
Abstract
Objective:
Psychostimulant medication is considered a mainstay in the treatment of attention-deficit/hyperactivity disorder (ADHD); however, research suggests that the typical duration of medication treatment for children and youth may be <3 years. The purpose of this study was to evaluate the psychostimulant treatment persistence for children and adolescents in New South Wales, Australia.
Methods:
This study used survival analysis to assess duration of medication treatment on a large administrative database of children and youth from New South Wales, Australia. Several models were fit to evaluate differences in survival rates among decades (1990–1999 vs. 2000–2010), gender, and age.
Results:
Results showed that: 1) Overall median treatment time (i.e., median survival time) was 1.96 years (99% CI=1.93, 1.99); 2) there were small, but significant changes over time in duration of treatment; 3) females had shorter treatment duration than males; and 4) there were relatively large differences in treatment duration across age groups.
Conclusions:
These results indicate that the majority of children and youth receive medication treatment for only a small portion of childhood/adolescence, and that there are differential patterns in treatment duration across age groups.
Introduction
A
Medication treatment is considered a mainstay for ADHD because, in most cases, psychostimulants such as methylphenidate have been shown to be effective in the management of ADHD (MTA Cooperative Group 2004). The number of children and adolescents who receive medication treatment has increased markedly over the last two decades (Castle et al. 2007; Visser et al. 2007). Although psychostimulants are an effective component of treatment, significant concerns have arisen over high rates of medication discontinuation, often after one initial filled prescription (Adler and Nierenberg 2010; Charach and Fernandez 2013). Medication persistence (i.e., maintaining medication treatment over time) has been linked to characteristics of health systems, patients and medications (for recent reviews, see Adler and Nierenberg [2010] or Charach and Fernandez [2013]).
Despite our increased understanding of ADHD's protracted course, limited guidance exists on the optimal length of time patients should be maintained on psychostimulants. There is some indication that longer-term (>2 years) medication may be associated with improved standardized academic achievement (Langberg and Becker 2012), but there is insufficient evidence to develop clinically relevant guidance on what represents the optimal length of time. The 2007 practice parameters by the American Academy of Child and Adolescent Psychiatry do not address recommended duration. They recommend only that treatment should continue as long as symptoms remain present and cause impairment (Pliszka 2007).
A recent review of adherence, persistence, and medication discontinuation in patients with ADHD showed average treatment persistence of 136 days (Gajria et al. 2014). Studies from community-based samples show wide ranges of medication persistence. Bussing reported that in one Florida school district, ∼50% of students discontinued medication after 2 years (Bussing et al. 2005). Similarly, Reid et al. (2002) found that in South Australia, the mean duration of medication use was a little more than 2 years. The results of several studies using large data sets of children and adolescents receiving mediation treatment reported courses of medication treatment ranging from 4 to 19 months (Miller et al. 2004; Marcus et al. 2005; Barner et al. 2011).
Shorter medication persistence in community samples might reflect an insufficient level of follow-up support (e.g., lack of physician monitoring). However, similar length periods of persistence have also been noted among children enrolled in medication studies, who presumably would receive high levels of support. For example, Thiruchelvam et al. (2001) found that 48% of 63 children ceased medication within 3 years, whereas Atzori et al. (2009) reported that 54% of children had ceased medication at 3 years. In contrast, Charach et al. (2004) reported a much lower 5 year cessation rate of 42% for 79 students enrolled in a medication trial in Canada.
Studies using survival analysis have also found that treatment durations are relatively short. For example, 3 year cessation rates of 60–100% were reported in three studies (Miller et al. 2004; Trip et al. 2009; Hodgkins et al. 2011), whereas 4 year cessation rates of 52–73% were reported by Zetterqvist et al. (2013) and Wong et al. (2009). These studies also reported potential moderators. Zetterqvist et al. (2013) found higher survival times among 6–14-year-olds than among 15–21-year-olds. Trip et al. (2009) found that girls had lower survival times than boys. Additionally, Wong et al. (2009) found that those who began treatment between 2004 and 2006 were 40% less likely to cease treatment than were those who began between 1999 and 2003, which suggests that there was some change in persistence over time.
The available data vary widely in their estimates of the time children and youth persist with medication treatment. In part this is likely a function of the varying criteria used to define cessation. Very short periods of persistence, such as those reported by Barner et al. (2011) and Marcus et al. (2005), used 30 days as a criterion for cessation. Meanwhile, studies using a longer criterion for cessation tended to report longer periods of persistence with medication (e.g., Thiruchelvam et al. 2001; Trip et al. 2009; Zetterqvist et al. 2013).
In addition, the samples used could also have affected persistence. For example, some of the longest periods of persistence were reported in studies in which participants were enrolled in clinical trials and had relatively small sample sizes and, therefore, may not be representative (Thiruchelvam et al. 2001; Charach et al. 2004). Other studies used Medicaid groups, who also might not be representative of the population (Marcus et al. 2005; Barner et al. 2011). The use of different age ranges across studies may also have affected estimates, as the age when medication is initiated may be a moderator of persistence. Another potential source of variability across studies is that persistence with medication may be changing over time. The rate of psychostimulant medication use for ADHD increased dramatically in the early 1990s. As medical practitioners became more accustomed to prescribing psychostimulant medication, it is possible that treatment practices changed. Only two studies used a time frame sufficient to examine the possibility of change over time (Trip et al. 2009; Wong et al. 2009), and the longest was limited to 10 years. Finally, it should be noted that six different countries were represented in the abovementioned studies, and that differences in persistence could be a result of differences in treatment practices across these countries.
Given the importance of effective treatment for ADHD and the significant role of medication persistence, the aim of this study was to provide an additional estimate of persistence with medication among children and adolescents ages 5–17 using a large, representative sample drawn from the state of New South Wales (NSW), Australia over two decades, 1990–2010, and to assess possible moderators of persistence. We hypothesized that there would be: 1) Difference in persistence across the decades, with 2000–2010 having shorter persistence than 1990–1999; 2) differences in persistence across age groups, with younger subjects having longer persistence than older ones; and 3) differences across boys and girls, with boys having longer persistence.
Methods
Data source
In NSW, the stimulants dexamphetamine and methylphenidate are considered drugs of addiction, and prescriptions are regulated by the NSW Ministry of Health (MOH). Physicians must secure approval from the MOH to prescribe dexamphetamine, lisdexamfetamine (Vyvanse), or methylphenidate (Concerta, Ritalin, Ritalin LA) for the treatment of ADHD, and prescriptions have been tracked by the MOH since 1985. There are two types of approval: General approval and individual patient approval. General approval is only available to pediatricians, and psychiatrists who are members of the NSW Faculty of Child and Adolescent Psychiatry of the Royal Australian and New Zealand College of Psychiatrists. Physicians who have been granted general approval may prescribe stimulant medication to treat children with ADHD without the need to obtain individual MOH approval for each child, providing certain routine prescribing criteria are met: 1) Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for ADHD must be met, 2) the child must be ≥4 years of age, 3) the prescribed dose cannot be high (>0.9mg/kg/day for dexamphetamine; >1.8mg/kg/day for methylphenidate), and 4) there cannot be significant side effects, evidence of psychiatric comorbidity, or a preexisting tic disorder.
Generally approved physicians prescribe for children who meet the routine prescribing criteria and must notify the MOH of prescriptions on a monthly basis. Physicians must provide details of the child, including his or her name, date of birth, postal code and suburb or town of residence, the drug and daily dosage prescribed, and the date for each prescription written. Except for cases for which individual authorizations are required, prescriptions for drugs of addiction are valid for 6 months from the date they are written. The great majority of prescribing occurs under general approval.
Individual approvals are required for patients who do not meet the routine prescribing criteria. Physicians other than pediatricians or child psychiatrists (e.g., general practitioners in pediatric oriented practices, general practitioners with pediatric training working in rural areas) may apply to the MOH to prescribe stimulants on individual basis. If approved, these doctors must procure individual approval for each child for whom they wish to prescribe stimulant medication. Individual approvals are limited to patients who meet routine prescribing criteria, and are granted in the form of an authority. Individual authorities are issued for no longer than 12 months.
Data for prescriptions are kept in the Pharmaceutical Drugs of Addiction System (PHDAS), a computerized administrative database used by the Pharmaceutical Services Unit within the NSW MOH. It is used to facilitate the authorization of medical practitioners to prescribe drugs of addiction. Unique identifiers are kept for each patient, which allows for longitudinal tracking of prescriptions for each patient. At present, the PHDAS holds records for ∼100,000 patients who have received medication. After receiving NSW Population and Health Service Research Ethics Committee approval (ref: HREC/13/CIPHS/18), the MOH provided us with records for all patients 5–17 years of age who had received their first prescription for psychostimulant medication for ADHD between 1990 and 2010. This resulted in an initial data set of 88,204 persons.
Because the survival model used for analyses (discussed subsequently) assumes that each individual experienced a single episode of risk, we included only individuals with continuous treatment. Continuous treatment was defined as treatment with prescription gaps of <1 year. Individuals who started medication, ceased for >1 year, and subsequently restarted were excluded from the analysis. We purposely used a very conservative gap criterion for two reasons: 1) This definition allowed for drug holidays or other temporary interruptions in treatment, and permitted focus on long term stimulant use as opposed to individual treatment bouts; and 2) a shorter gap period (e.g., 30–60 days) could potentially downwardly bias the duration estimates because psychostimulant nonresponders would be over represented. This approach resulted in 69,903 cases. Table 1 lists the demographic characteristic for the final sample and those excluded. The censor date was May 2012. Of the total cases, 12.4% (n=8691) were censored (i.e., still receiving treatment at the time of data collection May 2012) .
ADHD, attention-deficit/hyperactivity disorder.
We determined the age at which individuals began psychostimulant medication by subtracting their date of birth from the date of their first prescription. Duration of psychostimulant medication treatment was calculated for each individual. The cessation date was the last date that an individual with continuous treatment was authorized to be prescribed medication. This was determined either through the cessation date (in an individual approval record) or by adding 6 months to the last recorded prescription date (in a general approval). Subtracting the cessation date from the date when medication was initially authorized provided the length of time individuals were authorized to receive medication. To avoid overestimating the duration of treatment, we subtracted out any time that an individual was not authorized to receive medication (e.g., if an individual was authorized over a calendar period of 3 years, but had a 6 month gap with no prescriptions, the duration of treatment would be 2 years 6 months).
Data analysis
Survival analysis was used to assess the degree to which treatment cessation differed among start decade, gender, and age groups, as well as to derive median and mean survival times and 99% confidence intervals. Survival analyses were calculated using the Kaplan–Meier method (Kaplan and Meier 1958) and Cox regression (Cox 1972) approaches. The Kaplan–Meier method directly estimates survival times and survival curves (the proportion of youth still receiving treatment at any time). Mantel–Cox tests (Mantel 1966) were used to test for differences among survival curves derived from the Kaplan–Meier method. Cox regression (also referred to as the proportional hazards model), was used to estimate the simultaneous effects of multiple predictors on the hazard functions, and to yield parameter estimates that could be transformed into effect sizes.
Hazard in the Cox model is reexpressed using a log transformation, because the logarithm of a rate has a lower bound of zero and no upper bound, which provides a properly constrained set of values for the model to reproduce (see Mosteller and Tukey 1977 or Box and Cox 1964 for an explanation of transformation in survival modeling). Because hazard is transformed from the raw scale to the log scale, parameters from the Cox model can be expressed as the effect of the log scale and as an effect on the raw scale. The effect expressed on the raw scale is referred to as the hazard ratio (HR) that is expressed as the multiplicative increase in the hazard rate (i.e., probability that an individual will cease treatment in a given time period) for the focal group relative to the reference group's hazard rate. The 99% confidence intervals for HRs were computed to provide the precision of the estimates. The statistical significance of the HR was assessed using the Wald test (w), where the degrees of freedom are equal to the number of predictors in the model.
Results
For the entire population across both decades, survival times ranged from 0.01 to 20.00 years with a median survival time of 1.96 years (99% CI=1.93, 1.99) and mean survival time of 3.09 years (3.06, 3.12). We also report the median survival time (i.e., the point at which 50% of individuals have ceased treatment) subsequently, because survival times are strongly positively skewed and the median times are less sensitive to the effect of outliers (e.g., individuals with long-term persistence). For the following results, we report the results of Cox models for each predictor, because a multivariate model (simultaneously testing all predictors) did not differ substantively from the bivariate models.
Decade
The median survival time for youth who started treatment between 1990 and 1999 and between 2000 and 2010 was 2.01 years and 1.79 years, respectively. Therefore, the typical duration of medication treatment for youth starting in 1990–1999 was 2.63 months longer than for youth in 2000–2010. The survival curves (presented in Fig. 1) differ significantly as indicated by the Mantel–Cox test (χ2 MC (1)=22.85, p<0.0001). The HR was 1.04 (1.02, 1.06) (w=22.57, p<0.0001) when 1990–1999 was the reference group, indicating that youth who started treatment in 2000–2010 were, at any given time point, 4% more likely to cease treatment than were youth who started treatment in 1990–1999. Therefore, although the difference was statistically significant, the effect size was small.
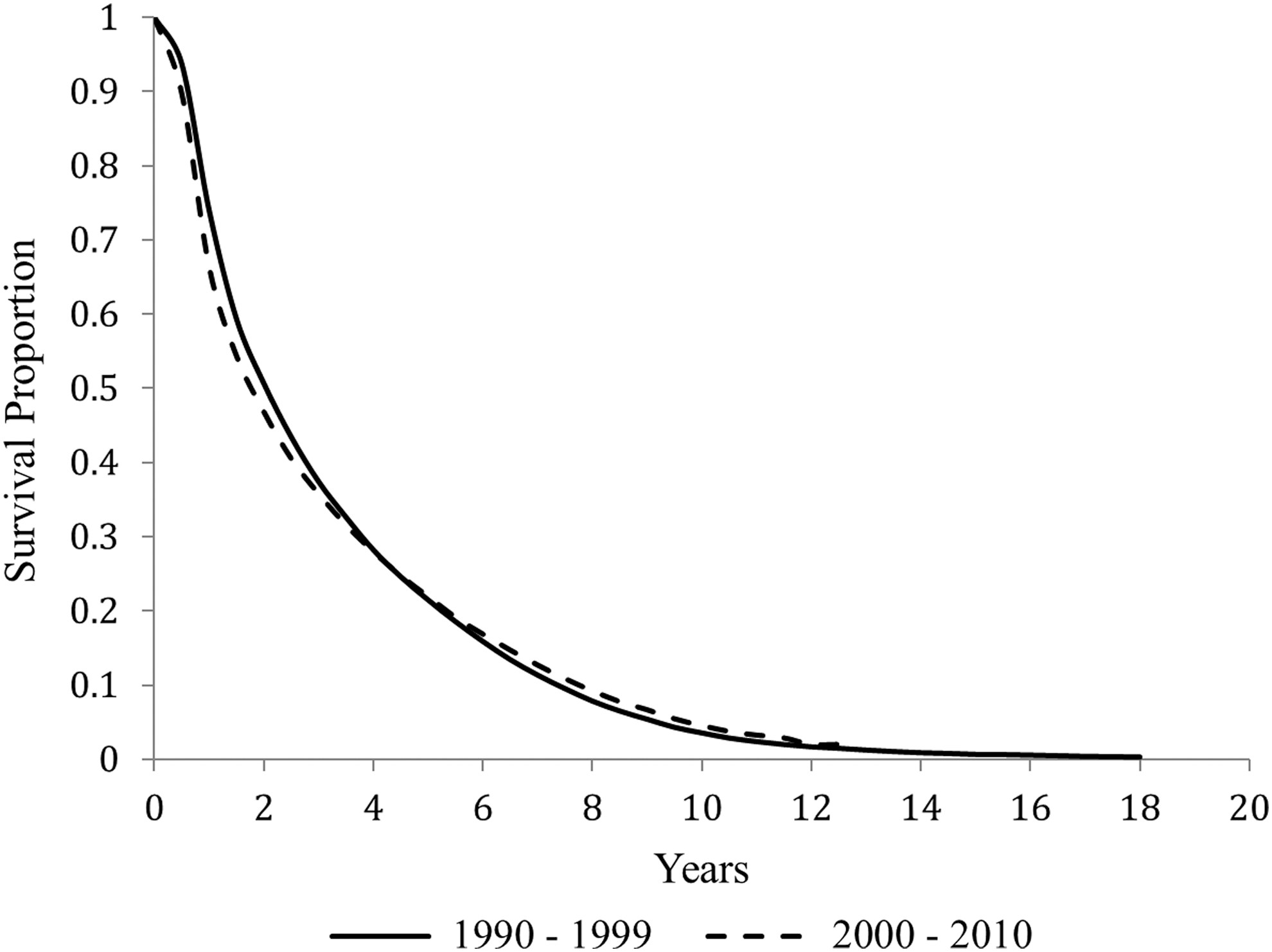
Survival curves by decade (proportion of youth still receiving psychostimulant medication).
Gender
The median survival time for females was 1.64 years and for males was 1.99 years; therefore, the typical duration of treatment for females was 4.2 months shorter than the typical duration for males. The survival curves for females and males (presented in Fig. 2) differed significantly (χ2 MC (1)=37.81, p<0.0001). Visual inspection of the survival curves confirms that there is a small, albeit nonuniform, difference between males and females, with males having a higher survival rate over the majority of time points. The HR was 1.06 (1.04, 1.09), (w=37.33, p<0.0001) when males were the reference group, indicating that females were, at any given time point, 6% more likely to cease treatment than were males.

Survival curves by gender (proportion of youth still receiving psychostimulant medication).
Age
The median survival times for youth who initiated psychostimulant treatment between the ages of 5 and 9 years, 10 and 14 years, and 15 and 17 years were 2.63, 1.50, and 1.00 years, respectively. The typical length of treatment for the youngest group was 13.92 months and was 19.56 months longer than the typical treatment for the middle and oldest groups, respectively. The typical length of treatment for the 10–14-year-old youth was 6 months longer than the typical treatment for the oldest youth. The survival curves, displayed in Figure 3, differed significantly across the three age groups (χ2 MC (2)=6449.69, p<0.0001). The Cox model demonstrated that the 5–9 year age group differed significantly from both the 10–14 year group (HR=1.74 [1.70, 1.78], w=4002.13, p<0.0001) and the 15–17 year group (HR=2.56 [2.46, 2.66], w=3746.36, p<0.0001). The HRs indicate that the differences across ages are both statistically significant and of meaningful practical significance. Children who initiated psychostimulant treatment between the ages of 10 and 14 years were 74% more likely to cease medication, at any given time point, than were children ages 5–9. Meanwhile, adolescents who initiated psychostimulant treatment between the ages of 15 and 17 were 156% more likely to cease medication than were children ages 5–9.
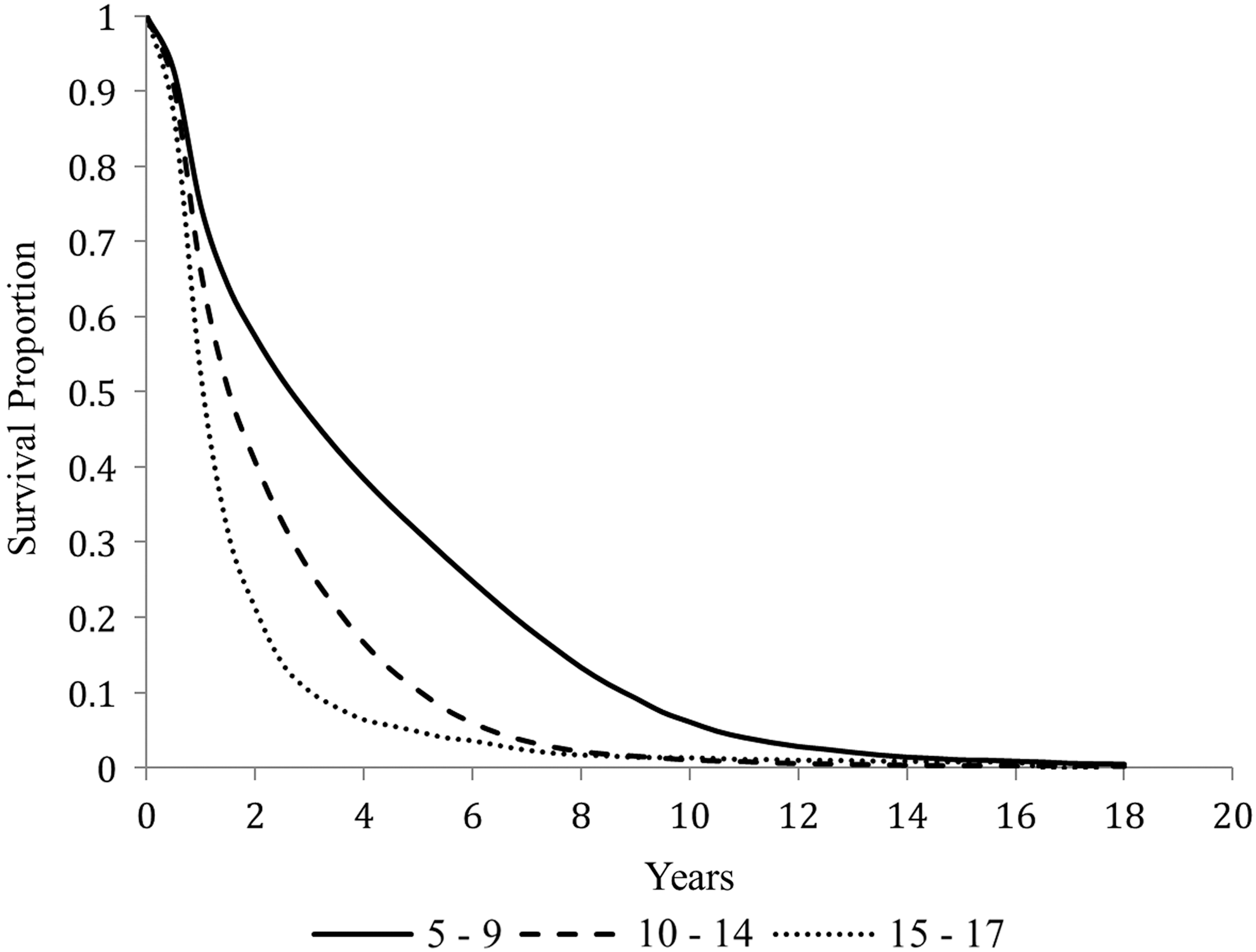
Survival curves by age group (proportion of youth still receiving psychostimulant medication).
Discussion
The results of this study are consistent with previous research and strongly suggest that the great majority of children or youth receive psychostimulant medication treatment for <5 years. The average child in this study would begin medication at age 10 and discontinue medication by age 12. This poses a potentially serious clinical treatment concern. Children and youth who receive psychostimulant medication for ADHD may constitute a more severely impaired group with more serious symptoms and increased rates of comorbid conditions than children who receive only nonmedication treatments (Hechtman 2006). If the majority of those children and youth using medication cease after <2 years, then they may be at increased risk for adverse outcomes in educational and social domains unless other supports (e.g., psychosocial treatments) are available. Interestingly, other studies have shown that children who received medication alone are significantly more likely to cease treatment than those who receive combined treatment (Stein et al. 2012).
The survival curves in the present study demonstrate that within 1 year, ∼30% of children have ceased medication. This most likely reflects those individuals who either do not respond positively to medication or who cannot tolerate medication (Toomey et al. 2012). However, patterns of cessation continue past the first 12 months, until by year 5 nearly three quarters of the children have ceased medication. Exactly why youth cease medication after the 1st year is not well understood. Some factors that have been suggested are perceived stigmatization, lack of parent/family support, parental concerns over long-term treatment, skepticism of the value of medication, and children's dislike of the effects of stimulants (Swanson 2003; Hansen and Hansen 2006; Moses 2011). It is also possible that the effectiveness of medication diminishes over time for some children (Jensen et al. 2007). Some research suggests that for some children, symptom remission occurs after medication treatment (Atzori et al 2009). After year 5, the rate of cessation begins to decrease, with ∼25% of the children still receiving medication. However, these individuals are a distinct minority, and the factor(s) that result in this level of persistence are not well understood.
Decade, gender, and medication start age all were statistically significant moderators of persistence. Our results found that median survival was shorter by 2.63 months for the decade 2000–2010 than for 1990–1999. This is consistent with previous studies on other Australian groups (Prosser and Reid 2009) and suggests that there may be changes in treatment patterns in Australia. In contrast, Trip et al. (2009) found an increase in survival over time in the Netherlands, although the magnitude is not reported, and Wong et al. (2009) reported that for 15-year-olds in Great Britain, there was a 40% less likelihood of cessation in 2004–2006 than in 1999–2003. These results suggest that there may be differences in survival times across nations. We would caution, however, that it is not clear whether these differences in gender survival times are meaningful. Previous studies reported mixed findings on the effects of gender. Trip et al. (2009) found significant differences, but Wong et al. (2009), Zetterqvist et al. (2013), and Bussing et al. (2014) did not. Our results suggest that gender has only a small effect on persistence.
Consistent with previous research, start age is a powerful moderator of survival time (Barner et al. 2011; Zetterqvist et al. 2013). The individuals most likely to demonstrate longer survival times were the 5–9-year-old age group, followed by the 10–14-year-old group. For those who initiated medication at 15 years of age or later, medication treatment lasted ≤2 years for ∼80% of individuals. The likelihood of cessation increases over time for both groups compared with the 5–9-year-old group. One possible explanation for the differences is that the groups differ in terms of the degree of impairment and the availability of supports. Many of the children identified at an early age may be those who are more significantly impaired, are more likely to have a comorbid disorder, and are more likely to lack familial supports (Atzori et al. 2009). These children would experience extreme difficulty in the school and home environments, which medication could greatly alleviate. This, in turn, would increase the likelihood that caregivers would maintain medication for longer periods.
Those in the 10–14-year-old group may represent children who had fewer symptoms or a lower degree of impairment than the 5–9-year-old group. They may also have had access to more environmental supports (e.g., school services, familial supports, compensation strategies), and were able to function effectively without medication treatment until environmental demands changed with the advent of middle school. Problems such as declining grades and temporary reversal in developmental symptoms have been noted with this age group (Langberg et al. 2008; Schultz et al. 2009). The increase in educational expectations initially resulted in the need for medication; however, as the children acclimated to the increased school demands, symptoms begin to abate again and the need for medication decreases.
The 15–17-year-old group is a small but growing group, as evidenced by the increase across decades. The increase among this group may be because of the increased attention to ADHD in adults. Why individuals would begin medication at this age is unclear. During the period of 1990–1999, this might have been because of increases in the use of medication. This group might have represented youth who would normally have received medication at an earlier age. However, this is not consistent with an increase in the proportion of the 15–17-year-old group in the following decade. The 15–17-year-old group differs markedly from others in terms of survival. For the great majority of this group, medication persistence was <2 years. It is possible that for this group, medication was a response to a transitory event or environmental change.
Limitations
The following are limitations to the study. 1) The data reflect authorizations for prescriptions. We do not know whether the prescriptions were actually filled or whether medication was administered as prescribed. 2) We could not distinguish the type of psychostimulant used (i.e. immediate release or extended release). Extended release methylphenidate has been available in Australia since 2003, and the use of extended release methyphenidate has increased 300% from 2003 to 2009 (Hollingworth et al. 2011). There is evidence to suggest that ER can increase survival time among some age groups (Miller et al. 2004). Changes over time in type of psychostimulants prescribed could have affected survival times. However, any increase in extended release psychostimulants would have increased survival times, which is contrary to our findings. 3) We cannot determine from the available data if some individuals who ceased psychostimulants began other medication for ADHD (e.g. antidepressants). 4) We excluded children and youth with significant gaps in treatment. 5) We cannot address why medication was discontinued (e.g., switched to another treatment such as psychotherapy) or whether it was discontinued appropriately. It is possible that some cessation was because of remission or decrease in the number and/or severity of ADHD symptoms and, therefore, medication was no longer needed. As we have discussed, however, this cannot be assumed.
Conclusions
The results of the present study add to others that provide a largely consistent picture of patterns of persistence with medication, as well as factors that moderate persistence. Unfortunately, what is not known is whether what occurs in practice best meets the long-term needs of children and youth. Our results show that the great major of children and youth receive medication treatment for ≤5 years; however, at present, we cannot answer the question of whether this is an optimal or even an adequate period of time. In response, we would argue that the question that should now be addressed is: What is the expected right length of medication treatment for a chronic psychiatric condition that has been seen to respond to medication? This is a complex question, but it hits at the heart of effective and efficient clinical treatment for children and youth with ADHD. Until this question can be addressed with empirical data, concerns over whether children and youth remain on medication too long (or not long enough) would appear speculative and prone to sensationalism. To address the question of “right length” requires controlled studies into outcomes as they relate to duration of medication and potential moderators. Additionally, a better understanding of why parents cease medication for their children may provide knowledge of other malleable factors that could affect persistence.
Clinical Significance
The present study's results suggest that clinical practitioners need to broaden their treatment approaches beyond solely using medications for children and adolescents with ADHD. The research findings are quite consistent (across age groups, genders, and different countries) in demonstrating that irrespective of clinical standards or guidelines, in actual practice, the great majority of children and adolescents with ADHD will spend only a fraction of their youth on medication. Unless other multimodal options are included in treatment planning, these youth are at risk of going untreated and/or unsupported, which might increase the probability of adverse outcomes for them as they move into adolescence and adulthood.
Disclosures
No competing financial interests exist.