
Abstract
Objectives:
Unlike adult major depressive disorder (MDD) which requires anhedonia or depressed mood for diagnosis, adolescent MDD can be sufficiently diagnosed with irritability in the absence of the former symptoms. In addition, the current Diagnostic and Statistical Manual of Mental Disorders (DSM) schema does not account for the interindividual variability of symptom severity among depressed adolescents. This practice has contributed to the high heterogeneity and diagnostic complexity of adolescent MDD. Here, we sought to examine relationships between two core symptoms of adolescent MDD – irritability and anhedonia, assessed both quantitatively and categorically – and other clinical correlates among depressed adolescents.
Methods:
Ninety adolescents with MDD (51 females), ages 12–20, were enrolled. Anhedonia and irritability scores were quantified by summing related items on the Children's Depression Rating Scale-Revised and the Beck Depression Inventory. Extremes of score distribution were defined as high or low irritability/anhedonia subgroups. A significance level of p=0.01 was set to adjust for the five comparisons.
Results:
Despite all subjects exhibiting moderate to severe MDD, both irritability and anhedonia scores manifested a full and normally distributed severity range including the lowest values possible. However, only anhedonia severity was associated with more severe clinical outcomes, including greater overall illness severity (p<0.001), suicidality scores (p<0.001), episode duration (p=0.006), and number of MDD episodes (p=0.01). Similarly, only the high-anhedonia subgroup manifested more severe outcomes; specifically, greater illness severity (p<0.0001), number of MDD episodes (p=0.01), episode duration (p=0.01), and suicidality scores (p=0.0001).
Conclusions:
Our findings suggest the significance of anhedonia as a hallmark of adolescent MDD and the need to incorporate dimensional analyses. These data are preliminary, and future prospective studies are needed to better characterize the syndrome of adolescent MDD.
Introduction
A
Views on adolescent depression changed radically, so that current clinical wisdom led to the position that adolescent and adult MDD are indistinguishable, although it is also possible for secondary manifestations to differ as a function of age and brain development. The Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. (DSM-III), published in 1980, gave impetus to this view by requiring depressed mood or loss of interest as the sole, essential, and necessary clinical feature throughout development (American Psychiatric Association 1980). Coinciding with the publication of the DSM-III, systematic research in child and adolescent depression emerged, under the leadership of Joaquim Puig-Antich (Puig-Antich et al. 1978). The work had a strong influence, and was the source of the modification of the essential feature of MDD in children and adolescents. Specifically, the Diagnostic and Statistical Manual of Mental Disorders, 3rd ed., Revised (DSM-III-R), which appeared in 1987, introduced irritable mood as a cardinal symptom that could substitute for depressed mood in children and adolescents (American Psychiatric Association 1987; Ryan et al. 1987). Therefore, irritability sufficed and depressed mood was no longer required for diagnosing MDD in adolescents. This diagnostic standard has been maintained ever since; it appears unusual that irritability should be an essential feature of MDD in adolescence, while it is not even an associated clinical feature in adult MDD.
Such diagnostic classification can result in contrasting clinical phenotypes and may have augmented the heterogeneity of adolescent MDD. Similarly, it has contributed to the substantial failure to obtain consistent, well-replicated findings of the efficacy of psychotherapeutic and psychopharmacological treatments for adolescents with MDD (Bridge et al. 2009). In parallel, to minimize the conundrum of clinical heterogeneity, research in MDD has turned increasingly to the study of key features of depression (Gabbay et al. 2012a,b, 2013; Henderson et al. 2013). However, research investigating the clinical relevance of core symptoms in depressed youth is limited. In a population-based study, irritability among youth with MDD was associated with increased rates of disruptive disorders (Stringaris et al. 2013). Others have focused on anhedonia, which in adolescence, was identified as a predictor for MDD in adulthood (Pine et al. 1999; Wilcox and Anthony 2004). Anhedonia was also associated with greater illness severity in depressed preschoolers (Luby et al. 2004). Furthermore, Treatment of Resistant Depression in Adolescents (TORDIA), a multisite study of treatment-resistant adolescents with MDD, documented that anhedonia, assessed quantitatively, was the only clinical predictor of poor treatment response to antidepressant treatment/therapy (McMakin et al. 2012).
Building upon these observations, we sought to extend prior work to examine relationships between both irritability and anhedonia – assessed quantitatively and categorically – and other clinical correlates among depressed adolescents. To our knowledge, this is the first of such work, and, therefore, it will be a significant contribution to clinical practice. Based on our prior investigations in smaller samples (Gabbay et al. 2012a,b, 2013; Henderson et al. 2013), we hypothesized that: 1) Both anhedonia and irritability would be normally distributed and manifest the full distribution of symptom severity, and 2) anhedonia would be associated with increased illness severity measures; specifically, overall illness severity, level of suicidality and number of suicide attempts, current episode duration, and number of episodes. Directional hypotheses were not posited for irritability. We also explored other possible correlates with age, gender, body mass index (BMI), and ethnicity.
Methods
Study subjects
The sample consisted of 90 adolescents with MDD who were evaluated at pediatric mood and anxiety disorders research programs in the New York metropolitan area from 2004 to 2013. Prior to clinical evaluation, study procedures were explained to the subjects and the parents. Participants ≥ 18 years of age provided signed informed consent; those < 18 years of age provided signed assent, and a parent provided signed informed consent.
Inclusion and exclusion criteria
Adolescents ages 12–20 had to meet Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) criteria for MDD (American Psychiatric Association 2000) as well as having a current episode of at least 6 weeks' duration and a severity score of at least 35 on the Children's Depression Rating Scale-Revised (CDRS-R). Exclusionary criteria included current or past DSM-IV-TR diagnoses of bipolar disorder, schizophrenia, pervasive developmental disorder, obsessive-compulsive disorder, Tourette's disorder, or conduct disorder. Ongoing diagnoses of eating disorders, posttraumatic stress disorder, or a substance-related disorder in the past 12 months were also exclusionary.
Clinical assessments
All adolescents were assessed by a trained child and adolescent psychiatrist or psychologist using the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997), a semistructured, clinician-administered diagnostic interview performed with both the subjects and the parents. In addition, depression severity was assessed by the clinician-rated CDRS-R and the self-rated Beck Depression Inventory-Second Edition (BDI-II), and suicidality was quantified by the self-rated Beck Scale for Suicidal Ideation (BSSI). Furthermore, anxiety was measured using the self-rated Multidimensional Anxiety Scale for Children (MASC).
Irritability
Severity was quantified by summing one item reflecting irritability on the clinician-rated CDRS-R (item 8: “Irritability,” rated 1–7) and one from the self-rated BDI-II (item 17: “Irritability,” rated 0–3), with the total score potential ranging from 1 to 10. Low irritability scores were defined as irritability scores of 1–4, and high scores as ranging from 7 to 10.
Anhedonia
For all subjects, anhedonia severity was assessed by the sum of one item reflecting anhedonia in the clinician-rated CDRS-R (item 2: “Difficulty having fun,” rated 1–7) and two from the self-rated BDI-II (item 4: “Loss of pleasure,” rated 0–3, and item 12: “Loss of interest,” rated 0–3), with the total score potential ranging from 1 to 13. This approach to quantifying anhedonia has been used in our own as well as others' investigations (Gabbay et al. 2012a,b; McMakin et al. 2012; Gabbay et al. 2013; Henderson et al. 2013). Extremes of the score distribution define low- and high-anhedonia subgroups: 1–5 for low anhedonia, and 9–13 for high anhedonia.
Among patients enrolled within the last 2 years of the study, anhedonia was also rated via the Snaith–Hamilton Pleasure Scale (SHAPS), a 14 item self-report measure of anhedonia constructed to minimize age, sex, and cultural influences. The SHAPS is widely used as a quantitative measure of anhedonia, and has been validated in both clinical and nonclinical populations of adolescents and adults, making it a useful instrument as a dimensional measure of anhedonia. The SHAPS was collected on the same day as the CDRS-R and BDI-II.
Illness severity
CDRS-R was used for illness severity. However, when overall MDD severity was tested in relation to anhedonia and/or irritability, the specific questions used to quantify these symptoms were removed from the overall severity score.
Statistical analyses
Statistical analyses were computed using Minitab16 (Minitab Inc., State College, PA). Each parametric analysis was preceded by an assessment of its underlying assumptions, including a Ryan–Joiner test of normality. When the assumptions appeared unreasonable, a nonparametric analog of the proposed analysis was performed. To examine relationships between anhedonia/irritability and illness severity (i.e., overall illness severity, suicidality scores, duration of current MDD episode, number of episodes, and past suicide attempts), Pearson/Spearman correlations and bivariate logistic regressions were applied for continuous and dichotomous outcome variables, respectively. Additionally, generalized linear models and bivariate logistic regressions were used with both irritability and anhedonia entered into the model as predictors of the outcome variables. Mann–Whitney and χ2 tests were used to assess differences between low and high levels of anhedonia and irritability. Exploratory analyses examined associations between both anhedonia and irritability with age, BMI, gender, and ethnicity. Depending on the nature of the data, correlations, t tests and χ2 tests were applied.
To address multiple comparisons, each set of analyses accounted for the five comparisons (overall illness severity, suicidality scores, current episode duration, number of past MDD episodes, and past suicide attempts), with a Bonferroni-corrected α value of 0.01.
Results
Participants
Sample characteristics are summarized in Table 1.
Includes generalized anxiety disorder and social phobia.
Respective percentages do not add up to 100% because of rounding.
CDRS-R, Children's Depression Rating Scale, Revised; BDI-II, Beck Depression Inventory, Second Edition; BSSI, Beck Scale for Suicidal Ideation; MASC, Multidimensional Anxiety Scale for Children; ADHD, attention-deficit/hyperactivity disorder.
Distribution of irritability and anhedonia
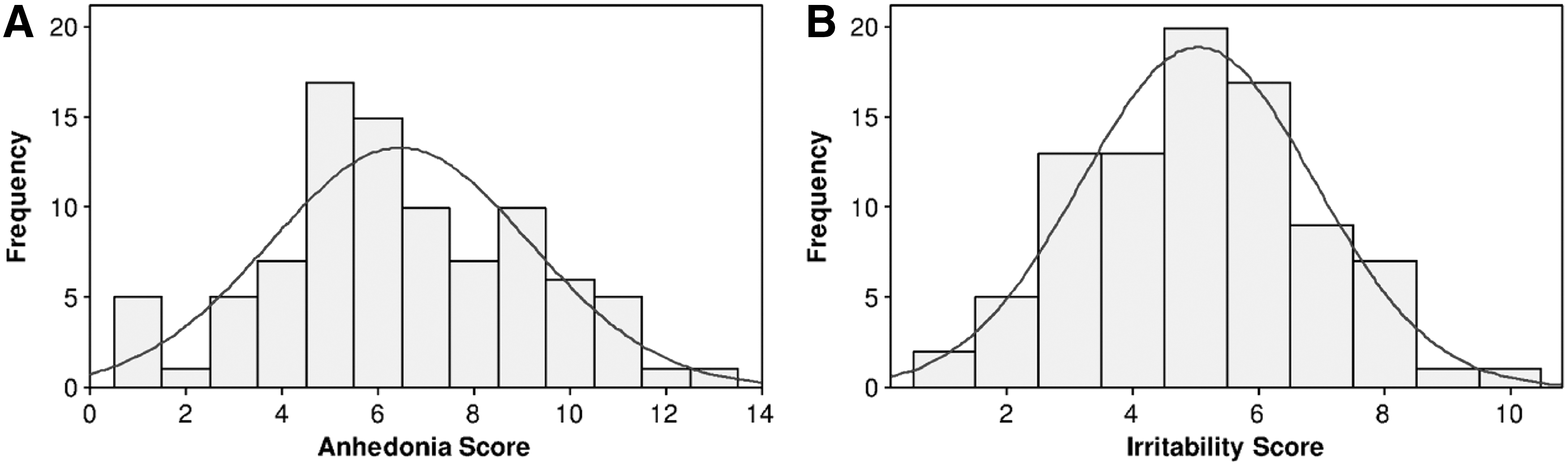
Severity ranges for irritability (mean [SD], 5.03 [1.85], range: 1–10) and anhedonia [6.46 (2.70), range: 1–13] were wide and normally distributed. Anhedonia and irritability were significantly correlated (Pearson r[86]=0.28, p=0.008). SHAPS scores of anhedonia and anhedonia ratings (adding CDRS-R and BDI-II items) were significantly correlated (Pearson r[22]=0.65, p=0.001) (FIG. 1).
Irritability as a correlate of adverse clinical features
Irritability was not significantly correlated with any of the measures of illness severity examined.
Anhedonia as a correlate of adverse clinical features
As we hypothesized, anhedonia severity was significantly correlated with illness severity measures, including overall illness severity (computed by CDRS-R without the anhedonia question; Spearman r[88]=0.59, p<0.001) (FIG. 2A); suicidality scores (Spearman r[86]=0.45, p<0.001) (FIG. 2B), as well as the duration of the current MDD episode (Spearman r[86]=0.27, p=0.010) (FIG. 2C). There was no association with number of MDD episodes or number of past suicide attempts.

Irritability and anhedonia in the model
When both anhedonia and irritability were entered into the model, only anhedonia severity was significantly associated with overall illness severity (F[1,85]=42.73, p<0.001), suicidality scores (F[1,83]=20.84, p<0.001), duration of the current episode (F[1,83]=8.02, p=0.006), and number of MDD episodes (df=85, odds ratio [OR]=1.32, p=0.01). No significant association was found with suicide attempts. Irritability was not significantly associated with any clinical measure of illness severity.
Clinical comparison between patients with low and those with high irritability
Clinical and demographic characteristics of the subgroups are summarized in Table 2. The low and high irritability groups did not differ in overall illness severity; however, those with high irritability manifested greater anhedonia than those with low irritability (Mann–Whitney U statistic: U[49]=720.5, p=0.007). No other differences with respect to illness severity measures were found.
P value indicates significance of difference between the two subgroups. Significance level at p≤0.01 and p≤0.001 are indicated by * and **, respectively.
Respective percentages do not add up to 100%, because of rounding.
Children's Depression Rating Scale, Revised score without the irritability-related item.
Includes generalized anxiety disorder and social phobia.
MDD, major depressive disorder; BSSI, Beck Scale for Suicidal Ideation; MASC, Multidimensional Anxiety Scale for Children; ADHD, attention-deficit/hyperactivity disorder.
Clinical comparison between patients with low and those with high anhedonia
Clinical and demographic characteristics of the subgroups are summarized in Table 3. As was found in the correlational analyses, the high anhedonia subgroup exhibited significantly higher illness severity measures including higher overall illness severity (U[56]=745.0, p<0.0001), greater number of MDD episodes (χ2[1, n=58]=6.3, p=0.01), and greater duration of the current episode (U[55]=832.0, p=0.01). In addition, the high anhedonia subgroup revealed significantly higher suicidality scores (U[55]=743.0, p=0.0001), but no relative excess of suicide attempts.
P value indicates significance of difference between the two subgroups. Significance level at p≤0.01 and p≤0.001 are indicated by * and **, respectively.
Children's Depression Rating Scale, Revised score without the anhedonia-related item.
Includes generalized anxiety disorder and social phobia.
MDD, major depressive disorder; BSSI, Beck Scale for Suicidal Ideation; MASC, Multidimensional Anxiety Scale for Children; ADHD, attention-deficit/ hyperactivity disorder.
Exploratory associations with gender, age, ethnicity, and BMI
None of these characteristics were associated with level of anhedonia or irritability.
Discussion
This cross-sectional study supported the hypothesis that depressed adolescents would exhibit a wide and normally distributed severity range of irritability and anhedonia. Findings documented that anhedonia, but not irritability, whether assessed quantitatively or categorically, was associated with increased overall illness severity, suicidality scores, illness duration, and number of MDD episodes.
Our findings that anhedonia and irritability – two core symptoms of adolescent MDD – manifest a normally distributed, wide severity range that includes the lowest values possible (comparable with those of healthy nondepressed individuals) replicates our prior findings in our small sample of biological studies (Gabbay et al. 2012a,b, 2013; Henderson et al. 2013). Such findings underscore the need to take into account the interindividual variability of symptom severity both in biological and intervention studies in adolescents with MDD (Insel et al. 2010).
Anhedonia, but not irritability, was associated with more severe illness outcomes. The relationship of anhedonia with overall illness severity was reported in hospitalized adolescents (Gutkovich et al. 2011) and in preschoolers with depression (Luby et al. 2004). Similarly, a significant positive relationship between anhedonia severity and suicidality was found among hospitalized youth regardless of their diagnoses (Robbins and Alessi 1985; Nock and Kazdin 2002). Our study extends these findings to depressed outpatient adolescents. In addition, research with depressed adults documented similar relationships (Fawcett et al. 1983, 1990; Spijker et al. 2010), with one exceptional study that found that low anhedonia was associated with completed suicide (Loas 2007). Our finding of a positive association between MDD episode duration and anhedonia severity is consistent with a report from the TORDIA study that anhedonia was the only feature to predict longer time to remission (McMakin et al. 2012). We did not find BMI differences between the high/low anhedonia patient groups nor any relationship between anhedonia and BMI, measured continuously. This finding seems unexpected since low-anhedonia patients exhibit reactive mood and often fit the diagnosis of atypical depression, which is characterized by increased appetite. However, this diagnosis is based on adult clinical presentation; adolescents may have different patterns of clinical function because of their documented distinct appetite/metabolism habits from adults. It may also be that anhedonic patients are less physically active resulting in higher than expected BMI. Our group of depressed adolescents as a whole scored at the high end of the normal BMI range (mean=24.09 compared with the normal BMI range of 18.5–24.9).
Our findings in relation to irritability in the context of pediatric MDD are consistent with those of a recent large epidemiological study (n=1420) which found no differences between depressed youth with and without irritability, with respect to illness severity, number of depressive episodes, anhedonia, or suicidality (Stringaris et al. 2013). Authors also reported that irritability by itself without depressed mood was rare among depressed youth, a finding reported in depressed adults as well (Fava et al. 2010).
Importantly, irritability is highly prevalent in many pediatric and adult psychiatric disorders and constitutes a core symptom of mania; the polar opposite of depressed mood. The classification of disruptive mood dysregulation disorder (DMDD) (Leibenluft 2011) and the tripartite delineation of oppositional defiant disorder (ODD) to include an irritable cluster (Stringaris and Goodman 2009) in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-V) have added to the clinical complexity associated with irritability (American Psychiatric Association 2013). Similarly, several investigations in youth and adults report associations between irritability in the context of MDD, and disruptive and substance-related disorders (Fava et al. 2010; Judd et al. 2013; Stringaris et al. 2013).
As a whole, our work suggests that anhedonia, and not irritability, is associated with more severe adolescent MDD illness.
Limitations
Several limitations are noted. First, the cross-sectional study design does not provide longitudinal data to ascertain predictive value, an essential aspect of diagnostic validity. Additionally, although our sample is comparable in size to samples in other studies, it is still modest. Furthermore, our scales for anhedonia and irritability were derived from other scales. However, the high correlation between the SHAPS and our anhedonia rating suggest that, at least for anhedonia, the method is adequate. Despite these limitations, our results appear sensible, as this study involves a well-characterized group of adolescents with moderate to severe MDD of at least 6 weeks' duration, assessed using validated diagnostic procedures performed by a trained psychiatrist/psychologist. Further, the application of multiple comparison correction limits the chances of a type I error. We look forward to attempts at replication.
Conclusions
To our knowledge, this is the first study to focus on anhedonia and irritability simultaneously in adolescents with MDD using both a dimensional and categorical approach. Our results support our hypothesis that both symptoms would manifest a wide range of severity and provide further support to the inclusion of dimensional analyses in psychiatric research. Our finding that only anhedonia was associated with more severe illness outcomes suggests that anhedonia is a more significant core symptom of adolescent MDD than irritability.
Our findings have important public health implications. All clinicians who evaluate and treat adolescents with MDD should assess the severity of anhedonia and provide careful monitoring to severely anhedonic patients. Future prospective studies that determine potential biological markers, specific phenomenological features, and the clinical course of adolescents with MDD are needed.
Clinical Significance
Unlike adult MDD, adolescent MDD includes irritability as a core symptom in addition to anhedonia and depressed mood. The present study is the first to examine both anhedonia and irritability as correlates of clinical outcomes among depressed adolescents. Utilizing both a categorical and dimensional analytic approach, we report that only anhedonia was associated with greater overall illness severity, suicidality, and illness duration. Our findings suggest the significance of anhedonia, but not irritability, as a hallmark of adolescent depression. This further emphasizes the importance of closely monitoring highly anhedonic depressed adolescents.
Footnotes
Acknowledgments
We thank Ana Vallejo and Timothy Rice of the Icahn School of Medicine for their assistance with this project.
Disclosures
No competing financial interests exist.