
Abstract
Objective:
Guanfacine, in the immediate release form, remains a commonly used medication for the treatment of clinically significant hyperactivity, impulsivity, or disruptive behaviors. This article reviews the available literature regarding guanfacine use in very young children (<6 years of age), and explores some of the factors that may uniquely impact the clinical pharmacology of guanfacine in very young children and that deserve consideration when it is used in this patient population.
Methods:
The authors performed electronic literature searches in PubMed through October 2015 using the terms
Results:
Despite the fact that guanfacine is commonly used in very young children, there is a paucity of published studies that looked specifically at its use in this population. In reviewing the pharmacology of guanfacine, there are specific factors that may play a unique role in its disposition in very young children.
Conclusions:
Guanfacine is an important medication option in very young children; however, there is a significant pharmacologic “information gap,” and further research is needed to help establish appropriate, safe, and effective dosing of guanfacine in this population.
Introduction
D
Taking all of the foregoing into consideration, it becomes very clear that further evaluation of psychotropics commonly used in the clinical care of very young patients is needed. To do that effectively, we need to understand the factors that may uniquely impact efficacy of and response to specific medications in preschool patients. It is within that context that we will specifically discuss guanfacine, an alpha agonist sometimes used as a first-line treatment in preschool-age children with symptoms of hyperactivity, impulsivity, or disruptive behaviors, despite the absence of clinical trials in such patients to document its true safety and efficacy. A recent study looking at national trends in psychotropic medication use in preschoolers showed that from 2006 to 2009, almost 25% of psychotropics used in this population were alpha agonists, such as guanfacine (Chirdkiatgumchai et al. 2013). A previous study looking at prescription rates for psychotropics in a Medicaid population found that alpha agonists represented approximately one third of psychotropic drugs prescribed to patients 2–4 years of age (Zito et al. 2007). Despite this, there is only a single case series in the literature that specifically describes use of guanfacine in this population, and this included only four patients with ADHD, 2–3 years old, prescribed guanfacine for symptoms of hyperactivity, impulsivity, and aggressive behaviors (Lee 1997).
Clearly, more information is needed to effectively use guanfacine in this special population. In this review, we summarize the current body of evidence in relation to the potential dose–exposure–response relationship for guanfacine in this population, while considering contributions of ontogeny and genetic variation on its disposition and action.
Guanfacine Use in Children
After years of use as antihypertensives, alpha agonists were first studied for use in ADHD in 1985, starting with evaluation of clonidine (Hunt et al. 1985). Although clonidine has been found to have some efficacy in treating the condition, guanfacine emerged as an alternative consequent to fewer sedative and other bothersome adverse effects, along with a longer duration of action (Arnsten et al. 1988). By 1995, open-label studies were published demonstrating the benefits of guanfacine for the treatment of ADHD in children, particularly for hyperactive and impulsive symptoms (Chappell et al. 1995; Horrigan et al. 1995; Hunt et al. 1995). Subsequent studies evaluated guanfacine use in treatment of hyperactivity symptoms in specific pediatric populations, including those with Tourette's syndrome (Chappell et al. 1995), autism spectrum disorders (Posey et al. 2004; Scahill et al. 2006; McCracken et al. 2010), and intellectual disabilities (Handen et al. 2008), all demonstrating therapeutic benefit on the target symptom of hyperactivity. In addition to improvements in ADHD symptoms, guanfacine has also been demonstrated to improve tic severity in patients with Tourette's syndrome (Scahill et al. 2001). However, dosing strategies among these studies varied significantly, with doses ranging from 0.25 mg to 9 mg per day, divided among two to four administrations per day. Although some of these studies included patients <6 years of age, no study to date has specifically examined guanfacine use in that population, except for the case series by Lee (1997) noted previously. Collectively, guanfacine has been demonstrated as a viable treatment option for treatment of hyperactive and impulsive symptoms seen in ADHD. Potential cognitive effects, particularly in young children, are not well characterized.
Other medications with similar symptom targets, particularly methylphenidate, have been studied in the preschool population, most notably through the Preschool ADHD Treatment Study (PATS) (Abikoff et al. 2007). Alhough results from that trial showed clinical benefit from methylphenidate, the response was not as robust as in school-age children, and rates of side effects were higher, therefore highlighting the need to investigate other therapeutic options, such as guanfacine, for this population. As data describing the pharmacokinetics and exposure-response relationship for immediate release guanfacine in the treatment of ADHD in young children are currently nonexistent in the published literature, the age-appropriate dose of the drug is not known. Also, there may be significant variability in systemic exposure in young children because of potential age-related differences in drug disposition and/or action (Kearns et al. 2003) and because of the administration of fixed-dose tablet formulations to children of different weights, as was done in previous studies (Table 1).
ADHD, attention-deficit/hyperactivity disorder; PDD, pervasive developmental disorder.
An extended-release formulation has been shown to be effective in ADHD management, and in 2009, was approved by the United States Food and Drug Administration (FDA) for use in children and adolescents, ages 6–17 years. The half-life for this formulation is reported to be ∼2 hours longer in adults, relative to the immediate release formulation (Guanfacine Extended Release Package Insert 2011). Although relative use of long-acting alpha agonists has been rising, as of 2011, children continued to be almost three times more likely to be prescribed a short-acting alpha agonist (Fiks et al. 2015). It is likely that younger children are even more likely to be prescribed a short-acting agent, because of greater dose flexibility and the fact that many insurance company formularies do not offer coverage for the long-acting agents in children <6 years of age. In the following sections of this review, we will highlight some specific clinical factors, such as underlying diagnosis, safety/polypharmacy, and formulation, each of which can have an impact on effective utilization of guanfacine in very young children.
Important Clinical Factors
Underlying diagnosis
Appropriate treatment planning for any patient is optimized by diagnostic clarity. Although a diagnosis of psychiatric illness in preschool patients requires careful clinical assessment, evidence suggests that some disorders, such as autism spectrum disorder, can be reliably diagnosed in children as young as 2 years of age (Lord et al. 2006). Therefore, although there are no studies that look at guanfacine use in specific preschool populations, we can use data from studies that include older children to help guide clinical practice and inform development of prospective research protocols in young children. One example is that Posey et al. (2004) showed that patients diagnosed with pervasive developmental disorder (PDD) or Asperger's disorder were more likely to respond to guanfacine than children diagnosed with autistic disorder. Additionally, patients without intellectual disabilities tended to show a higher rate of response than those with intellectual disabilities. Overall, 13–39% of participants in the study were responders, depending upon the underlying diagnosis. The authors suggested that either underlying differences in pathophysiology or increased severity of baseline symptoms in children diagnosed with autism may have accounted for the response variability. It is of note that the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) has been published in the interim and no longer contains distinct diagnoses of PDD-not otherwise specified (NOS) or Asperger's disorder, with the new diagnostic criteria for autism spectrum disorder likely subsuming most of those populations (Huerta et al. 2012; American Psychiatric Association 2013).
Safety
Increased clinical use of guanfacine correlates with an increase in unintentional pediatric exposures reported to the National Poison Data System (NPDS) from 2000 to 2011 (Wang et al. 2014). Of the 6143 unintentional guanfacine exposures reported in children ≤12 years of age, 841 (13.7%) were reported as having moderate of major effects. There were no deaths reported in patients with guanfacine exposures that were reported to NPDS. Overall, the most common side effects seen with guanfacine ingestions included central nervous system (CNS) depression (28.9%), bradycardia (8.1%), and hypotension (5.8%). Rebound hypertension is another important safety concern to consider, especially with abrupt cessation of guanfacine. When prescribing guanfacine in any population, particularly in younger children, providers must be careful to counsel families and caregivers on the importance of keeping medications out of reach of children.
Drug–drug interactions
In addition to unintentional ingestions of guanfacine, polypharmacy is an ever increasing safety issue as well. With evidence suggesting rising prescription rates for psychotropics in young children, instances of polypharmacy are also on the rise in this population, highlighting the importance of considering drug–drug interactions in prescribing decisions (Zito et al. 2000; Rappley et al. 2002; Zito et al. 2007). Stimulants are the most common class of medications coadministered with guanfacine, and there have been previous concerns about the safety of combining stimulants and alpha agonists (Popper 1995). A recent study also reported heightened autonomic response caused by guanfacine and amphetamine interaction (Gaiser et al. 2015). Importantly, there have been previous analyses of guanfacine extended-release coadministration with methylphenidate, demonstrating stable pharmacokinetic profiles (Roesch et al. 2013). Other potentially important interactions also exist. For example, carbamazepine and oxcarbazepine, each of which can be utilized as an antiepileptic or mood stabilizer, are both strong inducers of CYP3A4. Although coadministration of guanfacine with such agents is not common in the general preschool population, they are sometimes prescribed in young patients with underlying epilepsy. Coadministration of either of these drugs with typical guanfacine doses may mitigate the desired therapeutic effects of guanfacine by enhancing its biotransformation, and thereby, reducing its systemic (including CNS) exposure. However, potential clinically relevant interactions with other coadministered drugs may also need to be considered when guanfacine is prescribed, especially in young children, in whom its metabolism may be expected to change as a function of age.
Formulation
Immediate-release guanfacine is typically provided in 1 mg fixed-dose tablets, whereas typical starting doses range from 0.25 to 0.5 mg per dose in preschool patients. This necessitates use of a pill cutter to administer the prescribed dose, a process that can be difficult because of it being an unscored tablet with a diameter of ∼7 mm. Previous authors have raised concerns about medication regimens that require pill splitting, as >20% variation in dosing can occur at least 10% of the time. One study found that participants asked to split their pills said that they were willing to pay a premium for lower dose tablets instead (McDevitt et al. 1998), highlighting the difficulty in pill splitting experienced by patients. Use of extended-release guanfacine in young children presents its own challenges surrounding the swallowability of this formulation and the fact that dividing an extended-release tablet destroys the physicochemical integrity of the formulation, making its bioavailability unpredictable. Therefore, achieving an age-appropriate dose for a preschool patient using the extended-release formulation can be a challenge. Although the 1 mg extended-release version of the formulation has approximately the same physical dimensions as the immediate-release version, this may represent a difficult barrier for preschool patients to overcome. A study by Meltzer et al. in 2006 evaluated pill-swallowing ability in a group of 6–11-year-olds. Only ∼20% of the 6-year-olds in that study were able to reliably swallow a tablet without help. This rate increased with intervention and training; however, it is unlikely that similar interventions would be effective in younger children, given the potential for developmental differences in the biomechanics of swallowing coupled with expected behavioral differences that may make them less “teachable.” Commercial availability of a stable, palatable liquid formulation of guanfacine would obviate most all of the challenges with using tablet formulations, including the ability to more precisely dose titrate (e.g., enable true mg/kg dosing).
Clinical Pharmacology
In addition to the clinical factors discussed, there are specific issues related to the clinical pharmacology of guanfacine that deserve consideration, especially as they relate to potential differences in the dose–exposure–response relationship in the preschool population. Following a review of the mechanistic properties of guanfacine and its pharmacokinetic profile, we discuss specific important factors, such as ontogeny of drug disposition, developmental pharmacodynamics, and pharmacogenetics that may require further study in order to identify efficacious and safe dosing guidelines for young patients.
Mechanism of action
Guanfacine, (N-[diaminomethylidene]-2-[2,6-dichlorophenyl]acetamide), is an α-2A adrenergic agonist. Originally approved for the treatment of hypertension, guanfacine exerts these effects by activating α-2A norepinephrine autoreceptors in the CNS, which, in turn, reduces sympathetic outflow, and also reduces peripheral sympathetic tone. The heavy concentration of these receptors in the prefrontal cortex (PFC) form the pharmacologic basis for guanfacine use in ADHD, as symptoms of this disorder are known to be related to impairments in the PFC (Arnsten et al. 2007). Specifically, guanfacine is known to be an agonist of postsynaptic α-2A receptors in the PFC (Arnsten and Goldman-Rakic 1985). Animal models have shown improvement of cognitive performance tasks after administration of α-2 agonists and imaging studies have shown increased cerebral blood flow to portions of the PFC in animals performing a spatial working memory task after α-2 agonist exposure (Arnsten et al. 1988; Avery et al. 2000). Guanfacine has specific affinity for the α-2A subtype, which studies have demonstrated to be the most important in conferring the therapeutic effects of α-2 agonists (Uhlen and Wikberg 1991; Franowicz et al. 2002). The α-2A receptors are located on dendritic spines near potassium channels that, when opened by cyclic adenosine monophosphate (cAMP) signaling or other mechanisms, can weaken network connections. An α-2A agonist such as guanfacine works to inhibit cAMP signaling, thereby closing the potassium channels and enhancing PFC connectivity (Wang et al. 2007) (Fig. 1).
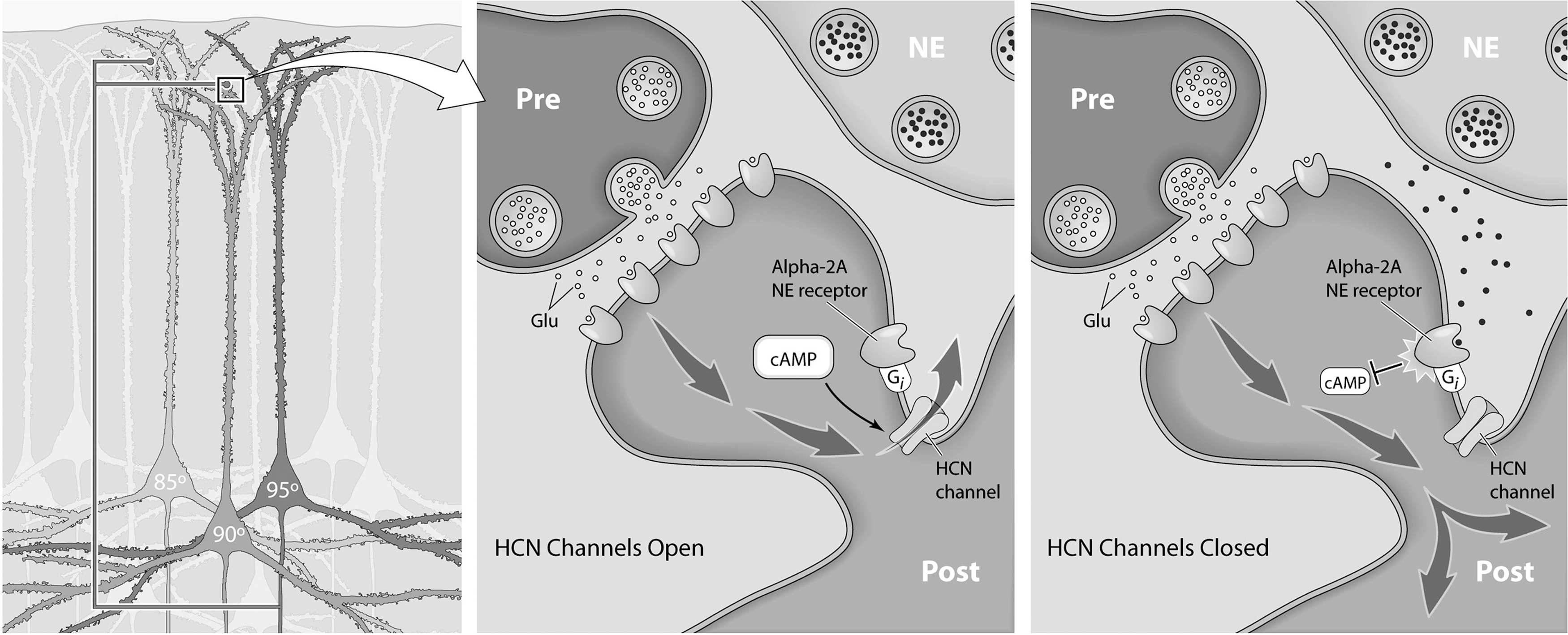
Guanfacine mechanism of action. The α-2A receptors are located on dendritic spines near ion channels that, when opened by cyclic adenosine monophosphate (cAMP) signaling or other mechanisms, can weaken network connections. Guanfacine inhibits cAMP signaling, thereby closing the potassium channels and enhancing prefrontal cortex (PFC) connectivity. Reprinted from Wang et al. 2007, with permission from Elsevier. HCN, hyperpolarization-activated cyclic nucleotide-gated; NE, norepinephrine.
Pharmacokinetics
The disposition of guanfacine has been reasonably well characterized in adults, and is, to a considerable degree, dependent upon the formulation of the drug studied. Guanfacine is ∼70% bound to plasma proteins, independent of drug concentration, and the immediate-release formulation has an absolute bioavailability of ∼80% (Guanfacine HCl Package Insert 2011). It is extensively distributed throughout the body, with an apparent volume of distribution of 6.3 L/kg, which suggests extensive tissue distribution. The drug is extensively metabolized, primarily by the cytochrome P450 isoform CYP3A4. After an oral dose, ∼30–50% of the parent drug is excreted unchanged in the urine (Kiechel 1980). The apparent elimination half-life of guanfacine from immediate-release formulations is ∼16 hours in adults, and is slightly longer in patients given the extended release formulations (Guanfacine Extended Release Package Insert 2011).
Important Pharmacological Factors
Potential role of ontogeny in guanfacine disposition
It is generally known that normal growth and development are associated with changes in the disposition and action of many drugs (Kearns et al. 2003). One of the processes most profoundly impacted by ontogeny is drug metabolism. As denoted, guanfacine is thought to be a substrate of the CYP3A isoform, CYP3A4. CYP3A4 is the most abundantly expressed cytochrome P450 enzyme in the human liver and small intestine (Watkins et al. 1987; Kolars et al. 1994), and is a member of the CYP3A subfamily that also includes CYP3A5 and 3A7, the genes for which are all known to be located on chromosome 7, with CYP3A4 located specifically at position q22.1 (Inoue et al. 1992). CYP3A4 activity in fetal liver is extremely low, but increases dramatically after birth, reaching near normal adult levels of activity by ∼6 months of age (de Wildt et al. 1999). In addition to its ability to catalyze the biotransformation of guanfacine, CYP3A4 is primarily responsible for the biotransformation of at least 30% of prescribed drugs in the United States (Zanger and Schwab 2013). As reviewed by de Wildt et al. (1999), there are at least two developmental “break points” for CYP3A activity during the first 3 years of life. Over the 1st month, activity levels (relative to adult values) remain low. This is followed by rapid accretion of activity during the first 6 months, and as shown for some CYP3A4 substrates (e.g., cyclosporine), activity levels in children between 24 and 36 months of life can exceed those in adults. Although variability exists among the literature describing CYP3A ontogeny, it is clear that development of activity in the first 2–3 years of life is dynamic (Ince et al. 2013). Given the impact of ontogeny on CYP3A4 activity, it is likely that important differences in guanfacine metabolism (with resultant alterations in its plasma clearance) occur among very young children relative to older age groups, which may be of sufficient magnitude to alter the exposure-response relationship and, thereby, affect therapeutic response.
Developmental pharmacodynamics
As with the potential for development to alter guanfacine disposition, the impact of ontogeny on the affinity of guanfacine for α-2A receptors may form the basis for developmental differences in the drug's pharmacodynamics. Previous studies have identified differences in α-2A receptor expression in the rat neocortical development as a function of age (Winzer-Serhan and Leslie 1999). Alpha-2A receptor mRNA is expressed at high levels in the basal ganglia, amygdala, thalamus, spinal cord, and brainstem during early development, but decreases in these areas with nervous system maturation (Winzer-Serhan et al. 1997). Because the therapeutic benefit of guanfacine is known to derive from action on α-2A receptors in the PFC, such differential expression in the developing human brain could conceivably have implications on guanfacine efficacy in the preschool population. To date, however, the impact of development on the pharmacodynamics and pharmacologic effect of guanfacine in young children is not known.
Pharmacogenetics
There has been extensive evaluation of the potential role of pharmacogenetics in guiding psychopharmacotherapeutic treatment decisions for many drugs including guanfacine (Stein and McGough 2008; Froehlich et al. 2010). McCracken et al. examined whether gene variants encoding the P-glycoprotein drug transporter were associated with variability in the efficacy of guanfacine in children with PDD and hyperactivity. They noted differences in drug efficacy among subjects who were homozygous for the variant allele of the MDR1 gene (C3435 TT) compared to alternative genotypes (C3435 CT and C3435 CC). Subjects with the C/T and C/C genotypes showed threefold greater improvement in parent-rated hyperactivity scores than those with the T/T genotype. This evidence suggests that genetic differences among drug transporters may affect guanfacine therapeutic response among children. Future studies are needed to validate these findings in both a pharmacokinetic and pharmacodynamics context.
Genetic variation within CYP3A4 has been observed to result in alterations in response to simvastatin, which is also primarily metabolized by this enzyme (Elens et al. 2011). It is plausible that CYP3A allelic variants (e.g., CYP3A4*…, CYP3A5*…) could play a role in the biotransformation of guanfacine as well. Variation of other genes associated with guanfacine disposition and response also merit consideration such as ADRA2A. For example, variation within ADRA2A, which encodes for the α-2A adrenergic receptor, has been associated with differential methylphenidate response in children (Polanczyk et al. 2007; Kim et al. 2013). In contrast, there is at present no published literature that describes investigations of ADRA2A variation and guanfacine response in pediatric patients with ADHD.
Conclusions
Immediate release guanfacine, an α-2A agonist, remains a commonly used therapeutic option in the management of impulsive, hyperactive, and disruptive symptoms in preschool-age patients. Although the use of guanfacine in this particular patient population is outside of the current FDA-approved indication, the AAP policy statement on off-label drug use states that: “off-label does not imply an improper, illegal, contraindicated, or investigational use” (Frattarelli et al. 2014). However, there remains a paucity of data regarding both the pharmacokinetics and pharmacodynamics of guanfacine in young children, which may preclude its optimal use. Although the current data support a role for guanfacine treatment in younger children with ADHD, the pharmacologic “information gap” that currently exists, and the lack of a child-friendly liquid formulation can, in some instances, limit the utility of a potentially useful drug simply as a consequence of a relative inability to provide accurate, age-appropriate doses. Future studies are essential to define the pharmacokinetic and pharmacodynamic profile of the drug in the younger age groups, thereby ensuring that safe and effective medications are given to these groups of children. Also, research is needed to inform the development of guanfacine formulations suitable for the treatment of young children with ADHD.
Clinical Significance
Guanfacine is often used in the management of very young children with ADHD; however, there are significant knowledge gaps regarding its use in this population. This review highlights some of these gaps, and discusses steps that can be taken to ensure that effective, accurate, and age-appropriate dosing can be achieved.
Footnotes
Disclosures
No competing financial interests exist.