
Abstract
Objective:
Adolescents with mental disorders are at increased risk for being overweight or obese, and subsequently developing metabolic syndrome. However, data regarding risk factors for weight gain during psychiatric hospitalization of adolescents are limited and inconsistent. The aim of this study was to investigate the sociodemographic, clinical, and pharmacological risk factors for weight gain during psychiatric treatment, in order to improve prevention of subsequent metabolic syndrome.
Methods:
We conducted a historical prospective study of 146 adolescent patients (mean age 15.2±1.9 years, 52.7% males), consecutively admitted for day treatment in an adolescent day unit (length of stay 141±76 days). Anthropometric measurements and laboratory analyses of fasting glucose and lipid levels were conducted as part of the routine medical care at admission and discharge. Psychiatric diagnoses, medication histories, and sociodemographic data were obtained from the electronic medical records system.
Results:
A significant increase in age- and gender adjusted body mass index (BMI) (i.e., z score) was observed (0.5±1.2 vs. 0.7±1.1 at admission and discharge, respectively, p<0.001). Male subjects were more prone to weight gain than females (odds ratio [OR]=3.5, 95% CI=1.2–10.3) and BMI z score at admission was inversely associated with weight gain (R 2 =0.2, p<0.0001). Surprisingly, age at admission, psychiatric diagnoses, length of stay, and number of medications were not associated with weight gain. Despite weight gain, fasting blood glucose and lipid profile did not change significantly during the study period.
Conclusions:
Hospitalization of adolescents in a psychiatric day unit may be associated with a significant weight gain, especially in male subjects and those with normal weight at admission. Efforts should be aimed to reduce weight gain among youth with psychiatric disorders during treatment, to avoid a subsequent metabolic syndrome.
Introduction
O
Adolescents are more susceptible to weight gain not explained by normal growth and to metabolic adverse effects, particularly lipid changes, than adults (Correll and Carlson 2006; Newcomer and Haupt 2006; Kryzhanovskaya et al. 2009; Maayan and Vakhrusheva 2010). Excessive weight gain in youth may result, in addition to disease burden, in a negative effect on self-esteem and social functioning, and decrease medication adherence (Patel et al. 2005). The relationship between overweight, obesity, and metabolic abnormalities with poor cardiovascular outcomes might even be accelerated when age-inappropriate weight gain and metabolic abnormalities begin during early development (Nathan and Moran 2008; Tirosh et al. 2011). It is of note that inappropriate weight gain, even when the individual stays in the normal weight category, is associated with a potentially atherogenic profile, independent of weight itself (Calarge et al. 2012).
Psychotropic polypharmacy is commonplace in the treatment of youth treated in a psychiatric day care and inpatient settings, and it often reflects the severity and multidimensionality of their mental illness. However, despite the potentially high cardiometabolic side effect burden in young patients, clinical studies directly comparing weight gain in a “real life” setting of patients with multiple diagnoses and medical treatments are scarce, and focused on second-generation antipsychotics (SGAs).
De Hoogd et al. demonstrated significantly greater gender- and age-adjusted body weight and abnormal weight status in a young (ages 4–18 years) Caucasian sample treated with SGAs than in those not receiving SGAs, independent of diagnoses (de Hoogd et al. 2012). Moreno et al. compared weight gain in youth diagnosed with bipolar disorder versus other psychotic and nonpsychotic disorders, who had been treated with SGAs for 3 months. The authors concluded that early weight gain and metabolic changes were present across diagnoses in youth treated with SGAs (Moreno et al. 2010). Another recent United States study indicated that increased weight among adolescents with severe mental illness may already occur before treatment with psychotropic medications (Gracious et al. 2010). Its authors reported that the combined prevalence of overweight and obesity in their patient cohort was 55.4% and of obesity alone 30%, approximately double the rate in national norms (Gracious et al. 2010). To date, this cross-sectional report is the only study available on patient weight status in an adolescent day treatment setting.
The aim of the present study was to characterize and identify sociodemographic, clinical, and pharmacological risk factors for age-inappropriate weight gain in a cohort of adolescent psychiatric patients hospitalized in a day care setting.
Methods
Participants
The study population comprised of 146 youth admitted consecutively to Geha Mental Health Center Adolescent Day Unit (ADU), in Israel. The ADU has a catchment area of ∼600,000 people, and serves as a tertiary academic center for child and adolescent psychiatry. Patients are referred by community mental health or other medical services, and are admitted voluntarily. Most patients have multiple comorbidities and have failed prolonged attempts at psychiatric outpatient treatments. To be included in the analysis, subjects were required to be hospitalized >30 days and ≤365 days, and to have had height and weight measurements at both admission and discharge. An exclusion criterion was a diagnosis of a restrictive eating disorder. The study was approved by the Institutional Review Board in accordance with the Declaration of Helsinki. The need to sign an informed consent was waived by the board because of the retrospective nature of the study.
Description of the ADU
The ADU is active 6 days a week throughout the year. The daily schedule consists of 7 hours (08:00–15:00) of various clinical and educational activities, among them 4 hours of physical activity per week. General Instructions for healthy lifestyle habits are given by the unit's dietitian to the caregivers. Breakfast and lunch are provided daily by the mental health center.
Definitions
Weight, height, and body mass index (BMI; kg/m2) measurements were converted into z scores using the 2000 Centers for Disease Control growth norms (Ogden et al. 2002). BMI z scores are considered the most appropriate weight variable for a long-term study with adolescents, as BMI score distribution varies heavily with gender and age. For this study, standard definitions of weight status in pediatric practice were used for sex and age: Underweight=≤ −1.96 BMI z score (BMI percentile ≤5th percentile); normal weight=−1.96–1 BMI z score (5th percentile to <85th percentile); overweight=1–1.96 BMI z score (BMI of 85th to <95th percentile); and obesity ≥1.96 BMI z score (≥95th percentile). Significant weight gain was defined as an increase ≥0.5 in BMI z score (Correll and Carlson 2006). Unfortunately, other parameters of the metabolic syndrome (such as abdominal circumference and blood pressure), were available only for a very small portion of the sample or only at a single time point. Therefore, they were not included in the current analyses, and were reserved for future investigation of a larger sample.
Study design
This was a naturalistic historical prospective study of data collected under standardized conditions. Medical records of all adolescents and young adults between the ages of 11 and 20 years who had been hospitalized at the ADU during the study period were reviewed. Demographic information, anthropometric measurements, laboratory metabolic data, psychiatric diagnoses, and past treatment history were extracted from the electronic medical records. Height and weight were measured at admission and discharge using Health O Meter Fitness Digital Scales (Precision Weighing Balances, Bradford, MA) while subjects were wearing indoor clothes without shoes. Psychiatric diagnoses were made in accordance with American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) criteria (American Psychiatric Association 2000) with the consensus of two senior child and adolescent psychiatrists.
In order to compare different diagnostic groups, patients were divided into different categories based on the clinically most prominent, termed “primary” diagnosis. Selection of medications, dosing, comedications, and treatment changes were naturalistic, based solely on clinical necessity according to daily observations in the ADU. Additional collected information concerning the patients was: 1) Previous substance abuse (no/yes), (2) smoking status (never smoked/not smoking now/smoking), and 3) suicide attempt (no/yes). Study outcome measures were body composition parameters: BMI, BMI z score and delta BMI z score (calculated as BMI z score at discharge minus BMI z score at admission) and laboratory metabolic parameters (fasting glucose, low-density lipoprotein [LDL], high-density lipoprotein [HDL], triglycerides, and total cholesterol).
Data analysis
Analysis of data was conducted using SPSS 21.0 statistical analysis software (IBM Inc., Chicago, IL). Normality of distribution of continuous variables was assessed using the Kolmogorov–Smirnov test (cut off at p=0.01). Continuous variables with approximately normal distributions were compared by gender and, separately, medication type, using the t test for independent samples, whereas those with distributions significantly deviating from normal were compared using the Mann–Whitney U test. Associations among categorical variables were assessed using the χ2 test. The effects on delta BMI z score of a model of weight gain (change from admission BMI z score ≥0.5 vs. <0.5) was calculated using a binary logistic regression analysis, adjusted for the variables that were found to be significant in a univariate analysis. The correlation among parameters was tested using a linear regression. All tests were two sided and considered significant at p<0.05. Prevalence of overweight and obesity was compared to national norms (Nitzan Kaluski et al. 2009; Levin et al. 2010). Israeli prevalence estimates of underweight, normal weight, overweight, and obesity were obtained from two databases of healthy individuals: The first Israeli national health and nutrition survey for ages 12–15 and 15–18 years (Nitzan Kaluski et al. 2009), and data from candidates for military service in the Israel Defense Forces (Levin et al. 2010).
Results
Study population
Of 191 youth who were consecutively admitted to the ADU, a total of 146 (76.4%) were included in this study. The following subjects were excluded from the analysis: 23 subjects were hospitalized <30 days, 3 subjects were treated for >365 days continuously, and no adequate information was available for other 19 others.
Demographic and clinical characteristics of the study sample are displayed in Table 1: Mean age 15.3±2 years old, 52.7% male (n=77), 62.3% normal body weight status (n=91), mean body weight 62.1±18.3 kg, mean BMI 23.3 kg/m2 and BMI z score 0.5±1.3 (equivalent to mean percentile of 69.1%). All patients were Caucasians.
ADHD, attention deficit hyperactivity disorder; ASD, autistic spectrum disorder; OCD, obsessive compulsive disorder; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Weight status of ADU subjects at admission compared to Israeli population
The prevalence of overweight and obesity was higher among the ADU adolescent patients than among the Israeli population: Among males ≤15 years, the prevalence of overweight in the general population was 13.2% versus 29.7% among the ADU subjects (p=0.004), whereas the prevalence of obesity in males>15 years of age was 4.2% in the general population versus 15% among the ADU subjects (p=0.003). Among females >15 years, prevalence of overweight in the general population was 11.3% versus 25% among the ADU subjects (p=0.002) (Fig. 1).
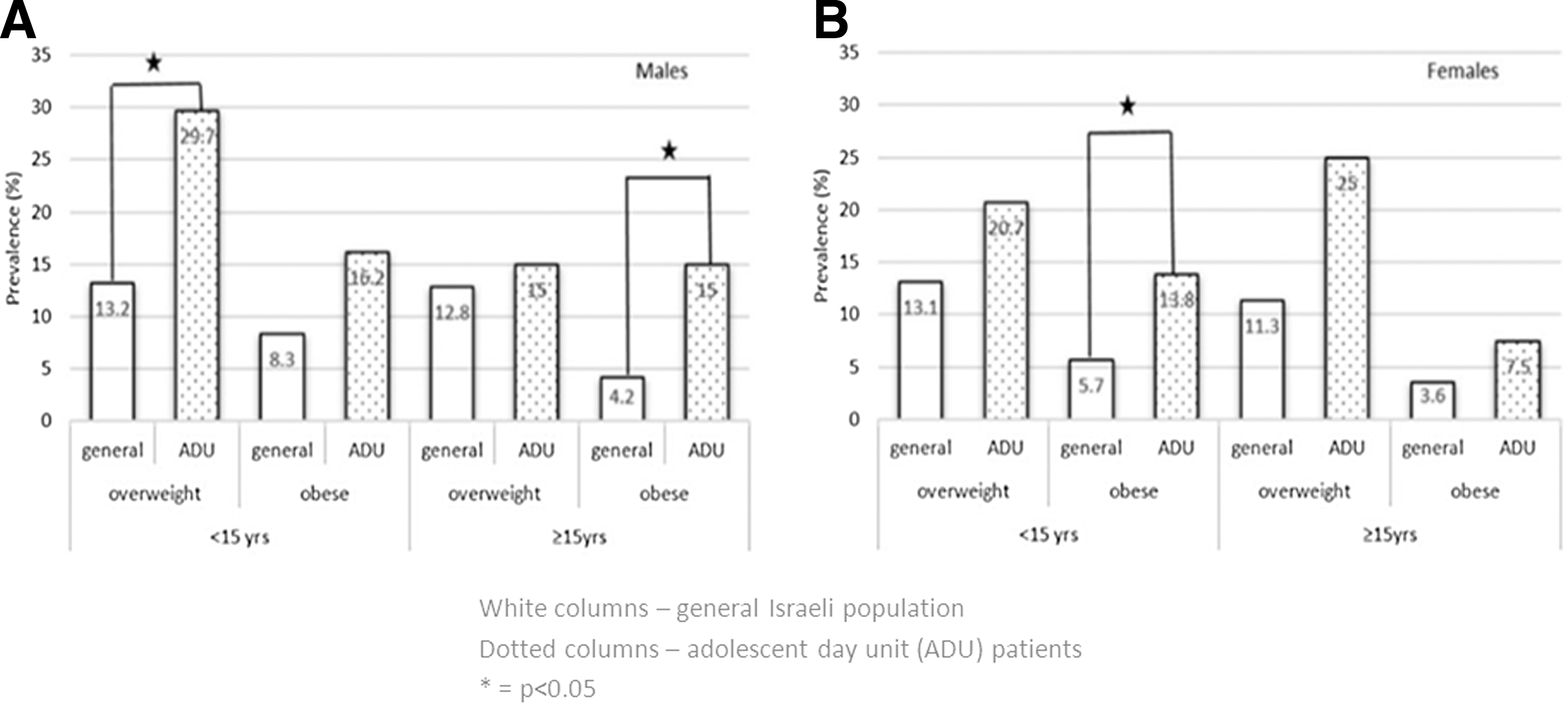
Prevalence of overweight and obesity in the sample compared with Israeli general population data by gender and age.
Weight status and metabolic parameters at admission and discharge
The distribution among weight status groups was similar at admission and at discharge: Underweight, 2.5% and 2.7%; normal body weight, 72.7% and 69.2%; overweight, 12.4% and 13%; and obese 12.4% and 15% respectively (p=NS). Fasting mean glucose, total cholesterol, LDL and HDL levels, and triglycerides of the cohort were not significantly changed during hospitalization (Table 1).
Follow-up data
For the whole cohort, mean body weight and mean BMI z score were significantly higher at discharge than at admission (65.6±18.9 kg. vs. 62±18.3 kg, p<0.001; z scores: 0.7±1.1 vs. 0.5±1.2, p<0.001). Weight gain was significantly greater among male subjects. Average weight gain in female and male subjects was 2.4±4.6 kg and 4.6±6.5 kg, respectively (p=0.002). Delta BMI z scores were 0.1±0.4 and 0.3±0.7 in female and male subjects, respectively (p=0.014). Delta BMI z score was inversely associated with BMI z score at admission (R2 =0.2, p<0.0001), and for both males (R2 =0.3, p<0.0001) and females (R2 =0.1, p<0.05) after adjusting for age, use of antipsychotics, and major depression (Fig. 2). Age at admission, length of hospitalization, and distribution of diagnoses and medications were similar among male and female subjects. No correlations were found between psychiatric diagnoses, age at admission, length of hospitalization, number of psychotrophic medications at discharge, and smoking status and weight gain during hospitalization.
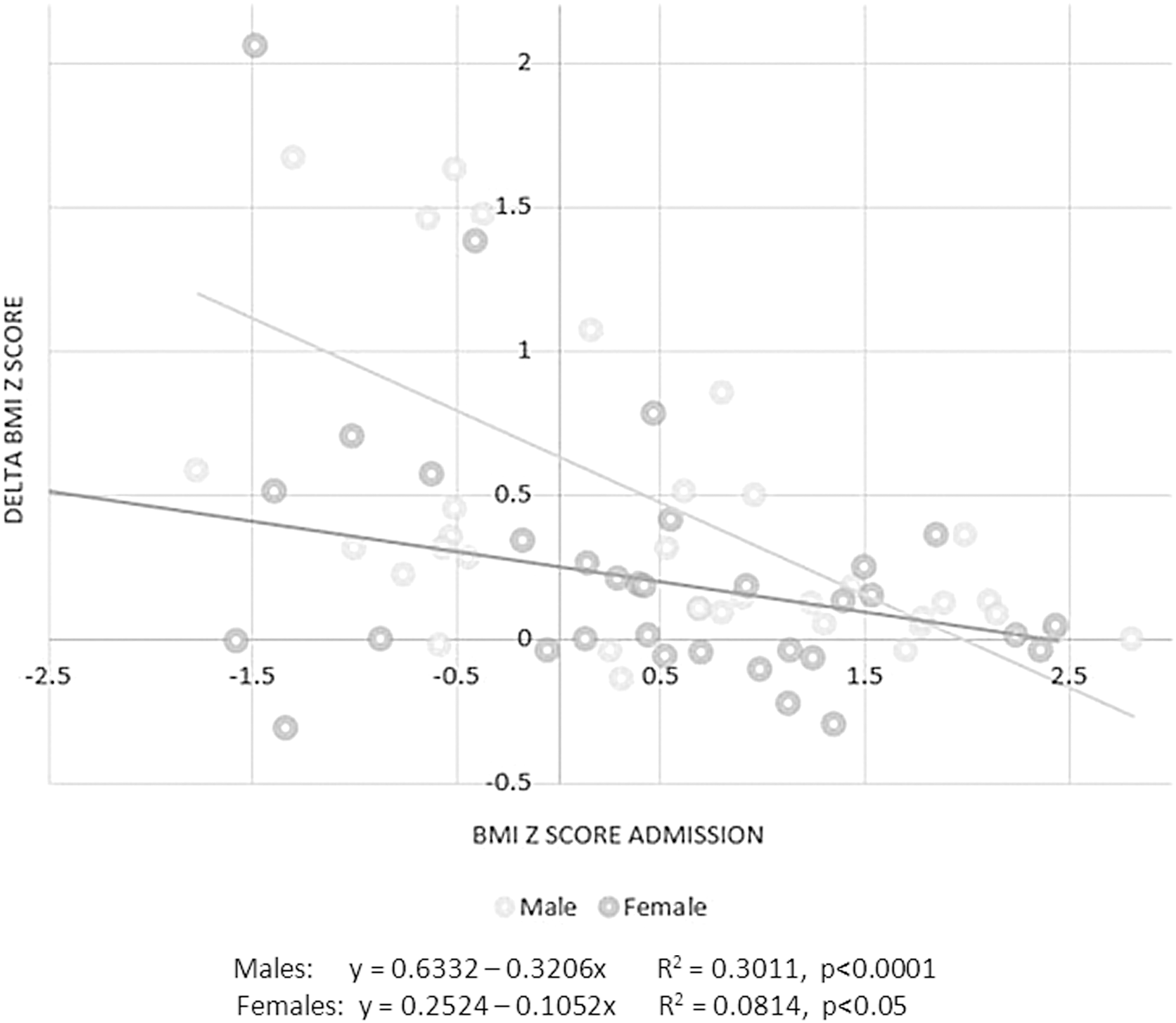
Correlation between body mass index (BMI) z score at admission and weight gain (delta BMI z score) during hospitalization for male and female patients in the adolescent day unit.
Weight gain in subjects treated with monotherapy
Sixty-two subjects (42.5% of the cohort) were treated with monotherapy during the hospitalization. Thirty subjects were treated with selective serotonin reuptake inhibitors (SSRIs): fluoxetine (n=16), sertraline (n=7), citalopram (n=3), escitalopram (n=3), fluvoxamine (n=1). Eighteen subjects were treated with SGAs: risperidone (n=9), olanzapine (n=7), and aripiprazole (n=2); 3 subjects were treated with first-generation antipsychotics (FGAs) or mood stabilizers or other antidepressants; 2 subjects were treated with serotonin-norepinephrine reuptake inhibitors (SNRIs) or stimulants, and 1 subject was treated with clozapine. Because of the wide heterogeneity in drug families, we present only the data regarding the medication groups with >10 subjects: SSRIs (n=30) and SGAs (n=18). Age at hospitalization, length of stay, and male to female ratio were similar in both groups. The admission body weight of the SSRIs-treated subjects was larger (61.6 vs. 58.1 kg, respectively), whereas SGAs-treated subjects gained more weight than SSRIs-treated subjects during the hospitalization (mean weight gain was 5.9 kg and 3.0 kg respectively; delta BMI z scores were 0.5 and 0.3 respectively, p=0.018).
Patients with significant weight gain (delta BMI z score≥0.5)
Delta BMI z score was ≥0.5 in 26 out of 146 subjects (17.8%), most of them males (n=19, 73%). Normal weight status was documented in 24 out of 26 at admission and in 25 out of 26 at discharge. Out of the 26 patients with significant weight gain, only 9 used SGAs. Multivariate analysis, adjusting for variables that were found to be significant in a univariate analysis (age, use of antipsychotics, and major depression) showed that male gender had an odds ratio (OR) of 3.46 (95% CI: 1.159–10.338) to gain weight. and that BMI z score at admission was negatively correlated with weight gaining (β=−1.210, p<0.0001, OR 0.29 95% CI: 0.173–0.515) (Table 2). Comparison of changes in metabolic blood parameters during hospitalization between significant weight gainers and nongainers showed a difference only in the level of LDL (delta LDL 8.7 vs. −2.6, respectively, df=88, t=−2.17, p=0.032).
Discussion
This naturalistic historical prospective study examined the impact of sociodemographic, clinical, and pharmacological risk factors on weight gain and laboratory metabolic parameters in a sample of 146 adolescent patients hospitalized in a day care unit of a tertiary mental health center. Our results indicate that male subjects were more prone (3.5-fold) to gain weight than were female subjects adjusted for age, use of antipsychotic medications, and major depression. Weight gain during hospitalization was negatively correlated with the BMI z score at admission; that is, weight gain was significantly higher among subjects with normal body weight at admission whereas minimal change in BMI z score was observed among the overweight and obese subjects. Inappropriate weight gain was not related to the psychiatric diagnosis, age at hospitalization, number of psychotropic medications, or length of hospitalization.
Weight gain was defined as an increase of≥0.5 of BMI z score, because this value is a reliable indicator for inappropriate weight gain over time (Correll and Carlson 2006). In this study, only 26 subjects (17.8%) had significant weight gain. A recent review of weight gain in adolescents associated with antipsychotic medications (Maayan and Correll 2011) described more prevalent and pronounced weight gain reported in previous cohorts. One possible explanation is that these studies examined the impact of monotherapy, and were held in an outpatient setting. This discrepancy could be also accounted for by the ADU's routine of meals and physical activity, which could have a positive influence on the patients' regular habits.Taken together with our observation that fasting blood glucose and lipid profile at discharge remained unchanged compared with at admission, it is possible that a day care setting may have a protective value against weight gain, at least for some adolescent psychiatric patients.
Despite the significant weight gain of the cohort during hospitalization, the prevalence of overweight and obesity did not significantly change in the sample as a whole, or for any diagnostic group. This reflects the observation that significant weight gain occurred mainly in subjects with normal body weight (24 out of 26 weight gainers had normal body weight at admission). Our findings are in line with previous reports regarding SGAs (Ratzoni et al., 2002; Patel et al. 2004; Calarge et al. 2009) but a study on SSRIs (Michelson et al. 1999) did not demonstrate that relationship. Therefore, we suggest interpreting these findings with caution until more data are available. Interestingly, we showed that weight gain occurred not only in patients receiving SGAs, as only 9 out of the 26 patients with significant weight gain used SGAs. The current study expands the existent data from the perspective of showing this effect in a “real life” sample of adolescent patients with polypharmacotherapies, combining different medication groups.
Another finding of this study is that males had a 3.5-fold adjusted risk of gain weight compared with females. The previous few reports on gender difference in weight gain among adolescent patients varied in methodology (some cohorts included children mixed with teens), focused almost entirely on SGAs, and yielded conflicting findings (Martínez-Ortega et al. 2013). Female gender has been associated with a higher probability of antipsychotic-induced weight gain in several studies (Jerrell and McIntyre 2008; McIntyre and Jerrell 2008). In contrast, in subjects treated with risperidone or olanzapine, males were reported to be at greater risk for weight gain (Ratzoni et al. 2002), whereas in other studies no gender effect was observed (Martin et al. 2000; Ghate et al. 2013). Our study sheds more light on this important debate and may help to adopt gender-specific prevention strategies against inappropriate weight gain in adolescent psychiatric patients.
We found no association between the number of medications and weight gain. It is often recommended that polypharmacy be avoided because of a potential increase in side effects and low medication adherence (Jureidini et al. 2013), but our results indicate that weight gain does not necessarily ensue. However, we lacked power to analyze data regarding weight gain under certain combinations of medications. Future larger-scale studies would have to determine whether and to what extent popular pharmaceutical combination strategies are associated with increased weight gain in adolescent psychiatric patients.
The patients' primary psychiatric diagnosis was not a predictor of weight gain in our cohort. This finding is in line with previous studies (Moreno et al., 2010; de Hoogd et al. 2012). Therefore the efforts to prevent inappropriate weight gain should include all mental diagnoses. This is the second report of weight status in adolescent psychiatric day unit patients, giving a naturalistic reflection of the course of weight gain during day treatment in a mental health care center. The previous study (Gracious et al. 2010), describing a cross-sectional sample, showed that the prevalence of overweight and obesity was double the national rate, but yielded very few further findings regarding the risk factors for that weight gain in this population. ADUs are widely utilized globally, including in North America (Barwick and Boydell 2005; National Service on Drug Use and Health Report: Adolescent Mental Health: Service Settings and Reasons for Receiving Care 2009; Comprehensive Community Mental Health Services for Children and Their Families Program, Evaluation findings—Report to Congress, 2009, 2012) and particularly in Europe (World Health Organization 2011). Better understanding of weight change in this population, in whom polypharmacotherapy is very frequent, is important for developing appropriate recommendations and strategies to combat this phenomenon.
Limitations
Our study needs to be interpreted in light of several methodological limitations. First, we used a naturalistic uncontrolled design. However, we maintain that analysis of “real-life” data is extremely important when the contribution of randomized control trials of a single medication regimen may not reflect complex psychiatric disorders and pharmacotherapies. Second, the assessment was conducted at the beginning of hospitalization and at discharge and not at regular intervals. Nevertheless, because of the relatively large cohort and prolonged hospitalization, we believe that these results can help understand the nature of weight gain in this setting. Third, half of our subjects were treated with two or more medications. Therefore we had limited ability to examine the impact of different compounds and classes of medications on weight gain. Other limitations were the lack of data regarding previous exposure to medications with propensity to weight gain, information regarding patient history of physical or sexual abuse, their Tanner stage, and the absence of drug-naïve participants. Finally, it is clear that generalizability of findings from a single unit to the general adolescent psychiatric population is limited.
Conclusions
In this study, we demonstrated that male adolescent patients and those with normal weight at admission are in a higher risk for weight gain during psychiatric day treatment, whereas weight gain was not related to psychiatric diagnoses, age at hospitalization, the number of psychiatric medications, or length of hospitalization. These findings are of special importance because weight gain is a major risk factor for a metabolic syndrome later in life (Atlantis et al. 2014).
Weight gain in our cohort was less prominent than in previous adolescent studies; however, our cohort represented a naturalistic sample with multiple comorbidities, frequently receiving polypharmacotherapy. These findings are essential for adopting strategies to combat weight gain among adolescent psychiatric patients during day treatment in particular, and in other psychiatric settings in general.
The rate of increase in weight during adolescence has been shown to be associated with adverse metabolic and cardiac effects (Monteiro and Victora 2005; Sinaiko et al. 1999). Therefore, health providers should be aware of the tempo of the weight gain, not only of a patient's current weight status. Given the potential risk of weight gain to physical health, close monitoring of weight and metabolic indices should be implemented starting at treatment initiation and along continuation. Counseling on healthy dietary and lifestyle habits could also attenuate the development of severe health problems, and optimize patient metabolic outcomes (Correll 2008a,b).
Clinical Significance
Adolescents with psychiatric disorders are particularly vulnerable to weight gain, adverse metabolic changes, and subsequent metabolic syndrome. Therefore, preventing obesity and rapid weight gain among this population has become a major health concern. We report overall significant weight gain, especially in male adolescents compared with females (OR=3.5) and in those with normal weight at admission to our day unit. In light of the dearth of knowledge derived from prospective naturalistic data regarding weight gain and related clinical and laboratory parameters, our findings are important for identifying adolescent patients at risk for inappropriate weight gain, and for better understanding the development of metabolic syndrome in adolescent psychiatric patients.
Footnotes
Disclosures
No competing financial interests exist.