
Abstract
Objective:
The purpose of this study was to describe the patterns of psychotropic drug use in a large representative population of children and adolescents drawn from the French National Health Insurance databank.
Methods:
Data were drawn from a sample of 1% of the beneficiaries of the French national health insurance, selecting those 0–17 years old in 2010 (n=128,298). In addition to age and gender, data included the identification number of each drug allowing a European Pharmaceutical Marketing Research Association (EphMRA) classification, as well as the type of the prescriber.
Results:
Overall, 2.5% of children and adolescents had been prescribed psychotropic medication. A majority were prescribed anxiolytics (1.9%), followed by antidepressants (0.3%), antipsychotics (0.3%), and stimulants (0.2%). Between the ages of 15 and 17, 6.1% of girls were prescribed anxiolytics and 1.1% were prescribed antidepressants. For boys, the anxiolytics remained the most prescribed psychotropic medication; however, between the ages of 11 and 14, and between the ages of 15 and 17 they received more antipsychotics (0.7% and 0.8%) and between the ages of 6 and 10, and between the ages of 11 and 14 (0.7% and 0.6%), they were prescribed more stimulants than were girls. Among those who received a prescription, a majority of youth (84.6%) received only one class of drugs, and general practitioners were found to be prescribing most of these prescriptions (81.7%).
Conclusions:
The prevalence of psychotropic drug use in France is similar to that of the Netherlands and much lower than what is observed in the United States. Stimulants are less frequently prescribed in France than in other European countries, but anxiolytics are prescribed considerably more in France than in any other country.
Introduction
A
The increase in prescriptions for children and adolescents has been reported for most classes of drugs. For example, the use of antipsychotics has risen in all developed countries (Verdoux et al. 2010; Gyllenberg et al. 2012; Olfson 2012). Possible reasons include a greater use of the atypical antipsychotics for the treatment of behavioral disorders (Jensen et al. 2007; Domino and Swartz 2008) and the treatment of high-risk patients in an effort to prevent psychosis though this practice has been strongly criticized (McGorry et al. 2009). The use of antidepressants has also risen in the United States since the 1990s (Zito et al. 2002), whereas a slight decrease was observed in several other countries after the black box warning (Tournier et al. 2010). In the United States (Hunkeler et al. 2005) and the United Kingdom (Murray et al. 2004), this increase has been largely driven by the greater use of selective serotonin reuptake inhibitors (SSRIs). However, international comparisons indicate that although the overall use of antidepressants in the United States (1.63%) exceeded by at least threefold that of three Western European countries (prevalence ranging from 0.11% to 0.54%), there were major variations in the use of subclasses of antidepressants. Tricyclic antidepressants (TCAs) were predominant in Germany, whereas SSRIs prevailed in the United States, Denmark, and the Netherlands (Zito et al. 2006).
The rise of stimulant use in children is by far the most frequently reported increase (Zito et al. 2003). The use of methylphenidate decreased, whereas the use of extended-release amphetamine products increased (Habel et al. 2005). In the Netherlands, stimulant use increased as well, from 0.6% in 1998 to 1.2% in 2002 (Faber et al. 2005). This increase has been linked to a rise in attention-deficit/hyperactivity disorder (ADHD) and to improvements in its identification (Centers for Disease Control 2010). In addition, increased concomitant and multiple treatments have been reported (Mojtabai and Olfson 2010) together with the increased use of nonstimulants across diagnostic groups, such as antipsychotic treatment for nonpsychotic indications and antidepressants for ADHD or disruptive disorders (Zito and Safer 2005).
A review of 15 studies published between 1994 to 2002 revealed a very large range of overall yearly prevalence of use of any psychotropic drug in children and adolescent populations (0 to 17 or 18) ranging from 0.3% in Italy to 6.2% in the United States and 2.3% in the Netherlands (Bonati and Clavenna 2005). In France, four studies have evaluated psychotropic drug consumption in youth (Lecadet et al. 2003; Schick et al. 2004; Sevilla-Dedieu and Kovess-Masfety 2008; Acquaviva et al. 2009). These studies have shown that psychotropic medication was prescribed to 2–4.2% of children or adolescents within a year. Anxiolytics and hypnotics were mostly used, whereas stimulants were rare (rate of 0.02–0.1%). Contemporary increases in other countries underscore the need for more recent national French data on psychotropic drug use in children and adolescents.
The objectives of the present study are to examine a large nationally representative sample of children and adolescents ages 0–17 to describe: 1) The use of subclasses of psychotropic medication, 2) the number of prescriptions and multiclass prescriptions, and 3) the types of prescribers.
Methods
Sample
Data were drawn from a random sample of one out of every 97 beneficiaries affiliated with the French National Health Insurance (Caisse Nationale d'Assurance Maladie [CNAM]) who were ≤18 years old in 2010 (Echantillon Géneral des Bénéficiaires [EGB], n=128,298). All French residents are covered under the statutory health insurance plan, which is managed by different organizations depending upon the person's professional status. The salaried workers are affiliated with CNAM, which constitutes our sample and represents 76% of the overall population. (The other organizations are the Régime Social des Indépendants [RSI] for independent workers [5%]; the Mutualité Sociale Agricole [MSA] for farm workers [5%]; the Mutuelle Générale de l'Education Nationale [MGEN] for teachers [5%]; and special organizations such as the national railway employees or the Parisian suburban metro system, mineworkers, lawyers, sailors, the armed forces, and other special professions [9%]).
Children and adolescents <18 years of age are affiliated with their parents' insurance plan. Each prescription issued by a physician and dispensed by a pharmacy is coded and entered into a database linked to the beneficiary's identity. The present study was approved by the local ethical committee (Institut des Données de Santé), which is responsible for the access to the EGB data for researchers in France (Authorization No. 57 obtained on March 19, 2013).
Data collected
Sociodemographic information
Sociodemographic data included date of birth, gender, coverage status regarding both statutory and complementary health insurance including the relevant start and end dates of the coverage, geographical location, and an indicator of poverty (Couverture Maladie Universelle [CMU] available for those with less than a certain level of household income.)
Psychotropic medication
The data included all reimbursement claims for medication prescribed between January 1, 2010 and December 31, 2010. Specifically, data were collected for each reimbursement associated with a prescription. This included the CIP13 code for each drug, which is a 13 characters code that identifies each pharmaceutical product distributed in France (CIP), the name of the drug, the dosage and formulation packaging, the region in which the claim was made, the prescription date, and the type of professional who prescribed it. Only 3% of data regarding the prescribers were missing. Other medical specialties (such as cardiologists, endocrinologists, ophthalmologists) were included in the pediatrician category, as they represent only a small portion (2.6%) of the prescribers of psychotropic medication.
Therapeutic classes
The European Pharmaceutical Marketing Research Association (EphMRA) developed a classification that aggregates drugs into classes based on their anatomical site of action, main indication, therapeutic use, and composition. In the present study, five therapeutic classes were selected on the basis of the EphMRA classification: Antipsychotics (N05A) (e.g., risperidone), hypnotics (N05B), anxiolytics (N05C) (e.g., hydroxine dichlorhydrate), antidepressants (N06A) (e.g., amitriptyline), and stimulants (N06B) (e.g., methylphenidate). Only non-herbal drugs were included in the analyses, as herbal drugs are no longer reimbursed in France (since 2006).
Data analysis
The analyses were conducted using two approaches. First, a person-based approach was used to characterize the prevalence of psychotropic medication use and the number of claims per user. Second, a claim-based approach was used to describe the use of psychotropic drugs according to gender, age, therapeutic class, co-prescription patterns, and the medical specialty of the prescribing physician. Chi-square tests (χ2) were used to examine differences between ratios. Statistical significance was set at 0.05. SAS Enterprise guide 4.3 was used to perform all analyses.
Results
Sample description
A total of 128,298 children and adolescents between birth and age 17, affiliated with the CNAM, were included in the sample. Boys represented 51.4%, and there was no significant difference in gender distribution among the four age groups (χ2=3.9, df=4, p=0.42) (Table 1).
χ2=3.9; df=4; p=0,42 (Pearson's chi-squared tests)
One-year prevalence rates of psychotropic drug consumption
Prevalence rates are presented in Figure 1. Overall, a total of 3241 children and adolescents were associated with at least 1 of the 9571 reimbursement claims, with a prevalence rate of 2.50% (CI=2.41%; 2.59%). The majority of medications were prescribed to adolescents between 15 and 17 years of age (5.50%; CI=5.17%; 5.83%), a rate that was much higher than what was observed in younger age groups (χ2=844, df=4, p<0.001). The use of anxiolytics or hypnotics (respectively 1.92% and 0.08%) was the most prevalent (2.00%; CI=1.92%; 2.08%), followed by antidepressants or normothymics (0.3%; CI=0.27%; 0.33%), both culminating between the ages of 15 and 17 (4.90%, CI=4.59%, 5.21%, χ2=965, df=4, p<0.001; and 0.80%, CI=0.67%, 0.93%, χ2=245, df=4, p<0.001).
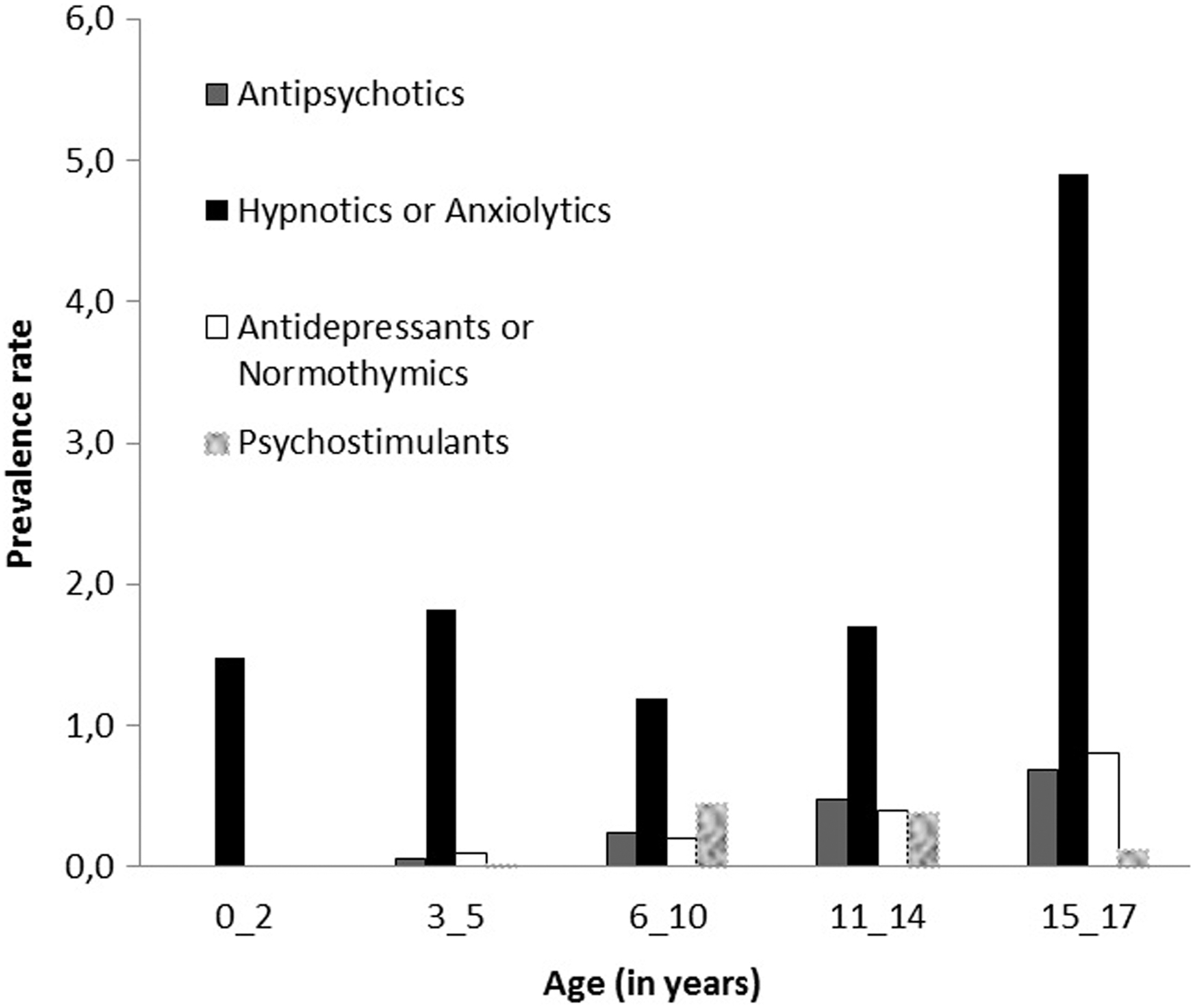
Prevalence rates of psychotropic medication by therapeutic class and by age in 2010.
In third place were antipsychotics (0.30%; CI=0.27%; 0.33%) also culminating in the 15–17-year-old group (0.70%; CI=0.58%; 0.82%; χ2=253; df=4; p<0.001), followed by stimulants (0.20%; CI=0.18%; 0.22%) more frequent in the 6–10-year-old group (0.40%; CI=0.34%; 0.46%; χ2=208; df=4, p<0.001).
The overall usage was largely driven by the anxiolytic/hypnotic category for each age group. Use started at 1.5% for the 0–2-year-olds, 1.8% for the 3–5-year-olds, then decreased at 1.2% for the 6–10-year-olds, and 1.7% for the 11–14-year-olds, and finally culminated at 4.9% for the 15–17-year-olds (6.6% for girls and 3.3% for boys). The three most frequent anxiolytic drugs were: Hydroxyzine (Atarax® Syrup 0.2 g/100 mL), hydroxyzine (Atarax Tab 25 mg), and etifoxine (Stresam® Cap 50 mg) overall, and hydroxyzine (Atarax Syrup 0.2 g/100 mL), diazepam (Valium® Inj 10 mg/2mL), and diazepam (Valium Oral Solution 10 mg/mL) in the 0–2-year-old group. The three most frequent drugs, respectively, accounted for 60% and 96% of the reimbursements in the overall population and in the 0–2-year-old age group.
Overall, boys and girls had similar prescriptions rates (2.5%; CI=2.38%, 2.62%; and 2.6%; CI=2.48%, 2.72%). However, significant gender differences were observed with regard to therapeutic classes (χ2=209, df=3, p<0.001). Boys were prescribed more antipsychotics (0.4%, CI=0.35%, 0.45%) and stimulants (0.4%; CI=0.35%, 0.45%) than were girls (0.2%; CI=0.16%, 0.24%; and 0.1%; CI=0.08%, 0.12%). Conversely, girls received more hypnotics and anxiolytics (2.3%; CI=2.18%, 2.42%) than did boys (1.8%; CI=1.70%; 1.90%).
When all age groups were compared, significant differences were observed for all therapeutic classes (χ2=542, df=12, p<0.001). Antipsychotics and antidepressants were rarely prescribed to children <6 years of age. Hypnotics or anxiolytics were prescribed to all age groups, although the 15–17-year-olds were clearly more likely to receive a prescription for either of them than were younger children. Stimulants were rarely prescribed to children <6 years of age, and few were prescribed to adolescents ≥age 15 (Table 2).
Multiclass psychotropic treatment
Out of the 3241 children and adolescents who were associated with at least one reimbursement claim for psychotropic medication, 2908 (89.7%) received only one therapeutic class of drugs. The most frequent association of psychotropic drugs was the prescription of antipsychotics with hypnotics or anxiolytics (30.4%). Antidepressants were prescribed mostly with antipsychotics (12.8%). Stimulants were mostly prescribed with antipsychotics (7.5%).
Number of claims per psychotropic medication user
Of the 3241 youth to whom a psychotropic medication was prescribed, 2100 (64.8%) had a single claim. However, this pattern was seen mainly for anxiolytics, for which single prescriptions represented 77.5% of all prescriptions. Conversely, single prescriptions for stimulants were rare (9%). Unexpectedly, half of the antidepressants and 27.6% of the antipsychotics were prescribed only once. When considering the average number of prescriptions in the prior 12 months, stimulants were the most frequent (7.5 prescriptions) followed closely by antipsychotics (6.2 prescriptions). Anxiolytics were prescribed an average of 1.6 times and antidepressants were prescribed an average of 2.9 times (Table 3).
All results are in percentages.
Mean number of prescriptions per patient.
Prescribers of psychotropic medication
Prescribers were examined based on the claims rather than on the beneficiaries, as any patient could have multiple prescribers. In each therapeutic class, a similar pattern was found, with the great majority of psychotropic drug prescriptions being written by general practitioners (GPs) (80.1%), regardless of the patient's age. However, two exceptions were noted. First, among antipsychotic prescriptions in 3–5-year-olds (n=39 claims), 50% were prescribed by psychiatrists and neurologists, and the other 50% by GPs. Second, among antidepressant or normothymic prescriptions, in 3–5-year-olds (n=38 claims), 50% were prescribed by GPs, 10.5% by pediatricians, and 39.5% by psychiatrists or neurologists.
The results showed that there were no prescriptions from pediatricians of antipsychotics or stimulants for children <5 years old or of antidepressants for children <2 years old. The most prescribed drugs by psychiatrists and neurologists were antipsychotics for the 3–5-year-olds (50%), whereas pediatricians prescribed hypnotics and anxiolytics to children <2 (15.7%). The types of prescribers were significantly different among all the age groups (χ2=268, df=8, p<0.001).
With regard to gender, the types of prescribers were significantly different between boys and girls (χ2=12, df=2, p=0.002). Pediatricians and psychiatrists or neurologists prescribed more to boys than to girls, and GPs prescribed more to girls than to boys (Table 4).
The total percentage is not equal to 100% for each of the therapeutic classes, because a few data about the prescribers were missing.
GP, general practitioner, Ped, pediatrician (and other medical specialties), MPH, mental health professional (Psychiatrist or neurologist).
Discussion
In 2000, the annual prevalence of prescriptions of any psychotropic medication in youth was significantly greater in the United States reported sample 1 (6.7%) than in the Netherlands (2.9%) or in Germany (2.0%) (Zito et al. 2008). In comparison, the present study shows that rates of psychotropic drug prescription in France 10 years later (2.5%) are closer to what was reported in the Netherlands or Germany, and reflect a much lower rate of prescription than what was documented in the United States. However, 18-year-olds were included in the data reported by the United States, the Netherlands, and Germany whereas they were not in the present data set. Nevertheless, the present rates are much higher than what was reported in Italy (0.03%) (Clavenna et al. 2007), although the latter study included reimbursed drugs in 2004 in a country where stimulants were not on the market and anxiolytics were not included in the analyses.
Stimulants
Stimulants are the most country-driven psychotropic drugs used. The United States has the highest rate (4.3%) followed by the Iceland (2.8% in 2007), the Netherlands (1.2%), and Germany (0.7%) (Zito et al. 2008; Zoega et al. 2009). Stimulant use in France is significantly lower, with a rate of 0.2%. Because rates decrease as age progresses, the exclusion of 18-year-olds in the French database may suggest that the observed difference is in fact even greater. This gradient of stimulant use across different countries is observed in all age groups, even though rates decrease dramatically after age 15 in all countries.
Although the rates are very low in the present study, they have doubled when compared with previous French studies (Sevilla-Dedieu and Kovess-Masfety 2008; Acquaviva et al. 2009). Such an increase has also been documented in recent years in other countries such as Iceland (Zoega et al. 2009), Denmark (Steinhausen and Bisgaard 2014), the United Kingdom (Hsia and Maclennan 2009), and the United States (Zito et al. 2003; Habel et al. 2005). Several hypotheses have been formulated to account for the overall increase in stimulant use, such as a larger pool of eligible youth because of the expanded diagnostic criteria for ADHD since 1980, more girls being treated for ADHD, a greater acceptance of biological treatments for behavioral disorders, and the expanded role of school and preschool health personnel in identifying mental health needs. Interestingly, France and the United Kingdom, the countries with the lowest rates, have policies that restrict the initial prescription of stimulants to specialists such as child psychiatrists.
Anxiolytics and hypnotics
By far, the largest difference between France and other countries are found in the anxiolytic prescription rates, which are substantially higher in France (1.92%), whereas the rates for the prescription of hypnotics are similar or lower (0.08%). Furthermore, French rates for anxiolytic prescriptions are marked by strong gender differences, 1.7% in boys and 2.1% in girls, a trend similar to what is reported in other European countries. Surprisingly, the United States has lower rates for anxiolytics (0.49%) and hypnotics (0.16%), with no reported gender differences (Zito et al. 2008). The French rates are high in all age groups, including 0–2-year-olds. In this age group, only two drugs are responsible for 96% of the prescriptions.
One possibility is that country-specific patterns of attitudes toward “natural” drugs and reimbursement policies drive the observed differences. France no longer reimburses herbal drugs and the present study did not include herbal products. However, previous studies have shown that one third of the psychotropic drugs were herbal (Sevilla-Dedieu and Kovess-Masfety 2008), which is similar to reports from Germany (Koelch et al. 2009), indicating that hypnotics/sedatives were mostly Valerian-based and prescribed for use during short periods of time. Nonetheless, it is very likely that in France, where any prescribed drug will be reimbursed in full, and where access to physicians is free of charge, most of the drugs aimed at calming children or adolescents will be medically prescribed rather than being acquired and purchased over the counter. Consequently, most, if not all of these drug purchases would be registered in health insurance data banks, whereas in other countries, these drugs might not appear on insurance data banks because of poorer reimbursement policies. This may result in the drug-driven effect that has been described for other drugs: By reimbursing medically prescribed drugs and not herbal compounds, the consumption shifts toward stronger drugs for an identical mental health problem.
To test this hypothesis, we analyzed another set of data drawn from a stratified sample of 13% of all French community pharmacies (Celtipharm [
It has also been argued that some anxiolytics may have been used for nonpsychiatric reasons. However, a previous study (Schick et al. 2004) estimated the potential neurological portion of prescriptions to be 30%, which brings to 1.4% the rate of psychotropic drug prescribing for those <15 years of age, and certainly could not account for such large differences with other countries (Schick et al. 2004).
Antidepressants and lithium
A similar country-specific pattern similar was found with antidepressants and mood stabilizers; a higher prevalence in the United States (2.71% for antidepressants and 0.15% for lithium) than in European countries (Netherlands 0.53% and 0.01%, respectively, Germany 0.17% and 0%, respectively, and France 0.3% overall) (Zito et al. 2008). The difference between the United States and European countries is observed in age groups 5–9, 10–14, and 15–17, whereas prescription rates among the youngest children (<4 years of age) are low in all countries (0–0.10%). Gender differences were found only in European countries, and only in the highest age group, with girls being treated more frequently.
Antipsychotics
Antipsychotics are rarely prescribed to children in any country. Rates range from 0.76% in the United States, 0.51% in the Netherlands, and 0.34% in Germany, which is similar to what was found in France (0.3%, without the 18 and 19-year-olds) (Zito et al. 2008). In Italy, the rate is even lower (0.07%) (Clavenna et al. 2007). Prescription rates for antipsychotics are very low for the youngest age group, except in Germany (0.64%), a quite unexpected result, as noted by the authors, which warrants further investigation. In the United States and the Netherlands, there is a strong gender difference, with higher rates for boys; the same pattern is present in France and in Germany for certain categories of antipsychotics, only and to a lesser extent.
Multiprescription and number of prescriptions within the previous year
Multiprescription has been recently brought up as a major trend in the United States (Martin et al. 2002; Comer et al. 2010) where as much as 20% of the children are prescribed at least two classes of psychotropic drugs; this percentage reaching up to 32.2% for children with a diagnosed psychiatric condition. This pattern has been observed more frequently in children receiving Medicaid than in the privately insured. Multiprescription is raising serious concerns, because little is known about the safety and efficacy of the involvement of two or more psychotropic drugs in children. This phenomenon seems less frequent in Europe, with an estimated 10.3% in the present study, 8.5% in the Netherlands, and 5.9% in Germany (Zito et al. 2008). In the United States, the leading pair was stimulants and antidepressants, whereas in the Netherlands and in Germany it was stimulants and antipsychotics. In France, the leading pair is a very different combination, with co-occurring prescriptions of antipsychotics and anxiolytics. Given the fact that stimulants are so rarely prescribed, the probability of having them co-prescribed was very low.
In the present data, children who received a stimulant prescription received on average 7.5 prescriptions during the year, a number very similar to that reported by Stevens et al. in the United States (Stevens et al. 2005), and much higher than the number reported in California alone: Two prescriptions on average, with 24% of children receiving only one prescription (Habel et al. 2005). Because the present data allowed us to examine 1 year patterns only, we could not determine whether the French patterns were similar to patterns reported in the Netherlands, where the data are provided for a 3-year time frame (Faber et al. 2005).
Prescribers
In the present study, most of the medications were prescribed by GPs or pediatricians (∼75–80%). These results are consistent with previous French studies (Schick et al. 2004). Prescriptions by child psychiatrists were much lower than in the United States, and similar to the European trend.
The type of prescriber is known to influence prescription patterns for any given mental health problem (Radigan et al. 2005). In France, 81.1% of stimulants are prescribed by GPs. In Europe, prescriptions are mostly written by GPs, although some restrictions exist, as in France or the United Kingdom, where treatment has to be initiated by a specialist, and these are restrictions that could influence prescription patterns. The observed differences have been linked to the rates of child psychiatrists being higher in the United States (10/1000) than in France (8/100,000) or other European countries, such as Germany or the Netherlands. In addition, important cultural differences exist regarding this medical profession. In the United States, an individualistic and proactive therapeutic mentality is more frequent than in Europe, especially in France, where child psychiatrists often work on a salary basis in government-funded institutions.
Limitations
Several limitations merit attention regarding the present study. First, the sample does not cover the entire French population, as the sample is missing certain occupational categories such as teachers, independent workers, agricultural workers, and their beneficiaries, representing a total of 24% of the population. It is a possibility that these groups have different psychotropic drug use patterns. Second, in an estimated 15% of youth, the link between the child and the child's parents could not be ascertained, because changes such as divorce or changes in names were not registered properly. Third, psychotropic drug use was estimated based on drugs that were retrieved from pharmacies, and, therefore, did not take into account medication that may have been provided during a hospital stay. However, children are very rarely hospitalized for mental health problems, and if they are provided medication during a hospital stay, they would typically be given a follow-up prescription at discharge, which would be retrieved from a pharmacy and would subsequently appear in the present database. A fourth limitation is related to the age of the children in the present sample (ages of 0–17 years). Other studies may report on a different age range to include youth as old as 19 or 20. Considering that psychotropic drug use increases with age for some classes of drugs, a 1 year difference may represent an important difference.
In addition, the present study did not include herbal drugs, although these drugs represent one third of psychotropic drug use in France (Sevilla-Dedieu and Kovess-Masfety 2008). Furthermore, a prescription for psychotropic medication does not necessarily mean that a child is taking the prescribed medication, nor does it imply that the child has a diagnosed psychiatric disorder. Finally, most of the available studies have focused on the 1990s and 2000s, whereas more recent data are rare, limiting our comparisons, considering the recent increase documented. Furthermore, comparisons are complicated by the diversity of the data used for analysis. Whereas some studies have relied on health insurance claims data, others have examined GP surveys, which are known to yield different results.
In addition to the United States comparisons, it should be kept in mind that there is no single national health insurance coverage, and, therefore, that United States inclusive national data are lacking. Any reported United States comparisons are based on authors' available data banks, usually from diverse Medicaid state organization and health maintenance organizations (HMOs), which may differ from state to state and not be representative of the “national” United States situation. Therefore, caution is needed when making comparisons.
Conclusions
Psychotropic drugs are prescribed to children and adolescents in France as in other European countries and the United States, although there are insufficient data on their long-term effects, and many of these drugs have not been properly tested or labeled for use in children. Prescription patterns are strikingly different between the United States and Europe and within Europe. In France, anxiolytics are the most prescribed class of psychotropic drugs in children as in adults, and a considerably larger number of children use anxiolytics in France than in any other country, for which data are available. Conversely, stimulants are rarely prescribed to children in France compared with in other countries, especially when the more recent data are examined.
GPs and pediatricians are the main prescribers of psychotropic drugs, even psychostimulants, despite regulations regarding the involvement of a mental health specialist. GPs and pediatricians do not rely on available classifications to obtain diagnoses and prescribe to treat symptoms, in most cases anxiety and agitation. Paradoxically, stimulants are rarely prescribed, and are feared for their side effects, although this is not the case for anxiolytics. As a result, children who may benefit from stimulants are not being prescribed these medications, and too many children are being prescribed anxiolytics despite their uncertain effects and safety. Furthermore, most of these anxiolytics could be replaced with nonpharmacological approaches if, for example, psychologists were to be reimbursed or if the often-criticized long school hours in place in France were to be reduced. Finally, psychotropic drug prescription in France should be carefully monitored in children and adolescents, as it relies on GPs and pediatricians whose initial training in child psychiatry may not be adequate, which makes a case for their continuing education regarding psychiatric disorders in children, and whose relationships with specialized mental health providers is often problematic (Kovess-Masfety et al. 2007).
Clinical Significance
Use of psychotropic medication in children is high in France.
French GPs and pediatricians have to be trained to better use anxiolytics in children and adolescents, and warned against their side and long-term effects.
On the other hand, practitioners in contact with children should better use Diagnostic and Statistical Manual of Mental Disorders (DSM) classifications in their precise definitions, in order to prescribe psychostimulants for those who qualify for this diagnostically, after having tried nonpharmacological approaches such as adaptation of study hours, a better balanced day program with some physical exercise, or psychotherapy if needed.
Because France may not be unique in this situation, these recommendations may extend to other European countries as well as outside Europe.
Disclosures
No competing financial interests exist.