
Abstract
Background:
Obsessive-compulsive disorder (OCD) is a relatively frequent disease in childhood, which is generally treated with selective serotonin reuptake inhibitors (SSRIs) and/or clomipramine and cognitive behavioral therapy (CBT). However, nearly half of the cases are treatment resistant. Aripiprazole was shown to be beneficial in augmentation therapy in treatment-refractory OCD. This study evaluated its effectiveness as a single agent in these cases.
Methods:
Sixteen children (nine girls, seven boys), who were nonresponders to treatment with at least two types of SSRIs and CBT, were administered 12 weeks of aripiprazole treatment with a mean dose of 4.75 mg/day (range: 2–7.5 mg/day). Treatment outcomes were evaluated by the Childhood Yale-Brown Obsessive Compulsive Scale (CY-BOCS), and the Clinical Global Impressions-Severity and Improvement (CGI-S and CGI-I) scales.
Results:
Children with a mean age of 10.9±2.9 years had severe obsessive compulsive symptoms at baseline, and >80% of them had another comorbid psychiatric disease. Significant improvements in symptoms were achieved after 12 weeks of aripiprazole treatment, which were evaluated by significant decreases in symptom scores in the CY-BOCS, and improvements in CGI-I scores.
Conclusions:
This very small study of aripiprazole, given to children with OCD resistant to at least 12 weeks treatment with at least two SSRIs and CBT, demonstrated striking improvement in CGI scores (all subsets, p≤0.002) for 13 of 16 children, and halved all CY-BOCS subscores after ∼12 weeks of treatment.
Introduction
O
Several conventional (Sareen et al. 2004) and atypical antipsychotics (Delle Chiaie et al. 2011), were tested for augmenting the effects of SSRIs or clomipramine in OCD. The atypical antipsychotic aripiprazole was used in many clinical trials as an augmentation agent in refractory OCD cases (Thomsen 2004; Masi et al. 2010). The anti-OCD properties of aripiprazole were proposed to be related to its agonistic effect on 5-HT1A receptors (Matsushita et al. 2005). Previous studies showed that aripiprazole was also effective in monotherapy (Connor et al. 2005). Moreover, it was found to be effective in obsessive-compulsive symptoms in schizophrenia (Glick et al. 2008), bipolar disorder (Uguz 2010), and tic disorders (Murphy et al. 2009).
This study was conducted for evaluating the efficiency of the atypical antipsychotic aripiprazole as a single agent in treatment-resistant OCD cases.
Methods
Data from 16 consecutive cases with treatment-resistant OCD were retrospectively analyzed in the study that was conducted at Ege University Faculty of Medicine, Department of Child and Adolescent Psychiatry. The recruitment period was between June 2013 and June 2014. Cases were diagnosed according to the diagnostic criteria of Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) (American Psychiatric Association 2000). All patients had been given CBT together with at least two types of SSRIs or clomipramine for a minimum of 12 weeks, but showed no improvement in symptoms, according to the clinical evaluation of a senior child and adolescent psychiatrist. Data from patients with bipolar disorder, schizophrenia, or any clinically significant medical disorder, and data from patients using another antipsychotic drug were not included in the analyses. The design of the methodology is presented in Figure 1.
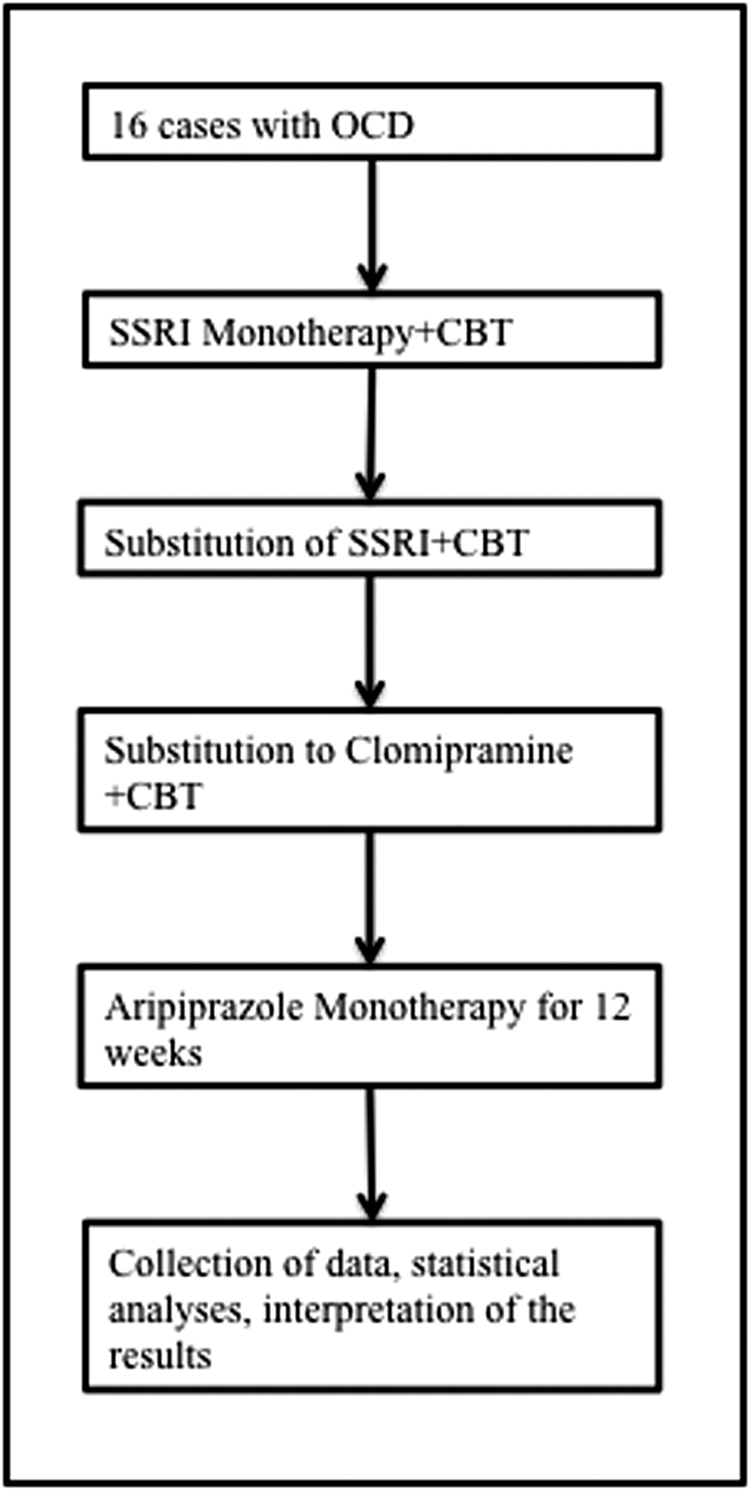
Flow chart of the design of the methodology.
Patients used aripiprazole (ABILIFY®, Bristol-Myers Squibb S.r.l. Anagni – Italy) with a mean dose of 4.75 mg/day (range: 27.5 mg/day). The duration of treatment was 12 weeks. Patients were evaluated at baseline, and at the end of the 12th week of treatment. The symptoms of obsessive and compulsive behaviors were evaluated according to the Childhood Yale-Brown Obsessive Compulsive Scale (CY-BOCS) (Goodman et al. 1989). This scale was shown to be a valid and reliable tool for evaluating obsessive-compulsive symptoms in Turkish children (Yucelen et al. 2006). The other scales used for evaluating treatment outcome in addition to the CY-BOCS were the Clinical Global Impressions-Improvement (CGI-I), and Severity (CGI-S) scales. Adverse events during aripiprazole treatment were evaluated by the Extrapyramidal Symptom Rating Scale (ESRS) (Chouinard and Margolese 2005). The patients were seen on a monthly basis for the evaluation of treatment response and adverse events. Necessary permissions were obtained from the Hospital Administration Office for analyzing the clinical data from the patients.
Statistical analysis
Categorical data from the study were presented in frequency tables, and numerical data were presented by means and standard deviations. The comparisons of numerical and ordinal variables at baseline and the 3rd month of treatment were conducted by Wilcoxon tests, and comparisons between sexes were conducted by Mann–Whitney U test. SPSS version 21 was used for statistical analyses. A type I error of 5% was considered for the significance level in the analyses.
Results
A total of 16 patients with a mean age of 10.9±2.9 years were included. The patient group consisted of nine girls (56.3%) and seven boys (43.8%) with mean ages of 11.6±2.5 years and 10±3.4 years, respectively. The education levels of more than half of the parents were university level and higher, and most of the parents had no psychiatric disease history. The sociodemographic characteristics of the patients are presented in Table 1.
OCD, obsessive-compulsive disorder; ADHD, attention-deficit/hyperactivity disorder.
The distributions of comorbidities and frequently observed obsessive-compulsive behaviors are presented in Table 2. More than 80% of the cases had at least one psychiatric comorbidity, and the most frequent comorbid disease was attention-deficit/hyperactivity disorder (ADHD) (Table 2). In the adverse event evaluations, only one patient showed increased appetite, and no additional adverse event was observed.
ADD, attention-deficit disorder; MDD, major depression disorder; ODD, oppositional defiant disorder; CD, conduct disorder; MD, mood disorder; ADHD, attention-deficit/hyperactivity disorder.
The CGI-S and CGI-I scores revealed that the severity of the disease was similar in boys and girls (p=0.354 and p=0.548, respectively; Table 3). The total obsession and compulsion scores on the CY-BOCS at baseline and 3rd month evaluations are presented in Table 4. Accordingly, the scores in both obsession and compulsion domains were significantly decreased after 3 months of aripiprazole treatment. The detailed evaluation of obsessive and compulsive behaviors by CY-BOCS at baseline and after 3 months of treatment is presented in Tables 5 and 6. Analyses revealed that all of the domains in the scales were significantly improved by aripiprazole treatment.
CGI, Clinical Global Impressions.
CY-BOCS, Childhood Yale-Brown Obsessive Compulsive Scale.
CY-BOCS, Childhood Yale-Brown Obsessive Compulsive Scale.
CY-BOCS, Childhood Yale-Brown Obsessive Compulsive Scale.
Discussion
The results of current study showed that 12 weeks of single-agent aripiprazole treatment is effective in refractory OCD. The cases showed significant improvements in obsessive and compulsive behaviors, and the mean scores of the CY-BOCS were decreased by at least 50% when compared with baseline. Also, CGI evaluations showed that the majority of the cases exhibited significant improvement in their clinical assessments.
One of the major concerns in the treatment of OCD is no or poor response. The first line choice of medication is SSRIs, delivered in addition to CBT. However, a significant proportion of cases are treatment resistant because of the severity of the disease and the presence of comorbidities with other psychiatric conditions (Storch et al. 2010; Rosa-Alcazar et al. 2013). Our patient group had high scores at baseline CY-BOCS evaluations, and most of them had at least one comorbid psychiatric disease showing a high risk for treatment failure with conventional OCD treatments. Consequently, an improvement in their clinical condition could not be achieved despite intensive treatment with their prior medication and CBT.
The first evidence regarding the efficiency of aripiprazole in SSRI-resistant OCD cases came from several case reports (Friedman et al. 2007; Sarkar et al. 2008; Storch et al. 2008), and clinical trials (Pessina et al. 2009). These studies showed that using aripiprazole as an augmentation agent in addition to SSRIs provides more beneficial effects on symptom reduction, compared with its use as a monotherapy agent. However, our results showed that it is also effective in monotherapy. This may be partly related to the pharmacological properties of aripiprazole. Previous studies suggested that interactions between serotonin and dopamine systems have significant effects on obsessive-compulsive symptoms (Goodman et al. 1996). Aripiprazole has a partial agonistic effect on D2 receptors (Mailman and Murthy 2010), and this partial agonism causes stabilization of D2 receptor mediated neurotransmission (Bortolozzi et al. 2007). Because of its 5-HT1A agonistic properties, combined with D2 selectivity, aripiprazole was suggested as a potential therapeutic agent in OCD (Shapiro et al. 2003).
The current study has some limitations. First, it lacks a randomized control group to evaluate the efficiency of aripiprazole in the treatment of SSRI-refractory OCD. Second, our findings showing favorable effects of aripiprazole monotherapy may also be biased by the narrow sample size, especially when additional grouping was performed. However, this is a promising study for providing evidence about the treatment of SSRI-resistant OCD cases in childhood with single-agent aripiprazole, which may be proven by further large-scale randomized and controlled studies in these patients.
Clinical Significance and Conclusion
Poor response to treatment in childhood OCD is particularly important, because the consequences of the disease are debilitating if left untreated. Current evidence favors the use of aripiprazole as an augmentation agent, rather than as monotherapy, in SSRI-resistant OCD cases. Our findings indicate that single-agent aripiprazole treatment may be effective in these cases, which provides an additional alternative option in this vulnerable patient group.
Footnotes
Disclosures
Eyup Sabri Ercan is in charge of the advisory board of Lilly and Janssen-Cilag. The other authors have no competing financial interests. The study received no funding.