
Abstract
Objective:
In most Eastern and Central European countries, except Germany, there is a lack of drug consumption studies for attention-deficit/hyperactivity disorder (ADHD). The main purpose of the present study was to present the pattern and the evolution of national ADHD drug consumption in Slovenia.
Methods:
The national consumption data for the period 2001–2012 and medication costs were obtained from the database of the Health Insurance Institute of Slovenia. A defined daily dose (DDD) per 1000 inhabitants per day and the total medication cost in euro were extracted. Only immediate-release methylphenidate (IR-MPH), methylphenidate-osmotic release oral delivery system (OROS-MPH) and atomoxetine (ATX) have been approved for ADHD in Slovenia and are included in this study. Amphetamines have not been available in Slovenia.
Results:
ADHD drug consumption increased in Slovenia from 0.0537 DDD/1000 inhabitants/day in 2001 to 0.0687 DDD/1000 inhabitants/day in 2006 and to 0.3076 DDD/1000 inhabitants/day in 2012. The rise was largely because of an increase in OROS-MPH consumption and increase in ATX consumption, whereas the consumption of IR-MPH decreased rapidly. During the study period, the total cost of the medicines increased 31-fold. From 2007 to 2010, the total cost of ADHD medicines increased 14-fold and from 2010 to 2012 the cost increased by 11.4% only.
Conclusions:
When new drugs are licensed in a jurisdiction, their prescription rates increase rapidly. The changes in the pattern of prescribing medicines are evident in Slovenia, primarily in the increase of OROS-MPH and ATX prescriptions and in the rapid decrease of IR-MPH prescriptions. Results indicate a need for appropriate interventions in Slovenia.
Introduction
A
In Slovenia, only immediate-release methylphenidate (IR-MPH) has been approved for the treatment of patients with ADHD before the introduction of ATX in 2006, and of methylphenidate-osmotic release oral delivery system (OROS-MPH) in 2007. Currently, amphetamine, lisdexamfetamine dimesylate (LDX), and pemoline are not available in Slovenia. In Slovenia, only ATX has been officially approved for adult ADHD since 2013 (Slovenian Central Database of Medicines 2014).
Studies conducted in several countries have shown a significant increase in the use of ADHD drugs in recent years (McCarthy et al. 2012). There are a number of countries for which these data are unavailable; for example in Eastern Europe and the former Yugoslavian countries. The main aim of the present study was to present the pattern of national ADHD drug consumption in Slovenia.
Methods
A descriptive drug utilization study has been chosen for the purpose of this study. The national consumption data and medication cost for the period 2001–2012 were obtained from database of the Health Insurance Institute of Slovenia (NHI). The database offers information on the national consumption and cost of the medicines dispensed in Slovenian outpatient pharmacy. The NHI included 10 regional centers, which cover almost the entire Slovenian population. These data are mainly used for administrative purposes, and serve to review the drug use and its consumption, and drug dispensing in the primary health system. The database does not include information about patients' characteristics such as age, gender, or specialty of prescribing physician and pharmacist. All prescriptions in one region are usually dispensed in the same region, except medicines for very rare diseases.
This database does not cover the hospital drug consumption from hospital and self-paid medicines. According to the consumption data for Slovenian hospitals, <1% of the total ADHD medications used in Slovenia was prescribed in hospitals in the past 5 years, and, therefore, these data were also excluded (imshealth 2014). The NHI database is known for its reliability and accuracy, and has been used in many published studies (Svab et al. 2011; Subelj et al. 2012).
Prescription indications for medicines are not identified through data collection, but we assumed that all medicines were used for ADHD, because they only have this indication in Slovenia. In Slovenia, only psychiatrists specializing in child and adolescent psychiatry and some psychiatrists with many years of practice in child and adolescent psychiatry can prescribe drugs for ADHD. Drugs in Slovenia are prescribed for 3 months in the maintenance phase of pharmacotherapy (one prescription). Therefore, four prescriptions are usually necessary for 1 year of treatment in the maintenance phase with a single drug, as was assumed in this study to assess the number of patients with ADHD in Slovenia.
Slovenia is a Central European county, with a population of ∼2,000,000; 300,000 live in its capital, Ljubljana, and ∼120,000 live in its second largest city, Maribor. The data obtained from the Institute of Public Health of the Republic of Slovenia from 2001 to 2012 show that >90% of new patients with hyperkinetic disorder (ADHD) in Slovenia are children and adolescents; therefore, the consumption trend obtained from NHI shows a prescribing trend for children and adolescents with ADHD in Slovenia (Statistical Office of the Institute of Public Health of the Republic of Slovenia 2014). Therefore, >90% of established patients with an existing diagnosis of hyperkinetic disorder (ADHD) in Slovenia are children and adolescents. In Slovenia, the price of medicinal products is regulated by the Slovenian Agency for Medicinal Products and Medical Devices, whereas their financing from public revenues is regulated by the Health Insurance Institute of Slovenia. All children and adolescents (<18 years of age) have their healthcare covered by a state-controlled mandatory insurance, paid through the Health Insurance Institute of Slovenia. Currently, there are no professional restrictions on prescribing ATX, OROS-MPH, and IR-MPH in Slovenia.
The data are presented in defined daily doses (DDDs) per 1000 inhabitants per day (DDD/1000/inhabitants/day). The results of drug consumption were expressed in DDD and number of DDD per 1000 inhabitants per day.
The DDD values were as follows: ATX, 60 mg; IR-MPH, 30 mg; OROS-MPH, 30 mg and were recorded by the World Health Organization (WHO) (WHO Collaborating Centre for Drug Statistics Methodology 2007). The required population data for this study was obtained from the Statistical Office of the Republic of Slovenia. The total cost per year for DDD was calculated by dividing the total cost by the total DDD consumed for a drug studied. All values were expressed in euros. The data are graphically presented as the total national consumption. Analyses, tables, and graphs were made with Microsoft Excel® 2010.
Ethical approval for the study was obtained from the National Medical Ethics Committee of the Republic of Slovenia.
Results
National consumption
The total amount of consumed ADHD drugs in Slovenia increased by 5.75-fold during the observed 12 year period and by 4.17-fold from 2007 to 2012. This study started in 2001, when only IR-MPH was available on the Slovenian market. IR-MPH was the only available drug for ADHD until 2006, when ATX was introduced, followed by OROS-MPH in 2007 (Fig. 1). The total Slovenian consumption of all drugs for ADHD was stable from 2001 to 2007, and increased rapidly from 2007 to 2012, mainly because of MPH. During the first 6 years, drug consumption was stable, and increased from 0.0537 DDD/1000 inhabitants/day in 2001, to 0.0687 DDD/1000 inhabitants/day in 2006, representing only 28% of the total growth in consumption in the 6 year period in Slovenia. MPH increased much more rapidly than ATX, from 0.0687 DDD/1000 inhabitants/day in 2006, to 0.2501 DDD/1000 inhabitants/day in 2012. ATX consumption rose rapidly from 0 to 0.0447 DDD/1000 inhabitants/day in 2010 and was relatively stable from 2010 (0.0447 DDD/1000 inhabitants/day) to 2012 (0.0575 DDD/1000 inhabitants/day). The consumption of MPH also increased by 2012 and was not stable (0.0735 DDD/1000 inhabitants/day in 2007, 0.2040 DDD/1000 inhabitants/day in 2010, and 0.2501 DDD/1000 inhabitants/day in 2012). From 2010 to 2012, there was an even greater difference in consumption of ATX and MPH than before; the ratio between MPH/ATX in consumption expressed in DDD/1000 inhabitants/day was 4.6 in 2010 and 4.4 in 2012. The ratio of total consumption of ATX and MPH between 2012 and 2007 was 4.2, and it was 1.2 between 2012 and 2010.
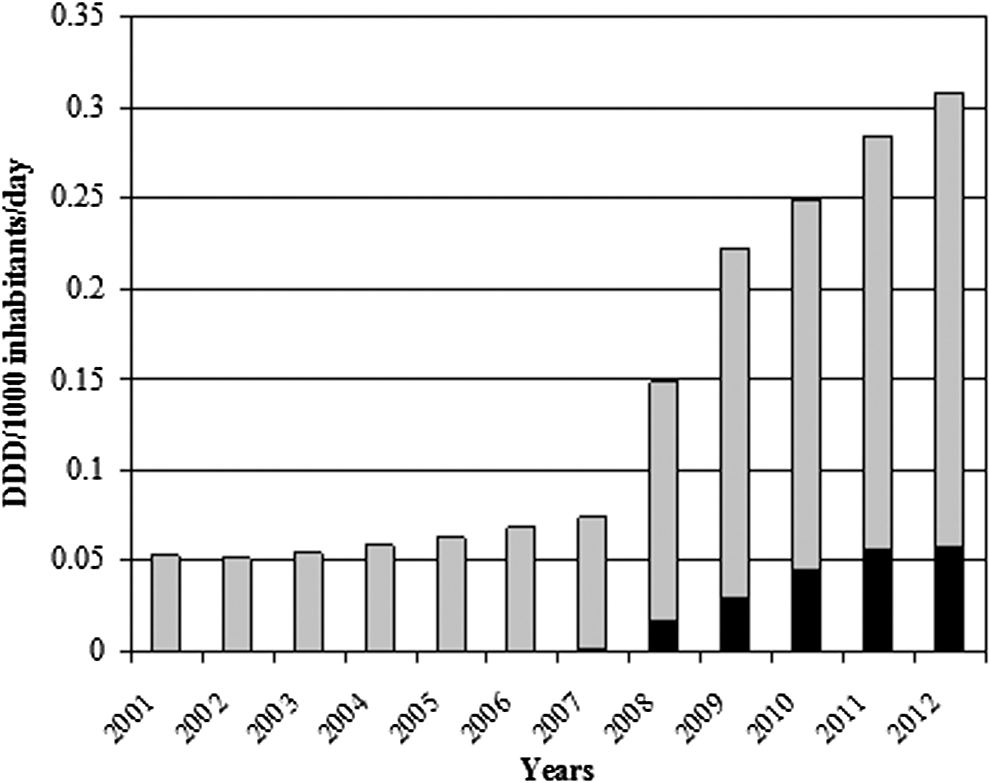
The pattern and the evolution of attention-deficit/hyperactivity disorder (ADHD) drug consumption in Slovenia expressed in defined daily dose (DDD)/1000 inhabitants/day. Atomoxetine (black); methylphenidate (grey); atomoxetine+metylphenidate (black+grey).
After ATX and OROS-MPH were introduced on the Slovenian market in 2006 and 2007, the total consumption of IR-MPH rapidly decreased until 2009 (0.0537 DDD/1000 inhabitants/day in 2001 to 0.0416 DDD/1000 inhabitants/day) and was again more stable from 2009 to 2012 (0.0416 DDD/1000 inhabitants/day in 2009 to 0.0401 DDD/1000 inhabitants/day in 2012) (Fig. 2). In 2012, at the end of the studied period in Slovenia, the consumption of OROS-MPH was 3.65 times greater than that of ATX, and 5.24 times than that of IR-MPH. IR-MPH contributed only 13.0% to the total drug consumption for ADHD; ATX contributed 18.7%; and OROS-MPH contributed 68.3%.

The pattern and the evolution of attention-deficit/hyperactivity disorder (ADHD) drug consumption in Slovenia expressed in defined daily dose (DDD)/1000 inhabitants/day. Atomoxetine (black); osmotic release oral delivery system (OROS)-methylphenidate (grey); immediate release (IR)-methylphenidate (white).
Total costs of ADHD medicine consumption
In the studied period, the total costs of medicines increased from 15,529 euro in 2001 to 484,343 euro in 2012 (Fig. 3). Average total costs per year of ADHD medicines in Slovenia increased rapidly after OROS-MPH and ATX were introduced in 2006 and 2007. In 2010, the total costs of prescriptions for ATX and MPH were almost equal, but they were 27.5% higher for ATX than for MPH in 2012. From 2007 to 2010, the total costs for ADHD drugs rose 14-fold, but from 2010 to 2012 it rose only 11.4%. The total costs in Slovenia from 2001 to 2012 increased 31-fold, and they increased 16-fold from 2007 to 2012. Overall, new drugs on the ADHD market have a higher cost. In 2012 ATX cost 6.36 euro per day, OROS-MPH cost 1.24 euro per day, and IR-MPH only cost 0.63 euro per day.
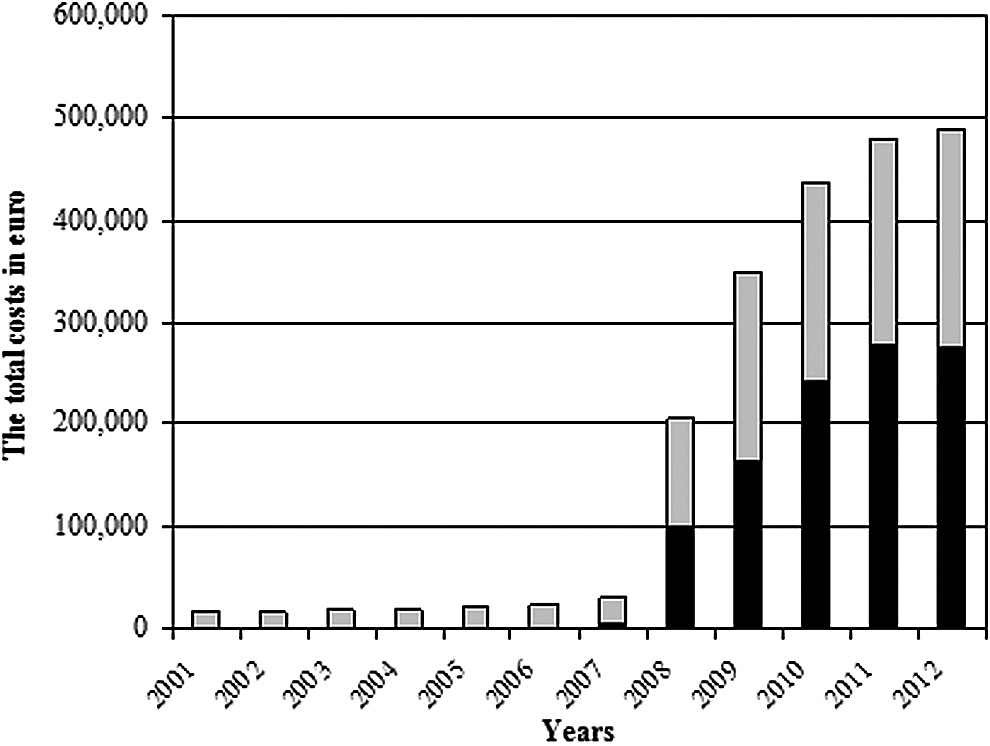
The total costs of attention-deficit/hyperactivity disorder (ADHD) medicine consumption in Slovenia expressed in euro per year. Atomoxetione (black); methylphenidate (grey); atomoxetine+methyphenidate (black+grey).
Discussion
When new drugs became available on the Slovenian market, their prescription rates increased rapidly. The rapid increase in consumption of ADHD medicines in Slovenia from 2007 to 2010 could be the result of new medicines on the Slovenian market (OROS-MPH and ATX), better pharmaceutical marketing, and, consequently, more education about ADHD among Slovenian physicians, patients, and parents. It is interesting how availability and marketing may have changed and increased prescribing, because from 2006 to 2012, the total consumption increased almost fivefold. Prior to 2006, marketing of these drugs was nonexistent. In addition, Slovenia introduced specialization in child and adolescent psychiatry in 2003, which increased the number of diagnosed and treated patients over the past 5 years. Lastly, Slovenia has been a member of the European Union (EU) since 2004, which allowed easier access to information about ADHD from Western countries. One of the important factors could be a lack of national treatment guidelines and the adoption of European guidelines after joining the EU in 2004, which may be a reason for the low but stable consumption before 2007 (Štuhec 2013b). The result is an observed time shift in the total consumption in Slovenia in comparison with Western countries (Schubert et al 2012; Register of Medicinal Products Statistics 2014; Norwegian Institute of Public Health 2014). These arguments are also confirmed by the data on the total sale of ADHD medicines and their market share by pharmaceutical companies in Slovenia during this period obtained from imshealth (rapid increase in unit sales and in the total price in euros).
The pattern of consumption in Slovenia is not comparable with that of other countries. Norway and Denmark's consumption of ADHD drugs in 2009 was 6.5 DDD/1000 inhabitants/day and 4.5 DDD/1000 inhabitants/day, compared with only 0.221 DDD/1000 inhabitants/day in Slovenia (Danish Medicines Agency 2014; Norwegian Institute of Public Health 2014). Norway and Denmark saw a dramatic increase from 2004 to 2009. Slovenia followed with a delay, from 2007 to 2012, mainly because of the late arrival of new medicines to the Slovenian market, slow pharmaceutical marketing, and underdiagnosis. On the other hand, ADHD drug consumption increased in Castilla y León (part of Spain) from 0.1 DDD/1000 inhabitants/day in 1992 to 1.5 DDD/1000 inhabitants/day in 2009 (Treceño et al. 2012). These results are much lower than in Norway and Denmark, but are still almost sevenfold higher than in Slovenia. Consumption of all ADHD drugs covered by Israel's national healthcare system doubled from 4.02 DDD/1000 inhabitants/day in 2005 to 9.92 DDD/1000 inhabitants/day in 2012 (Ponizovsky et al. 2014). DDD/1000 inhabitants/day for all ADHD drugs in Turkey was 0.28 in 2009, 0.41 in 2010, 0.52 in 2011, and 0.59 in 2012 (Oner et al. 2014).
In France in 2003, the overall annual prevalence of prescriptions to children and adolescents <18 years of age for MPH was 0.15%, and MPH was less often prescribed than in other European countries. Acquaviva et al. (2009) suggested that ADHD is underdiagnosed in France. Because of the different methodology of study, it is difficult to compare results directly, but it can be concluded that Slovenia had a lower consumption rate of ADHD medicines than France in 2003. In 2012, however, the consumption was almost equal in both countries, according to the calculated annual prevalence of prescriptions in Slovenia and the calculated consumption obtained from our study (Statistical Office of the Republic of Slovenia 2014).
In the United Kingdom, the prevalence of prescribing (measured in number of prescriptions) across all ages increased 6.23-fold from 1999 to 2006. Their database included patients 15–21 years of age from 1999 to 2006. MPH (immediate and modified-release preparations), LDX, and ATX were included. ADHD medicines consumption in Slovenia only increased 1.27-fold from 2001 to 2006 (expressed in DDD/1000 inhabitants/day), which indicates a much slower increase than in the United Kingdom.
In the German region of Hesse in 2007, 1.06% of the children and adolescents received at least one prescription for MPH; a 96% increase compared with the prescription rate in 2000. The average consumption during 2000–2007 increased by 82 % (Schubert et al. 2010). In Slovenia in 2007, the overall annual prevalence of prescriptions was approximately threefold lower than that in Germany, but the increase in consumption (DDD) was similar in both countries. These differences are mainly because of reasons already mentioned (marketing, medicines availability, lack of guidelines, national health policy).
The Turkish pattern of consumption is more similar to the Slovenian, which indicates low total consumption in Slovenia and Turkey, compared with in Israel, Denmark, and Norway. Currently in Slovenia, these medicines are only prescribed by a low percentage of psychiatrists, who work mainly in child and adolescent psychiatry, and, currently, there are no Slovenian treatment guidelines for ADHD (Štuhec 2013a,b).
According to the results, IR-MPH was not the treatment choice in Slovenia after new drugs entered the market, which is not in line with the recommendations of the European Society for Child and Adolescent Psychiatry (ESCAP) (Taylor et al. 2004), because ATX consumption is Slovenia was high and IR-MPH consumption has been almost insignificant in recent years. The guidelines group in 2006 considered the key advantages of IR formulations of stimulants to be their lower cost and flexibility of dosage. The conclusions were that controlled release formulations should be available and used; but that they should not entirely replace the IR formulations (Banaschewski et al. 2006). In a study in Germany, 6210 newly diagnosed ADHD patients (children and adolescents) were followed from 2005 for a maximum of 4 years. At the beginning of drug treatment with MPH, the majority of patients (82.3%) started on IR-MPH formulations (Garbe et al. 2012). In Israel, a big rise in consumption was largely the result of a fivefold increase in OROS-MPH consumption (from 0.46 DDD/1000 inhabitants/day in 2005 to 2.28 DDD/1000 inhabitants/day in 2012) and a threefold increase in IR-MPH consumption (from 1.43 DDD/1000 inhabitants/day in 2005 to 4.84 DDD/1000 inhabitants/day in 2012) (Ponizovsky et al. 2014). In Turkey in 2012, OROS-MPH represented almost 75% of all ADHD drug utilization, which is very close to the Slovenian pattern (Oner et al. 2014). In Slovenia, the consumption of IR-MPH preparation decreased rapidly after 2007, and its consumption was only 13.0% among ADHD drugs in 2012, which indicates a very high percentage of patients in whom IR-MPH was not started, which is, again, not according to the treatment guidelines (Banaschewski et al. 2006).
According to the European guidelines, intensive management in ADHD can be effective for translating the guidelines into clinical practice, which is currently inadequate in Slovenia (Banaschewski et al. 2006). These results also suggest possible strong pharmaceutical marketing against the use of IR-MPH as a first line therapy, which could be resolved with the introduction of national treatment guidelines for and monitoring of prescribing.
ATX use in Slovenia, compared with that of MPH, is very similar to their use in other countries. In Castilla y Leon, the consumption of ATX was 0.05 DDD/1000 inhabitants/day in 2009 (Treceño et al. 2012). A similar increase as was the case with MPH has not been observed for ATX in Germany, although ATX is not subject to controlled substances legislation in Germany and is, therefore, easier to prescribe (Garbe et al. 2012). ATX is usually regarded to be of lower efficacy than MPH (Vaughan et al. 2009; Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011); therefore, a fast increase in ATX consumption and decrease in IR-MPH consumption in Slovenia indicate inappropriate prescription in daily practice. Currently in Slovenia, there are no restrictions on prescribing on ATX, although the prescription trend and the total costs for ATX indicates inappropriate prescribing in Slovenia, and possible strong activities from pharmaceutical companies in light of the elevation of ATX prescribing and its larger market share.
These data also shows that general practitioners (GPs) should be involved in ADHD treatment more intensively. A study of Slovenian primary care concluded that there are serious barriers among GPs to becoming involved in the treatment and prevention of mental health disorders (Poplas Susič et al. 2010). This is because Slovenian psychiatry is predominantly hospital based. Also, ADHD is predominantly treated in non-hospital settings in Slovenia, but Slovenian psychiatry and its organization are predominantly hospital based (not community based). A program for the development of general community psychiatric services is not appropriately formed to improve access to, and the quality and comprehensiveness of psychiatric care according to the modern standards of psychiatric service delivery. Another reason is that factors that have little to do with science have a major impact on policy decision making (Svab and Svab 2013). These gaps in ADHD are to be addressed through team coordinated action involving GPs, specialists from child and adolescent and adult psychiatry, specialists from clinical pharmacy and psychology, nongovernment organizations with service users and carers, the Health Insurance Agency, and politicians involved in the planning of health services in ADHD and the provision of appropriate care for these patients.
Limitations
There are some limitations to this study. One of the limitations of this study is the DDD value, which is an approximate unit of measurement and does not necessarily reflect the real daily dose consumed by patients. If the real prescribed daily dose is lower than the DDD, the use of DDD leads to an underestimation of the prevalence of use. If the prescribed daily dose is higher than the DDD, the use of the DDD overestimates the number of patients taking this medicine (Treceño et al. 2012). The DDDs as set by the WHO are within average, and could be influenced by the age distribution of the patients as well. Therefore, we cannot make any conclusion about the dosage used in Slovenia.
Another limitation is the database used in this study. From this database we cannot get the exact number of patients with ADHD. The database does not allow for any stratification by age or gender. There is also no information available regarding the clinical conditions and indications for medication use (it is assumed these medications were prescribed for ADHD). We can only speculate from the total DDD/1000 inhabitants/day calculation that there are currently ∼600 patients with ADHD in Slovenia, if adherence to drug therapy were 100%, which is not likely. From this study, we do not know how long one patient might wait for an appointment with an ADHD specialist.
Another small limitation of our study is that the database does not include drug consumption in hospitals. A small percentage of the total medications for ADHD used in Slovenia are prescribed in hospitals (<1% in past 5 years) and, therefore, results refer not only to consumption in the primary care or non-hospital setting (imshealth 2014). It is also possible that the medicines dispensed by pharmacists were not actually consumed by the patients, which is often the case in psychiatric disorders. Garbe at al. reported that ∼20% of treated ADHD patients discontinued drug treatment within the first 6 months (n=6210), with girls stopping drug treatment earlier than boys. After 6, 12, and 24 months of treatment initiation, 22.4%, 43.4%, and 66.3% of treated girls, and 17.8%, 36.1%, and 54.1% of treated boys had discontinued ADHD treatment (Garbe et al. 2012).
Conclusions
The calculation indicates that there are ∼600 people with ADHD receiving pharmacologic treatment in Slovenia in a population of 2,000,000 (∼3:10,000). Given the low percentage of adult patients with ADHD in Slovenia, the results primarily show the drug consumption trend in children and adolescents with ADHD in Slovenia. The results show that some of the newer ADHD medications became more widely available and used in Slovenia with a “delay” relative to other countries. There has been a rapid increase in ADHD drug consumption in Slovenia in the past 6 years, after OROS-MPH and ATX were marketed. Fast increase in ATX consumption and decrease in IR-MPH consumption in Slovenia indicates urgent introduction of treatment guidelines into daily practice. Adherence to new Slovenian guidelines will greatly improve the management of ADHD patients. A general scheme for ADHD practice in Slovenia should be provided.
Clinical Significance
The authors have written about an under-studied topic: ADHD medication use in Central and Eastern Europe. This is the first study that describes national ADHD drug consumption trends in this part of Europe, and, consequently, the results may be widely applicable. The inadequate translation of European guidelines into clinical practice in Slovenia is evident. The results suggest possible strong pharmaceutical marketing against the use of IR-MPH as a first line therapy, and indicate a need for appropriate interventions in Slovenia, such as making more effective ADHD medicines available by prescription. These results also open a new window for possible restrictions from the NHI on ATX prescribing, which could also reduce the price of ATX. This article presents the first rough estimation on the epidemiology of ADHD in Slovenia, derived from the calculation of pharmacoepidemiologic data.
Footnotes
Disclosures
No competing financial interests exist.