
Abstract
Objective:
Offspring of parents with bipolar disorder (BD) have been shown to be at high risk for BD. Anxiety symptoms, even at subclinical levels, have been associated with increased risk for BD in these youth. The s-allele of the serotonin transporter-linked polymorphic region (5-HTTLPR) has been implicated in the pathophysiology of both BD and anxiety disorders and has been associated with pharmacological treatment response and increased risk for antidepressant side effects. Therefore, we aimed to explore 1) whether anxiety symptoms in offspring of BD parents were associated with presence of the 5-HTTLPR s-allele and 2) whether anxiety symptoms in the offspring of BD parents according to the 5-HTTLPR genotypes are related to antianxiety medication status.
Methods:
A total of 64 offspring of BD parents (mean age: 13.7 years) and 51 healthy controls (HC) (mean age: 13.7 years) were compared genetically and on the Multidimensional Anxiety Scale for Children (MASC).
Results:
Offspring of BD parents showed higher levels of overall anxiety than did the HC group. Only antianxiety medication naïve offspring of BD parents were found to have an association between 5-HTTLPR genotypes and anxiety symptoms. The antianxiety medication naïve offspring of BD parents with the s-allele showed higher level of overall anxiety than offspring of BD parents with the l/l genotype. No significant differences in anxiety symptoms or their association with the 5-HTTLPR genotype were found in the HC group.
Conclusions:
This study indicated that there may be an association between 5-HTTLPR genotypes and anxiety symptoms in offspring of BD parents, and that antianxiety medication status may affect anxiety symptoms in the offspring of BD patients according to genotype.
Introduction
C
The serotonin transporter gene (SLC6A4) has been implicated in the pathophysiology of anxiety disorders (Lesch et al. 1996; Lapalme, et al. 1997; Hariri et al. 2002; Heinz et al. 2005; Munafò et al. 2008; Surguladze et al. 2008) and mood disorders including BD (Cho et al. 2005; Kenna et al. 2012). The serotonin transporter-linked polymorphic region (5-HTTLPR) is the most studied serotonergic gene polymorphism in psychiatric behavioral genetics (Margoob and Mushtaq 2011). The l-allele of the 5-HTTLPR is associated with a relative acceleration of serotonin reuptake and the subsequent decreased concentration of serotonin in synapse, whereas the s-allele is associated with decreased serotonin reuptake (Lesch et al. 1996). Most studies that have examined the association between the response to selective serotonin reuptake inhibitors (SSRIs) and the 5-HTTLPR genotypes in patients with depression or anxiety have reported that the s/s genotype or s-allele is related to a poor response, because serotonin transporter activity is depressed; therefore, if additional SSRIs are administered, it is impossible to expect an additional decrease in serotonin transporter activity because of the floor effect (Murphy et al. 2004). Serotonin receptors are a common target of pharmacotherapy for anxiety (Roerig 1999) and mood disorders (Kenna et al. 2012). Furthermore, the serotonin transporter (5-HTT) is abundantly distributed throughout the brain and most highly expressed in medial structures such as the amygdala (Du et al. 2000), which is principally involved in anxiety states and emotional regulation (Davidson 2002).
Although anxiety symptoms may serve as a predisposing factor for BD development in offspring of BD parents, and the 5-HTTLPR polymorphism is thought to be implicated in both BD and anxiety, no previous study has investigated the relation between anxiety symptoms and the 5-HTTLPR genotype in offspring of BD parents. Furthermore, the 5-HTTLPR genotype may moderate antianxiety medication response and risk for adverse effects (Kronenberg et al. 2007).
Therefore, we aimed to examine 1) whether the offspring of BD parents group would show higher anxiety than the healthy control (HC) group, 2) whether the 5-HTTLPR s-allele is associated with higher anxiety symptoms, and 3) whether anxiety symptoms in the offspring of BD parents are affected by their antianxiety medication status, according to the 5-HTTLPR genotype.
Methods
Participants
The protocol was approved by the Stanford University Panel of Medical Research in Human Subjects. One hundred BD offspring and 60 HC were recruited from an ongoing study of youth at risk for BD and from the community. After obtaining oral and written informed consent and assent from parents from their offspring, respectively, we conducted semistructured interviews to assess for BD in parents and psychopathology in their offspring. Parents were diagnosed using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) (First et al. 1996), and were interviewed for psychiatric history of first- and second-degree relatives following the Family History-Research Diagnostic Criteria (FH-RDC) (Andreasen et al. 1977). BD offspring were assessed using the Affective Disorders Module of the Washington Schedule for Affective Disorders and Schizophrenia for School-Age Children (WASH-U-KSADS) (Geller et al. 2001) and Kiddie-SADS-Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997). All evaluations were conducted by either a child and adolescent psychiatrist or a trained master's level research assistant with at least 2 years' experience in psychiatric interviewing. Evaluators were aware of parental diagnoses, and parents were interviewed while they were euthymic at the time of their child's assessment. Interrater reliability was established by rating videotaped interviews, observing trained rater interviews, and performing interviews with observation by a trained rater. Diagnostic decisions were ultimately made by a board-certified child and adolescent psychiatrist (K.C. or M.S.) based on personal interview, discussion with the research assistant, and written notes of parent and offspring responses to interview questions. Current and lifetime diagnoses were established according to Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria (American Psychiatric Association 1994).
Youth 9–17 years of age who had at least one biological parent with BD were included in the BD offspring group. BD offspring with the following disorders or conditions were excluded: BD I or II, schizophrenia, pervasive developmental disorder, Tourette's disorder, substance use disorder, obsessive-compulsive disorder (OCD), panic disorder, or a neurological condition (such as a seizure disorder). HC had no personal or parental psychiatric history and no family history of BD, and were excluded with current Young Mania Rating Scale (YMRS) (Young et al. 1978) scores >8 or Childhood Depression Rating Scale (CDRS-R) (Poznanski et al. 1985) >26.
Multidimensional Anxiety Scale for Children (MASC)
To assess anxiety symptoms, we used the MASC (March et al. 1997), a 39 item scale, distributed into four major factors: physical symptoms, social anxiety, harm avoidance, and separation anxiety. The MASC has been shown to reliably distinguish anxiety from depression, and to differentiate various anxiety disorders (Dierker et al. 1999).
Genotyping
DNA was extracted from 200 uL of frozen blood using the QiagenDNeasy Kit (Qiagen, Hilden, Germany [Cat. #69506]). Oligonucleotide primers flanking the 5-HTT-linked polymorphic region and corresponding to the nucleotide positions −1416 to −1397 (stpr5, 5′-GGC GTT GCC GCT CTG AAT GC) and −910 to −888 (stpr3, 5′-GAG GGA CTG AGC TGG ACA ACC AC) of the 5-HTT gene 5′-flanking regulatory region were used to generate 484 bp or 528 bp fragments. Polymerase chain reaction (PCR) amplification was conducted in a final volume of 30 uL, consisting of 50 ng of genomic DNA, 50 ng each of sense and antisense primers, 15 uL of Taq PCR Master mix (Qiagen, Cat.#201445), 10% dimethyl sulfoxide (DMSO), and 1 mol/L betaine. Annealing was performed at 61°C for 30 seconds, extension was performed at 71°C for 1 minute, and denaturation was performed at 95°C for 30 seconds, for a total of 35 cycles. The PCR products were electrophoresed through 5% polyacrylamide gel (acrylamide/bis-acrylamide ratio19:1) at 60 V for 60 minutes. A 100 bp marker was used to measure the PCR product size for the l- and s-alleles. Alleles were called by raters blind to clinical status of the participant.
Statistical analysis
To compare categorical variables, we conducted χ2 tests. To compare continuous variables, we conducted independent t tests for parametric data, and Mann–Whitney U tests for nonparametric data. To compare subjects with different genotypes (s/s vs l/s vs l/l), we conducted a three way ANOVA with post-hoc Tukey (b) tests. The initial three groups sorted by genotype were then redivided into two groups of offspring of BD parents dichotomized by the presence of or absence of the s-allele. This method has been used in previous studies to determine the effect of having at least one s-allele (Kaufman et al. 2004, 2006). The statistical significance for all tests was set at p<0.05. We corrected significance levels for multiple comparisons using a Bonferroni correction (0.05/5 comparisons=0.01).
Results
Among 100 offspring of BD parents and 60 HC, 35 offspring of BD parents and 9 HC were excluded because of incomplete MASC data (34 offspring of BD parents and 9HC) or genotyping failure (1 offspring of BD parents), leaving 64 offspring of BD parents (mean age, 13.7 [SD 3.45); males=30, females=34) and 51 HC (mean age, 13.68 [SD 2.68]; males=23, females=28) to be included as subjects for statistical analysis. Among the total of 64 offspring of BD parents, 37 (57.8%) showed subthreshold mood symptoms (YMRS>12 or CDRS>27). The offspring of BD parents group had significantly higher anxiety scores than HC in the physical subscale (p=0.001) and the social anxiety subscale (p=0.037), as well as in the overall MASC score (p=0.018). Results for the physical subscale and MASC total scores remained significant after adjusting for multiple comparisons (Fig. 1a). Participant demographic and clinical characteristics are provided in Table 1. In the offspring of BD parents group, the l/l genotype of the 5-HTTLPR was observed in 19 subjects (29.7%), the l/s genotype was observed in 30 subjects (46.9%), and the s/s genotype was observed in 15 subjects (23.4%). In the HC group, the l/l genotype was observed in 8 subjects (15.7%), the l/s genotype was observed in 28 subjects (54.9%), and the s/s genotype was observed in 15 subjects (29.4%) in the HC group. The distributions of genotypes for the 5-HTTLPR polymorphism were consistent, with expected values based on Hardy–Weinberg equilibrium in both the offspring of BD parents (p=0.64) and HC groups (p=0.40).

Anxiety symptoms differences
BD, bipolar disorder; CDRS, Children's Depression Rating Scale; MASC, Multidimensional Anxiety Scale for Children; YMRS, Young Mania Rating Scale.
There was no significant difference in the current usage of antianxiety medications (Table 2) among the three 5-HTTLPR genotype groups. Similarly, there was no significant difference in the current usage of stimulant medications, which may have anxiogenic properties. Among the offspring of BD parents not currently taking antianxiety medications, no one had a past history of antianxiety medication use. In other words, there were no offspring of BD parents who had formerly taken antianxiety medication who were not current antianxiety medication users in this study. Therefore, we were able to dichotomize the offspring of BD parents group into those who were taking antianxiety medications and those who were antianxiety medication naïve. The offspring of BD parents who were taking antianxiety medications generally showed higher anxiety than the offspring of BD parents who were not taking antianxiety medications (Supplementary Table S1) (see supplementary material in the online article at
ADHD, attention-deficit/hyperactivity disorder; BD, bipolar disorder; CDRS, Children's Depression Rating Scale; GAD, generalized anxiety disorder; NOS, not otherwise specified; ODD, oppositional defiant disorder; SSRI, selective serotonin reuptake inhibitor; YMRS, Young Mania Rating Scale.
Comparisons by 5-HTTLPR genotype (s/s vs. l/s vs. l/l)
Analysis of the entire study group showed no significant difference in the MASC scores by 5-HTTLPR genotype. Similarly, neither the offspring of BD parents nor the HC group showed a significant difference in the MASC scores by the 5-HTTLPR genotype within each group. However, when we excluded offspring of BD parents currently taking antianxiety medication, certain trends in anxiety patterns according to genotype appeared. The antianxiety medication naïve offspring of BD parents with both the s/s (n=15) and l/s (n=30) genotypes reported higher levels of anxiety than the offspring of BD parents with the l/l (n=19) genotype, except in the harm avoidance subscale.
The symptom patterns observed in the offspring of BD parents were not observed in the HC group except in the social anxiety subscale (Fig. 2), where social anxiety symptoms tended to be greater (trend) in those with the s-allele in both the offspring of BD parents and HC groups.
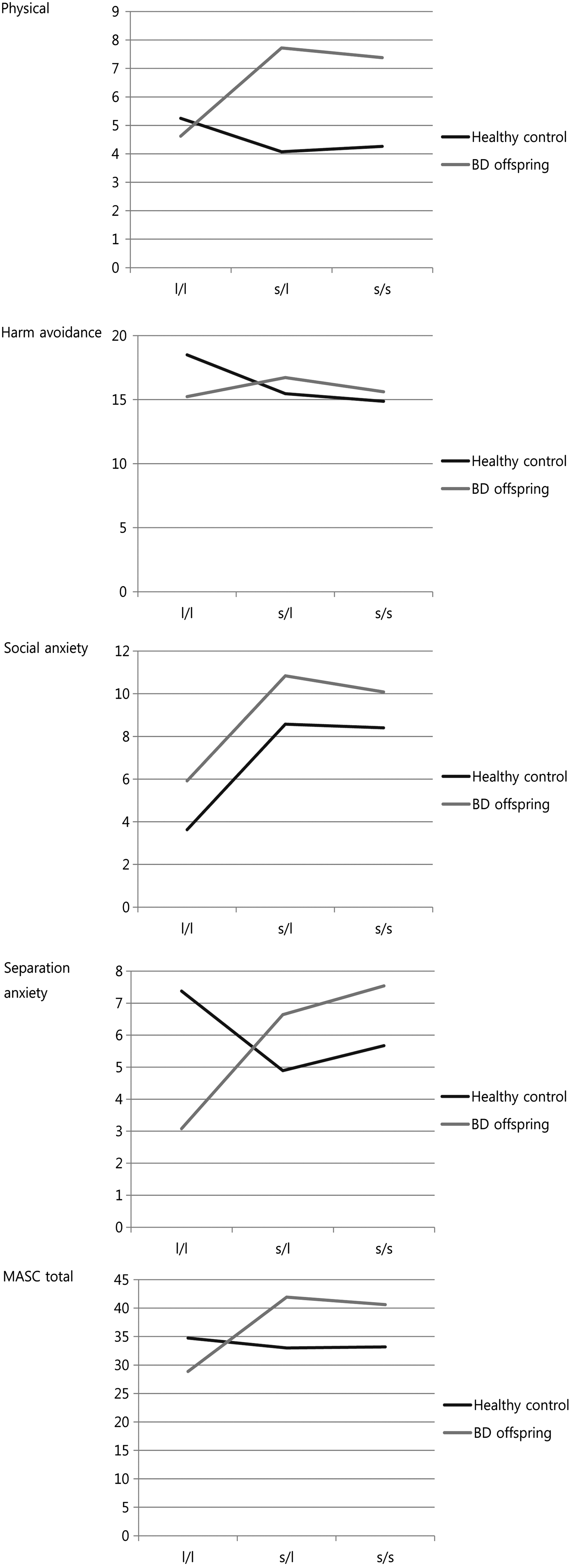
Anxiety symptoms according to 5-HTTLPR genotype.
Comparisons according to presence of an s allele (l/l vs. l/s+s/s)
When dichotomized according to presence or absence of the s-allele (l/l vs. l/s+s/s), no significant difference was observed in the MASC scores according to presence of the s-allele in either the entire study group or the HC group. After excluding the offspring of BD parents taking antianxiety medications (n=13), we examined only the remaining offspring of BD parents who were naïve to antianxiety medications (n=51). Within this latter group, offspring of BD parents with at least one s-allele had significantly higher MASC anxiety scores than offspring of BD parents without the s-allele in the social anxiety subscale (p=0.020), separation anxiety subscale (p=0.022), and total MASC score (p=0.013) (Fig. 1b). Results for the MASC total scores remained significant after adjusting for multiple comparisons (Table 3). However, when we examined only the offspring of BD parents currently taking antianxiety medication, no significant differences were observed in the MASC scores by presence/absence of the s-allele.
Corrected by CDRS.
BD, bipolar disorder; CDRS, Children's Depression Rating Scale; MASC, Multidimensional Anxiety Scale for Children; YMRS, Young Mania Rating Scale.
Discussion
In this study, the offspring of BD parents group demonstrated higher anxiety levels than the HC group, which was to be expected, given that 57.8% of the offspring of BD parent subjects were recruited for presence of mood dysregulation.
In addition, antianxiety medication naïve offspring of BD parents with at least one s-allele had higher reported anxiety than antianxiety medication naïve offspring of BD parents without an s-allele.
Concerning the relationship between BD and the 5-HTTLPR genotypes, even though some studies have shown negative results, meta-analytic results (Cho et al. 2005; Lasky-Su et al. 2005; Jiang et al. 2013) have consistently reported that the presence of the s-allele has a significant association with BD, albeit the effects sizes are mostly small.
Regarding the relationship between anxiety and the 5-HTTLPR genotypes, studies on anxiety manifestations below clinical disorder level, such as subclinical anxiety symptoms or anxiety traits, have shown relatively consistent results, and found that s-allele carriers tend to have increased anxiety-related temperament traits (Lesch et al. 1996; Mazzanti et al. 1998; Katsuragi et al. 1999; Osher et al. 2000; Melke et al. 2001; Jacob et al. 2004; Schinka et al. 2004; Sen et al. 2004; Calapoğlu et al. 2011), although a few studies have reported negative results (Willis-Owen et al. 2005; Middeldorp et al. 2007; Munafò et al. 2009) and Jorm et al. (2000) reported the l-allele as being a risk allele. However, the studies on clinical level anxiety disorder, such as panic disorder (Deckert et al. 1997; Ishiguro et al. 1997; Matsushita et al. 1997; Maron et al. 2005; Martinez-Barrondo et al. 2005; Blaya et al. 2007; Lonsdorf et al. 2009; Strug et al. 2010), generalized anxiety disorder (Samochowiec et al. 2004), social anxiety disorder (Strug et al. 2010), generalized social phobia (Ohara et al. 1998; Stein et al. 1998), and OCD (McDougle et al. 1998; Bengel et al. 1999; Hamilton et al. 1999) have shown conflicting results. Therefore, high scores on subscales of trait anxiety may be related to the subclinical range of anxiety symptoms that may place youth at high risk for BD.
That youth may be biologically predisposed to developing anxiety is supported by functional magnetic resonance imaging (fMRI) studies on the relationship between the 5-HTTLPR genotype and amygdala activity, which have consistently shown that s-allele carriers have significantly greater amygdala excitability than individuals with other genotypes (Hariri, et al. 2002; Heinz, et al. 2005; Munafò, et al. 2008; Surguladze, et al. 2008). The 5-HTTLPR genotype-mediated effect on brain region excitability was specific to the amygdala (Hariri et al. 2002), and as amygdala excitability plays a role as an intermediate phenotype of anxiety symptoms (Davidson 2002; Blackford and Pine 2012), it may be that amygdala excitability may be a mediating factor that links genotype with anxiety symptoms.
Interestingly, in our study, the association between increased anxiety and the presence of the s-allele was only observed in the antianxiety medication naïve offspring of BD parents group in this study. To understand this finding, we need to first comment on the characteristics of BD offspring and the role of antianxiety medication in BD offspring by the 5-HTTLPR genotype. Key gene-by-environment interactions may be leading to epigenetic modulation in BD offspring. Specifically, the BD offspring group is subject to not only genetic risk factors but also to environmental risk factors such as parent–child relationship problems that result from parents' illnesses (Chang et al. 2001). The presence of the s-allele of 5-HTTLPR polymorphism plays a role as a risk factor for the development of depression or anxiety, especially in individuals with stressful life events (Caspi et al. 2003; Eley et al. 2004; Kaufman et al. 2004; Kendler 2005; Kaufman et al. 2006; Stein et al. 2008; Karg et al. 2011), which are common among BD offspring (Moreno et al. 2012).
Second, one needs to consider the effect of antianxiety medications by 5-HTTLPR genotype. Except in some studies with Asian populations (Yoshida et al. 2002; Kim et al. 2003), antidepressant effectiveness by the 5-HTTLPR genotype in adults with depression (Smeraldi et al. 1998; Pollock et al. 2000; Zanardi et al. 2000, 2001; Durham et al. 2004) and anxiety (Perna et al. 2005; Stein et al. 2006) have found that individuals with the s/s genotype show poorer response to antidepressants than do individuals with other 5-HTTLPR genotypes. However, a study with children and adolescents with depression and/or anxiety (Kronenberg et al. 2007) found that the s/s genotype was associated with poor antidepressant treatment response only to depressive symptoms but not anxiety symptoms. Further, animal studies have shown that, unlike the anxiolytic effects of antidepressants in adults (Holick et al. 2008), antidepressant exposure during adolescence appears to have anxiogenic rather than anxiolytic effects (Oh et al. 2009; Warren et al. 2011). Moreover, studies with children and adolescents with depression or anxiety disorders have reported high rates of agitation or anxiety-like symptoms during antidepressant treatment (Rey-Sánchez and Gutiérrez-Casares 1997; March et al. 1998; Ambrosini et al. 1999; Cook et al. 2001; Emslie et al. 2002; Braconnier et al. 2003; Wagner et al. 2003). For example, Kronenberg et al. (2007) found that depressed children and adolescents with the s/s genotype showed a low agitation rate as a side effect of citalopram treatment.
Our study showed that BD offspring treated with antianxiety medication had higher anxiety symptoms than BD offspring who were antianxiety medication naïve, suggesting that some of BD offspring might not show full response to antianxiety medication or may be vulnerable to developing anxiety-like symptoms as a side effect of treatment. Further, antianxiety medication treatment may alleviate the 5-HTTLPR genotypes' moderating effect on anxiety symptoms regardless of whether this possibility results from poor treatment response or side effects.
Finally, BD offspring with the s-allele had a subclinical range of anxiety symptoms. It is possible that such subclinical anxiety symptoms may represent prodromal symptoms of BD (Chang 2010). Importantly, subsyndromal manic symptoms can be mistaken for anxiety symptoms. BD offspring are at relatively high risk for the development of manic symptoms (Baumer et al. 2006; Strawn et al. 2014), and subsyndromal manic symptoms commonly first manifest as motor hyperactivity or irritability (Strawn et al. 2014). Furthermore, it is unclear whether mood instability or irritability during pharmacological treatment results from medication side effects or indicates bipolar psychopathology (Faedda et al. 2004) in BD offspring taking medications that exacerbate anxiety symptoms.
Limitations
First, although there is a high possibility of epigenetic and gene–gene interaction effect, we only examined anxiety symptoms and the 5-HTTLPR polymorphism of the 5-HTT gene in the offspring of BD parents and HC. We did not evaluate environmental risk factors such as parent–child relationships, traumatic life events, or levels of early life stress. We also did not look at other genetic polymorphisms, which may interact with the 5-HTT gene. Second, this study is a cross-sectional study that will require longitudinal follow-up to determine whether trait anxiety predicts conversion to BD in youth at familial risk. Furthermore, because of this study's cross-sectional nature and the lack of follow-up concerning the response to antianxiety medication or side effects, we could not fully investigate the alleviating effect of antianxiety medication on the 5-HTTLPR genotypes' moderating effect on anxiety symptoms. Third, the number of subjects was relatively small for genetic analysis, and our sample contained multiple ethnic groups. However, our results did not change significantly when we re-analyzed our data after excluding non-Caucasian participants.
Conclusion
This study found an association between the 5-HTTLPR genotype and anxiety symptoms in BD offspring not exposed to antianxiety medications. Future longitudinal studies may confirm whether or not anxiety symptoms and certain 5-HTTLPR genotypes serve as risk factors for the development of BD in high-risk offspring. Studies that monitor symptom change in high-risk youth may capture subtle changes that may occur at a very early age. Other possible risk factors such as gene–gene interaction and genetic–environmental interactions should also be examined longitudinally. Pharmacological treatment response and side effects according to 5-HTTLPR genotype should also be explored. There have been some preliminary studies that have explored these relationships (Stein et al. 2006; Kronenberg et al. 2007). However, those studies have shown conflicting results, and the number and sample sizes of these studies are small. Finally, because BD offspring may be at high risk for manic switching, pharmacogenetic studies may aide in determining which youth are most likely to benefit from certain pharmacotherapies, and which youth may develop adverse reactions to them. Early identification of these comprehensive risk factors will enable clinicians to intervene earlier with the hope of preventing poor outcomes in these youth (Chang et al. 2003b).
Clinical Significance
This study indicated that there may be an association between 5-HTTLPR genotypes and anxiety symptoms in offspring of BD parents. Antianxiety medication status may affect anxiety symptoms in the offspring of BD patients according to genotype. Therefore, youth at high risk for BD who are not treated for anxiety may present with increased anxiety symptoms based on their 5-HTTLPR genotype. Such presentation may place them at even higher risk for development of BD.
Footnotes
Acknowledgments
We thank the participants who gave their time for this study.
Disclosures
Dr. Chang is a consultant for Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, and Sunovion, and has received research support from GlaxoSmithKline and Merck in the last two years. The other authors have nothing to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.