGAs, and tranquilizers. No significant effects of comedications on serum plasma levels were noted. In patients in whom more than one blood sample was taken, intraindividual variability was assessed. They reported a 1–9.3 times intraindividual variability and 6.4 times interindividual variability for concentration to dose (C/D) ratios. For its metabolite, dehydroaripiprazole, a 1–8.6 times intraindividual variability and a 6.8 times interindividual variability were reported. Overall, the available literature on the effects of aripiprazole in the pediatric population describes a similar safety profile to that found in adults (Bachmann et al. 2008; Findling et al. 2008,\ 2009,). Although limited data exist, the current body of literature indicates similar plasma level variability in children and adults (Bachmann et al. 2008).
Clozapine
Clozapine was the first SGA to have been used widely (Crilly 2007). It has moderate-to-low affinity for D1 receptors and low affinity for D2 and D3 receptors, but high affinity for D4 receptors (Ashby and Wang 1996). Clozapine has been shown to possess high affinity for both 5-HT2A and 5-HT2C receptors, and moderate affinity for 5-HT3 receptors. Clozapine is unique among SGAs because it is known to be beneficial in patients with treatment-resistant schizophrenia, and for persistent psychotic symptoms for which other antipsychotic agents have proven ineffective (Meltzer 2013).
Three clozapine studies met the inclusion criteria for this review. The study by Couchman and colleagues was the largest and most comprehensive study investigating the plasma levels of clozapine in a pediatric population (Couchman et al. 2013). Data were collected from a therapeutic drug monitoring (TDM) service that included 1408 samples from 484 patients 8–17 years of age. In this study, retrospective TDM data were examined, and the relationship between plasma levels and dose, age, sex, weight, plasma clozapine:norclozapine metabolite ratio (MetR), and smoking habits were examined (based on the high incidence of smoking in patients treated with SGAs) (Barr et al. 2008). Median plasma levels increased with increasing dose up to age 13, but remained stable thereafter. Plasma drug levels were related to prescribed dose, with 66% of samples <0.35 mg/L at doses of 50–150 mg/dose, and 12% of samples <0.35 mg/L at doses of ≥650 mg. In 90 of the samples with a plasma level of ≥1.00 mg/L, the median dose range was 400 mg/dose. Plasma clozapine levels were found to be 34% higher in females than in males, and 41% higher in nonsmokers than in smokers. A 5% increase in plasma clozapine level was seen per 10 kg of body weight up to 80 kg. Lastly, as the MetR with norclozapine increased by 0.1 from 1.6 (mean value), a 6% increase in plasma clozapine level was observed. A 7% increase in plasma clozapine was observed between ages 16 and 17 years.
In the smaller study by Frazier et al. (2003), six inpatients (two male) 9–16 years of age (mean 13.7±[2.7]) with confirmed schizophrenia were studied (Frazier et al. 2003). Steady state serum concentrations were collected prior to and after the morning dose of clozapine. Dosing was similar to adult dosing of 3–4 mg/kg (Centorrino et al. 1994). Serum drug concentrations correlated with weight-adjusted doses of clozapine. A significant finding of this study was the high MetR of norclozapine to clozapine. This contrasts with an adult comparison study in which 10–25% higher clozapine to norclozapine ratios were reported (Perry et al. 1998). Correlations between serum levels and clinical improvement of symptoms as evaluated by Scale for the Assessment of Negative Symptoms (SANS) and Scale for the Assessment of Positive Symptoms (SAPS) rating scales were also reported. Furthermore, frequency of side effects observed also correlated with serum levels of clozapine and norclozapine. Strengths of this study include strict time serum level testing and the relatively small numbers of concomitant medications, although it was limited by the small number of subjects.
Lastly, Toepfner et al. (2013) described a case report of a 13-month-old female toddler who presented with symptoms of clozapine toxicity (Toepfner et al. 2013). This toddler had not been previously prescribed clozapine, and accidental ingestion was suspected. From this case, the authors concluded the elimination kinetics of clozapine to be similar in toddlers and adults. Furthermore, they suggest clinical monitoring after overdose even when serum concentrations are below the therapeutic range (200–400 ng/mL) recommended for school-age children.
Risperidone
Risperidone is currently one of the most commonly prescribed SGAs in children and adolescents. Similar to other SGAs, it occupies >80% of cortical 5-HT2A receptors and >70% of D2 receptors at therapeutic dosages (Miyamoto et al. 2005). Recently, Thyssen and colleagues reported differences in protein binding of risperidone and its metabolite between children and adolescents (Thyssen et al. 2010). However, plasma concentrations and elimination were found to be similar to that described in adults. Five articles that included the investigation of plasma levels of risperidone met the inclusion criteria, and are relevant to this review.
Aman and colleagues conducted a study of 19 patients 4–15 years of age, and compared the pharmacokinetic characteristics of plasma concentrations and their relationship to saliva concentrations (Aman et al. 2007). A large interindividual variability among concentration-time profiles was reported. The time to reach Cmax for both risperidone and its metabolites was found to be similar to that reported in adults (Heykants et al. 1994). In addition, the plasma half-life (t 1/2) was found to be slightly shorter than has been reported in adults (Heykants et al. 1994). The authors suggest that dosing four times daily could be performed for optimal risperidone administration in children, based on their findings. Their findings also indicate that the average Cmax concentration for the metabolite (+)-9-hydroxy-risperidone ([+]-9-OH-risperidone) was 2.8 times higher, and that the AUC was 2.5 times higher than that of (-)-9-OH-risperidone. One additional finding in this study worth noting is the presence of a poor metabolizer of risperidone as evidenced by CYP2D6 genotyping, concentration profile, and AUC. A person is a poor metabolizer if they have two inactive alleles or one inactive and one deficient allele (Mrazek 2010). This genotypic variation results in a lower metabolic capacity, which increases the risk of adverse events with comedications that share the CYP2D6 metabolic pathway. The authors emphasized the benefits of genotyping enzymes involved in metabolism to assist in the accuracy of dosing.
Calarge and Miller conducted a 6 month study in 107 youth 7–17 years of age who were being treated with risperidone (Calarge and Miller 2011). Plasma levels of risperidone and its active metabolites, along with other data, were collected. Interestingly, levels of risperidone were found to be undetectable in 40 of the participants, whereas metabolite levels were within the detection level of the assay. In their findings, males had higher plasma levels of risperidone than females. Comedication with sertraline, citalopram, and escitalopram were associated with lower plasma levels of risperidone. Duval and colleagues investigated the effects of risperidone on prolactin levels (Duval et al. 2008). They reported a dose-dependent relationship between risperidone treatment and elevated prolactin levels in youth.
Thyssen and colleagues conducted a study composed of nine clinical trials of oral risperidone (Thyssen et al. 2010). Of these nine trials, three were conducted in subjects <19 years of age. These authors reported a lower plasma protein binding of the active moiety of risperidone in adolescents (12–17 years of age) compared with children (6–12 years of age). They found that peak plasma concentrations and t1/2 were similar to those of adults. Overall, they concluded that risperidone had similar pharmacokinetic profiles in children, adolescents, and adults.
In a study by Aichhorn et al. (2007), the age and gender effects of olanzapine and risperidone were evaluated in children and adolescents (Aichhorn et al. 2007). Steady state plasma levels of two groups of patients one 10–18 years of age, and the other 19–45 years of age, were analyzed. The authors found that adolescents received ∼40% lower doses of risperidone and had lower total plasma levels risperidone in comparison with the adult group. Similar C/D ratios in both age groups were described. Females had significantly higher total plasma levels of risperidone than males, when receiving similar oral doses. Patients taking valproate had a 55% higher risperidone plasma level. The average dose of oral risperidone was 22% lower in adolescents than in adults. Plasma levels and C/D ratios were higher in female patients than in males in children, adolescent, and adult groups. The authors concluded that age is a major variable that affects plasma levels of olanzapine, but not those of risperidone. With regard to the gender variable in their study, they found higher risperidone plasma levels in adolescent females than in adolescent males, but this discrepancy was not observed in adults. Gender did not appear to have an effect on olanzapine plasma levels. The authors hypothesized that higher levels of risperidone were observed in female patients because of the effects of female sex hormomes on CYP3A4 metabolism. To summarize, Aichhorn and colleagues studied the age and gender differences as well as the differences between children and adults (Aichhorn et al. 2007). They reported similar C/D ratios in both children and adults. Although they reported no significant differences in plasma concentrations related to age specifically, they found that females exhibited significantly higher total plasma levels than males when receiving similar doses, and higher C/D ratios. These differences were not observed in adults.
Previously, Gagliano and colleagues undertook a study with 20 children diagnosed with autism according to Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria (American Psychiatric Association 1994; Gagliano et al. 2004). Total plasma levels (active fraction or the sum of risperidone level plus its [+]9-OH-risperidone metabolite in a sample) were measured at 12 weeks of risperidone treatment with values ranging from 8 to 55 ng/mL. The authors noted plasma concentrations to be higher in those who responded to the treatment than in those who did not, although results were not statistically significant. They concluded that no correlation among total plasma levels of risperidone, its active metabolite, and clinical response were found. Improvement was seen according to their evaluation criteria (Children's Psychiatric Rating Scale [CPRS]) over the course of risperidone treatment. In terms of adverse effects, they saw no correlation between prolactin level increase and plasma levels of total risperidone.
Quetiapine
Quetiapine is a commonly used SGA in children and adolescents. Similar pharmacokinetic properties have been described in children, adolescents, and adults (Winter et al. 2008). A study investigating pharmacokinetic differences of quetiapine in adolescent patients found similar profiles to those reported for adults, indicating that dose adjustments for adolescents are not required (McConville et al. 2000). The pharmacological mechanism of action of quetiapine is slightly different than for other SGAs. Quetiapine exhibits weaker antagonistic effects at dopamine D2 and serotonin 5-HT2 receptors, stronger antagonistic effects at α-1 receptors, and modest histaminergic effects (Nasrallah 2008). This combination of receptor antagonism is thought to be responsible for its therapeutic effects and low risk of EPS. Four articles were included in the review.
McConville and colleagues conducted a study of 10 youth 12–15 years of age taking varying doses of quetiapine, and observed dose-proportional pharmacokinetics (McConville et al. 2000). They described a similar pharmacokinetic profile for quetiapine to that observed in adults. Decreases in total and free T4 were found in subjects, but were not associated with clinical symptoms. No significant changes in prolactin levels were described in this study.
Findling and colleagues conducted an 8 week study of 17 youth 6–12 years of age with a diagnosis of conduct disorder, who were taking quetiapine (Findling et al. 2006). Plasma levels were obtained at weeks 2 and 8 of the study. Interestingly, the authors reported a correlation between plasma concentration and clinical response. Those with serum plasma levels >300 ng/mL were found to be responders using various assessment scales.
Gerlach et al. (2007) studied 21 adolescent patients 13–17 years of age taking quetiapine 100–800 mg/day (Gerlach et al. 2007). A weak correlation was observed between oral dose and serum plasma level, and no correlation was observed between plasma level and treatment response. Interestingly, plasma drug concentration in 42% of subjects were below the recommended level for adults (Baumann et al. 2004).
Winter and colleagues conducted a study in 28 children and adolescents 10–17 years of age and 29 adults18–45 years of age taking immediate-release quetiapine (Winter et al. 2008). Large variability of pharmacokinetic parameters within age groups, as well as a trend toward a higher steady state AUC and Cmax of norquetiapine and quetiapine sulfoxide were described in younger patients. This trend in norquetiapine and quetiapine sulfoxide was not observed when the exposure was adjusted by body weight. When adjusted by body weight, a lower steady state Cmax and AUC of quetiapine and 7-hydroxyquetiapine were reported. Overall, similar pharmacokinetics were described, with a recommendation that no dosage adjustment was required for pediatric patients treated with quetiapine.
Olanazpine
Like other SGAs, olanzapine produces antipsychotic effects through the antagonism of dopamine at D2 receptors and serotonin at 5-HT2A receptors (Kantrowitz and Citrome 2008). In addition, olanzapine also has antagonistic effects at 5HT-2C, 5HT3, 5HT6, D1-4, histamine H1, α1-adrenoreceptors, γ-aminobutyric acid (GABA)a, β-adrenoreceptors, and muscarinic M1-5 receptors (ibid). Olanzapine's effects at these other receptors have been hypothesized to be responsible for its adverse effects (Kantrowitz and Citrome 2008). Studies have indicated that olanzapine may be associated with significant pharmacokinetic interindividual variability because of induction and inhibition of its primary metabolizing enzyme CYP1A2. One study found that patients who smoked cigarettes cleared olanzapine 55% faster than nonsmokers, men cleared olanzapine 38% faster than women, and black patients cleared olanzapine 26% faster than other ethnicities (Bigos et al. 2008). Five studies investigating olanzapine met criteria for the current review.
Lobo et al. (2010) investigated the pharmacokinetics of oral olanzapine in pediatric patients with schizophrenia or bipolar disorder (Lobo et al. 2010). This study consisted of 106 patients 13–17 years of age given olanzapine 2.5–20 mg for a period of 4.5 weeks. Overall, they found similar pharmacokinetics to those previously described for adults. They also concluded that olanzapine dosage adjustments based on age, weight, or sex are not necessary, and that doses should be similar to those used in adults.
A study by Theisen and colleagues described a retrospective analysis using TDM data from 130 patients 10–21 years of age (mean:16.8) receiving oral olanzapine (Theisen et al. 2006). One hundred and twenty-two of the 130 patients enrolled in the study had more than one serum measurement, and were evaluated for intraindividual variability and other parameters including dose, metabolite concentrations, diagnoses, age, gender, smoking, gender and smoking combined, comedication, time of administration, and effects the parameters combined.
They reported a large interindividual variability of olanzapine that was observed predominantly in adolescents. Interindividual variability was also seen in plasma metabolite levels of N-desmethyl olanzapine (DMO) and 2-hydroxymethyl olanzapine (2-OH-OLZ). Male adolescents were found to have a lower olanzapine/DMO ratio and a higher percentage of metabolite than female adolescents. The authors hypothesize that male adolescents metabolize olanzapine through the CYP1A2 enzyme at a higher rate than female adolescents. The authors also infer that, according to their data, the DMO metabolite is likely formed to a lesser degree in adolescents than in adults. Consistent with other studies (Grothe et al. 2000; Bigos et al. 2008), lower olanzapine concentrations were seen in smokers than in nonsmokers, suggesting a higher rate of clearance. The study by Thiesen and colleagues also reported a trend toward higher olanzapine concentrations in females than in males, although this was not statistically significant (Theisen et al. 2006). Patients taking SSRIs or CYP inhibitors were found to have higher C/D ratios of olanzapine than with monotherapy. Patients taking carbamazepine were found to have significantly decreased levels of olanzapine; 86% of patients in this study were found to have olanzapine concentrations within the recommended therapeutic range for adults as described in a previous study (Ereshefsky 1996). Theisen and collegues concluded that, although individual variability of olanzapine plasma concentrations in pediatric patients was observed, they were of the same order of magnitude as that observed in adults.
Grothe et al. (2000) conducted a pharmacokinetic study of eight patients, 10–18 years of age receiving olanzapine 2.5–20 mg/day (Grothe et al. 2000). The average steady state olanzapine plasma concentration while receiving 20 mg per day was 92.6±27.0 ng/mL. Similar concentrations were found in both males and females. No participants in this study were cigarette smokers. Average steady state plasma olanzapine concentrations were found to be higher than previously reported in adults who smoke, and were similar to those previously reported in adult patients who did not smoke. Lower plasma clearance was found in adolescents compared with that described in adults (Patel et al. 1996).
Bachmann and colleagues conducted a study of 85 patients 10–20 years of age taking olanzapine (Bachmann et al. 2008). Plasma levels of olanzapine and its metabolites DMO and 2-OH-olanzapine were also assessed. Mean olanzapine serum concentration was determined to be 45.98 ng/mL (range: 1.86–110.89 ng/mL). The authors concluded that there was a large intraindividual variability in olanzapine concentration. They concluded that TDM could be warranted, and would be essential to obtaining targeted levels; however, repeated TDM measurements with each subject would be essential to account for intraindividual variability. The authors calculated the number of repeat measurements (>20) that would need to be taken from each patient in order to obtain an accurate individual range. Obtaining such a large number of measurements may be unrealistic for adolescents with a psychotic illness.
In the previously mentioned study by Aichhorn et al. (2007), the age and gender effects of olanzapine and risperidone were compared in four cohorts, two of youth 10–18 years of age and the other two of adults 19–45 years of age. Age-related effects were observed in patients taking olanzapine. It was concluded that further studies would be required to determine whether dosage adjustment of olanzapine should be implemented based on age. In this study, olanzapine plasma levels in adolescents were not significantly higher than those in adults. The average dose of olanzapine was found to be an average of 22.5% lower in adolescents, and 40% higher C/D ratios were found in adolescents when compared with adults. The authors concluded that age is a major variable that significantly affects olanzapine plasma concentrations. No effect of gender was seen on olanzapine plasma concentrations in this study.
Ziprasidone
Ziprasidone is a newer SGA that has pharmacological properties distinct from other SGAs. Ziprasidone is understood to have high affinity for 5-HT2A, 5-HT2C, 5-HT1A, 5-HT1B, and 1D receptors (Schmidt et al. 2001). Ziprasidone is also understood to possess a high affinity for D2 receptors (Stahl and Shayegan 2003). Only one article describing ziprasidone serum concentrations in youth met the inclusion criteria for this review. Sallee and colleagues conducted a study of 24 patients 7–26 years of age diagnosed with Tourette's syndrome or chronic tic disorder who were taking ziprasidone at a dosage of 0.2–0.3 mg/kg once daily (Sallee et al. 2003). Mean AUC plasma concentrations of ziprasidone ranged from 247 to 457 ng/mL. Ziprasidone Tmax occurred at 4 hours. Transient elevations of prolactin were reported and were similar to a comparison study of postmenopausal women (Muirhead et al. 2000). Overall, serum prolactin levels appear to be lower in this study of youth than in reports of other FGAs and SGAs (Markianos et al. 2001; Masi et al. 2001).
Discussion
Aripiprazole
Literature describing aripiprazole plasma levels and pharmacokinetics in a pediatric population was limited to two studies. The study by Findling et al. (2008) reported higher Css and Tmax in children than what had been previously reported in adults (Findling et al. 2008). However, Bachmann et al. (2008) found no differences in relation to age. A high degree of intraindividual variability of serum concentrations was described in Bachmann et al. (2008); however, this was similar to the variability seen in adult comparison studies (Mallikaarjun et al. 2004; Kirschbaum et al. 2005; Molden et al. 2006; Zuo et al. 2006). Because of the lack of published literature and variability of results, more research into the plasma concentrations of aripiprazole is needed to determine if TDM would be warranted in pediatric patients taking aripiprazole.
Clozapine
Based on the literature that met the inclusion criteria for this review, the pharmacokinetics of clozapine in children and adolescents are similar to those described in adults. Data on plasma levels and pharmacokinetics of clozapine in a pediatric population are limited to two small studies and one large study. Conclusions were, therefore, made based predominantly on the study by Couchman et al. (2013). Overall, plasma clozapine levels appear to be influenced by dose, cigarette smoking, plasma clozapine:norclozapine MetR, gender, age, and body weight similar to in adults. Based on the limited available data, TDM of clozapine in a pediatric population could be warranted (Couchman et al. 2013). This could be an important tool in achieving optimal response, while minimizing adverse effects. Furthermore, single nucleotide polymorphism (SNP) genotyping may also be a useful in identifying metabolic outliers in this population. Although limited to one study, Frazier et al. (2003) reported that clozapine and norclozapine plasma levels may be associated with both efficacy and adverse events in youth.
Risperidone
The literature on plasma levels of risperidone in youth was not consistent. Two studies reported similar differences in risperidone serum levels compared with adults (Aman et al. 2007; Thyssen et al. 2010). One study reported higher serum levels in females (Aichhorn et al. 2007), whereas another study reported higher serum levels in males (Calarge and Miller 2011). One study reported no correlation among clinical response, serum prolactin levels, and total plasma levels of risperidone (Gagliano et al. 2004). In contrast, the study by Duval et al. (2008) reported a dose-dependent relationship between serum prolactin and risperidone in youth. Gagliano et al. (2004) reported higher plasma levels in those who responded to treatment versus those who did not, although this was not statistically significant (Gagliano et al. 2004). Additionally, higher plasma concentrations were also found in patients taking concomitant CYP- inhibiting comedications (Aichhorn, et al. 2007; Calarge and Miller 2011). Interestingly, Aichhorn and colleagues reported higher plasma concentrations in females than in males with similar dosing (Aichhorn et al. 2007). Aman and colleagues described the presence of a patient who was a poor metabolizer of risperidone, with elevated plasma levels (Aman et al. 2007). This emphasizes the importance of genotyping in identifying outliers in order to ensure accuracy of dosing and, ultimately, patient safety. Based on available data, more research is required to determine if TDM of risperidone would be of benefit in a pediatric population. It is evident, however, that SNP genotyping may be a useful clinical tool to identify nonresponders such as the example given in Gagliano et al. (2004).
Quetiapine
Overall, the literature suggests a similar pharmacokinetic profile for quetiapine in children and adults (McConville, et al. 2000; Winter, et al. 2008). The two studies previously cited concluded that no dosage adjustment between pediatric patients and adults is required. Findling et al. (2006) reported that plasma levels of quetiapine were correlated with clinical response; however, these results were not seen in a similar study by Gerlach et al. (2007).
Olanzapine
Overall, the literature suggests that the pharmacokinetics of olanzapine are similar in children and adults, with no dosage adjustments required for pediatric patients. The literature surrounding the serum level variability appears to be inconsistent across studies. Gender does not appear to have a significant impact on serum olanzapine concentrations in a pediatric population. A study by Theisen and colleagues described a trend of higher olanzapine concentrations in females than in males (Theisen et al. 2006). The effects of comedication may alter olanzapine plasma levels, whereas the effects of age remain inconsistent across studies. Similarly to in adults, smoking habit appears to significantly affect olanzapine plasma concentrations in youth. Correlations between olanzapine plasma levels and clinical response were limited to one study only. Given that olanzapine appears to share a similar safety profile in children and adults, routine TDM may not be warranted. However, when changes in concomitant medications or smoking habit occur, olanzapine TDM may be rational.
Ziprasidone
Ziprasidone is among the newer antipsychotics that are understood to have improved metabolic adverse effect profiles compared with those of their predecessors. However, limited research into the efficacy of this medication in a pediatric population exists. Further research is needed to determine a sound safety profile for this medication in youth.
Conclusions
The general consensus regarding TDM for antipsychotics is that evidence has been too inconsistent to warrant TDM as a standard of care in all antipsychotic drug treatment; however, there are particular scenarios in which patients may benefit from its use (Baldessarini et al. 1988; Hiemke et al. 2004). Baumann et al. (2004) suggest that the inconsistent results among TDM studies may be a result of reviews consisting of studies with inadequate methodologies.
There is conflicting evidence in the literature correlating plasma levels of SGAs to adverse events and clinical efficacy (Remington et al. 2013). In the case of clozapine, TDM is recommended to maintain levels within established upper and lower therapeutic ranges and for safety (Remington et al. 2013). Therapeutic drug monitoring of clozapine has also been shown to be beneficial in terms of therapeutic response rates and limitation of side effects (Hiemke et al. 2004). Risperidone and olanzapine plasma levels have been shown to correlate with therapeutic response, whereas correlations between plasma levels of quetiapine and clinical effects have also been reported (Hiemke et al. 2004). A correlation between clinical effects and drug levels has been reported for olanzapine, and may be recommended in adults because of interindividual variability in drug levels (Patteet et al. 2012). For other SGAs, such as quetiapine and risperidone, the use of TDM is recommended if plasma concentrations above or below the therapeutic range are suspected (Patteet et al. 2012). This could include assessment of adherence, or identifying differences in metabolism.
Studies in adults have shown that plasma drug levels of antipsychotics correlate with dopamine receptor occupancy, and that the best therapeutic responses are seen with a 60–80% receptor occupancy (Farde, et al. 1992; Baumann et al. 2004). Furthermore, studies in animals have shown that plasma concentrations of olanzapine show stronger correlations with brain concentrations than with dosages (Hiemke et al. 2004).
At present, clozapine remains the only SGA that requires TDM as a standard of care. However, Hiemke et al. (2004) suggest that TDM of other SGAs would be warranted in cases in which the clinician wishes to assess medication adherence, or when the patient is experiencing adverse events at therapeutically recommended doses.
Research investigating the pharmacokinetics of SGAs in pediatric populations is limited. According to the Arbeitsgemeinschaft fur Neuropsychopharmakologie und Pharmakopsychiatrie (AGNP) - TDM Expert Group Consensus Guidelines (2004), TDM may also be helpful when pharmacokinetic data are lacking (Baumann et al. 2004). For the existing data, a high degree of variability in plasma concentrations of SGAs was observed in youth. Ongoing TDM may, therefore, be a useful tool for medications such as clozapine (Couchman et al. 2013), whereas for other SGAs, TDM is best justified when the above-described concerns are raised, there are changes in comedications, or there is a change in cigarette smoking status (Bachmann et al. 2008). Alternately, levels may be evaluated when the clinical presentation suggests that plasma levels may be outside therapeutic range. Increasing use of SGAs in pediatrics (Patten, et al. 2012; Penfold et al. 2013), combined with the limited available pharmacokinetic data, confirms that more research is urgently needed to develop a sound pharmacokinetic safety profile for SGAs in youth.
Clinical Significance
Although SGAs are routinely used in youth, there is a lack of knowledge concerning therapeutic blood plasma drug levels and their associated clinical response. The overall aim of this systematic review is to provide a summary of the literature on the relationship between plasma drug levels and their administered dose, psychiatric indication, therapeutic range, and pharmacokinetic parameters, to help establish optimal dosing in youth.
Disclosures
Dr. Procyshyn is a paid consultant for and is on the speaker's bureau of AstraZeneca, Bristol-Myers Squibb, Janssen, Otsuka, Pfizer, and Sunovion. Dr. Barr has received consulting fees or sat on paid advisory boards for Roche and Bristol-Myers Squibb. All other authors report no disclosures or conflicts of interest.