
Abstract
Objective:
The purpose of this study was to evaluate the long-term safety and tolerability of paliperidone extended-release (ER) in adolescents with schizophrenia.
Methods:
This was a 2 year open-label, multicenter study in adolescents (12–17 years of age, inclusive) with schizophrenia. Eligible patients were initially treated with 6 mg/day paliperidone ER, and the dose could be adjusted between 1.5 and 12 mg/day based on clinical need. Safety parameters were treatment-emergent adverse events (TEAEs), weight, Tanner staging, blood chemistry (including prolactin, glucose, insulin, and lipid levels), and extrapyramidal symptom (EPS) scales. The main efficacy end-point was change from baseline to endpoint in Positive and Negative Syndrome Scale for Schizophrenia (PANSS) total score.
Results:
Of 400 enrolled patients (mean age, 15.4 years; boys, 61%), 220 were completers. Median (range) exposure was 604.5 (2–765) days. TEAEs were reported in 85.3% of patients; most frequently reported TEAEs included somnolence, increased weight, headache, insomnia, nasopharyngitis, akathisia, schizophrenia exacerbation, and tremor. No deaths were reported. There were no clinically significant mean changes in growth-adjusted z score for change in weight, height, or body mass index (BMI). Tanner ratings showed normal maturation. Most frequently occurring EPS-related events were related to Parkinsonism (15.5%) and hyperkinesia (13.8%). No cases of tardive dyskinesia were reported. Hyperprolactinemia (based on laboratory values) was noted in 56% of patients and 9.3% of patients had prolactin-related TEAEs. A low percentage of patients (4.3%, n=14) had a shift from normal or impaired fasting glucose to high levels. Mean (SD) decrease (improvement) in PANSS total score from baseline to end-point was −19.1 (21.89). The majority of patients had a ≥20% improvement in PANSS total score (responders) from initial treatment with paliperidone ER. Overall, 41.7% of patients achieved remission during the study.
Conclusions:
Paliperidone ER was generally tolerable, and exhibited efficacy in the maintenance treatment of schizophrenia in adolescents in this large 2 year study.
Introduction
T
The use of second-generation antipsychotics (SGAs), including risperidone, paliperidone extended-release (ER) (INVEGA® prescribing information 2011), aripiprazole, clozapine, and olanzapine has increased considerably in children and adolescents (Correll 2008a; Vitiello et al. 2009; Zuddas et al. 2011). Paliperidone ER is a once-daily atypical antipsychotic, approved in many countries, for the treatment of schizophrenia in adults (INVEGA® prescribing information) and adolescents (12–17 years of age, approved in the United States, and 15–17 years of age, approved in the European Union). Paliperidone ER was efficacious and generally tolerable in a completed double-blind (DB), 6 week, placebo-controlled, phase 3 study, which evaluated 1.5–12 mg/day dose range in adolescents (Singh et al. 2011). These results were similar to those in studies of adults with schizophrenia treated with paliperidone ER (Marder et al. 2007; Emsley et al. 2008; Meltzer et al. 2008) and also in adolescents with schizophrenia treated with risperidone (Sikich et al. 2008; Haas et al. 2009; Findling et al. 2010). There are several pharmacokinetic advantages for the use of paliperidone ER. Because of the ER formulation, the plasma concentration-time profile of paliperidone ER after a single dose exhibits a gradual ascending increase in plasma concentrations over a period of 24 hours, which increases the possibility of achieving stable dopamine-2 receptor occupancy (Boom et al. 2009). This pharmacokinetic property allows once- daily dosing, which increases adherence, and reduces the potential for adverse events associated with peak levels. Paliperidone ER is primarily eliminated via renal excretion, potentially leading to fewer drug–drug interactions as opposed to risperidone, which is extensively metabolized in the liver (Vermeir et al. 2008; RISPERDAL® prescribing information 2005).
A recent systematic review suggested that the clinical efficacy of first generation antipsychotics (FGAs) and SGAs in adolescents was comparable (Datta et al. 2013). However, SGAs are preferred in the treatment of early-onset schizophrenia as they are less likely to cause extrapyramidal symptoms (EPS) at therapeutic doses, and produce lower dropout rate from trials than FGAs (Cawthron et al. 1994; Correll 2008b; Sikich et al. 2008; Caccia et al. 2011; Datta et al. 2013; Zhang et al. 2013). However, they are associated with certain side effects such as weight gain, sedation, cardiometabolic disorders, and hyperprolactinemia, which may affect normal growth and maturation of adolescents (Cawthron et al. 1994; Correll 2008b; Fraguas et al. 2011; Sikich et al. 2008; Findling et al. 2010). Very limited information on the long-term safety profile of antipsychotic medication in general, and of paliperidone ER in particular, exists in this patient population; therefore, a systematic benefit–risk evaluation is needed.
This open-label (OL), single-arm, flexibly-dosed study (extension of the 6 week DB study) (Singh et al. 2011) was designed to evaluate the long-term safety and tolerability of paliperidone ER in adolescent patients with schizophrenia. The efficacy of paliperidone ER in the long-term treatment of schizophrenia was also assessed as a secondary objective.
Methods
Study population
The Independent Ethics Committee or Institutional Review Board at each study site approved the protocol, and the study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and that are consistent with good clinical practices and applicable regulatory requirements. All patients provided assent, and parents or guardians provided written informed consent before entering the patients in the study.
This 2 year OL, multicenter study was conducted in patients who were 1) either directly enrolled, 2) had completed the DB, 6 week, placebo-controlled study (Singh et al. 2011), or 3) had discontinued that study because of lack of efficacy (completed a minimum of 21 days of the study and were expected to benefit from paliperidone ER in a flexible dose range) (Fig. 1). Boys or girls 12–17 years of age (inclusive, at the time of study enrollment), weighing ≥29 kg, diagnosed with schizophrenia (per Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [DSM-IV] criteria) for ≥1 year, were included in the study (American Psychiatric Association 1994). Diagnosis of schizophrenia was established using the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (KSADS-PL) with a score of ≤2 for each item related to suicide or self- harm. Patients entering the study directly had to have had at least one adequate treatment with an antipsychotic before participation in this study. Patients who at screening met the DSM-IV diagnosis of bipolar disorder, major depressive disorder, schizoaffective disorder, schizophreniform disorder, autistic disorder, mental retardation, dissociative disorder, primary substance-induced psychotic disorder, significant medical or neurologic disorder, or active substance dependency (past 3 months before screening) were excluded from the study. Female patients who were pregnant, planning to become pregnant, or were nursing were also excluded.
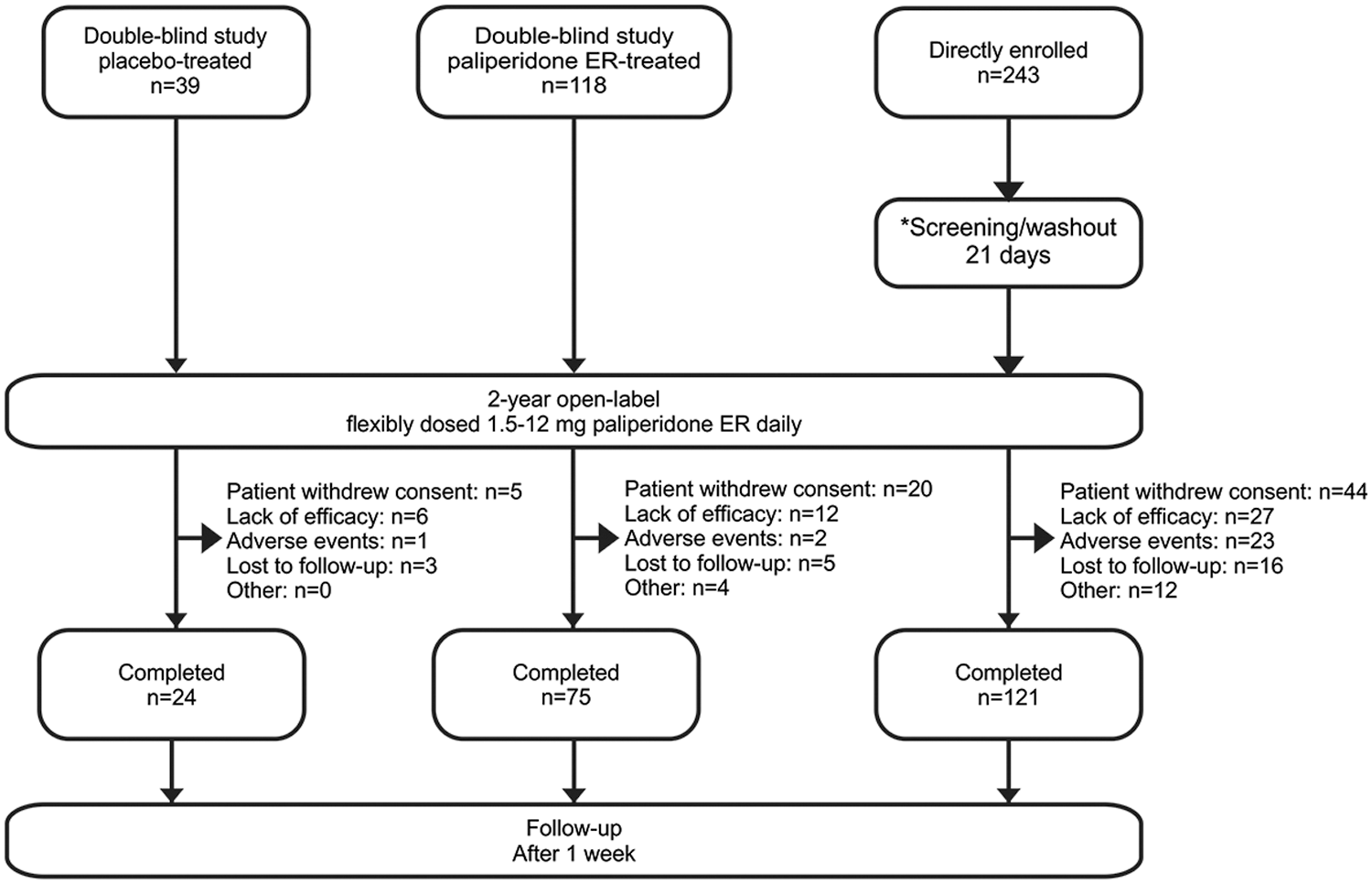
Study design and patient disposition. Some completers were 6 month completers. *Only for patients who directly enrolled in the open-label study.
Study design and treatment
For patients who entered the study directly, a screening and washout phase (maximum of 21 days) was included. The OL treatment phase for all patients was up to 2 years, which was followed by a posttreatment (follow-up) phase of 1 week after the patient's final dose of the study drug. It is of note that prior to a study amendment, the initial study length was 6 months of OL treatment, and some patients chose to discontinue after only 6 months of treatment. The study was amended to extend the duration of the study up to 2 years, in order to allow for an adequate duration and sufficient number of patients to study the effect of paliperidone on growth and development over time.
The ER formulation was based on the osmotic pump technology (OROS®) of ALZA Corporation. Paliperidone ER was supplied as a capsule-shaped tablet at dose strengths of 1.5 mg, 3 mg, and 6 mg. The initial dose was a 6 mg daily dose, which was titrated up to 9 or 12 mg/day (increments of 3 mg, not more frequently than once every 5 days), or titrated down to 3 or 1.5 mg/day, based on efficacy or tolerability and investigator's discretion.
Concomitant and prohibited medications
Use of other central nervous system agents and treatments (e.g., antidepressants, benzodiazepines, psychotherapy) was allowed. Other antipsychotic medications, lithium, electroconvulsive therapy, psychostimulants, or dopamine agonists (e.g., pramipexole, ropinirole, modafinil) were prohibited. Oral benzatropine 1–2 mg b.i.d. or biperiden 2 mg t.i.d. was permitted for the treatment of EPS. Other anticholinergics, such as trihexyphenidyl were permitted at the discretion of the investigator. Certain sedatives, hypnotics, or anxiolytics (including barbiturates) were also prohibited. Oral lorazepam (≤1mg/day after week 4) was the preferred benzodiazepine for the study, although other benzodiazepines could be used at equivalent doses. The flexibility in permitted medications allowed investigators to treat patients to their optimal level, as they would be treated in routine clinical care.
Assessments
The primary objective of the study was to evaluate the long-term (2 year) safety and tolerability of paliperidone ER in adolescents with schizophrenia. Assessment of safety parameters was the primary objective. Safety assessments included treatment-emergent adverse events (TEAEs); weight; height; waist circumference; metabolic parameters; electrocardiogram (ECG); vital signs; Tanner staging (conducted by a physician); clinical laboratory tests (hematology, fasting lipid levels, glucose, insulin and serum chemistry, and urinalysis); prolactin and testosterone (males only) levels; EPS monitored by means of Abnormal Involuntary Movement Scale (AIMS), Barnes Akathisia Rating Scale, and Simpson–Angus Scale; and Columbia Suicide Severity Rating Scale. Adverse events were reported by the patient from the signing of informed consent/assent until all end-of-study and posttreatment procedures were completed. Fasting blood samples for serum chemistry and hematology and a random urine sample for urinalysis and Tanner staging were collected at screening, baseline, week 8, week 20, week 24, week 48, study end or upon early withdrawal, and at the follow-up visit. Investigators were trained at the investigator meeting on the assessment of Tanner staging. For patients who entered the study after completion of the DB study, the end-of-study or early withdrawal assessments from the DB study served as the baseline values for this study, and were not repeated. ECGs were recorded at screening and baseline before study drug administration and at week 4, week 12, week 24, and end of study or upon early withdrawal. A follow-up visit was conducted 1 week after end-of-study visit and discontinuation of study medication. At this visit, data regarding vital signs, body weight, waist measurement, blood samples for serum chemistry and hematology; and urinalysis; Tanner staging; concomitant medication; and adverse events was collected.
The secondary objective of the study was efficacy. Efficacy assessments included change from baseline to the end-point (week 104 or the last postbaseline assessment) in the Positive and Negative Syndrome Scale for Schizophrenia (PANSS) scores, Clinical Global Impressions-Severity (CGI-S) scales, and Children's Global Assessment Scale (CGAS). Patients who had a ≥20% improvement in PANSS total score from OL baseline to end-point after treatment with paliperidone ER were considered to be responders. Remission was defined as a score of ≤3 on all of the following eight PANSS items: P1, P2, P3, N1, N4, N6, G5, and G9 for the last 6 months of treatment) (Andreasen et al. 2005) during the study. The raters of the efficacy outcomes were certified prior to study initiation and then recertified on a yearly basis.
Data analysis
No formal sample size calculation was performed. Based on the discontinuation rate seen in a similar study evaluating risperidone in adolescents, ∼400 patients were to be enrolled, in order that at least 100 patients would complete 2 years of treatment (Haas et al. 2009).
All patients who received one or more doses of the OL study drug were included in the safety analysis set, and this set was used for safety analyses. Safety was analyzed using descriptive statistics and frequency distributions. The intent-to-treat (ITT) analysis set, which included all enrolled patients who received one or more doses of the OL study drug and had both the baseline and one or more postbaseline efficacy assessments in the OL phase was used for the efficacy analyses. Descriptive statistics of the change from baseline to each time point (both observed and last observation carried forward [LOCF]) were provided for PANSS, CGI-S, and CGAS.
Results
The study was conducted from June 2007 to July 2012 at 55 centers in 10 countries (Bulgaria n=6, Estonia n=3, Finland n=3, India n=64, Korea n=40, Poland n=47, Romania n=20, Russia n=109, Ukraine n=48, and the United States of America n=60). Patients were either directly enrolled into the study (n=243, 61%) or were those who had continued from the 6 week DB study (n=157, 39% [n=118, 30% on paliperidone ER; n=39, 10% on placebo]). Of the 400 patients enrolled, 220 (55%, 184 patients completed the 2 year study and 36 patients completed the 6 month study before the study was extended to 2 years) completed the study (Fig. 1). The demographics and baseline characteristics are listed in Table 1.
Prior hospitalization for psychosis, excluding the current hospitalization.
CGAS, Children's Global Clinical Assessment; CGI-S, Clinical Global Impressions-Severity; OL, open-label; PANSS, Positive and Negative Syndrome Scale for Schizophrenia scores.
Prior and concomitant medication
The majority (92%) of the patients had received at least one prior psychotropic medication, excluding the treatment in the DB study. Prior treatment with atypical antipsychotics was reported in 72% patients, and treatment with typical antipsychotic medication was reported in 37% of patients. The most commonly received prior medications were risperidone 39% (n=157) and lorazepam 28% (n=111). The most commonly used benzodiazepine during this study was lorazepam (27%, n=108). The anti-EPS medications received by at least 5% of patients during the OL study were trihexyphenidyl (n=58, 15%), benzatropine (n=29, 7%), and biperiden (n=18, 5%) (Table S1) (see supplementary material in the online article at
Exposure
The most common paliperidone ER dose was 6 mg/day (38%); ∼50% of the patients had a mode dose of 9 (21% of patients) or 12 (29% of patients) mg/day and 11% patients had a mode dose of 3 mg/day. The patient retention was high, considering the patient population and the 2 year treatment duration, with mean (SD) exposure of 459.6 (290.20) days and median exposure (range) of 604.5 (2–765) days.
Safety
Overall, 85.3% (341/400) of patients experienced TEAEs (Table 2). The most common TEAEs were somnolence and weight increase (18.3% each). Most TEAEs were mild or moderate. The only TEAEs rated severe in three or more patients were schizophrenia exacerbation (n=19), suicidal ideation (n=8), dystonia (n=4), increased weight (n=4), akathisia (n=3), and anxiety (n=3). The incidence of TEAEs was higher in patients (88.0%) who weighed ≥51 kg than in patients (77.2%) who had weighed <51 kg at the baseline. There were no deaths in this study. Serious TEAEs occurred in 14.8% (59/400) of patients, and most were psychiatrically related (12.5%). The most common (>5%) serious TEAE was worsening of schizophrenia (7.5%). TEAEs leading to discontinuation occurred in 6.3% (25/400) of patients. These TEAEs included suicide attempt and akathisia (three patients each), as well as insomnia, suicidal ideation, alanine transaminase increase, aspartate aminotransferase increase, and amenorrhea (two patients each).
TEAEs, treatment-emergent adverse events.
Vital signs, physical findings and ECG
No clinically meaningful effects of paliperidone ER on pulse rate, blood pressure, and ECG parameters were observed. Most patients had changes in QTc values ≤30 msec; no postdose QTc >480 msec was observed (Table 3). The mean weight increase from baseline to the end-point was modest (4.7 kg). Overall, 43.3% of patients experienced weight gain of ≥7.0% from baseline to the end-point. Because adolescence is a time of rapid growth and development and weight gain is to be expected for most adolescents over 2 years, z scores were used to compare the height and weight increase in the study patients with the general adolescent population. The z score value indicates how many standard deviations an observed value is away from the expected value of weight, height, or body mass index (BMI) based on age and sex. A change z score of >0.5 is considered clinically relevant. Mean z scores showed no meaningful change from baseline to the end-point for height (0.0), weight (0.1), and BMI (0.1) (Table 3). The proportion of patients who had clinically meaningful increases in end-point z scores of >0.5 were 5.8% of patients for height, 17.2% for body weight, and 17.5% for BMI. A total of 84 (21.0%) patients had weight gain related TEAEs.
Insulin and glucose levels collected only in a fasting state are included in the determination of HOMA-IR and
HOMA-%B.
The z score indicates how many standard deviations an observed value is away from the expected weight, height, or BMI based on a patient's age (in months) and sex.
These results are based on maximum postbaseline value, not end-point.
These results are only for boys among the patients that enrolled directly.
HOMA-%B and HOMA-IR are expressed as geometric mean {exp[mean (logs) - 1*SD(logs)], exp[mean (logs)
+1*SD(logs)]}.
AIMS, Abnormal Involuntary Movement Scale; BARS, Barnes Akathisia Rating Scale; BL, baseline; BMI, body mass index; HOMA-IR, Homeostatic Model Assessment for Insulin Resistance; HOMA-%B, Homeostatic Model Assessment for Beta-Cell Function; LDL, low-density lipoprotein; SAS, Simpson–Angus Rating Scale.
Most Tanner ratings were 4 or 5 at baseline and the end-point, which indicated a mostly postpubertal population in this study. In younger patients (12–13-year-olds), normal sexual maturation occurred, which was evident with a shift from a baseline score of <4 to ratings of 4 and 5 at study end. No clinically meaningful laboratory parameters (other than prolactin, discussed subsequently) were observed.
Other significant TEAEs
Metabolic disturbances
A majority of the patients with normal fasting plasma glucose at OL baseline maintained normal glucose levels during treatment (Table 3). Overall, a low percentage of patients (4.3%, n=14) had a shift from normal or impaired fasting glucose to high levels. A total of 6 (1.5%) patients had a glucose-related TEAE, all of which were mild in intensity. At the baseline, geometric mean values of Homeostatic Model Assessment (HOMA) for Insulin Secretion indicated a mild degree of insulin resistance (2.38), and β cell dysfunction (128.7%) (Table 3). A small decrease (improvement) in these values from baseline to the end-point was observed. Mean values of lipid measurements remained stable over the course of the 2 year study.
Suicidality-related TEAEs
Overall, 9.3% (n=37) patients experienced suicidality-related TEAEs, and most events were mild to moderate in severity. Suicide attempts were reported in three (0.8%) patients, all of which led to study discontinuation. There were no completed suicides in the study.
EPS-related TEAEs
The most common EPS-related TEAEs were grouped under Parkinsonism (15.5%) and hyperkinesia (13.8%); the most common were akathisia (13.0%), tremor (11.0%), muscle rigidity (6.5%), and dystonia (5.3%). These TEAEs were mostly mild to moderate in severity; only musculoskeletal stiffness, hypokinesia, akathisia, and dystonia were reported as serious TEAEs. The EPS-related TEAEs leading to study drug discontinuation were akathisia, tremor, dystonia, and oculogyric crisis. No cases of tardive dyskinesia were reported in this long-term study. Further confirmation of the absence of tardive dyskinesia cases was obtained by applying Schooler–Kane criteria to the AIMS scores (Table S2) (see supplementary material in the online article at
Potentially prolactin-related TEAEs
Serum prolactin levels increased in the paliperidone ER treatment group. Greater than normal prolactin values occurred in a higher percentage of boys (60%) than girls (48%). The mean prolactin level increased early during treatment and then stabilized over time until the end-point (Table 4). Overall, 9.3% (37/400) of patients experienced a potentially prolactin-related TEAE; the incidence was greater (18.5%) in girls than in boys (3.3%). Most of these events were mild to moderate in severity. The most common prolactin-related TEAEs among girls were amenorrhea (5.1%) and galactorrhea (10.2%) (Table 5). Study discontinuation because of prolactin-related TEAEs was observed in four patients: amenorrhea (n=2), galactorrhea (n=1, girl), and gynecomastia (n=1, boy).
Percentages calculated with the number of patients per sex as denominator.
Incidence is based on the number of patients experiencing at least one adverse event, not the number of events.
Occurred only in girls.
Occurred only in boys.
Efficacy
PANSS
The mean change in PANSS total score improved (decreased) from baseline to the end-point (−19.1), and regardless of study entry, patients achieved a similar mean PANSS score at end-point (between 63.8 and 65.3) (Table 6 and Fig. 2). The PANSS total score (decreased) improved during the first 3 months of the treatment and was generally maintained during the rest of the study. Additional evaluation showed that PANSS total scores improved from baseline to end-point in both the 12–14 and 15–17 year age groups. There were mean decreases (improvement) in PANSS Marder factors and subscales from baseline to end of study in all patients (Table 5). As expected, changes in the positive symptom factor and subscale were numerically larger than other factor scores or subscales. The majority of patients had a ≥20% improvement in PANSS total score from initial treatment with paliperidone ER. Overall, 41.7% of patients achieved remission.
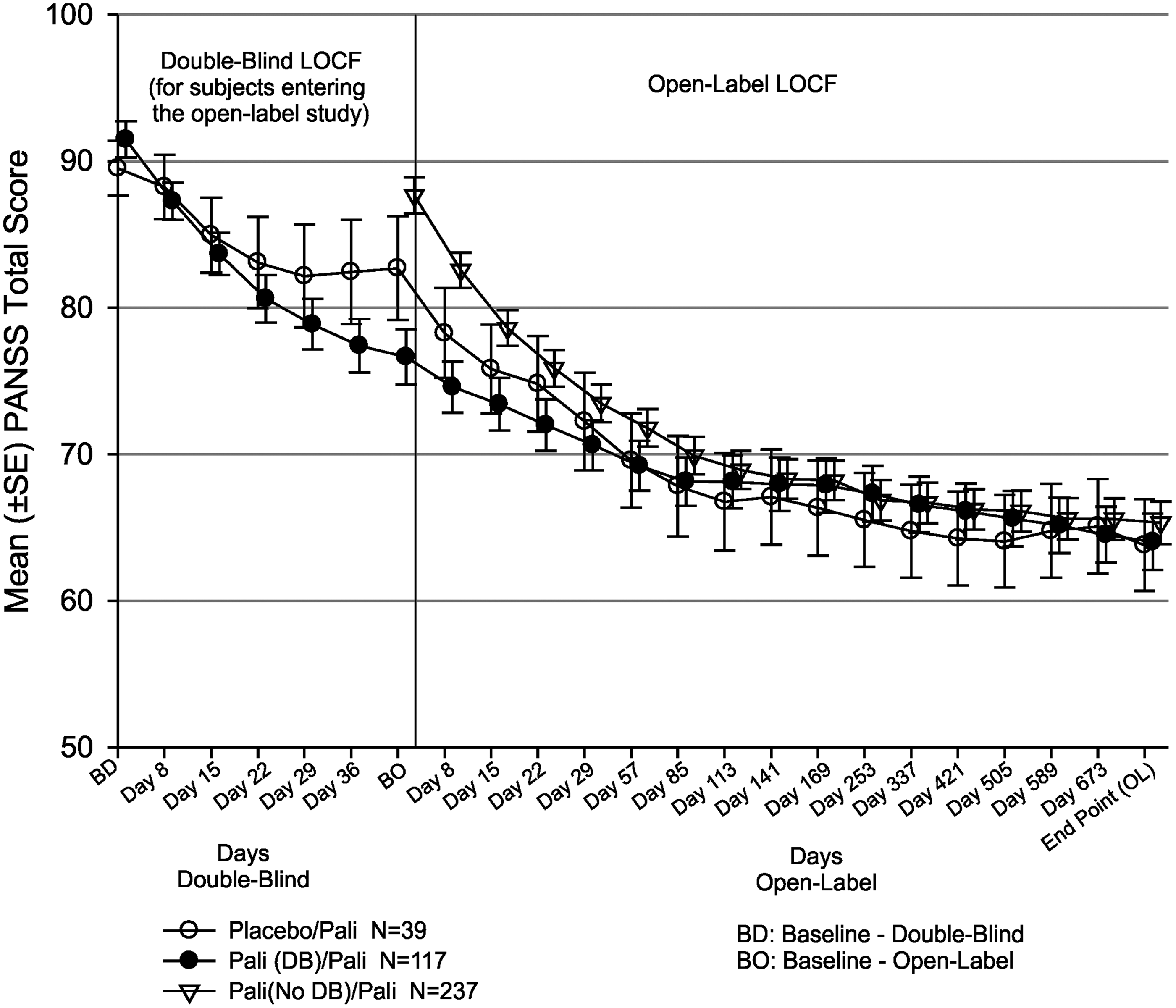
Mean (SE) Positive and Negative Syndrome Scale for Schizophrenia (PANSS) Total Score – Last Observation Carried Forward (LOCF) (open-label – intent to treat analysis set).
Responders had a change in PANSS score of >20%.
Remission was defined per Andreason et al. 2005.
PANSS, Positive and Negative Syndrome Scale.
CGI-S scale
The median change in CGI-S scores from baseline to the end-point was −1.0 (improved). The percentage of patients with a severity of illness rated as “not ill/very mild/mild” increased from 25.4% at baseline to 61.6% at the end-point. It is of note that some patients (n=117) had been treated with paliperidone ER during the 6 week DB study prior to the baseline for the OL study.
CGAS
The mean change in CGAS scores from baseline to the end-point was 13.1 (improved). A CGAS score of >70 is considered a likely indicator of near-normal social function. The proportion of patients who had a CGAS score of >70 increased from 9.4% at baseline to 37.4% at the end-point.
Discussion
This is the longest and largest safety study of an antipsychotic medication for adolescent schizophrenia that is available in the literature to date. The length and size of the study should provide a good indication of the long-term risks and benefits of paliperidone in adolescents with schizophrenia. Although the clinical efficacy of one SGA versus another is generally similar, the safety profile of various SGAs differs (Cawthron et al. 1994; Caccia et al. 2011; Datta et al. 2013). The safety profile of paliperidone ER in the adolescents in this study appeared to be consistent with the known profiles of paliperidone ER in adults (Marder et al. 2007; Emsley et al. 2008; Meltzer et al. 2008), and of risperidone in adolescents in terms of the incidence of TEAEs and the occurrence of the most common TEAEs (Emsley et al. 2008; Haas et al. 2009; Findling et al. 2010; Harrington and English 2010). The most common TEAEs included somnolence, weight increase, headache, insomnia, nasopharyngitis, akathisia, schizophrenia, and tremor. The higher incidence of TEAEs in patients who weighed ≥51 kg than in patients who weighed <51 kg at the baseline could be attributed to the 54% mode dose in the 9–12 mg/day range in the patients who weighed ≥51 kg as compared with 37% in the patients who had weighed <51 kg at the baseline. Rates of other psychiatrically related TEAEs (worsening of psychosis, depressed mood, agitation, and aggression) were relatively low for a severe mental illness in adolescents. The discontinuation rate resulting from lack of efficacy or TEAEs was low. Although this study was longer in duration than most other adolescent schizophrenia studies, the completion rate observed in this study was considerably high (55%) compared with that for olanzapine (23%) and risperidone (19%) in the 44 week DB extension phase of the treatment of early-onset schizophrenia spectrum study (Findling et al. 2010).
Weight gain is a serious complication observed in adolescents taking antipsychotics, and it is associated with other medical comorbidities such as abnormal glucose and lipid levels, and cardiovascular disorders (Krausz and Muller-Thomsen 1993). According to data reported in the clinical trials, mean weight gain ranging from 0 to 16.2 kg in adolescents treated with antipsychotics has been observed (Fraguas et al. 2011). As expected in an adolescent population, increase in body weight was observed in patients receiving paliperidone ER during the current 2 year study (4.7 kg mean increase). However, it was lower than the average weight gain observed in a 52 week study of risperidone (11.0 kg) and olanzapine (11.1 kg) treatment in adolescents (Findling et al. 2010). In the current study, 43.3% of patients experienced ≥7.0% weight gain. Weight gain in adolescents needs to be evaluated in the context of normal growth and development; therefore, z score values are more appropriate for evaluation. In this study, the observed mean z score change of 0.1 from baseline to the end-point was much lower than that observed for risperidone (0.5) and olanzapine (0.7) in the 52 week trial in adolescents (Findling et al. 2010). There were no clinically significant mean changes in z scores for weight or BMI; therefore, the weight gain observed in this study was generally similar to that expected for normal adolescent maturation. Weight gain in this study may have been less because almost all of the patients had had at least one prior treatment with antipsychotic medication.
With atypical antipsychotic medications, there is a concern about impaired glucose tolerance. The majority of patients had normal baseline fasting plasma glucose and the glucose level remained normal during the treatment. Less than 5% of patients shifted from normal or impaired fasting glucose at baseline to high levels of glucose at any point during the study, which is similar to the results observed in the risperidone treatment study in adolescents (Haas et al. 2009). Furthermore, <2% of patients demonstrated glucose-related TEAEs, and these numbers are consistent with those observed in adults treated with paliperidone ER (Emsley et al. 2008; Meltzer et al. 2008). There was little change in insulin sensitivity and β cell function during the course of the study. At study entry, based on HOMA analysis, patients had slightly impaired insulin resistance and a compensatory increase in insulin secretion, which improved slightly during the course of the study. No clinically meaningful changes in the vital sign values or ECG parameters were observed. Lipid levels remained stable during the course of the study. Other than prolactin and glucose levels, no clinically meaningful effects of paliperidone ER in the laboratory parameters were noted.
Even though the risk of EPS is reduced with atypical antipsychotics, adolescents are more likely to experience EPS-related TEAEs such as Parkinsonian side effects and dystonia than are adults (Sikich et al. 2004; Haas et al 2009). The EPS-related adverse events in this study were higher (37%), than those in adults treated with paliperidone ER (25%) (Emsley et al. 2008). The most common EPS-related TEAEs were Parkinsonism and hyperkinesia. There was no clinically meaningful change in scores on movement disorder rating scales. Anticholinergic medications are taken to control EPS, and use of these medications during this study was lower (25%) than prior to study entry (32%). This percentage was comparable with that observed in the DB paliperidone ER study for adolescents (15–29%) (Singh et al. 2011). Although the use of anticholinergic medications was higher than in adults treated with paliperidone ER (9–16%) (Marder et al. 2007) it was much lower than that in a previous study in children and adolescents (haloperidol, 67%; risperidone, 53%; and olanzapine, 56%) (Sikich et al. 2004). Overall, treatment-emergent EPS occurred more frequently in the first 3 months than later in treatment. A potential reason for higher EPS during the first 3 months may be because of switching from previous antipsychotics to the study drug, or changes in the doses during the titration period. Occurrence of EPS is more often during initiation of treatment, and tolerance may develop over time. No cases of tardive dyskinesia were reported.
Hyperprolactinemia is also a concern with drugs that antagonize dopamine D2-receptors (Alfaro et al. 2002), such as paliperidone ER. Galactorrhea, amenorrhea, gynecomastia, and impotence have been reported in patients with hyperprolactinemia. The propensity for prolactin elevation differs among antipsychotic medications. The majority of the SGAs are known to cause elevations of prolactin levels. The majority of adolescents with psychotic disorders were estimated to experience some prolactin elevation within the first few months of treatment (Anderson et al. 2007; Findling et al. 2010). In the current study, in girls, the mean prolactin levels were almost double the baseline value by 8 weeks, after which the levels declined by week 48 and were stable until study end-point, although still higher than baseline. However, in boys, twice the baseline mean prolactin value at week 8 declined after 24 weeks, although, similarly to in girls, these values were higher than the baseline. Similar results are reported for 2 year studies in adolescents treated with risperidone (Findling et al. 2010). An incidence of hyperprolactinemia ranging from 12% to 62% has been reported for risperidone, olanzapine, and quetiapine (Roke et al. 2009). In the current study, hyperprolactinemia (based on laboratory values) was noted in 56% patients. The incidence of prolactin-related TEAEs was 9.3%, indicating that in many patients the elevated prolactin did not result in clinically significant TEAEs. Prolactin-related TEAEs have been reported in 5.1–13.8% adolescents treated with olanzapine, quetiapine, and risperidone (Roke et al. 2009). Discontinuation because of prolactin-related adverse events was rare in this study, occurring in 1% of the patients. Despite the elevations in prolactin, which can have an impact on sex hormones, no clinically relevant difference in Tanner staging results was observed through the course of the study. Further, in the male patients, testosterone levels stayed in a normal range. Investigation of an association between 1 year risperidone treatment on pubertal development has demonstrated no effect on Tanner stage progression with long-term treatment of risperidone (Dunbar et al. 2004; Reyes et al. 2006).
The PANSS scores decreased (indicating improvement) after administration of paliperidone ER, and the improvement was maintained over the course of the study. This is particularly important because treatment guidelines recommend long-term treatment with antipsychotic medication. Other efficacy analyses, including the CGI-S and CGAS, corroborated the abovementioned findings. The data also support paliperidone ER's efficacy in maintaining symptom stability for schizophrenia over the 2 year treatment period in this population. Increasingly, there has been greater interest not only in reduction of symptoms with antipsychotics, but also in remission of symptoms, which has been rarely studied in adolescent schizophrenia (Andreasen et al. 2005). In this study, >40% of patients achieved remission (symptom severity of mild or better in core symptoms for 6 months) prior to the end of the study. The 6 week DB paliperidone ER study showed that 1.5 mg/day was ineffective, and that the minimum effective dose was 3 mg/day (Singh et al. 2011). In the current study, only six patients (1.5%) were on the 1.5 mg/day dose.
The limitations of this study were that it was not a placebo-controlled study, and there was no rater or patient blinding and no comparator; therefore, efficacy changes should be interpreted with caution. Although a flexibly dosed study is more naturalistic, it makes it impossible to determine if certain TEAEs may be dose related as was seen in the 6 week randomized, fixed-dose DB study (Singh et al. 2011). Of the total 400 enrolled patients, 220 (55%) completed the study up to end-point, hence it is likely that patients with more troublesome TEAEs or poor efficacy tended to drop out early in the trial. A majority of the adolescents were white and were 15–17 years of age, hence caution is warranted regarding extrapolating the observations of this study to the general adolescent population. Further, these patients all had had their illness for at least 1 year and had had prior treatment, hence safety and efficacy may be different for first episode patients. This study also included 61% patients who were directly enrolled, as compared with those who had continued from the DB study. Such a study design reflects the real world treatment scenario for patients requiring long-term treatment, as some patients were treated for up to 6 weeks in the DB study (paliperidone ER, 118; placebo, 39); this previous treatment impacted their baseline values for this study. It should be noted that 16% of the completers were treated for only 6 months as opposed to those who were treated for the entire 2 year period. The results for the patients treated for 6 months are not presented separately, as the outcomes were similar for both these groups.
Conclusion
In conclusion, paliperidone ER was generally tolerable for the long-term treatment of schizophrenia in adolescents 12–17 years of age. Symptoms of schizophrenia improved and the effect was generally maintained over a 2 year period.
Clinical significance
Paliperidone ER was generally tolerable in a 2 year long-term treatment of schizophrenia in adolescents 12–17 years of age. There were no clinically significant mean changes in z scores for weight or BMI. The incidence of prolactin-related TEAEs was 9.3%, and no cases of tardive dyskinesia were reported. Symptoms of schizophrenia improved and the effect was generally maintained over a 2 year period.
Footnotes
Acknowledgments
The authors thank the study participants, without whom this study would never have been accomplished, and also thank the following investigators for their participation in this study.
Dr. Sangita Patil (SIRO Clinpharm Pvt Ltd.) provided writing assistance, and Dr. Harry Ma (Janssen Research & Development, LLC) provided editorial support for the development of this manuscript.
Disclosures
Drs. Savitz, Nuamah, Singh, Hough, and Gopal, and Ms. Lane are employees of Janssen Research & Development, LLC. Drs. Singh, Nuamah, Hough, and Gopal designed the study; Dr Nuamah and Ms. Lane performed the statistical analysis; all authors were responsible for data collection and analysis. All authors met International Committee of Medical Journal Editors (ICMJE) criteria, and all those who fulfilled those criteria are listed as authors. All authors had access to the study data, provided direction and comments on the manuscript, and made the final decision about where to present these data.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.