
Abstract
Objectives:
The purpose of this study was to assess differences in the outcomes of youth with schizophrenia-spectrum disorders (SCZ-S) and psychotic disorder not otherwise specified (PsyNOS) during early antipsychotic treatment.
Methods:
The study was a prospective, naturalistic, inception cohort study of youth ≤19 years old with SCZ-S (schizophrenia, schizoaffective disorder, schizophreniform disorder) or PsyNOS (PsyNOS, brief psychotic disorder) and ≤24 months of lifetime antipsychotic treatment receiving clinician's choice antipsychotic treatment. Baseline demographic, illness and treatment variables, and effectiveness outcomes were compared at 12 weeks last-observation-carried-forward across SCZ-S and PsyNOS patients, adjusting for significantly different baseline variables.
Results:
Altogether, 130 youth with SCZ-S (n=42) or PsyNOS (n=88), mostly antipsychotic naïve (76.9%), were prescribed risperidone (47.7%), olanzapine (19.2%), aripiprazole (14.6%), quetiapine (11.5%), or ziprasidone (6.9%). Compared with those with PsyNOS, SCZ-S youth were older (16.4±2.1 vs. 14.8±3.2, p=0.0040), and less likely to be Caucasian (19.1% vs. 42.5%, p=0.009). At baseline, SCZ-S patients had significantly higher Clinical Global Impressions-Severity (CGI-S) scores (6.0±0.9 vs. 5.5±0.8, p=0.0018) and lower Children's Global Assessment Scale (CGAS) scores (29.6±9.2 vs. 36.1±8.9, p=0.0002) and were more likely to be in the severely ill CGAS group (i.e., CGAS≤40). SCZ-S and PsyNOS patients did not differ regarding all-cause discontinuation (40.5 vs. 40.3%. p=0.49), discontinuation because of adverse effects (12.2% vs. 12.4%, p=0.97), or nonadherence (29.3% vs. 30.9%, p=0.88), but somewhat more SCZ-S patients discontinued treatment for inefficacy (19.5% vs. 7.4%, p=0.063). CGI-S and CGAS scores improved significantly in both diagnostic groups (p=0.0001, each). Adjusting for baseline differences, PsyNOS patients experienced significantly better CGI-I improvement (CGI-I) scores (p=0.012) and more frequently reached higher categorical CGAS group status (p=0.021) than SCZ-S patients.
Conclusions:
Both youth with SCZ-S and those with PsyNOS experienced significant improvements with clinician's choice antipsychotic treatment. However, treatment discontinuation was common within 12 weeks, with greater inefficacy-related discontinuation in the SCZ-S group, whereas CGI-I and CGAS score-based improvements were greater in the PsyNOS group.
Introduction
S
Until a few decades ago, research on psychotic disorders in children and adolescents was scarce. Fortunately, knowledge about and research on early-onset schizophrenia have increased in the past decades. Data have emerged supporting the validity of the diagnosis in this age group (Maziade et al. 1996; Asarnow 2005; Helgeland and Torgersen 2005), and significant antipsychotic efficacy has been demonstrated in short-term placebo-controlled trials (Correll et al. 2011b; Kendall et al. 2013; McClellan and Stock 2013; Schimmelmann et al. 2013a). So far, randomized controlled trials (RCTs), guidelines, and long-term follow-up studies have primarily focused on early onset schizophrenia, and although this is the most severe psychotic disorder, other psychotic disorders are more common, and most youth presenting with psychoses are diagnosed with other disorders than schizophrenia. The child and adolescent first-episode psychosis study (CAFEBS) found psychosis not otherwise specified (PsyNOS) to be the most common psychosis-spectrum diagnosis, affecting 35.5% of their sample at baseline (Castro-Fornieles et al. 2007). Relatively limited research is available on the epidemiology, clinical characteristics, and outcome of PsyNOS. Although many clinical studies include patients with PsyNOS (Wozniak et al. 2008; Rapado-Castro et al. 2010; Swadi et al. 2010; Hassan and Taha 2011), studies rarely specify the outcome for different types of psychotic disorders, but either focus solely on schizophrenia or treat all psychotic disorders as one group. Moreover, trials just focusing on patients with PsyNOS are lacking. Therefore, treatment response and outcomes for patients with PsyNOS are much less known than are outcomes for patients with schizophrenia.
Because patients with PsyNOS already present with suprathreshold psychosis, they can be considered a particular high-risk population for the development of schizophrenia (Correll et al. 2008). Notably, PsyNOS is one of the least stabile diagnoses in the psychotic spectrum, but study results vary considerably. Studies in adults have shown that 25–73% will transition to other severe mental disorders, whereas others will recover or continue to fulfill PsyNOS criteria (Sivakumar and Chandrasekaran 1993; Chaturvedi and Sahu 1986; Schwartz et al. 2000; Sajith et al. 2002; Schothorst et al. 2006; Rahm and Cullberg 2007; Subramaniam et al. 2007; Salvatore et al. 2009; Kingston et al. 2013).
Studies in the child and adolescent population have been inconclusive regarding diagnostic stability. Some found diagnostic stability as low as 7.7% (Correll et al. 2005), 11.8% (Castro-Fornieles et al. 2011), or 16.7% (Fraguas et al. 2008), and transition rates to other severe mental disorders as high as 88% (Castro-Fornieles et al. 2011), whereas others found no transition even after several years of follow-up (McClellan and McCurry 1999a). Regardless of the rates and direction of diagnostic transition, PsyNOS is a serious condition in and of itself. McClellan and McCurry found 38% of youth with PsyNOS to be chronically impaired after 2 years; 75% were on psychotropic medications and only 13% were in regular school or work (McClellan and McCurry 1999). Another study of 26 adolescents with PsyNOS or brief psychosis found that 20% had full remission at 6 months follow-up, but 38% had transitioned to other, more severe disorders (schizophrenia, schizoaffective or bipolar disorder with psychosis) (Correll et al. 2008).
Although it is well established that patients with schizophrenia have a worse prognosis than those with other psychotic disorders with an early onset as recently summarized (Clemmensen et al. 2012), there remains a gap in the literature concerning how children and adolescents with PsyNOS differ from those with schizophrenia-spectrum disorders in terms of symptom severity and functioning at baseline, as well as treatment acceptance and responsiveness. Moreover, the generalizability of the efficacy observed in selected samples consenting to participate in RCTs to populations treated in general practice settings is less clear. Furthermore, because more chronically ill patients are overrepresented in RCTs, very little is known about outcomes in youth with short illness duration or even naïve to antipsychotic treatment (Sikich et al. 2008; Arango et al. 2009).
Therefore, the present study aimed at investigating baseline differences and short-term outcomes of antipsychotic treatment in children and adolescents with schizophrenia-spectrum disorders (SCZ-S) and psychotic disorder not otherwise specified (PsyNOS) in a naturalistic setting. Because early improvement in patients with schizophrenia-spectrum disorders is associated with later remission and outcome (Emsley et al. 2007), studies on the short-term progress are important. Based on the literature, we hypothesized that children and adolescents with early- onset schizophrenia would be more severely impaired and less responsive to antipsychotic treatment than patients with PsyNOS.
Methods
Study setting and design
Data for this study were collected as part of the
Inclusion criteria were: 1) Being 4–19 years of age; 2) having a psychiatric illness prompting antipsychotic initiation; and 3) consent and baseline anthropometric/biochemical assessments obtained within ≤7 days of the present antipsychotic initiation. Patients were considered antipsychotic naïve if they had ≤1 week of previous antipsychotic exposure. Patients who had been exposed to antipsychotics, but who had a treatment gap of >4weeks, were dubbed “patients with antipsychotic history.” Patients were considered antipsychotic switchers if they were moved to another antipsychotic either overlapping with the prior antipsychotic or within 5 half-lives of stopping the prior antipsychotic.
Exclusion criteria were: 1) Treatment with more than one antipsychotic; 2) active/past eating disorder; 3) biochemical evidence of thyroid dysfunction; 4) acute medical/neurologic disorders; 4) pregnancy/breastfeeding; 5) being wards of the state (as research consent by a public agency representative within 1 week was unlikely); and 6) leaving the catchment area within <4 weeks.
Inclusion criteria for the current analyses were the subsample of the full SATIETY study with SCZ-S disorders (i.e., schizophrenia, schizoaffective disorder, schizophreniform disorder) or PsyNOS (i.e., psychotic disorder not otherwise specified, brief psychotic disorder) who had <24 months of lifetime antipsychotic exposure and who were not started on clozapine. These two groups were compared at baseline and 12 week end-point. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) diagnoses were made based on a review of all clinical chart information, as well as an interview of the youth and caregiver (American Psychiatric Association 1994). To qualify for PsyNOS, several possibilities existed: 1) Only one A criterion symptom (other than bizarre delusions, running commentary, or at least two voices communicating with each other); 2) fulfilling A criteria but without presence of distress or functional impairment; or 3) duration of symptoms fulfilling criteria between 1 week and <4 weeks. Accordingly, brief psychotic disorder was subsumed under PsyNOS if the duration was at least 1 week, whereas psychotic disorder secondary to a medical disorder or substance use did not count as PsyNOS.
Treatment
Antipsychotic treatment was initiated as part of clinician's choice. Only after the antipsychotic choice was made by the treating clinician was written informed consent/assent for participation in the study obtained. Dosing, prescription of co-medications and other treatment changes were all performed by the patient's treating clinician based on clinical need.
Assessments
All assessments were conducted by medical doctors trained and supervised by C.U.C., with regular quality control to avoid rater drift.
Baseline
The following baseline assessments, conducted as part of the SATIETY study, were analyzed in the current study: Primary and comorbid psychiatric diagnoses (based on clinical chart information as well as patient and caregiver interview by study personnel, using DSM-IV criteria), ethnicity and past treatment history assessed by chart review, discussion with treatment providers, and clinical interview of the patient/caregiver. Socioeconomic status (SES) was categorized according to Hollingshead (Hollingshead and Redlich 1958), ranging from 1 (highest) to 5 (lowest). Postpubertal status (Tanner stages 3–5) was determined through inspection and interview of the patient and/or caregiver. Subject reports of adverse events were recorded by the investigators with a modified version of the Treatment Emergent Symptoms Scale (TESS)(Guy 1976). Fasting blood samples were used to assess glucose, insulin, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), total cholesterol, low- and high-density lipoprotein cholesterol (LDL-C and HDL-C), triglycerides, and prolactin. Furthermore, the Simpson–Angus Ratings Scale (SARS) (Simpson and Angus 1970), Barnes Akathisia Rating Scale (BARS) (Barnes 1989), and Abnormal Involuntary Movement Scale (AIMS) (Guy 1976) were used to rate extrapyramidal side effects, akathisia and dyskinesia, respectively.
The Clinical Global Impressions (CGI) scale (Guy 1976) was used to assess severity (CGI-S) and improvement (CGI-I). The CGI-S measures symptomatology on a scale from 1 (normal, not at all ill) to 7 (extremely ill). The CGI-I measures improvement on a similar seven point scale, ranging from 1 (very much improved) to 7 (very much worse). A CGI-I score of 4 indicates “no change.” The child version of the Global Assessment of Functioning Scale, the Children's Global Assessment Scale (CGAS) (Shaffer et al. 1983) was used to assess symptomatology as well as psychosocial functioning. The CGAS is a numeric scale ranging from 0 to 100, with higher scores indicating better functioning. CGAS ratings are independent of specific psychiatric diagnoses.
Follow-up
CGAS, CGI-I, CGI-S, detailed medication information (adherence, as reported by the patients and caregivers, discontinuation, reasons for discontinuation), and adverse affects were assessed at monthly follow-up assessments. Additionally, antipsychotic blood levels were measured as an objective measure of nonadherence. Patients were considered partially nonadherent when deemed to be taking <70% of the prescribed medication based on interview, and were considered nonadherent if they stopped the antipsychotic against medical advice for >5 half lives of the antipsychotic or when antipsychotic blood levels were not measurable.
Outcomes
Co-primary outcomes for the current study were CGI-I based global improvement and CGAS based categorical outcomes defining severe illness/functional levels as CGAS scores ≤50, moderate as 51–70, and mild as >70 as suggested in a recent review on the outcome of early-onset schizophrenia (Clemmensen et al. 2012).
Secondary outcomes included change in CGI-S score, CGI-S end-point score, CGI-I based response (defined as much or very much improved), change in CGAS, and CGAS end-point. Frequency of all-cause discontinuation and specific-cause discontinuation, as well as the frequency and severity of adverse events, were also analyzed.
Statistical analyses
Baseline data, length of inpatient stay, medication adherence, and discontinuation- related outcomes were compared across the two diagnostic groups in the full intent-to-treat (ITT) sample (n=130). In addition, the two diagnostic groups were also compared using the modified ITT (mITT) sample composed of patients with more than one postbaseline assessment (n=106, 81.5% of the entire sample), using last-observation-carried-forward (LOCF) analyses. These analyses included baseline data, treatment variables, and CGI and CGAS related outcomes, as well as side effect related outcomes.
For the majority of patients who did not return for any follow-up visits, medication information was available through hospital records. Seven patients were lost to follow-up without medication information or because they never started the antipsychotic because of family choice.
Group comparisons at baseline were performed using χ2 tests, t tests, Fisher's exact test, or Wilcoxon rank sum tests as per data type and distribution. Because this was a nonrandomized study, all statistical tests of outcome comparisons were adjusted for variables, which differed significantly (p<0.05) across the two diagnostic groups at baseline in the mITT sample. All analyses were two sided with α set at 0.05 and conducted using Stata12. Prospective outcomes based on continuous variables were analyzed with linear regression, binary outcomes with logistic regression and categorical CGAS outcome were analyzed using ordered logistic regression analysis.
Results
Patient flow
During the study period, 853 youth were started on an antipsychotic. Of these, 675 (79.1%) were excluded because they had primary diagnoses other than SCZ-S or PsyNOS. Of the remaining 211 subjects, 74 (35.1%) were excluded because they either refused study participation (n=33, 15.6%), guardians could not be reached within 7 days of antipsychotic initiation (n=31, 15.7%), or they fulfilled the remaining exclusion criteria (n=10, 4.7%). Furthermore, 8 patients were excluded due to >24 months of antipsychotic treatment or initiation of clozapine treatment (Fig 1).
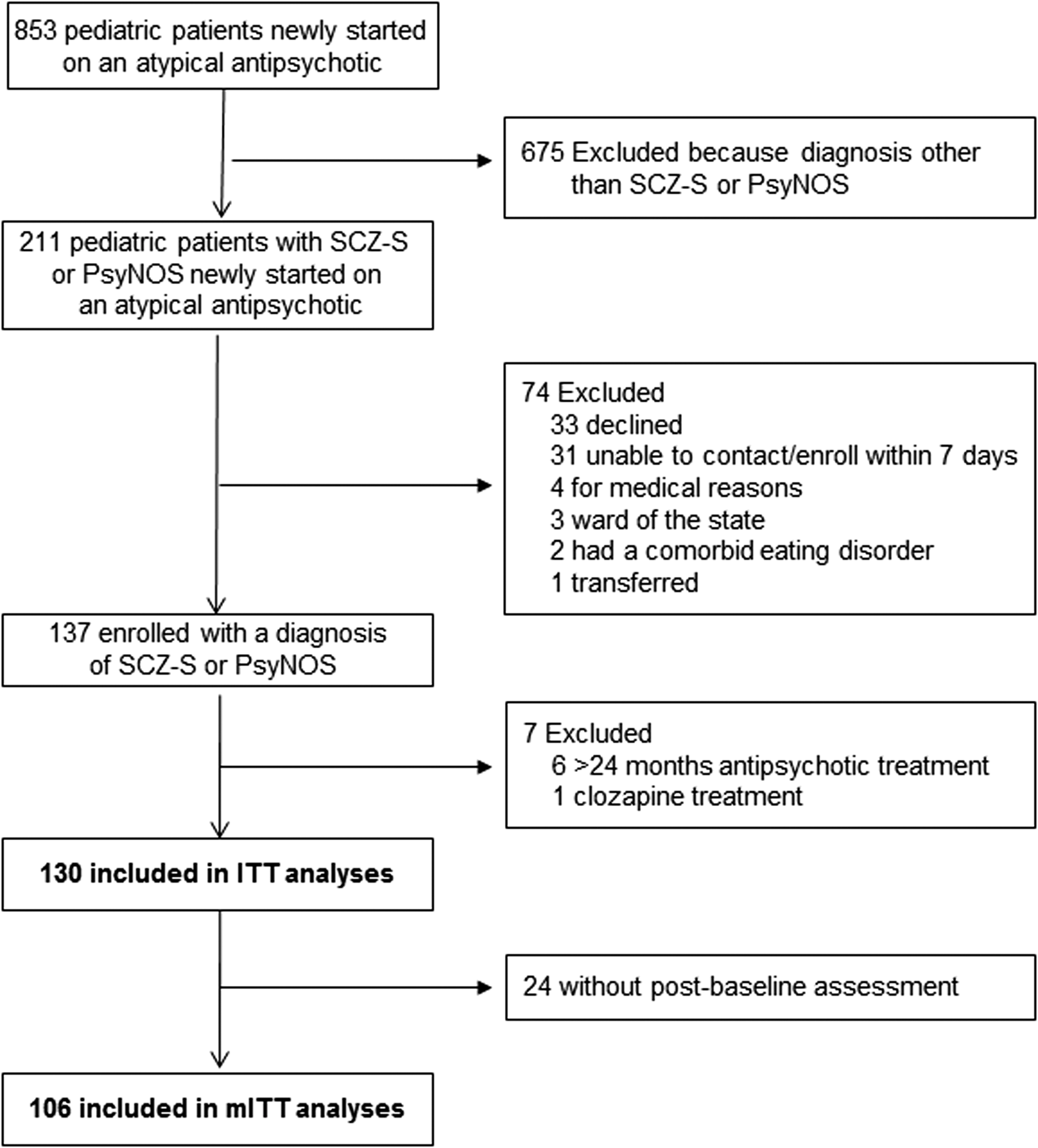
Patient flow.
Baseline characteristics
The full ITT study sample consisted of 130 children and adolescents (mean age, 15.3±3.0; range, 5–19 years; 85.4% postpubertal) diagnosed with SCZ-S (n=42, 32.3%) or PsyNOS (n=88, 67.7%) (Table 1). In the SCZ-S group, most patients had a schizophrenia diagnosis (n=36, 85.7%), and a few had either schizoaffective disorder (n=3, 7.1%) or schizophreniform disorder (n=3, 7.1%). In the PsyNOS group, all patients had a diagnosis of psychosis not otherwise specified, except for one patient with brief psychotic disorder. The majority of the sample was male (59.2%), and most were non-Caucasian (65.1%). The mean socioeconomic status was 2.7. The majority of the sample had a psychiatric family history (61%), the most common diagnosis being depression (18.7% first degree, 22.7% second degree), and 74.6% were inpatients at baseline and, overall, patients scored between markedly and severely ill (mean CGI-S, 5.6±0.9; CGAS, 34.0±9.4).
Significant differences at p≤0.05 have been bolded.
Including only patients with at least one follow-up assessment (Psychosis NOS=68, Schizophrenia-spectrum=38); mITT p values are shown for baseline variables in order to present variables that were significantly different across groups, which were adjusted for in the outcome analyses.
Including oppositional defiant disorder, conduct disorder, intermittent explosive disorder, and impulse control disorder not otherwise specified.
Including major depressive disorder, depression not otherwise specified, and adjustment disorder.
Compared with those with PsyNOS, SCZ-S youth were older (16.4±2.1 vs. 14.8±3.2, p=0.0090) and less likely to be Caucasian (19.1% vs. 42.5%, p=0.009) (Table 1). At baseline, SCZ-S patients had significantly higher CGI-S scores (6.0±0.9 vs. 5.5±0.8, p=0.0018) and lower CGAS scores (29.6±9.2 vs 36.1±8.9, p=0.0002). According to categorical CGAS criteria, almost all patients in both groups (97.6% vs. 96.6%) were severely ill. Although not significant in the ITT-sample (p=0.054), in the mITT sample, the SCZ-S group had a lower mean number of psychiatric comorbidities (0.4±0.5 vs. 0.7±0.9, p=0.031) (Table 1).
Of the 106 patients with at least one postbaseline assessment (mITT sample), 38 (35.8%) had SCZ-S and 68 (64.2%) had PsyNOS. Comparing the 24 patients who dropped out of the study after baseline with the 106 who had at least one baseline visit on all baseline characteristics (see Table 1), no significant group differences were found, indicating that the patients with follow-up data were representative of the entire sample.
Psychotropic treatment characteristics
The majority of the sample was antipsychotic naive (SCZ-S 73.8% vs. PsyNOS 78.4%) as well as being naïve to any psychotropic medication exposure (SCZ-S 66.7%; PsyNOS 61.4%; Table 2). The mean duration since first antipsychotic exposure was 0.3±0.7 years, and the mean duration of lifetime antipsychotic exposure was 1.7±4.5 months, without group differences. Risperidone was the most frequently initiated antipsychotic (47.7%), followed by olanzapine (19.2%), aripiprazole (14.6%), and quetiapine (11.5%), whereas ziprasidone was the least used (6.9%). Except for more patients with SCZ-S than with PsyNOS being started on olanzapine (38.1% vs. 10.2%, p<0.0001), treatments did not significantly differ across the two groups. Results were similar in the mITT group (Table 3).
Significant differences at p≤0.05 have been bolded.
AP treatment naïve:≤7 days of lifetime AP exposure.
AP treatment history, restarted: AP restarted after at least a 4 week gap.
Significant differences at p≤0.05 have been bolded.
Adjustment variables for p values in the mITT analyses of antipsychotic choice: Age, Caucasian, inpatient status, number of comorbidities, comorbid depression, Children's Global Assessment Scale (CGAS) baseline, Clinical Global Impressions – Severity (CGI-S) baseline.
Baseline ratings of adverse effects measured on the TESS showed only a difference between the two groups on psychomotor activation/retardation, with SCZ-S patients having more psychomotor retardation (41.5% vs. 15.4%, p=0.002 in ITT) and PsyNOS patients reporting more psychomotor activation (11.5% vs. 0%, p=0.03 in ITT). Results were similar in the mITT group (Table 4). Furthermore, the two groups did not differ on body weight, body mass index (BMI) z score, blood levels of glucose and lipid metabolism, or prolactin and adverse effect scales (Table 5), except for a higher HOMA-IR value in the SCZ-S group in the ITT sample (71.0±34.5 vs. 57.5±36.6, p=0.047).
Significant differences at p≤0.05 have been bolded.
Including only patients with at least one follow-up assessment (psychosis NOS=68, schizophrenia-spectrum=38).
The analyses on menstrual disturbance are restricted to postpubertal females.
The analyses on decreased libido and impaired sexual performance are restricted to postpubertal patients.
LOCF, last-observation-carried-forward; NOS, not otherwise specified; mITT, modified intent-to-treat.
Significant differences at p≤0.05 have been bolded.
All continuous outcomes are based on change scores from baseline to 3 months, LOCF. Data are presented as adjusted least square means (LSM)±standard error for each column.
Adjustments were made according to differences at baseline in the mITT sample between PsyNOS and SCZ-S of p value<0.05. Outcome analyses were adjusted for age, Caucasian y/n, inpatient status, olanzapine use, number of comorbidities, comorbid depression, Children's Global Assessment Scale (CGAS) baseline, Clinical Global Impressions – Severity (CGI-S) baseline and SCZ-S/PsyNOS. Continuous outcomes were also adjusted for baseline value of the respective outcome.
LOCF, last-observation-carried-forward; NOS, not otherwise specified; mITT, modified intent-to-treat; BMI, body mass index; HOMA-IR, Homeostasis Model Assessment of Insulin Resistance; LDL, low-density lipoprotein; HDL, high-density lipoprotein; AIMS, Abnormal Involuntary Movement Scale.
Primary outcomes: Mean CGI-I scores and categorical CGAS based outcomes
After 12 weeks of antipsychotic treatment, SCZ-S patients improved significantly less than PsyNOS patients on the CGI-I (2.9±0.4 vs. 2.1±0.3, p=0.0012; Table 6). Moreover, although both groups had significantly improved CGAS (p<0.0001), fewer SCZ-S patients reached a mildly ill or better CGAS-based outcome (0% vs. 7.4%), and more had a severely ill or worse CGAS-based outcome (65.8% vs. 42.7%), p=0.40; Fig. 2).

Categorical Children's Global Assessment Scale (CGAS) at baseline and follow-up.
Significant differences at p≤0.05 have been bolded.
Data are presented as number of patients (percent) or adjusted least square means±standard error for each column.
Adjustments were made according to differences at baseline in the mITT sample between PsyNOS and SCZ-S of p value<0.05. Outcome analyses were adjusted for age, Caucasian y/n, inpatient status, olanzapine use, number of comorbidities, comorbid depression, CGAS baseline, CGI-S baseline, and SCZ-S/PsyNOS.
Changes in CGI-S and CGAS scores from baseline to 12 weeks within groups were significant at p<0.0001.
Analyses conducted with baseline values as covariates.
Secondary outcomes: CGI-S and CGAS end-point and change scores, and CGI-I based responder status
Although both groups improved significantly on the CGI-S (p<0.0001), SCZ-S patients improved significantly less than PsyNOS patients (-1.0±0.3 vs. −1.6±0.3, p=0.036) and the end-point CGI-S score was significantly higher (4.6±0.3 vs. 4.0±0.3, p=0.036) (Table 6). Similarly, CGAS scores improved significantly less in SCZ-S patients than in PsyNOS patients (12.0±3.3 vs. 18.0±2.8, p=0.031), and the end-point CGAS score was significantly lower (46.3±3.3 vs. 52.3±2.8, p=0.031). Finally, at a trend level, fewer patients with SCZ-S were treatment responders, defined by a score of much or very much improved on the CGI-I scale (44.7% vs. 62.7%, p=0.067) (Table 6).
Secondary Outcomes: Treatment discontinuation, nonadherence, and length of hospital admission
Information on medication continuation was available for 95.4% of the sample. During the 12 weeks of the study, 40.3% discontinued medication, either as decided by the physician because of lack of efficacy or side effects, or because of the family's/patient's choice. Although SCZ-S and PsyNOS subjects did not differ regarding all-cause discontinuation (40.5% vs. 40.3%, p=0.49), more patients with SCZ-S discontinued their antipsychotic because of inefficacy (19.5% vs. 7.4%, p=0.063) (Table 7). There was no difference between SCZ-S and PsyNOS patients regarding discontinuation because of intolerability (12.2% vs. 12.4%, p=0.97), nonadherence (29.3% vs. 30.9%, p=0.88), or length of hospital stay (21.8±5.7 days vs. 24.3±4.8 days, p=0.65).
Data are presented as number of patients (percent) or adjusted least square means±standard error for each column.
Adjustments were made according to differences at baseline in the ITT sample between PsyNOS and SCZ-S of p value<0.05. Outcome analyses of the ITT-sample were adjusted for age, pubertal status, Caucasian y/n, inpatient-status, olanzapine use, Children's Global Assessment Scale (CGAS) baseline, Clinical Global Impressions – Severity (CGI-S) baseline, and SCZ-S/PsyNOS.
This analysis was restricted to patients who were inpatients at baseline. The adjustments were PsyNOS/SCZ-S, age, Caucasian y/n, comorbid anxiety disorder, olanzapine use, CGAS, and CGIS-baseline.
Interrupting medication taking for 1–6 days.
Interrupting medication taking ≥7 days or antipsychotic blood level of zero.
Adverse effects at 3 month follow-up
Measured with the TESS (Table 4), SARS, BARS, and AIMS (Table 5), there were no differences between the two diagnostic groups in reported or rated adverse effects at 3 months LOCF. Similarly, there were also no differences between the two diagnostic groups in weight, BMI z score, and laboratory test results, with the exception of significantly higher LDL (40.6±8.6 vs. 27.6±8.0, p=0.019) and nearly significantly higher HOMA-IR (1.3±0.6 vs. 0.4±0.5, p=0.054) in the SCZ-S group (Table 5).
Discussion
This naturalistic study comparing 12-week outcomes of antipsychotic treatment within the first 2 years of illness across 130 youth with a DSM-IV diagnosis of SCZ-S or PsyNOS supported our initial hypotheses of greater treatment responsiveness in the PsyNOS group. The main findings of this study were: 1) SCZ-S patients had significantly greater illness severity and lower functioning than PsyNOS patients at both baseline and follow-up; and 2) although CGI-S and CGAS scores improved significantly in both diagnostic groups, SCZ-S patients experienced significantly less improvement in illness severity and functioning when adjusting for baseline differences.
Schizophrenia is a more severe illness than PsyNOS, which is reflected in the current study by the comparison of both baseline and follow-up data. This finding was expected and is consistent with other studies in youth (McClellan et al. 1999; Helgeland and Torgersen 2005; Hassan and Taha 2011; Clemmensen et al. 2012). For example, our results in the SCZ-S group are very comparable to the 8 week results from the Treatment of Early Onset Schizophrenia Spectrum Disorders (TEOSS) study, in which 44.0% were much or very much improved on the CGI-I (Sikich et al. 2008), compared with 44.7% in our sample. However, studies in youth with psychosis NOS are scarce, and direct comparisons of early treatment outcomes with a concurrently treated group of SCZ-S patients are rare. Although patients with PsyNOS are sometimes included in studies of first episode psychosis, the results are rarely reported separately by diagnosis, confounding results in patients with schizophrenia. Therefore, future studies that include both SCZ-S and PsyNOS patients should present results for both subgroups. In the few child and adolescent studies with separate results for each diagnostic group or with a specific focus on PsyNOS, the sample size of the PsyNOS group was generally small (McClellan et al. 1999; Nicolson et al. 2001; Correll et al. 2005, 2008; Fraguas et al. 2008; Hassan and Taha 2011) with numbers of PsyNOS patients ranging between 6 and 26. To our knowledge, the present study is the largest to date comparing child and adolescent PsyNOS patients with early-onset schizophrenia youth using the same assessment measures at baseline and follow-up with follow-up data in as many as 68 PsyNOS patients.
Studies in adults also reported that PsyNOS patients had better outcomes than patients with schizophrenia (Kendler and Walsh 1995; Harrison et al. 2001; Jobe and Harrow 2005; Crespo-Facorro et al. 2007; Simonsen et al. 2010; Crespo-Facorro et al. 2013; Diaz et al. 2013; Pelayo-Teran et al. 2014). However, even in adults, such comparative studies are sparse, and generally have the same limitations as studies in the child and adolescent population; either small sample sizes or lack of differentiation among the different diagnostic first-episode psychosis subgroups. The Genetic Risk and Outcome of Psychosis (GROUP) study is an exception to the sample size limitation; the study compared 1064 patients with nonaffective psychotic disorders (among these were 117 with PsyNOS and 731 with schizophrenia) and found PsyNOS patients to have higher remission rates (23%) than SCZ patients (14%), shorter duration of illness, better functioning, and less severe psychopathology (Korver-Nieberg et al. 2011). Additionally, an Asian study of 195 patients with PsyNOS found higher rates of recovery in PsyNOS than in schizophrenia (Verma et al. 2012). Notably, however, whenever patients with schizoaffective disorder or psychotic mood disorders were included, PsyNOS patients had outcomes in between those for schizophrenia and psychotic mood disorders, performing worse than those with mood disorders with psychosis, both in studies of youth (McClellan & McCurry, 1999b) and in studies of adults (Verma et al. 2012).
Importantly, short-term outcome benefits in patients with PsyNOS seem to translate into longer-term advantages, and studies in adults found remission rates >50% (Chaturvedi and Sahu 1986; Sivakumar and Chandrasekaran 1993).
In youth, however, the longer-term outcomes of patients with PsyNOS may be more heterogeneous. The few small studies point to remission rates or CGAS-defined good outcome between 20% and 68% (McClellan and McCurry 1999; Nicolson et al. 2001; Correll et al. 2008; Hassan and Taha 2011). As our co-primary outcome, we assessed categorical CGAS ratings, using the same cutoffs for good, moderate, and poor outcome as selected in a recent review on 21 studies in patients with early-onset schizophrenia and other psychotic disorders (Clemmensen et al. 2012). In terms of poor outcome, our results were quite similar: In the SCZ-S group, Clemmensen et al. found 60.1% with poor outcome, compared with 66% in our study. For the group of mixed psychotic disorders, Clemmensen et al. reported 46.8% with poor outcome and we found 42.7% in the PsyNOS group. In the pooled analysis, more individuals were reported to have a good outcome (i.e., 15.4% in SCZ-S and 19.6% in groups of mixed psychotic disorders), whereas in our sample, we found rates of 0% with good outcome in the SCZ-S group and only 7.4% in the PsyNOS, probably because some patients needing >12 weeks to improve substantially. These findings indicate that poor long-term outcome might be predictable from the early treatment phase, whereas transition from moderate to good outcome may require more time.
Although both patients with SCZ-S and those with PsyNOS improved during the 3 month follow-up, it is concerning that 40.8% of the patients in our study discontinued antipsychotics in the first 12 weeks of treatment, either because of patient/family choice (18.0%) or because of the practitioner's choice based on side effects (12.3%) or lack of efficacy (11.5%). This finding is very similar to findings from the TEOSS study, which reported all-cause discontinuation in 39.7% of youth after 8 weeks of treatment, with 13.8% discontinuing because of lack of efficacy (Sikich et al. 2008). It is even more concerning that patients with the most severe disorder, schizophrenia, more often experienced a lack of efficacy, even in this group of patients who were mostly previously antipsychotic naïve. Notably, full nonadherence, a clear mediator of poorer outcomes (Kane et al. 2013), was present in 22.0% of our sample, compared with 11.2% in the TEOSS sample (Sikich et al. 2008), but we also had antipsychotic blood levels available to supplement patient and caregiver data to identify nonadherence. These data indicate that clinicians need to pay attention to overt and covert nonadherence in the early illness phase in youth with SCZ-S.
Our finding that the PsyNOS group experienced significantly better outcomes on the CGI-I, CGI-S, and CGAS and had less discontinuation as a result of inefficacy than the SCZ-S group suggests that earlier treatment of people with psychotic disorders, including prior to having developed full schizophrenia, provides a chance for better outcomes. To what degree this translates into the ability to prevent transition from PsyNOS to full-blown schizophrenia (Correll et al. 2005, 2008) requires further study, especially in youth, in whom the diagnosis of PsyNOS is more common than that of schizophrenia. Although the present study followed patients only for 12 weeks, data have accumulated that symptomatic improvement after as little as a few weeks predicts ultimate outcomes at 3 months and beyond (for review, see Correll et al. [2011a], including in adolescents [Correll et al. 2013; Stentebjerg-Olesen et al. 2013]). Therefore, our findings of better outcomes in patients with PsyNOS than in schizophrenia patients stress the need for effective interventions in the early phases of psychotic disorders. However, more research is needed into the group of patients with poor early outcomes, trying to identify effective treatment strategies that may alter the trajectory of the illness at this early time. Even though most patients with PsyNOS will likely not go on to develop schizophrenia, treating psychosis quickly and effectively is important in order to minimize long-term disability. As mentioned, one study found 38% of youth with PsyNOS to be chronically impaired after 2 years, even without transitioning into other disorders (McClellan et al. 1999). Nevertheless, the fact that in our study both diagnostic groups had similar adverse effect burdens underscores that for patients with PsyNOS long-term antipsychotic treatment needs to be balanced against the potential for adverse effects, and that proactive adverse effect monitoring and management of antipsychotics is essential (Correll et al. 2008; Maayan and Correll 2011).
Limitations
The results of this study have to be interpreted within its limitations. These include the nonrandomized design, naturalistic treatment setting and choice, lack of research diagnostic interviews and specific psychopathology ratings, the still relatively small sample size, and short duration of follow-up. Further, more patients with SCZ-S than PsyNOS consented to the study, which could have introduced a bias. Additionally, we did not have data on long-term diagnostic outcome data in the PsyNOS group, which could indicate that the better initial outcome in this sample was driven by a subgroup of patients who ultimately turned out to have mood disorders with psychosis. Moreover, we focused only on global effectiveness and efficacy measures of all antipsychotics combined and did not formally assess nonpharmacologic treatments. Also, 18.5% of the sample did not return for follow-up visits.
High attrition is a well-known problem in psychiatric research (Martin et al. 2006; Thompson et al. 2011; Jorgensen et al. 2014). Our attrition after baseline were rather low, and we were able to capture information on medication persistence and reasons for treatment discontinuation in 124 (95.4%) of 130 patients.
Conclusion
In this naturalistic study with clinician's choice antipsychotic treatment, youth with SCZ-S disorders had both greater illness severity and lower functioning at baseline as well as after 12 weeks of antipsychotic treatment relative to PsyNOS patients, even though both groups improved significantly. Treatment discontinuation was common within 12 weeks in both groups of patients.
These data suggest that early treatment and intervention in youth during the initial stages of psychotic disorders are critical for increasing the chances of improving the symptomatic and functional outcome in this vulnerable population. These data also underscore the high percentage of noncompliance and discontinuation with antipsychotic treatment early during the illness course.
Clinical Significance
Our findings indicate that clinicians should comprehensively screen for the presence of psychotic symptoms in children and adolescents and address full psychotic disorders as early as possible. Treating patients in the early phases of psychosis may lead to better short and long-term outcomes, reducing the risk of more chronic impairment. Following this line of argument, identification of prodromal youth and intervention with the lowest risk treatment options during that earliest stage of illness development should also be aimed for (Correll et al. 2010; Schimmelmann et al. 2013b; Stafford et al. 2013). Antipsychotics, however, should likely be avoided during the clinical high-risk stage, as the majority of people with attenuated positive symptoms will not go on to develop full-blown psychosis (Fusar-Poli et al. 2012), which is also true for adolescents (Cornblatt et al. 2015). The clinical high-risk stage, or attenuated psychosis syndrome as per Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-V), is differentiated clinically from PsyNOS by the absence of threshold psychotic symptoms; that is, delusions, hallucinations, or disorganized thought/speech (American Psychiatric Association 2013). Finally, proactive monitoring of side effects and efficacy along with careful risk–benefit evaluation of treatment choice continue to be extremely important in this patient population because of the high likelihood of nonpersistence, with a relatively high incidence of side-effects and lack of efficacy (Correll 2008; Maayan and Correll 2011).
Footnotes
Disclosures
Ms. Vernal and Drs. Al-Jadiri, Sheridan, Borenstein, Mormando, David, Singh, Seidman, Gerstenberg, and Saito, have nothing to disclose. Dr. Kane has been a consultant to Alkermes, Amgen, Astra-Zeneca, Bristol-Myers Squibb, Dainippon Sumitomo/Sepracor/Sunovion, Eli Lilly, IntraCellular Therapies, Janssen, Johnson & Johnson, Lundbeck, Merck, Novartis, Otsuka, Pfizer, Pierre Fabre, Proteus, Roche, Rules Based Medicine, Sunovion, Takeda, Targacept, and Vanda, and has received honoraria for lectures from Boehringer-Ingelheim, Bristol-Myers Squibb, Eli Lilly, Esai, Janssen, Merck, and Otsuka, and he is a shareholder of MedAvante. He has received grant support from The National Institute of Mental Health. Dr. Steinhausen has worked as an advisor and speaker for Eli Lilly, Janssen-Cilag, Medice, Novartis, Shire, and Union Chimigul Belge. More than 4 years ago, he received unrestricted grants for postgraduate training courses or conferences and research from Eli Lilly, Janssen-Cilag, Medice, Novartis, and Swedish Orphan International. Dr. Correll has been a consultant and/or advisor to or has received honoraria from: Actelion, Alexza; American Academy of Child and Adolescent Psychiatry, Bristol-Myers Squibb, Cephalon, Eli Lilly, Genentech, Gerson Lehrman Group, IntraCellular Therapies, Lundbeck, Medavante, Medscape, Merck, National Institute of Mental Health, Janssen/J&J, Otsuka, Pfizer, ProPhase, Roche, Sunovion, Takeda, Teva, and Vanda. He has received grant support from Bristol-Myers Squibb, Feinstein Institute for Medical Research, Janssen/J&J, National Institute of Mental Health, Novo Nordisk A/S, and Otsuka. Dr. Carbon has the same disclosure information as Dr. Correll because of a family relationship. Dr. Kapoor has nothing to declare.