
Abstract
To The Editor:
I
The aims of the present study were to identify 6–17-year-olds at risk for BD in a population-based sample (n=474) and to examine the potential association of mania symptom severity according to CBCL-MS with co-occurring child psychopathology and maternal anxiety/depression. Mothers of 6–17-year-olds were interviewed in a cross-sectional study conducted in a low-income urban community in southeast Brazil.
The study was based on a probabilistic sample of clusters of eligible households (women ages 15–49 years, son/daughter <18 years), with one mother–child pair randomly selected per household (n=813; response rate: 82.4%). Based on CBCL-MS total raw score percentiles, our sample was classified into three categories for mania: Clinical (>97), borderline (93–97), and no mania (<93). The current study considered the presence of psychopathology other than mania when any CBCL narrow-band scale (Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior) or any CBCL broad-band scale (Internalizing Behavior Problems, Externalizing Behavior Problems, and Total Behavior Problems) had t scores in the clinical range. This definition of psychopathology does not imply psychiatric diagnoses, as CBCL is a screening measure of emotional/behavioral problems that do not require the presence of impairment in global functioning. The Brazilian version of CBCL showed high sensitivity among pediatric outpatients and children referred to psychiatric evaluation (Bordin et al. 2013). Also, the Self-Reporting Questionnaire (SRQ-20) was applied to assess maternal anxiety/depression. The SRQ-20 was validated for the Brazilian population with a cutoff point >7 (Mari and Williams 1986).
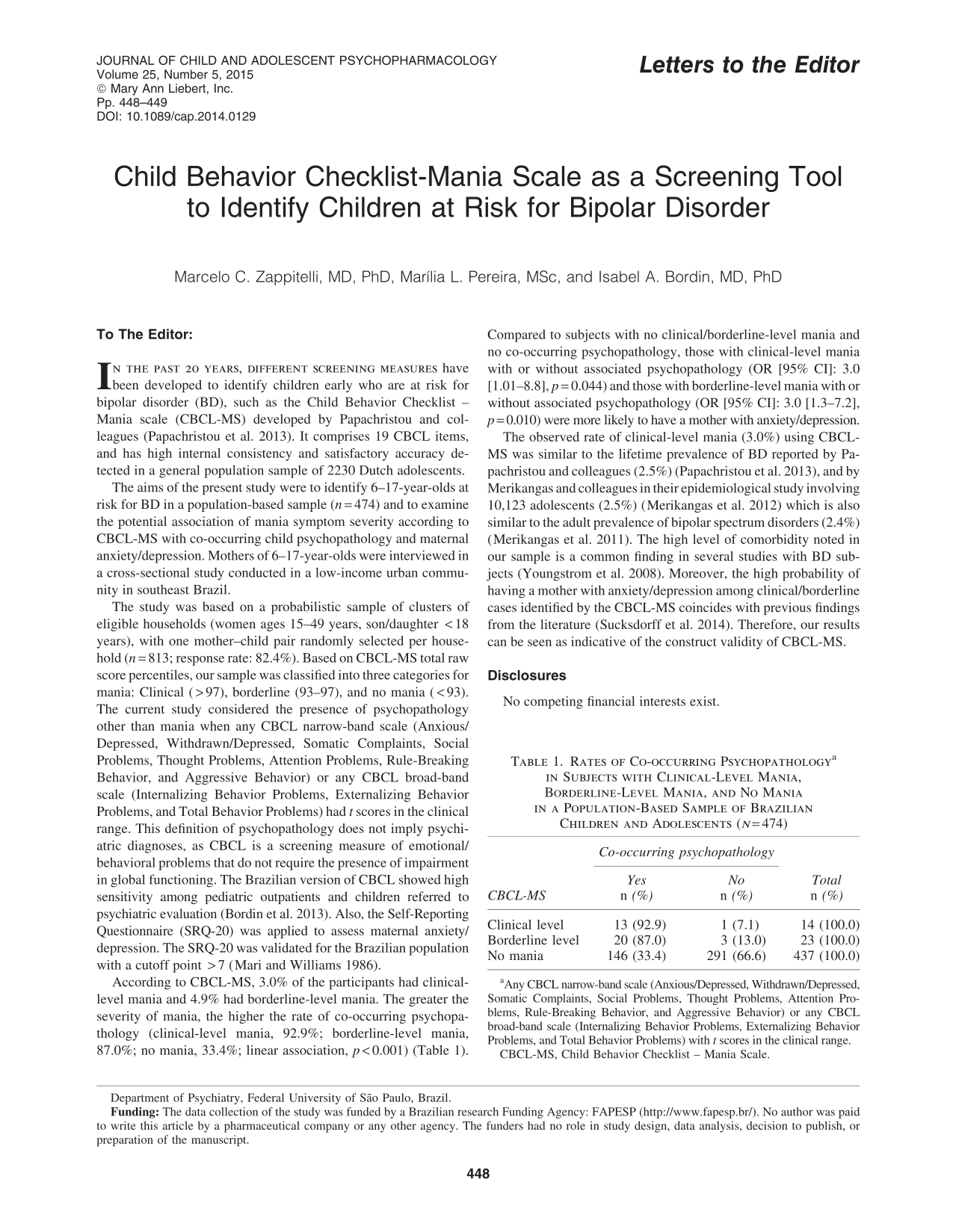
According to CBCL-MS, 3.0% of the participants had clinical-level mania and 4.9% had borderline-level mania. The greater the severity of mania, the higher the rate of co-occurring psychopathology (clinical-level mania, 92.9%; borderline-level mania, 87.0%; no mania, 33.4%; linear association, p<0.001) (Table 1). Compared to subjects with no clinical/borderline-level mania and no co-occurring psychopathology, those with clinical-level mania with or without associated psychopathology (OR [95% CI]: 3.0 [1.01–8.8], p=0.044) and those with borderline-level mania with or without associated psychopathology (OR [95% CI]: 3.0 [1.3–7.2], p=0.010) were more likely to have a mother with anxiety/depression.
Any CBCL narrow-band scale (Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior) or any CBCL broad-band scale (Internalizing Behavior Problems, Externalizing Behavior Problems, and Total Behavior Problems) with t scores in the clinical range.
CBCL-MS, Child Behavior Checklist – Mania Scale.
The observed rate of clinical-level mania (3.0%) using CBCL-MS was similar to the lifetime prevalence of BD reported by Papachristou and colleagues (2.5%) (Papachristou et al. 2013), and by Merikangas and colleagues in their epidemiological study involving 10,123 adolescents (2.5%) (Merikangas et al. 2012) which is also similar to the adult prevalence of bipolar spectrum disorders (2.4%) (Merikangas et al. 2011). The high level of comorbidity noted in our sample is a common finding in several studies with BD subjects (Youngstrom et al. 2008). Moreover, the high probability of having a mother with anxiety/depression among clinical/borderline cases identified by the CBCL-MS coincides with previous findings from the literature (Sucksdorff et al. 2014). Therefore, our results can be seen as indicative of the construct validity of CBCL-MS.
Disclosures
No competing financial interests exist.