
Abstract
Aims and Objectives:
The aim of the study was to determine whether there are differences in psychopharmacological practice for attention-deficit/hyperactivity disorder (ADHD) in children and adolescents dependent on the presence or absence of associated intellectual disability; and if there are, whether the differences are influenced by factors such as age, gender, and living circumstances.
Methodology:
A case–control cross-sectional design was used. Each arm of the study had a total of 107 children and adolescents aged 5–18 years. Case participants had diagnoses of having intellectual disability and ADHD; comparison participants had diagnoses of having ADHD, but no intellectual disability. Outcome measurements were (1) concurrent use of medications—single medication event as against concurrent multiple medication events—and (2) type of medication used—stimulants versus nonstimulants. Demographic factors considered were gender, age, and living circumstances.
Results:
Male-to-female ratio in each group was 90:17. Mean age in the case group was 10.93 years (standard deviation [SD]: 3.39 years) and in the comparison group, 12.34 years (SD: 3.22 years). Seventy percent of the case group lived with their biological families, while 84% of the comparison group did so. In the case group, 7.5% were in residential school placements compared with only 0.9% of the comparison group. There were no statistically significant differences in broad measurements of outcomes between the case and comparison groups. Age appeared to be an important moderating factor for type of medication prescribed. Younger children with intellectual disabilities and ADHD were more likely to be established on nonstimulant medications than those with ADHD and no intellectual disabilities (p = 0.024, odds ratio: 1.8; 95% CI: 1.2–2.7).
Conclusions:
Being between the ages of 5 and 12 years and having intellectual disability and ADHD are associated with raised likelihood of being prescribed nonstimulant medications for ADHD. This difference is maintained irrespective of gender and living circumstances. Reasons for these differences in prescribing practice require further exploration.
Introduction
A
Intellectual disability is often associated with clinically significant physical, social, and behaviorally driven comorbidities. Indeed, in intellectual disability, comorbidity is described as the rule rather than the exception (Turk 2010b). Some of these comorbidities require pharmacological interventions in their own right, and some of the medications used may include those with effects on the core symptoms of ADHD. Furthermore, the inherent problems in communication and expression of symptoms of ADHD by persons with intellectual disability may predispose them to diagnostic and hence therapeutic uncertainty, the prescribing of more than one medication, and the prescribing of medications targeting other psychiatric conditions and phenomena. There is also the possibility of a different choice of medication compared with their typically developing peers (Berney 2006; Bramble 2013).
A literature review by Rowles and Findling (2010) summarizes the evidence that pharmacological interventions are effective for managing ADHD in children and adolescents with intellectual disability. The authors also describe the scarcity of good quality studies on ADHD and pharmacological interventions in children and adolescents with intellectual disability. This predicament is compounded by these children often being excluded from such studies, despite the high prevalence and severity of ADHD in this population.
In the typically developing child, ADHD has been described as showing variable symptom profiles across the life span; behavioral problems such as conduct, oppositional, and antisocial disorders are reportedly more prominent in pubertal and postpubertal children (Hill 2005). However, this variation in symptoms across the age span has not been reported in children with intellectual disability (Neece et al. 2013). This may imply the need for differing interventions depending on the age of the patient and the presence or absence of intellectual and, indeed, other disabilities.
Gender is also known to influence expression of symptoms in ADHD. Male gender has been reported as being associated with more externalizing symptoms (Limnaiou and Turk 2012). This may in turn influence patterns of medication usage. Psychosocial circumstances have also been described as influencing the use of medications in persons with intellectual disability (Rasaratnam et al. 2004) and in those with ADHD regardless of whether they have intellectual disability or not (Harpur et al. 2008).
Rowles and Findling (2010) in their literature review describe methylphenidate as being the most extensively studied pharmacological intervention in children and adolescents with ADHD and intellectual disabilities. Other medications mentioned in their review include antipsychotics in the form of risperidone; alpha-2 adrenergic agonists such as clonidine and guanfacine; atomoxetine—a selective noradrenergic reuptake inhibitor (Harfterkamp et al. 2012); and cholinergic agents such as donepezil.
Possible medications used in managing ADHD, especially in children and adolescents with intellectual disability, also include mood-stabilizing agents such as sodium valproate (Torrioli et al. 2010), bupropion, and selective serotonin reuptake inhibitors (Hazell 2007). Furthermore, sleep disruption is common in both ADHD and intellectual disability, hence the use of sleep-promoting agents such as melatonin (Turk 2010a) or ADHD medications with calming properties such as the alpha 2 agonist clonidine (Ingrassia and Turk 2005).
There is increasing pressure for more inclusive services incorporating equality in quality and quantity of care for all persons irrespective of their disabilities (Department of Health 2004; Bernard and Turk 2009). It is therefore important to study current intervention patterns for ADHD in children and young people with intellectual disability and to compare these with intervention patterns for more able children and young individuals who have ADHD. This will help to establish if there are any significant differences in intervention patterns from those commonly applied to children and young individuals without intellectual disability and, if there are, to determine whether these differences are moderated by factors such as age, gender, and living circumstances.
Aims and Objectives
The purpose of this study was to explore patterns of pharmacological interventions for ADHD in children and adolescents with intellectual disability, comparing them to those individuals with average development and ADHD. The study also sought to identify the influence of factors such as living circumstances, gender, and age on pharmacological interventions.
The hypothesis tested was that pharmacological interventions for young individuals aged 5–18 years with ADHD and intellectual disability are different from those for 5–18-year-olds with ADHD, but no intellectual disability, and that the differences are influenced by age, gender, and living circumstances.
Methodology
A case–control cross-sectional design was used in this study. Potential participants were identified from already existing clinical record databases, which were used to identify a case population group; inclusion criteria comprised an age range of 5–18 years and diagnoses of intellectual disability and ADHD. A comparison group was selected of individuals aged 5–18 years with a diagnosis of ADHD, but no intellectual disability, matched groupwise for gender.
Furthermore, they were as follows: (a) Individuals diagnosed with ADHD and receiving or having previously received medication for ADHD within specialist Child and Adolescent Mental Health Services (CAMHS). (b) Individuals who have used medication continuously for a minimum of 6 months. The medications recorded as used are those identified in the literature review as above. (c) Case group participants required a recorded axis III diagnosis of ICD-10 mental retardation (equivalent to DSM-5 intellectual disability) (American Psychiatric Association, 2013) and also an axis I diagnosis of disorders of attention and activity—hyperkinetic disorders (equivalent to DSM-IV & DSM-5 ADHD) (American Psychiatric Association, 2000, 2013) using the multiaxial classification systems (World Health Organization 1992). The comparison group, while prescribed ADHD medication, did not have a significant intellectual disability. (d) Individuals who were not recorded as having profound mental retardation or a comorbid diagnosis of a psychotic illness or a major mood disorder.
Matching
Case and comparison groups were matched on gender so as to reflect an equal number of both sexes in the two groups. Initial review of samples was undertaken to establish similarities in demographic distributions.
Comparison individuals were chosen by means of stratified random sampling. Strata were divided to reflect the gender distribution of the selected cases—the male: female ratio was 90:17. The randomly selected comparison individuals were also analyzed (as much as possible without rendering ineffective the initial random selection) to ensure that they were close in demographic distributions to the case group.
Sample size
The database identified a total of 2784 children and adolescents with a diagnosis of ADHD. Of these, 263 met the criteria for the diagnosis of ADHD and associated intellectual disability and 2521 for a diagnosis of ADHD and no axis III diagnosis (see breakdown under the Results section).
Of the 263 individuals initially identified with both ADHD and intellectual disability, only 107 met the other conditions above for inclusion in the study, These 107 individuals were selected as the case group.
The Clinical Record Interactive Search (CRIS) database was developed in 2008 by a team from the National Institute of Health Research of the Biomedical Research Centre (NIHR BRC) for Mental Health at the South London and Maudsley (SLAM) NHS Foundation Trust and King's College, University of London. In late 2012, it was reported to have over 200,000 fully anonymized mental health records and has produced research information that has been helpful in formulating service policies for persons with mental health disorders. It is the largest of such known databases in Europe (KCL News, 2012).
Power calculation
Using a population size of 107 in each arm of the study, a power calculation of 0.7 was determined. The type 1 error (α) is 0.05 and the type 2 (β) error is 0.3.
Outcome measures
• Concurrent use of medications: Concurrent use of more than one ADHD medication for a continuous period of 6 months was referred to as cases on multiple medications. The use of only one medication was referred to as cases on single medication.
• Types of medications: Medications were grouped as stimulants and nonstimulants. The stimulant group of medications comprised dexamphetamine and methylphenidate preparations. The nonstimulant category comprised medications listed in the literature review, other than methylphenidate or dexamphetamine.
Clinical letters and clinicians' correspondence were used to decide the first-line medication and the add-on medications. In cases of augmentation treatments, the medication initiated first was regarded as the first-line medication. Records were reviewed to ensure that augmentations were used concurrently for at least 6 months.
Demographic factors
A younger age group was defined as 5–11.99 years old; an adolescent age group as 12–18 years old. Gender was as recorded on the database.
Family living circumstances were defined as living with both parents, single parent, local authority care, and residential school placements. These data were collapsed into two broad groups: living with family (those living with both or one parent) and living away from family (living in residential school or local authority care).
Data analysis
An initial descriptive analysis was done to establish the demographic distribution of both case and comparison data. This analysis also identified potential outliers and patterns of data distribution.
Inferential analysis of data was done to determine the existence of a true difference (if one did exist) between the groups in terms of the two outcome measurements described above. The null hypothesis was tested using the Pearson chi-squared test. The Pearson coefficient asymptotic value of 0.05 was taken as being significant in rejecting or accepting the null hypothesis.
Influences of the demographic factors were tested using the Pearson chi-square test. An asymptotic value of 0.05 was taken as significant. Any observed difference or nondifference between the groups in terms of type or concurrent use of medication was analyzed (as a 3 × 2 table) to establish the influence of the demographic factors.
Results
The male-to-female ratio in both groups was 8.5:1.5. There were slightly more adolescents over the age of 12 years in the comparison group. The mean ages were 10.934 and 12.234 years and the median ages were 10 and 13 years for the case and comparison groups, respectively. In both groups, most children and adolescents were living with both parents. There were also no significant between-group differences in terms of living with a single parent. Living in a residential school placement was more frequent in those with intellectual disability, with a ratio of almost 9:1 compared with those without intellectual disability. Records about living conditions were not obtainable or easily accessible for 31 of the children and adolescents in the case and comparison groups. Of these, 15 were in the case group and the rest in the comparison group (see Table 1).
SD, standard deviation.
In terms of first-line medications used, there were no differences in the generic medications used in both groups. The most commonly used first-line ADHD medication in both groups was the osmotic release oral system, Methylphenidate-Concerta XL (33.6% in both groups). There was a higher use of atomoxetine (20.6%) in the case group compared with the comparison group (13.1%). Similarly, all other nonstimulant-based medications such as clonidine (5.6%: 3.7%); antidepressants (2.8%: 0.9%); and mood stabilizers (0.9%: 0%) had a higher use as the first-line pharmacological intervention for ADHD in the case group. No significant differences were observed between the first-line medications used in both groups (p = 0.14). The study also revealed an equal amount of antipsychotic usage in both groups. See Figure 1.

1st-line generic medication distribution.
When first-line medications were grouped into stimulants, nonstimulants, antipsychotics, sleep enhancers, and others, there appeared to be a higher (60%) use of stimulant-type medications in the comparison group. This lesser use of stimulants in those with intellectual disability was accounted for by the more frequent use of clonidine and atomoxetine in the case group children and adolescents with intellectual disability (see Fig. 1).
Nonstimulants had a higher tendency (25.2%: 16.8%) to be prescribed as the first-line medication in the case group. There were equal frequencies in the use of antipsychotics in the groups, the most commonly prescribed antipsychotic being risperidone, followed by aripiprazole. A modestly higher prescription of sleep enhancers was observed in the case group—the most commonly used being melatonin preparations.
There were no significant differences between children and adolescents with intellectual disability and those without intellectual disability in terms of concurrent use of more than one ADHD medication or not. There were 77 instances of concurrent multiple medication use observed in the study. Of these, 56% were in children and adolescents with intellectual disability and ADHD (case group) and 44% in the comparison group (Table 1). There were two instances of four different types of ADHD medications being prescribed concurrently for a period of 6 months or more in the case group. In each instance, the medications used included mood stabilizers and sleep enhancers. In cases of concurrent multiple medication use, the most commonly used additional medications were sleep enhancers, then mood stabilizers, followed by antipsychotics, and then antidepressants.
Those under 12 years old with intellectual disability and ADHD were more likely (66.2%) to be prescribed and to be established on nonstimulant medication than the comparison group (33.8%; p = 0.024). This was the only statistically significant difference observed between the groups. In those over 12 years old, there was a higher use (57.5%) of stimulant-type medications in the intellectual disability group compared with the comparison group (42.5%). Overall, when the moderating factor of age group (younger and older age) was removed, no difference was observed.
The family living conditions did not show between-group statistically significant differences in terms of medication used (stimulant/nonstimulant) or in terms of medication events (single or multiple). Children and adolescents with intellectual disability were more likely to be in a residential school placement than those without intellectual disability (Table 1). Children and adolescents with intellectual disability and ADHD who were living away from family were more likely to be established on stimulants (59.6%). There was a trend toward higher use of stimulants than nonstimulants in those living away from family (Figs. 2 and 3).
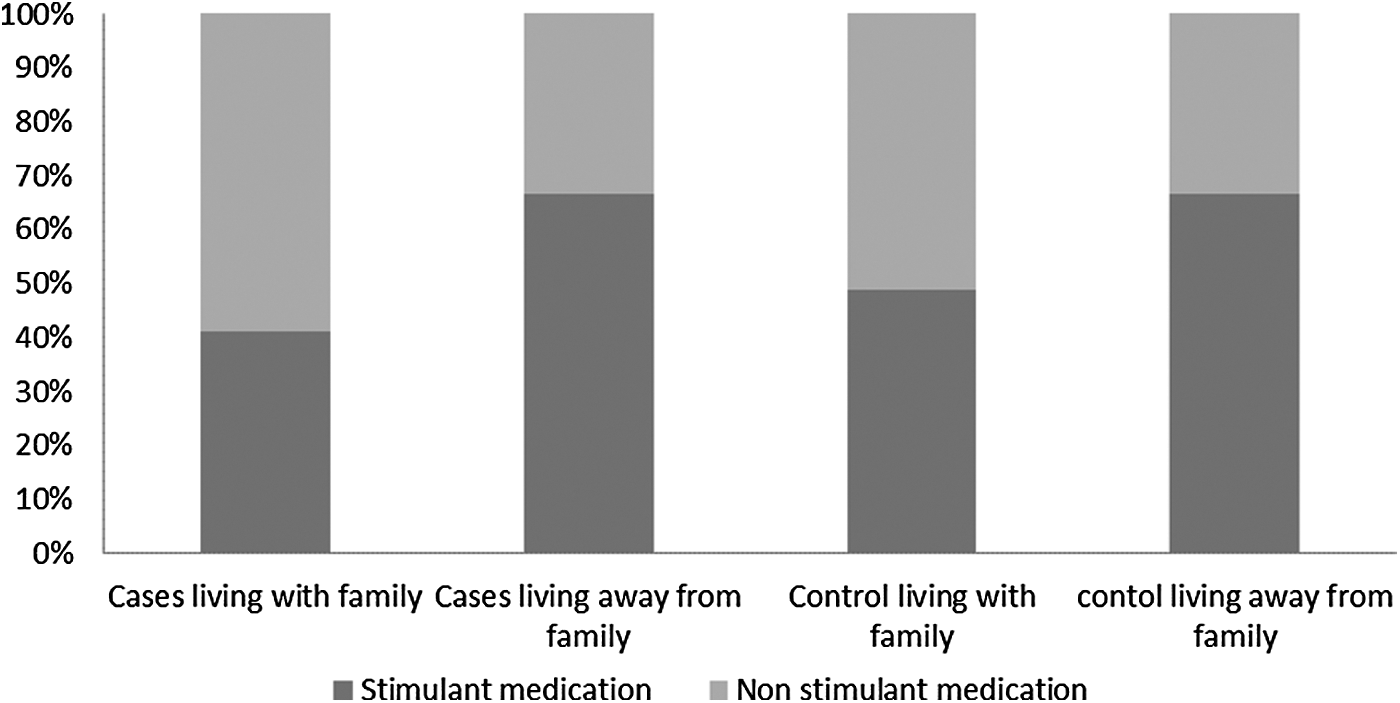
Living circumstance—type of medication.
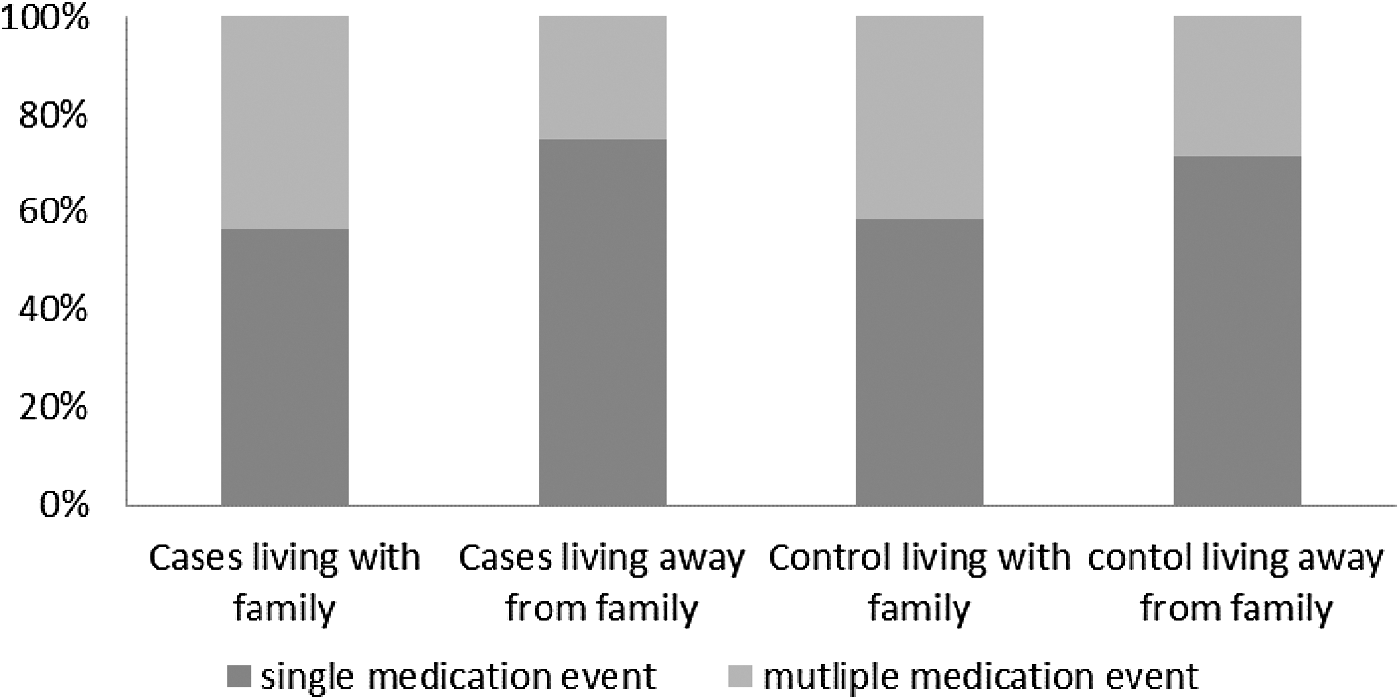
Living circumstance—medication events.
The family living conditions appeared to have an even spread in both cases and comparison in terms of medication events. There was a trend toward frequent occurrence of single medication across both groups irrespective of whether they were living with family or not.
Gender did not differentiate the two groups in terms of outcome measures. Females generally had a higher tendency to have a single medication if they had intellectual disability and ADHD (case group) compared with the comparison group. The use of nonstimulant medications was higher in females with intellectual disability and ADHD compared with those without intellectual disability.
Analysis of odds ratio indicated that for both measured outcomes (concurrent use of more than one medication and type of medication used), the only moderating factor with statistical significance differentiating both the case and comparison groups was the age group. The study indicated that those under 12 years old with intellectual disability and ADHD are 1.8 times more likely to be prescribed a nonstimulant medication than those without intellectual disability.
Discussion
The greater use of nonstimulant medication in the younger age group with intellectual disability and ADHD (5–11.99 years) might reflect clinician reluctance to prescribe stimulant medications for children with intellectual disability because of concerns relating to reports of higher side effect profiles in them (Aman et al. 1993; Handen et al. 1999; Wigal et al. 2006). Stimulant medications for ADHD can suppress appetite and cause weight loss, may worsen tics, and can cause sleep difficulties among other side effects (Handen et al. 1999; Paykina and Greenhill 2008; Turk 2014).
However, this may not be sufficient explanation for the significantly lesser use of stimulants in children aged 5–12 years who have ADHD and intellectual disability. It may also reflect reluctance to treat children and adolescents who have an intellectual disability and ADHD with medications normally used in the management of typically developing children with ADHD.
Another possible explanation for the findings from this study is the common pitfall of diagnostic/treatment overshadowing (Reiss et al. 1982; Jones et al. 2008). Thus, features of ADHD are seen as the expected behavior rather than recognizing it as a possible mental health comorbidity requiring treatment and intervention in its own right. As observed in this study, even though there is a diagnosis of ADHD, the treatment is still statistically significantly different depending on the presence or absence of intellectual disability, especially in younger-aged children.
Berney (2006) suggests that children and adolescents with ADHD and intellectual disability are less responsive to stimulant medication. He argues that this may be, in part, due to overdiagnosis, as opposed to diagnostic overshadowing. He explains that clinicians, rather than looking for other explanations or appreciating the degree of disability or communication difficulties in a child trying to complete a task, tend to infer problems of attention, hyperactivity, or impulsivity. Berney also suggests that the greater rate of poor responses to stimulants may be because of misdiagnosis as it is common for children and adolescents with intellectual disabilities to have underlying poorly controlled epilepsy or anxiety as well. He suggests that it is not unusual for treatment to start later in the intellectually disabled child, possibly because of diagnostic overshadowing.
The statistically significant finding in this study may also be an artifact caused by the selection process of the comparison group. Matching of the groups, genderwise, was considered important. However, this may have led to the comparison group having been inadvertently depleted. This is probably unlikely as all possible moderating factors, including age and psychosocial status (living conditions), were analyzed and well adjusted for in both groups. Indeed, descriptive analyses confirmed that both cases and controls were similar in their demographic distributions.
The greater usage of sleep enhancers as not only first-line but also as add-on medication in the case group is consistent with the literature showing sleep difficulties to be more common in those with intellectual disabilities than in the general population. The association between intellectual disability and sleep-related problems has been well established and reviewed in several reports (Quine 1991; Turk 2010a). A worsening of challenging ADHD-type behaviors has also been reported to be strongly correlated with sleep problems in children and adolescents (Wiggs and Stores 1996). Sleep difficulties associated with neurodevelopmental disabilities have been shown to respond to clonidine (Ingrassia and Turk 2005). Of all the clonidine prescribed as first-line medication, 60% was for children and adolescents with intellectual disability. However, as an add-on medication, there was equal representation in the use of clonidine in both groups.
Limitations
There are other possible factors influencing choice of medication that were not considered in this study. These include parental social class, their levels of education, and family income. It may be that these variables reflect family likelihood of receiving pharmacological versus other therapeutic options. Carers who are not empowered by reason of limited cognitive ability, or poor social status and resources, may also not be able to advocate successfully for their children to have one modality of intervention rather than another.
In recruiting the case group, intellectual disability was considered as a single homogeneous group. In reality, severity of intellectual disability does correlate with other comorbidities. For example, this study did not exclude persons who may have had a diagnosis of having epilepsy, which in itself could have accounted for at least some of the mood stabilizer prescriptions, given their benefits for epilepsy as well as fluctuating mood disorders.
The database used in this study has information on patients who have received interventions from a specialist mental health service trust. The service covers a geographically widespread urban community with significant sociocultural diversity. Even though all prescribing was initiated by psychiatrists working in the same trust, some variations in individual prescribing practices may exist. The database is anonymized and therefore it is not feasible to establish if the findings from this study are due to an individual clinician's practices or influenced by the specific geographical locations of the clinics.
Conclusion and Clinical Significance
Medication is frequently used for ADHD in children and young individuals, whether or not they have intellectual or indeed other developmental disabilities, singly or in combination.
The observed significant difference between children and adolescents with or without intellectual disability in terms of type of first-line medication (nonstimulant as against stimulant) used being influenced by the age group is clinically relevant. Further scientific exploration is needed to confirm whether there are genuine clinical reasons for this differential prescribing practice and to develop evidence-based guidelines to good practice in this under-researched field.
Disclosures
S.O. has been a speaker at academic programs sponsored by pharmaceutical companies (Eli Lilly—manufacturer of Strattera—and Flynn Pharmaceuticals—manufacturer of Medikinet). He has received payments for speaking at such events. J.T. has in the past received payment for contributions made to academic meetings organized by Novartis (manufacturer of Concerta XL) and Flyyn Pharmaceuticals (manufacturer of Medikinet XL).