
Abstract
Objective:
The purpose of this study was to evaluate the effectiveness and safety of antipsychotic and antidepressant medications in individuals with 22q11.2 deletion syndrome (22q11.2 DS) and psychiatric comorbidity.
Methods:
We used a record review, structured clinical interviews, and the Clinical Global Impressions (CGI) scale to retrospectively assess the effectiveness and safety of antipsychotic medications for schizophrenia spectrum disorders and of antidepressant medications for depressive and anxiety disorders in 40 individuals with 22q11.2DS.
Results:
We observed significant improvement in CGI-Severity scores in individuals with 22q11.2DS treated with antipsychotic or antidepressant medications, and a ∼50% response rate based on the CGI-Improvement score. Adverse events were similar in types and rates to those reported in non-22q11.2 individuals treated with antipsychotics or antidepressants.
Conclusions:
Our data show that treatment with antipsychotics and antidepressants may be effective while being relatively safe in individuals with 22q11.2DS. Antipsychotic and antidepressant medications should be considered in any individual with 22q11.2DS who has a psychiatric morbidity, such as psychosis or mood or anxiety disorders. Although the psychotropic medications were generally well tolerated in our sample, more rigorous metabolic and cardiovascular measures are required in future studies to conclusively verify the safety of these medications.
Introduction
T
Psychiatric medications, such as antipsychotics, antidepressants, and stimulants, are also commonly prescribed to individuals with 22q11.2DS; however, the effectiveness and safety of these treatments are mostly unknown (Tang et al. 2014). We had previously investigated the effectiveness and safety of methylphenidate in treating ADHD symptoms in children with 22q11.2DS. We found that methylphenidate was effective, but that it was associated with higher rates of adverse events in this population (Gothelf et al. 2003; Green et al. 2011). In a case series of four individuals with 22q11.2DS and comorbid schizophrenia, poor response to typical antipsychotics was reported in two individuals who later responded favorably to clozapine (Gothelf et al. 1999). Other case reports described favorable antipsychotic response to aripiprazole in one of two individuals with 22q11.2DS and comorbid schizophrenic-like symptoms, and in one individual treated with quetiapine (Carandang and Scholten 2007; Muller and Fellgiebel 2008; Lin et al. 2010). Possible effectiveness of antidepressants was described in three individuals with anxiety disorders (Stachon and De Souza 2011) and in four individuals with obsessive-compulsive disorder (OCD) (Gothelf et al. 2004).
There are several reasons why individuals with 22q11.2DS might have less favorable clinical response to antipsychotic and antidepressant medications than typically developing individuals. The cognitive deficits might affect the ability of the patients to reliably and effectively report on the clinical response and potential side effects. Biological factors, such as dopamine dysregulation related to haploinsufficiency of the catechol-O-methyltransferase (COMT) gene (which is within the deleted region), might reduce clinical response to psychotropic medications. Individuals with 22q11.2DS might also be more vulnerable to adverse events, such as drug-induced cardiac arrhythmias, caused by their high rates of cardiovascular anomalies (McElhinney et al. 2001). Specifically, the presence of cardiovascular anomalies increases the risk of QT prolongation induced by antipsychotics (Marmon et al. 1984).
The lack of data about drug effectiveness, tolerability, and safety in these at-risk individuals might explain the underprescription of psychotropic medications among those who have psychiatric comorbidities (Tang et al. 2014). Such knowledge is, therefore, essential for patients with 22q11.2DS, for their families, and for their treating physicians.
In the present study, we retrospectively assessed the effectiveness and safety of antipsychotic medications for schizophrenia spectrum disorders, and antidepressant medications for depressive and anxiety disorders in individuals with 22q11.2DS.
Methods
Participants
Individuals with 22q11.2DS were recruited from the Behavioral Neurogenetics Center in a major hospital in central Israel. This center is unique in Israel and receives referrals of individuals with 22q11.2DS from all over the country. We screened the medical records of all the 22q11.2DS individuals who attended this clinic between the time it was opened in 2000 up to 2012. They had all been treated over the years by one physician who was a trained child and adult psychiatrist (D.G.). The study was restricted to individuals diagnosed as having 22q11.2DS as genetically confirmed with a fluorescent in situ hybridization (FISH) test.
Assessments
The following data were collected from the medical charts: Age, gender, psychiatric diagnosis, medication history and present treatments, dosages, adherence, and adverse events. The institutional review board of Rabin Medical Center approved the study protocols and the review of medical records.
The psychiatric diagnoses of all participants were obtained by an interview using the Hebrew version of the Kiddie – Schedule for Affective Disorders and Schizophrenia for School-Aged Children (K-SADS) for pediatric patients and their parents (Kaufman et al. 1997; Shanee et al. 1997), or the Structured Clinical Interview for Axis I Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) (SCID) for adult patients (American Psychiatric Association 1994; First et al. 1996). Cognitive evaluation was conducted by well-trained master's degree-level psychologists using the age-appropriate versions of the Wechsler Intelligence Scale for Children, 3rd ed. (WISC-III) and Wechsler Adult Intelligence Scale, 3rd ed. (WAIS-III) (Wechsler 1991, 1997). Data were not available for three participants from the antipsychotic sample and for one participant from the antidepressant sample.
The retrospective improvement of the psychiatric symptoms was evaluated using the Clinical Global Impressions scale (CGI) (Guy 1976). CGI-Severity (CGI-S) rates the severity of the patient's mental illness at the time of the assessment from 1 (normal) through 7 (severely ill), based on the clinician's experience with patients with the same diagnosis. The CGI-Improvement (CGI-I) scale rates the improvement of psychiatric symptoms: Scores of 1, 2 and 3 represent very much, much, and minimally improved, respectively; 4 represents no change in symptoms; and 5, 6, and 7 represent minimal, much, and very much worse, respectively. All CGI-I scores are relative to baseline. Based on the medical reports, two psychiatrists separately rated the CGI-S scale at baseline and at the end of follow-up (last recorded visit), as well as the CGI-I scale at the end of follow-up. Overall agreement between the two raters was very good. There were discrepancies of 1 point in the CGI-S (mostly between scores 5 and 6) and 1 point in CGI-I (mostly between scores 1 and 2) in five cases in the antipsychotic sample and in four cases in the antidepressant sample. We considered clinical improvement as CGI-I=1 (very much improved) and 2 (much improved). The adverse events data were collected from the medical records and they consisted of the type of the adverse event, its severity, and the clinical implication (e.g., decision to change the medication's dosage or to discontinue medication).
Statistical analysis
We conducted the statistical analysis using SPSS software version 21 (IBM, Chicago, IL). Shapiro–Wilk test was applied to test for normal distribution of baseline and follow-up CGI-S scores. Baseline and follow-up CGI-S scores were not normally distributed in the antipsychotic-treated sample (CGI-S baseline Shapiro–Wilk=0.62 and CGI-S follow-up Shapiro–Wilk=0.89, p<0.01 for each) or in the antidepressant-treated sample (CGI-S baseline Shapiro–Wilk=0.60 and CGI-S follow-up Shapiro–Wilk=0.91, p<0.05 for each). Therefore, a Wilcoxon signed rank test was used to compare baseline and end-point CGI-S scores in both samples. We used the Fisher exact test to compare responses between specific antipsychotic medication types (risperidone, olanzapine, and quetiapine), and binary logistic regression with clinical improvement based on the CGI-I scale as our outcome measure, with sex, age and IQ as predictors. A two-tailed p value of 0.05 was considered significant. All results are expressed as mean±SD.
Results
Out of 190 records of individuals with 22q11.2DS, we detected 19 individuals (11 males and 8 females) who were treated with antipsychotic medications for psychotic spectrum disorders (9 diagnosed with schizophrenia, 1 with schizophreniform disorder, 2 with brief psychotic disorder, 1 with psychotic disorder not otherwise specified, 3 with schizoaffective disorder, 2 with psychotic depression, and 1 with bipolar disorder) (Table 1). Treatment “trial” was defined as the recorded time period of one antipsychotic drug treatment: Nine participants had one trial, seven had two trials (i.e., two discrete time periods with one antipsychotic drug treatment in each), and three participants had three or more discrete time periods with one treatment trial in each. It is of note that two participants (Table 1 participants 8 and 13) were prescribed quetiapine as an augmentation to the main antipsychotic; therefore, they were not included in the effectiveness analysis.
Quetiapine was prescribed as an augmentation treatment. OCD, Obsessive compulsive disorder; BDZ, Benzodiazepines; IVIG, Intravenous immunoglogulins.
Medication treatment started at a mean age of 23.5±7.8 years (range 11–41 years, median 24 years). Fourteen individuals (74%) started antipsychotic medications only as adults because they were referred to a psychiatrist and diagnosed as having a psychotic disorder only during adulthood. The mean duration of treatment was 41.3±58.3 months (range 1.5–233 months, median 10 months). The mean Full Scale Intelligence Quotient (FSIQ) was 69.8±12.4.
Twenty-one subjects (10 males and 11 females) had been treated with antidepressant medications, 10 for depressive disorders, 6 for non-OCD anxiety disorders (4 for generalized anxiety disorder, 1 for social phobia, and 1 for specific phobia), and 5 for OCD (Table 2). The mean FSIQ was 74.8±14.6. There were 23 treatment trials in the antidepressants sample: 19 participants had undergone one and 2 had undergone two. All 21 participants were treated with selective serotonin-reuptake inhibitors (SSRIs), and 19 (90%) were drug naïve (Table 2). Medications were started at a mean of 21.0±8.2 years of age (range 11–38 years, median 17 years), and the mean duration of treatment was 32.1±41.2 months (range 1–144 months, median 18.0 months). Tables 1 and 2 provide a full description of the samples.
MDD, Major depressive episode; OCD, Obsessive compulsive disorder; GAD, Generalized anxiety disorder; BDZ, Benzodiazepines; SAD, Social anxiety disorder.
The antipsychotic-treated trials
For the effectiveness analysis, we had 30 trials with single antipsychotics in each (Table1), and the individuals were drug naïve in 53% of them. There were 9 (30%) trials with risperidone (mean dosage of 3.1±1.4 mg/day, range 1–5 mg/day), 10 (33%) with olanzapine (mean dosage of 14.8±4.2 mg/day, range 10–20 mg/day), and 5 (17%) with quetiapine (mean dosage of 485±336 mg/day, range 75–800 mg). Additional medications used in our sample were: Clozapine, clothiapine (two trials for each medication), and amisulpride and fluphenazine (one trial for each medication). CGI-S scores significantly improved from baseline to end-point (6.0±0. 5 vs. 4.3±1.8, respectively, p<0.001) in the 30 trials with antipsychotics (Fig. 1). Significant clinical improvement (much=2 or very much improved=1 on the CGI-I scale) at follow-up was achieved in 15 (50%) of the 30 trials (Fig. 2). Sex, age, and IQ did not predict clinical improvement. Based on the CGI-I, we found that 7 of the 10 (70%) participants treated with olanzapine significantly improved compared with 3 of the 9 (33%) participants treated with risperidone, and 2 of the 5 (40%) participants treated with quetiapine. The differences in improvement in responses between individual medication types were not statistically significant.
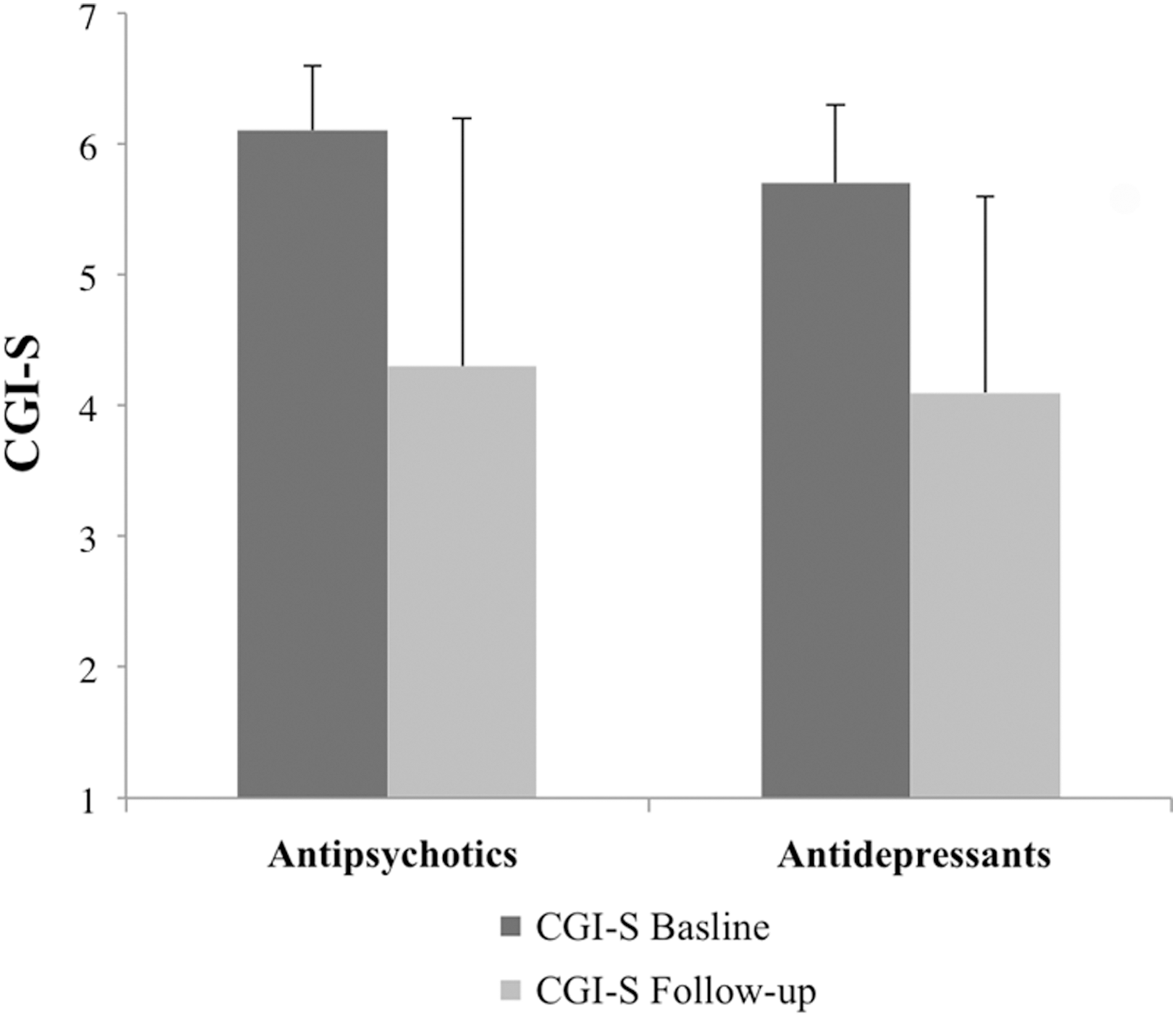
Significant improvement in Clinical Global Impressions–Severity scores from baseline to follow-up in participants with 22q11.2 deletion syndrome treated with antipsychotics or antidepressants.
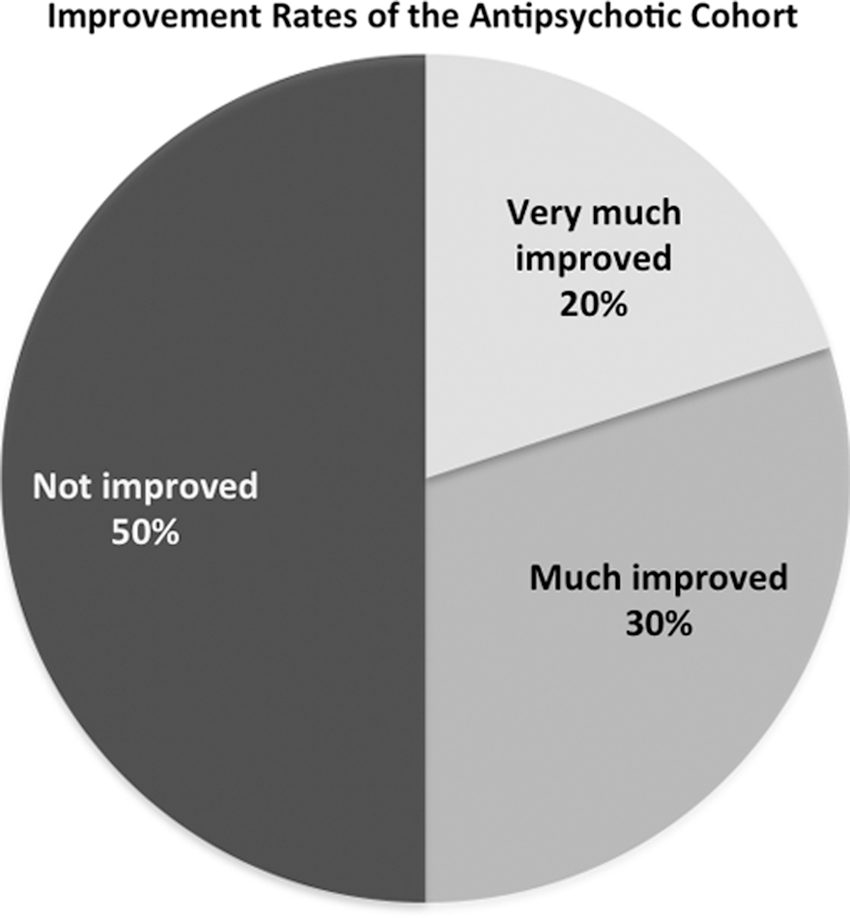
Antipsychotics' improvement rates based on Clinical Global Impressions-Improvement scores at follow-up.
Adverse events were reported in 21 out of 35 trials (60.0%). Of those 21 trials, 17 (58.6%) were considered mild, and 10 (34.3%) were rated as being severe (i.e., caused severe distress to the patient or caused dosage reduction or cessation of the treatment). The most frequent side effects were extrapyramidal symptoms, occurring in 9 (25.7%) of the 35 trials, and weight gain, occurring in 5 (14.2%) trials (Table 3). Individuals were also receiving either mood stabilizers and/or antidepressants concomitantly with antipsychotic medications in 20 trials (57.1%).
A 16-year-old male with 22q11.2DS and comorbidities of schizophrenia, OCD, and congestive heart failure caused by tetralogy of Fallot with pulmonary atresia developed QT prolongation after sertraline (150 mg/day) was added to quetiapine (850 mg/day), and risperidone 1.5 mg/day. The QT prolongation resolved after reduction in sertraline dosage to 100 mg/day.
Treatment with antipsychotics was discontinued in 16 (45.0%) of the trials. Causes for discontinuation were: Ineffectiveness in 10 participants, ineffectiveness and adverse events in 3 participants, and two episodes (in the same participant) of severe Parkinsonism that had developed with risperidone and then with amisulpride. One additional participant discontinued treatment because of poor treatment adherence.
Antidepressant- treated trials
There were 23 trials with antidepressants, and the participants were drug naïve in 75% of them (Table 2). Twenty-two of the 23 antidepressant trials involved SSRIs. These participants were included in the effectiveness and safety analysis (Table 2).
Based on the CGI-S scores, there was a significant clinical improvement from baseline to follow-up in the 22 trials with SSRIs (5.7±0.6 vs. 4.1±1.5, p<0.01, respectively, Fig. 1). Significant clinical improvement based on CGI-I scores (CGI-I ≤2) was observed in 12 (54.5%) trials (Fig. 3). Sex, age, and IQ did not predict clinical improvement. Clinical improvement was observed in 7 out of 10 (70%) trials for depressive disorders, in 4 out of 7 trials (57%) for any anxiety disorder, and in only 1 out of 5 (20%) trials for OCD (three out of the four remaining participants had CGI-I scores of 3, indicating “minimally improved”).
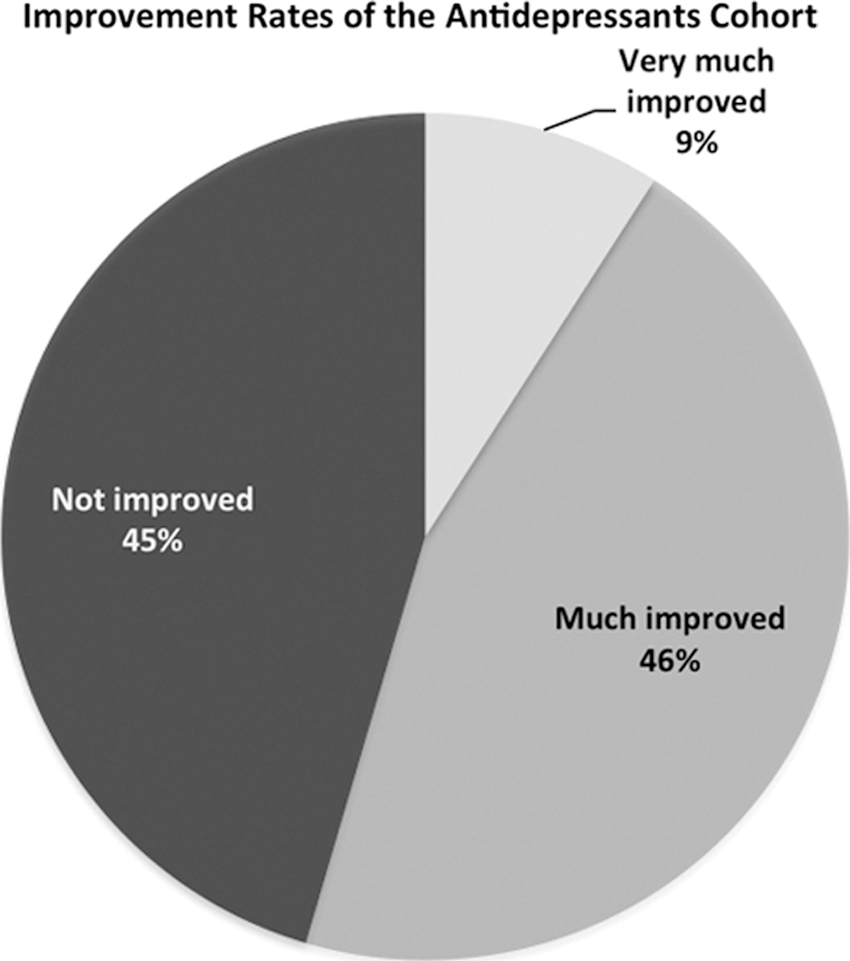
Antidepressants' improvement rates based on Clinical Global Impressions-Improvement scores at follow-up.
Adverse events were reported in 6 out of the 23 trials (26.0%). The adverse events were mild, and consisted of drowsiness, nausea, weight gain, and dry mouth in 5 trials. One participant diagnosed with major depressive disorder experienced mild confusion under venlafaxine treatment at a dose of 300 mg/day. The confusion resolved after dose reduction to 225 mg/day. Fluoxetine was discontinued because of the emergence of manic symptoms in one participant diagnosed as having OCD. No sexual adverse events were reported. Seven (30.4%) treatment trials were discontinued because of lack of clinical improvement.
Discussion
This is the first report that provided detailed data on the effectiveness and safety of antipsychotic and antidepressant treatments in individuals with 22q11.2DS. Overall, we observed significant improvement in CGI-S scores in individuals with 22q11.2DS treated with antipsychotics or antidepressants, and a response rate of ∼ 50% as assessed by the CGI-I. Adverse events were similar in nature and rates to those reported in non-22q11.2 individuals treated with antipsychotics or antidepressants.
Antipsychotics
Our findings suggest that individuals with 22q11.2DS have similar response rates to antipsychotic medications as non-22q11.2DS individuals with first-episode schizophrenia (Boter et al. 2009). We found a numerically higher rate of clinical improvement for olanzapine (70%) than for quetiapine (40%) and risperidone (33%); however, these differences were not statistically significant, probably because of the small sample size. It is of note that all 9 participants treated with risperidone were drug naïve, compared with only 4 out of 10 participants treated with olanzapine. Taken together, our results appear to suggest that olanzapine might be relatively more effective for treating psychotic symptoms in 22q11.2DS. The favorable antipsychotic effect of olanzapine in 22q11.2DS is in line with the findings of comparative trials on non-22q11.2DS schizophrenia patients by showing slightly larger response rates to olanzapine compared with other antipsychotics, including risperidone and haloperidol (Boter et al. 2009; Hartling et al. 2012).
Adverse events were reported in 60% of 22q11.2DS participants treated with antipsychotics, which is even somewhat lower than the rates (72–82%) reported in non-22q11.2DS schizophrenia patients treated with antipsychotics (Kahn et al. 2008; Boter et al. 2009; Findling et al., 2010). Akathisia and Parkinsonism were the most prevalent side effects, affecting 26% of the individuals in antipsychotic-treated trials and leading to discontinuation of treatment in five (14%) trials. The rates of reported akathisia in our sample are similar to reported rates of akathisia in non-22q11DS individuals with schizophrenia treated with second-generation antipsychotics (24–36%) (McEvoy et al. 2007; Miller 2008). Much lower rates of drowsiness (8%) and weight gain (14%) were recorded in our sample compared to reported rates in non-22q11.2DS (∼50% each) individuals (McEvoy et al. 2007). These differences might be the result of the retrospective nature of our assessment, and lack of structured assessments (e.g., regular weighing). The differences between reported rates of drowsiness in our study (8%) and in a non-22q11.2DS population may be related to difficulty in detecting drowsiness in 22q11.2DS individuals, who are characterized by low levels of activity and are commonly socially inhibited (Schonherz et al. 2013). These traits might obscure drowsiness, which might, therefore, have been overlooked.
Antidepressants
The response rates of participants with depressive disorders (70%) and anxiety disorders (57%) were similar to the response rates reported for SSRIs in non-22q11.2DS adolescents and adults with depressive disorders (58–60%) (March et al. 2007; Gibbons et al. 2012) and anxiety disorders (54–80%) (Birmaher et al. 2003; Wagner et al. 2004; March et al. 2007). Although the response rates of participants with OCD (20%) were relatively low, three of the four nonresponding individuals also had CGI-I scores that indicated modest improvement of OCD symptoms (CGI-I=3), which is in line with the description of only modest improvement in OCD symptoms in non-22q11.2DS individuals treated with SSRIs (Soomro et al. 2008). In all participants, except for one who developed manic symptoms, adverse events were relatively mild, and also resembled the reported rate of adverse events in non-22q11.2DS patients.
Limitations
The retrospective nature of this study increases the possibility of bias. Specifically, we relied on records to assess CGI-S and CGI-I scores, our primary outcome measure. In addition, our sample size reduced our power for detecting differences in effectiveness between specific medications and across different diagnoses. Although the psychotropic medications were generally well tolerated in our sample, more rigorous metabolic and cardiovascular measures are required in future studies to arrive at conclusions regarding the safety of these medications. We did not detect any effect of sex, age, or IQ on the likelihood of benefiting from treatment. Given the small sample size, it is possible that we were underpowered to identify predictors of drug response. With respect to our outcome measure, it should also be noted that patients in 4 out of the 30 trials with antipsychotics were concurrently being treated with antidepressants, and that patients in 4 out of the 22 trials with antidepressants were concurrently being treated with antipsychotics for nonpsychotic symptoms. Although these observations reflect the complex psychiatric phenotype in 22q11.2DS, they limit our ability to assess the effectiveness of each drug separately. It is our practice to consult with a cardiologist before initiating psychotropic medications in individuals with 22q11.2DS and comorbid cardiac anomalies and to recommend follow-up cardiac evaluations during the dosage titration. We were not able to extract cardiovascular measures, such as QT intervals and blood pressure values, from the patients' files, but the fact that QT prolongation related to sertraline combined with antipsychotic medications was found in only a single participant is encouraging. It is of note that overlapping treatments with two or more medications that may induce QT prolongation further increase the risk of ventricular arrhythmias, such as torsades de pointes (Olsen 2005).
Conclusions
Our data show that treatments with antipsychotics and antidepressants are effective and relatively safe in individuals with 22q11.2DS. Antipsychotic and antidepressant medications should be considered in any individual with 22q11.2DS who has a psychiatric morbidity, such as psychosis or mood or anxiety disorders. Large-scale prospective studies are needed to further explore the effectiveness and safety profiles of psychotropic medication treatments in 22q11.2DS, as well as the influence of these treatments on the course of psychiatric morbidity in this at-risk population.
Clinical Significance
It is surprising that in spite of the fact that psychotic, mood, and anxiety disorders are common and well studied in 22q11.2DS, data on pharmacotherapy in this at-risk population are lacking. The scarcity of medication treatment trials in 22q11.2DS might be related to the relatively rarity of 22q11.2DS, therefore imposing some difficulty in recruiting large cohorts of participants in one center and following them at regular intervals. Additionally, many individuals with 22q11.2DS cope with multiple psychiatric comorbidities (e.g., anxiety disorders and ADHD or schizophrenia and OCD) that require polypharmacy, making it very difficult to measure the effect of an individual medication. Furthermore, as 22q11.2DS is associated with medical comorbidities (e.g., cardiac anomalies and hypocalcemia), many clinicians are reluctant to prescribe medications to this at-risk population. For example, Tang et al. (2014) reported that only 42% of individuals with 22q11.2DS and psychosis received antipsychotics. The undertreatment of individuals with 22q11.2DS and psychotic symptoms underscores the need for data on the effectiveness and safety of these treatments in individuals with 22q11.2DS. Our observations from 40 individuals treated with antipsychotic and antidepressant medications considerably expand the very limited research and experience with these pivotal psychotropic medications in individuals with 22q11.2DS.
Both anxiety and subthreshold psychotic symptoms were described as predictors for the later development of psychotic disorders in 22q11.2DS (Gothelf et al. 2013). Data are lacking on the potentially protective effect of medications for anxiety and subthreshold psychotic symptoms against the later development of psychosis in 22q11.2DS. Future prospective, longitudinal studies should evaluate if treatments of these “risk” symptoms can postpone or even prevent the development of full psychotic disorders in 22q11.2DS.
Footnotes
Disclosures
No competing financial interests exist.